
Abstract
Objectives
Whether incompetent perforator veins (IPVs) require treatment remains controversial. We retrospectively evaluated the feasibility of IPV excision performed using the stab avulsion technique without ligation and sutures in patients undergoing endovenous ablation (EA).
Methods
This was a single-center, retrospective, observational cohort study. EA was performed in 1503 consecutive patients, including 33 patients with ulcers, between December 2014 and May 2021. Varicectomy was performed using the stab avulsion technique; IPV cases were included.
Results
Stab avulsion was performed at a mean number of 11.4 ± 7.8 sites. No deep vein thromboses or pulmonary emboli were noted. The incidence of nerve injury was 0.3%. All 33 (100%) patients with ulcers achieved healing by 1 year (median: 55.5 days; range: 13–365 days).
Conclusions
IPV excision via stab avulsion may be a viable option for treating varicose veins and ulcers. This technique offers multiple advantages, including simplicity, safety, and reduced healthcare costs.
Introduction
Endovenous ablation (EA) and stab avulsion are presently considered the standard treatment methods for saphenous vein insufficiency and varicectomy. However, whether incompetent perforator veins (IPVs) require treatment remains controversial. 1 Research has shown a clear association between the presence of IPVs and recurrent varicose veins/venous ulcers.2,3
Certain measures such as ligation of the IPV at the fascia, sub-fascial endoscopic perforator vein surgery (SEPS), 4 TRansLuminal Occlusion of Perforators (TRLOP) 5 techniques, and the use of cyanoacrylate products 6 are utilized in IPV treatment. As an open surgery, ligation of the IPV at the fascia carries the risk of infection and delayed wound healing. Endovenous methods require special techniques and/or instruments and are time-consuming. To address these issues, we performed IPV extraction using stab avulsion without ligation and sutures. 7 This method requires an appropriate strategy to prevent bleeding, infection, nerve injury, and deep vein thrombosis (DVT). We recently reported a multidisciplinary treatment strategy for venous ulcers that involved the use of stab avulsion and IPV extraction. 8 In the present study, we evaluated the benefits and safety of IPV extraction using stab avulsion in a larger sample of patients who underwent EA. Considering its simplicity, safety, efficiency, and impact on healthcare economics, this method may represent a viable option for treating varicose veins and ulcers.
Methods
Ethics statements
This study was performed in accordance with the principles of the Declaration of Helsinki. The experimental protocol of this study was approved by the Institutional Review Board of Okamura Memorial Hospital (approval number: A021-001, A021-002). Written informed consent, as well as publication consent, when applicable, was obtained from the participants.
Study population
We included 1503 patients who underwent EA between December 2014 and May 2021. The inclusion criterion was a diagnosis of primary varicose veins requiring correction of venous reflux. IPVs with a diameter of 4 mm or more, which are those having >0.5 s reflux duration, were generally considered for resection; however, those with a diameter of less than 4 mm, such as those directly underneath prominent varicose veins, were resected as much as possible. The exclusion criteria were secondary varicose veins, a history of DVT, and the use of hormone medications.
Basic treatment methods at our institution
Patients were admitted overnight, and treatment was performed on one leg under local anesthesia in all cases. 7 If both lower extremities required treatment, the opposite side was treated approximately 1 month later. Patients were instructed to quit smoking for at least 2 months before surgery. Two current smokers with ulcers had delayed intervention due to smoking cessation. A radiofrequency catheter (ClosureFast; Covidien, Tokyo, Japan) was used, and standard methods were employed. 9 Ablation of the great saphenous vein (GSV) was not performed on the peripheral two-thirds of the lower leg. Ablation of the small saphenous vein (SSV) was performed within the area spanning the back of the knee line to approximately one half of the proximal side. The stab avulsion technique 10 was used for the resection of varicose veins, including IPVs. An echogram was performed at the initial outpatient visit, and IPVs associated with varicose veins were noted. Our institution’s policy is to actively resect IPVs when they are not likely to cause nerve injury except the Cockett perforator and the IPV in the lateral area of the lower leg. If patients with active ulcers had IPVs, these were marked using ultrasonography immediately preoperatively, and varicose veins communicating with these IPVs were removed as much as possible via stab avulsion, as in the case of other types of varicose veins. The reflux time of common femoral veins was not recorded and analyzed in this study. 11 Lesions with a severity of C4b (lipodermatosclerosis or atrophie blanche) or greater that exhibited adhesions to the surrounding tissue and fragile vascular walls that were impossible to strip were treated by breaking down the vascular bed using a Varady hook and scraping spatula, and compression hemostasis was performed. Ligation of the IPV at the fascia was considered for relatively large IPVs of approximately 7 mm or greater.
If patients were taking anticoagulants or antiplatelet drugs that could not be withdrawn, stab avulsion was not performed. DVT prophylaxis adhered to the EA guidelines. 12 The following measures were taken to alleviate preoperative and intraoperative pain: To avoid saphenous nerve injury, the main trunk of the GSV in the peripheral one third of the lower leg was marked using echography preoperatively, and sufficient tumescent local anesthesia (TLA) fluid (40 mL of 1% lidocaine with epinephrine and 500 mL of saline prepared with 20 mL of sodium bicarbonate; adjusted to 0.1% lidocaine) was injected to avoid traction pain caused by varicectomy. Varicectomy was also performed carefully distally to the marking. It was not performed directly above the SSV along the course of the sural nerve and peroneal nerve, lateral to the lower leg, or peripheral to the ankle joint.
In the 1228 patients whose Okamura Pain Scale (OPS) 7 scores had been revised and made available for evaluation, intraoperative pain was objectively assessed using the OPS scores. The Numerical Rating Scale (NRS) 13 score (0–10) was assessed postoperatively and compared with the objective pain rating.
Prophylactic antibiotics (intravenous cefazolin 1 g) were administered. Notably, prophylactic antibiotics have not been used for general varicose vein surgery at our institution since November 2019. However, we used them in the presence of implant materials and in patients with advanced skin lesions (e.g., ulcers and atopic dermatitis), those with uncontrolled diabetes, and those using steroid ointment due to a high risk of infection.
Postoperative care
The stab avulsion sites were covered with absorbent pads and elastic bandages, and stockings providing moderate pressure (30–40 mmHg) were placed over the bandages with attention to the development of peripheral nerve injury. If the operation was performed on the thigh, the area was lightly compressed with a supporter overnight. Patients were encouraged to walk from the operating room back to the ward, to continue to walk actively (100–200 m in the ward approximately 3–5 times per hour) under observation by the medical staff; furthermore, they were advised to watch for bleeding after surgery. They were also instructed to move their legs if they woke up during the night on the day of surgery, as they were at high risk of developing a pulmonary infarction on the morning of the first day after surgery.
The stab avulsion sites were fixed with surgical tape and covered with dressings containing absorbent pads on the morning after surgery. The patient’s leg was placed in elastic stockings below the knee and asked to walk 300–500 m. Once the absence of bleeding was confirmed, the patient was discharged from the hospital. The surgical tape was removed during the first outpatient visit after surgery (postoperative days 1–5), and stab avulsion sites with oozing were once again fixed with surgical tape or covered with a hydrocolloid dressing. Below-the-knee elastic stockings were worn all day for 1 week postoperatively. Subsequently, they were worn only during the daytime for 2 weeks if edema occurred. This treatment continued until healing in cases of severe skin lesions, such as ulcers.
Patients underwent clinical examination and venous duplex ultrasonography before the operation, 1–5 days after the operation, and 1 and 3 months after the operation. Wounds with ulcers were treated as follows: (1) The ulcer site was washed under the shower twice daily after which it was semi-closed using a Plus moist™ dressing (Zuiko Medical, Osaka, Japan) or a Zuikopad (Zuiko Medical, Osaka, Japan) (bathing was permitted); (2) soap was not used; (3) agents such as povidone–iodine, antibiotic ointments, trafermin, and silver sulfadiazine were never used on the ulcer site; (4) debridement was usually unnecessary; and (5) patients were instructed to visit the hospital immediately they noticed any signs of infection, such as spontaneous pain, an unpleasant smell, redness of the skin, or increased discharge.
Ulcer healing was considered to have occurred when the ulcer was covered with the epidermis and no exudate adhered to the dressings. Moisturizers and bath additives rich in white petroleum jelly were recommended to prevent itching from stasis dermatitis.
Statistical analyses
Numbers are expressed as mean ± standard deviation (minimum–maximum). Median was calculated using Microsoft Excel 2019 version 2005 (Microsoft, Redmond, WA, USA).
Results
The mean patient age was 66.5 ± 11.2 years (17–92 years); 544 were male, and 959 were female. The Clinical–Etiology–Anatomy–Pathophysiology classifications 14 were as follows: C2, 686 limbs; C3, 152 limbs; C4a, 475 limbs; C4b, 129 limbs; C5, 28 limbs; and C6, 33 limbs. Cauterization sites were the GSV in 1206 limbs, SSV in 245 limbs, and GSV + SSV in 52 limbs.
The mean operative time for the 1503 legs was 32.6 ± 15.1 (5–116) min. Stab avulsion was performed at a mean number of 11.4 ± 7.8 (0–54) sites. The mean ablation length was 27.9 ± 10.7 (3–59) cm, and the mean volume of the TLA solution used was 536.1 ± 164.3 (44–1160) mL. The only sedative was a preoperative dose of intravenous hydroxyzine (6.25–12.5 mg), and no additional medication was required. No additional inhalation or intravenous anesthesia was used.
The intraoperative pain scores on the OPS and NRS were 1.5 ± 1.3 (0–4) and 3.0 ± 2.0 (0–10), respectively. All patients were able to walk immediately after surgery. No additional sclerotherapy was administered. No cases of DVT or pulmonary embolism occurred. One patient with class 3 endovenous heat-induced thrombosis (EHIT) required a direct oral anticoagulant (DOAC). Another patient had class 2 EHIT initially, which progressed to class 3 after hormone therapy at another clinic. This patient also required a DOAC as well as cessation of hormone therapy, following which the thrombosis disappeared. Overall, five patients (0.3%) had nerve injury: Three had sensory numbness in the distal part of the saphenous nerve, one had it around the IPV, and one had sural nerve injury. After radiofrequency ablation, recanalization was noted in two patients (an IPV ablation with a length of 3.5 cm in the thigh and SSV ablation with a length of 10 cm, respectively). No patient required hospitalization beyond a single night. However, several patients visited the outpatient department ahead of schedule because of bleeding; a few of these patients even required suturing. Approximately one in 10–20 patients experienced oozing on the outer sides of the elastic stockings after surgery. In such cases, gauze was applied from the outside to ensure greater pressure. 17 patients (1.1%) used oral or intravenous antibiotics for suspected surgical site infection.
Ulcer cases
Data for patients with ulcers.
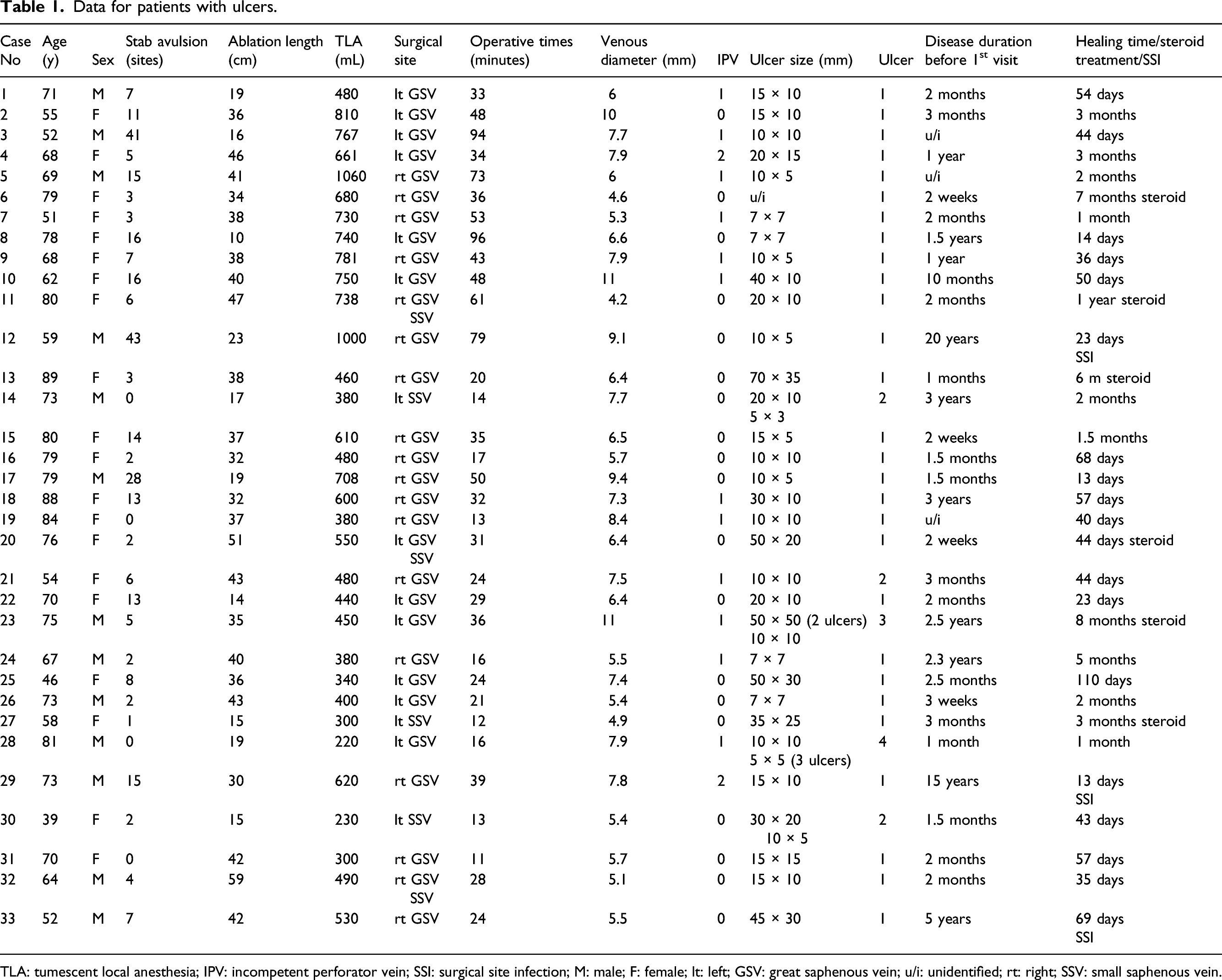
TLA: tumescent local anesthesia; IPV: incompetent perforator vein; SSI: surgical site infection; M: male; F: female; lt: left; GSV: great saphenous vein; u/i: unidentified; rt: right; SSV: small saphenous vein.
Figure 1 shows the typical course of ulcer healing. Cases 12, 29, and 33 (mentioned in Table 1) developed surgical site infections that were treated using antibiotics during postoperative outpatient appointments. Skin incisions measuring 1–3 mm healed within approximately 1 week, even in the case of C4b varicose veins. No ulceration except one: case 11 recurred. In addition, all 33 patients achieved healing within 1 year. Case 11 recently came to our hospital with recurrence of leg ulcer at 4 years postoperation. She was an elderly patient with dementia, and edema due to decreased ADL was considered the cause of the ulcer recurrence. Wound treatment with silver sulfadiazine at another clinic was also thought to be a factor in ulcer enlargement. Preoperative echocardiography showed no IPV in this case. Typical case of a healed venous ulcer. Case 4, a 68-year-old woman with a total healing time of 3 months. (a) Before the operation. (b) Five months after the operation.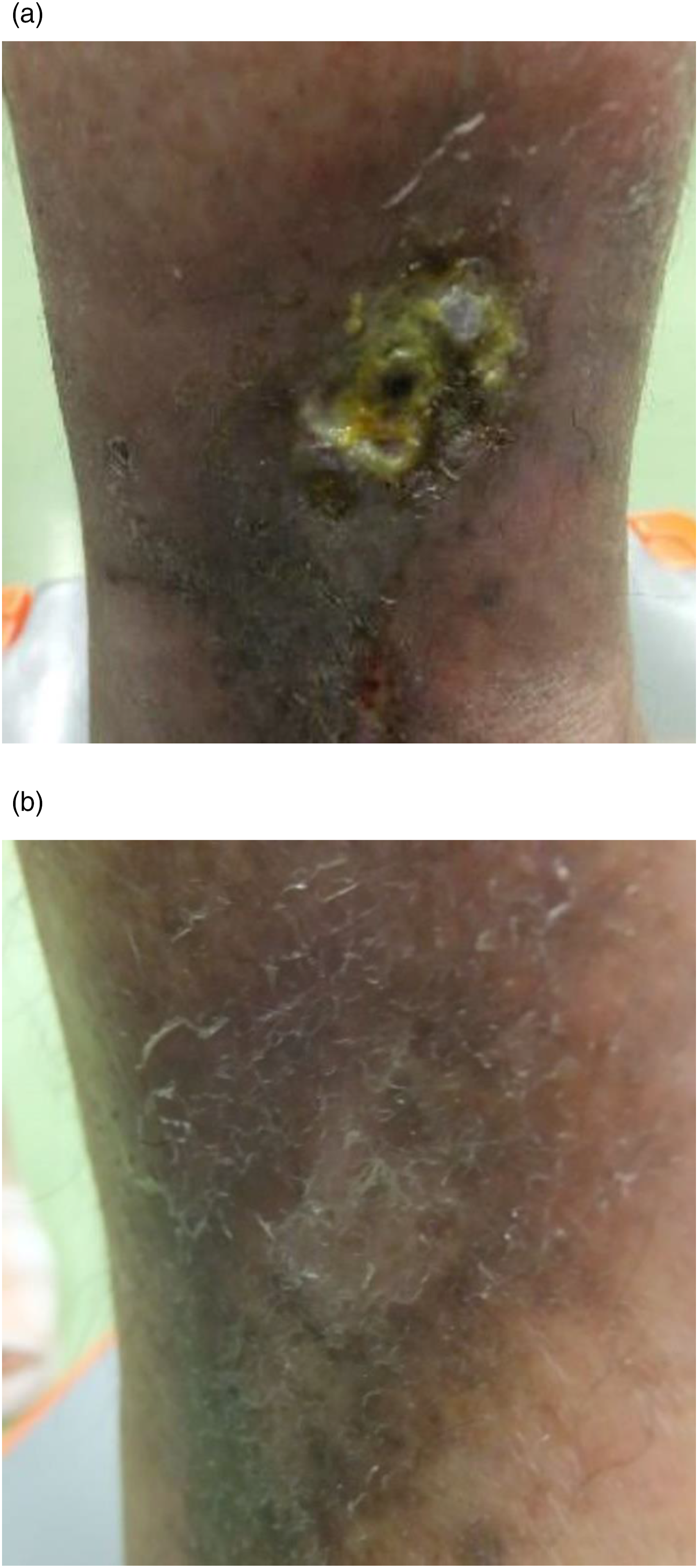
Discussion
In this retrospective analysis of 1503 consecutive patients who underwent EA with local anesthesia, we observed no cases of DVT or PE. The incidence of nerve injury was 0.3%. Additionally, nerve injury around IPVs occurred in only one case. DVT and PE are rare complications of EA, with reported frequencies of <0.5% and approximately 0.1% in Europe and the United States, respectively. 15 However, the incidence of nerve injury is relatively high, ranging from 1 to 5%. 16 In the present study, incidence rates of nerve injury in spite of IPV extraction using the stab avulsion technique were lower than those reported in previous studies. Complications associated with IPV removal include bleeding, DVT, nerve injury, surgical site infection (SSI), and delayed wound healing. Our results highlight the safety of removing IPVs via stab avulsion without the need for ligation and suturing. Before 1985, the ligation of IPVs required open surgery. However, blind extraction of IPVs has been performed successfully since the era of stripping, even when using the Dodd perforator. Our goal is to ensure a safe, uncomplicated, cosmetically superior procedure with a low risk of recurrence and no need for additional treatment. This goal is difficult to achieve when IPVs are preserved.
Ligation of the IPV at the fascia was performed in fewer than 10 cases in the present study. If the IPVs were not confirmed using preoperative echography, it is possible that they were unintentionally removed during stab avulsion.
Although the need for IPV treatment remains controversial, research has shown that there is a clear association between the presence of IPVs and recurrent varicose veins and ulcers. A previous study described the use of radiofrequency ablation (RFA) to treat IPVs. 17 However, we did not use the SEPS or TRLOP techniques except in one case. We performed this measure in one IPV of a young patient using RFA; however, early recanalization occurred in the thigh due to the short segment length, and we have ceased to use this method.
When patients with IPVs had active ulcers, they were marked using ultrasonography immediately preoperatively, and any varicose veins communicating with these IPVs were removed as much as possible by performing stab avulsion and compression hemostasis. Sites with IPVs often have prominent varicose veins; we do not believe that it is necessary to avoid IPVs when performing stab avulsion. It is also difficult to recognize IPVs during extraction. Even if the IPVs were not completely removed, the original goal was achieved by eliminating as much contact with the surrounding varicose veins as possible.
In terms of surgical site management, dermal adhesive and wound suturing should be avoided, given the risk of remaining TLA and hematoma in the subcutaneous area, which can lead to SSI. Wound management should incorporate moist wound healing 8 to achieve complete epidermis coverage.
An OPS score of 4 or higher should be considered indicative of possible nerve injury. In this study, one sural nerve injury was noted in a patient who underwent GSV ablation with 24 stab avulsion sites. Sural nerve injury can result in burning pain, diminished sensation, or loss of sensation. This nerve passes down from the back of the knee along the outside of the lower leg. It is located along the surface of the lower one-third of the leg. Injury to the sural nerve can occur due to compression of the bandage or stab avulsion on the outer side of the leg. SSV ablation was not performed, and such cases were excluded from this study. In this case, OPS scores for the stab avulsion section and other sections were 4 and 0, respectively, suggesting that the cause occurred during stab avulsion.
Adequate ambulation immediately after surgery is effective in preventing DVT. Most patients will stay in bed if not instructed otherwise; thus, active ambulation should be encouraged. Further, patients should be encouraged to quit smoking 18 as the first step in the process, as smoking is an important risk factor for thromboembolism, including DVT, 19 delayed wound healing, 20 venous insufficiency, 21 and SSIs. 22
This study has a few limitations, including its single-center design, which may have resulted in selection bias. Furthermore, we did not evaluate every IPV removal after surgery using echography; therefore, the success rate of resection of the IPVs in this study could not be determined. Thus, multicenter studies are needed to validate our findings.
In conclusion, IPV excision using stab avulsion without ligation or suturing may represent a viable option for treating varicose veins and ulcers; however, the percentage contribution of the IPV excision to this clinical success (all the ulcers healed and no additional sclerotherapy was required) is not known. While this method requires operation under local anesthesia as well as pain evaluation using the OPS to avoid nerve injury, it offers multiple advantages, including simplicity of intervention, safety, efficiency, and a positive impact on healthcare economics. Active leg movement and walking are essential for avoiding DVT after varicose vein surgery. Nonetheless, as IPVs were not ligated in this study, patients should be carefully monitored for increased bleeding due to lower limb movement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The experimental protocol of this study was approved by the Institutional Review Board of Okamura Memorial Hospital (approval number: A021-001, A021-002).
Guarantor
KY
Author contributions
Conception and design: KY and SM. Analysis and interpretation: KY, SK, and SE. Data collection: KY, TY, SS, and MH. Writing of the article: KY and SM. Critical revision of the article: KY, SM, TY, SS, MH, SK, and SE. Final approval of the manuscript: KY, SM, TY, SS, MH, SK, and SE. Statistical analysis: KY and SM. Overall responsibility: KY.