
Abstract
Objectives
To examine three different methods for evaluating the effect of percutaneous sclerotherapy on limb venous malformations in a series of patients with a relatively long follow-up.
Method
The study was a retrospective study.
Results
Thirty-eight patients treated with percutaneous sclerotherapy underwent sclerotherapy, with a median number of sessions of 4 (range, 1–10). They were followed up for 1–60 months (average 12.5 months). The kappa between clinical manifestations and Doppler ultrasound was 0.684 (P < 0.001). The kappa between clinical manifestations and magnetic resonance imaging was 0.217 (P = 0.006). The kappa between Doppler ultrasound and magnetic resonance imaging was 0.323 (P < 0.001). The rate of grade IV patients evaluated by clinical manifestations was significantly higher than that by Doppler ultrasound and magnetic resonance imaging.
Conclusions
Magnetic resonance imaging is the gold standard for VM imaging. Its consistency with clinical examination and Doppler ultrasound is poor, and Doppler ultrasound and clinical examination could be more appropriate for follow-up imaging after sclerotherapy.
Keywords
Introduction
Congenital vascular malformations (CVMs) are malformed vessels resulting from arrested development during various stages of embryogenesis. CVMs are further divided into slow-flow (venous, lymphatic, and capillary malformations) and fast-flow malformations (arteriovenous malformations and arteriovenous fistula). 1 Venous malformation (VM) is the most common CVM. VM often occurs in the head, neck, and limbs, 2 involving the skin, subcutaneous tissues, muscle nerves, and joints. VM may lead to pain, bleeding, severe deformity, dysfunction, complicated deep venous thrombosis, pulmonary artery embolism, and sudden death. 3 Large VMs are often associated with localized intravascular coagulopathy, a consumptive coagulopathy characterized by elevated D-dimer levels and decreased fibrinogen levels.4,5
The main auxiliary examinations of VMs include Doppler ultrasound (DUS), magnetic resonance imaging (MRI), and venography. DUS can clarify whether the CVM is arterial or venous in nature, and determine the blood flow rate and range and size of VMs. 6 MRI can clearly show the relationship between the lesions and the surrounding muscles, nerves, and joints, and guide the Birmingham typing. 6 Venography can reveal the size and range of the malformed vessels and their relationship with the deep veins and guide the Puig typing.6,7 Nevertheless, it is important to note that those imaging modalities provide different assessments of the lesions. Because of its high resolution for soft tissues, MRI remains the gold standard for VM imaging, while DUS and venography can provide useful information about the blood flow and blood distribution and path in the VMs. On the other hand, DUS is more easily accessible and less expensive than MRI.
The treatment methods of VMs mainly include conservative follow-up observation, surgical resection, and endovascular treatment. 8 Sclerotherapy is also an option. The commonly used sclerosing agents include ethanol and detergent-based sclerosants.9,10 In sclerotherapy, a sclerosing agent is injected into the vessels, making them shrink. 11 Pure ethanol is the most effective sclerosing agent available, but it can be associated with systemic complications at high doses. 12 The direct contact of pure ethanol with the vascular endothelium will promote protein denaturation, vessel wall necrosis, and disruption of erythrocytes, leading to thrombosis and fibrosis. 13 Detergent-based sclerosants will lead to organized thrombus, endothelium denudation, inflammation, and permanent luminal occlusion. 14 The possible adverse effects of sclerotherapy include skin and mucosal necrosis, deep venous thrombosis, pulmonary embolism, nerve damage, and acute cardiopulmonary failure.15,16
Previous studies showed that sclerotherapy is an effective treatment method for VMs.17,18 Imaging is mainly used for the efficacy evaluation of sclerosing agents in treating VMs, 19 but some studies also adopted the comprehensive assessment combined with clinical manifestations. 20 No recognized or unified evaluation method and standard exist in China and other countries, and the best monitoring method remains unknown. The long-term follow-up observation is important for the timely adjustment of sclerotherapy, determination of treatment timing, and prognosis.
Hence, this study aimed to examine three different methods for evaluating the effect of percutaneous sclerotherapy on limb VMs in a series of patients with a relatively long follow-up. The results could provide meaningful information for the clinical management of these lesions.
Methods
Study design and patients
The study was a retrospective clinical study conducted at the Department of Vascular Surgery of the No. 1 Affiliated Hospital of Fujian Medical University and included patients operated between 1 November 2011, and 31 December 2017. Thirty-eight patients were included and the follow-up was 1–60 months, with an average of 12.5 months. This study was reviewed and approved by the Medical Ethics Committee of the First Affiliated Hospital of Fujian Medical University (approval number [2018] No. 111).
The inclusion criteria were: (1) patients diagnosed with limb VM; (2) patients with signs or symptoms; (3) without a history of previous percutaneous sclerotherapy; and (4) patients with pre- and post-treatment DUS and MRI. The exclusion criteria were: (1) digital subtraction angiography (DSA), MRI, or DUS revealing arterial malformations, arteriovenous malformation, lymphatic malformations, capillary malformation, or combined vascular malformations; or (2) patients with incomplete clinical data.
Treatment
All patients were treated with sclerotherapy. The puncture needle was inserted into the VM lumen under DUS or DSA guidance. When the blood returned, the sclerosing agent was manually pushed. After sclerotherapy, the limbs were bandaged with an elastic bandage. Severe complications such as pulmonary embolism, pulmonary fibrosis, and limb necrosis were closely monitored in all patients after treatment. Transient pain, swelling, and numbness were observed.
Outcome assessment
The effect of treatment as evaluated by clinical manifestations was 11 : grade I, no improvement in symptoms and signs; grade II, pain, numbness, or swelling slightly relieved, dysfunction slightly improved, or pigmentation slightly improved; grade III, pain, numbness, or swelling reduced up to the degree of tolerance, functional recovery to normal daily life, or skin pigmentation improved significantly but not completely normal; grade IV, no pain, numbness, swelling, or dysfunction, and skin pigmentation returned to normal. The effect of treatment as evaluated by imaging was 21 : narrow scope of the degree evaluated by DUS or MRI; grade I, ≤25%; grade II, 26%–50%; grade III, 51%–75%; and grade IV, 76%–100%.
Statistical analysis
All evaluable patients included in the study were considered for analysis. All analyses were primarily performed by descriptive statistical methods. Continuous variables were described in terms of the number of patients with valid observations, median, and range. Categorical variables were described as frequencies and related percentages per class level, as well as the number of patients with valid observations. The results of the therapeutic evaluation in the clinical efficacy and imaging (DUS and MRI) were checked for consistency (kappa test), and pairwise consistency of the data was evaluated. Statistical analysis was carried out using SPSS 21.0 (IBM Corp., Armonk, NY. USA). Two-sided P-values <0.05 were considered statistically significant.
Results
Characteristics of the patients
Thirty-eight patients were included. Among them, 17 (44.7%) patients were male, and 21 (55.26%) were female; the mean age was 22.5 years (range, 5–48). Twelve (31.6%) patients had upper limb involvement, and 26 (68.4%) had lower limb involvement. The majority of the patients (33, 86.8%) had VMs larger than 5 cm. Meanwhile, 25 (65.8%) patients had pain and/or numbness, 19 (50.0%) had swelling after exercise, and two (5.26%) showed limb movement disorder (Table 1).
Characteristics of the patients.
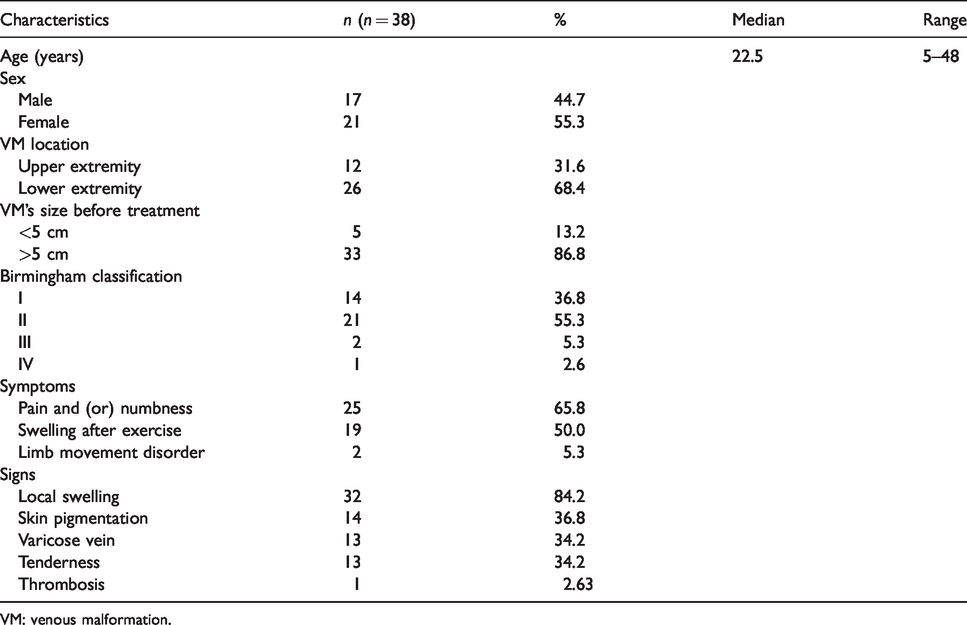
VM: venous malformation.
Treatment
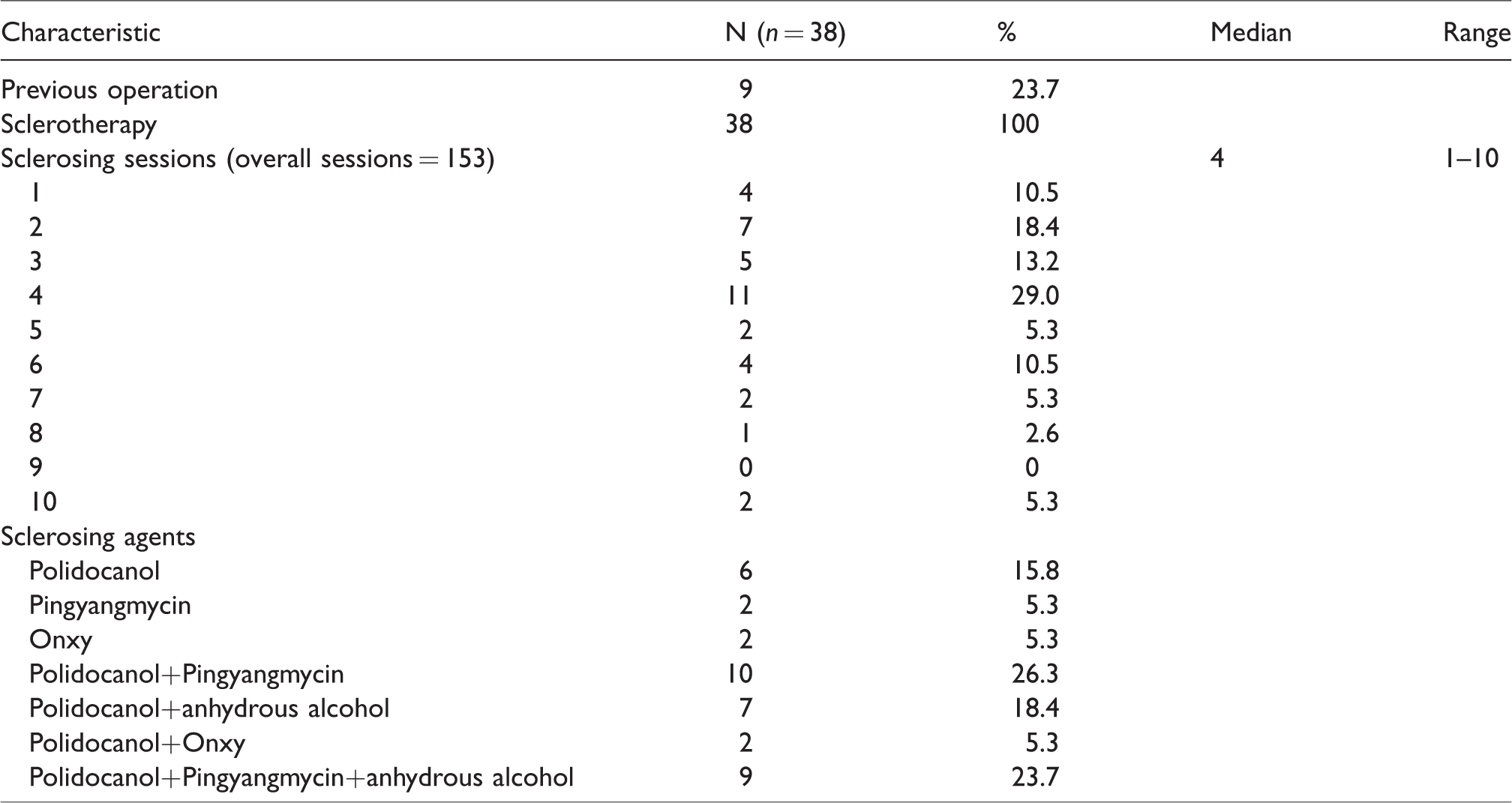
The follow-up was 1–60 months, with an average of 12.5 months. Nine (23.7%) had a history of another operation of their VM. All patients underwent sclerotherapy, with a median number of sessions of 4 (range, 1–10). The sclerosing agents used are shown in Table 2. The most common was polidocanol combined with pingyangmycin (n-10, 26.3%).
Treatment characteristics.
Sclerotherapy outcomes
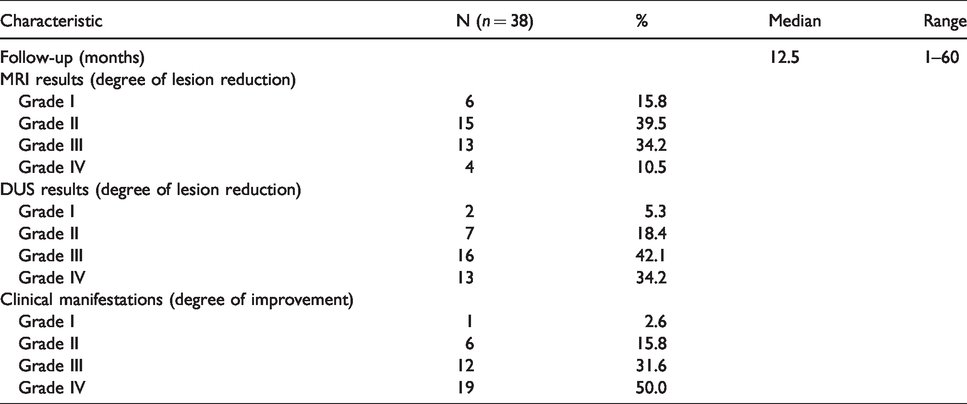
The effect of treatment, as evaluated by clinical manifestations, showed: grade IV in 19 patients (50%), grade III in 12 (31.5%), grade II in six (15.8%), and grade I in one (2.6%). The effect of treatment as evaluated by DUS showed: grade IV in 13 patients (34.2%), grade III in 16 (42.1%), grade II in seven (18.4%), and grade I in two (5.3%). The effect of treatment as evaluated by MRI: grade IV found in four patients (10.5%), grade III in 13 (34.2%), grade II in 15 (39.5%), and grade I in six (15.8%) (Table 3).
Sclerotherapy outcomes.
Agreement analyses
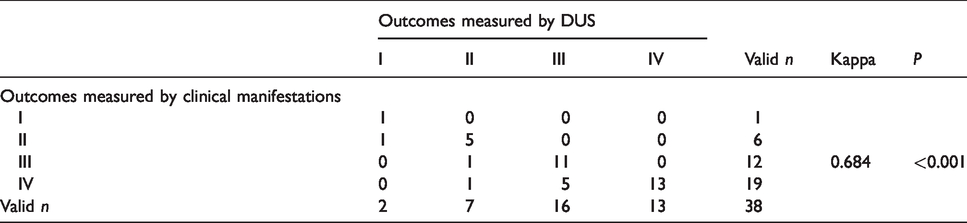
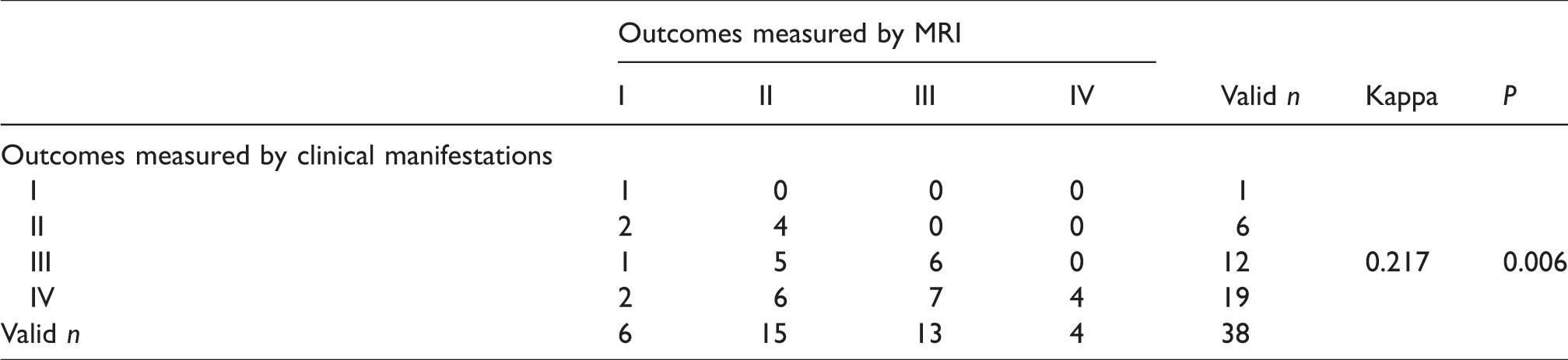
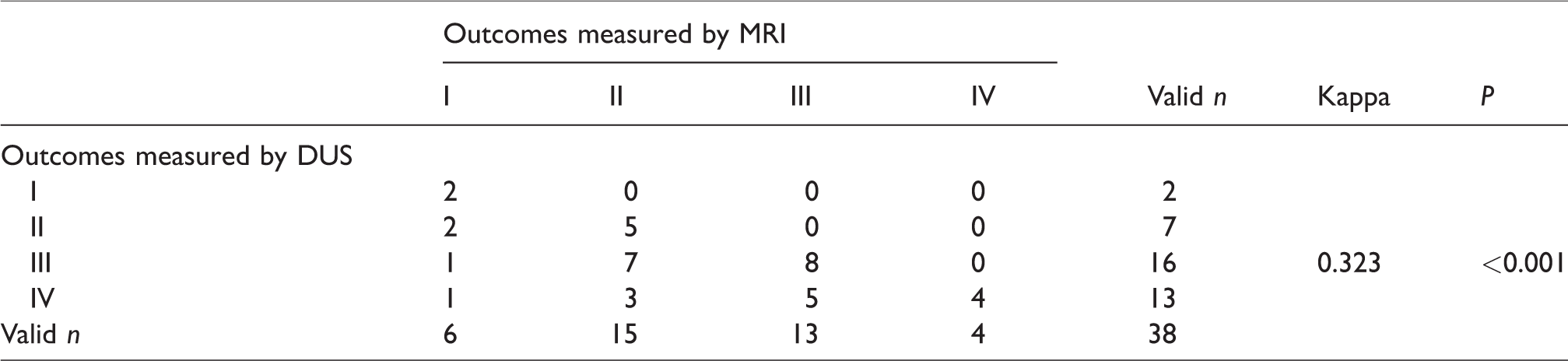
The kappa between clinical manifestations and DUS was 0.684 (P < 0.001) (Table 4). The kappa between clinical manifestations and MRI was 0.217 (P = 0.006) (Table 5). The kappa between DUS and MRI was 0.323 (P < 0.001) (Table 6). The rate of grade IV patients evaluated by clinical manifestations was significantly higher than that by DUS and MRI.
DUS and clinical manifestations-measured outcomes.
MRI and clinical manifestations-measured outcomes.
MRI and DUS-measured outcomes.
Typical case
Figures 1 (MRI) and 2 (clinical evaluation) show a typical case. A 23-year-old female patient had a right upper arm mass for 15 years. The mass was treated with polyoxyethylene lauryl ether and Pingyangmycin combined with absolute alcohol. After six months, the clinical performance was grade III. The color Doppler ultrasound evaluation was grade III. The MRI evaluation was grade III.
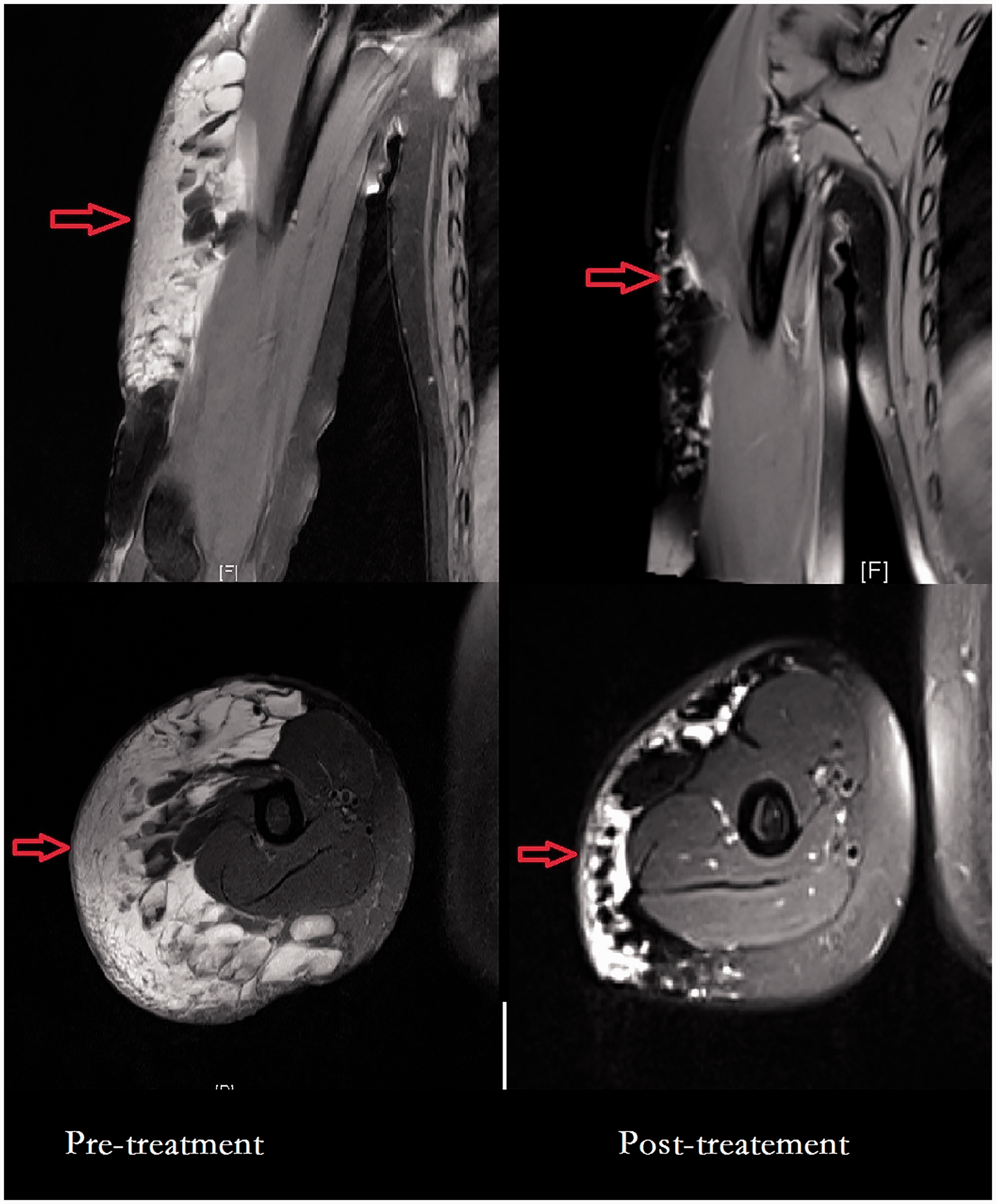
Comparison of magnetic resonance imaging before and after sclerotherapy.
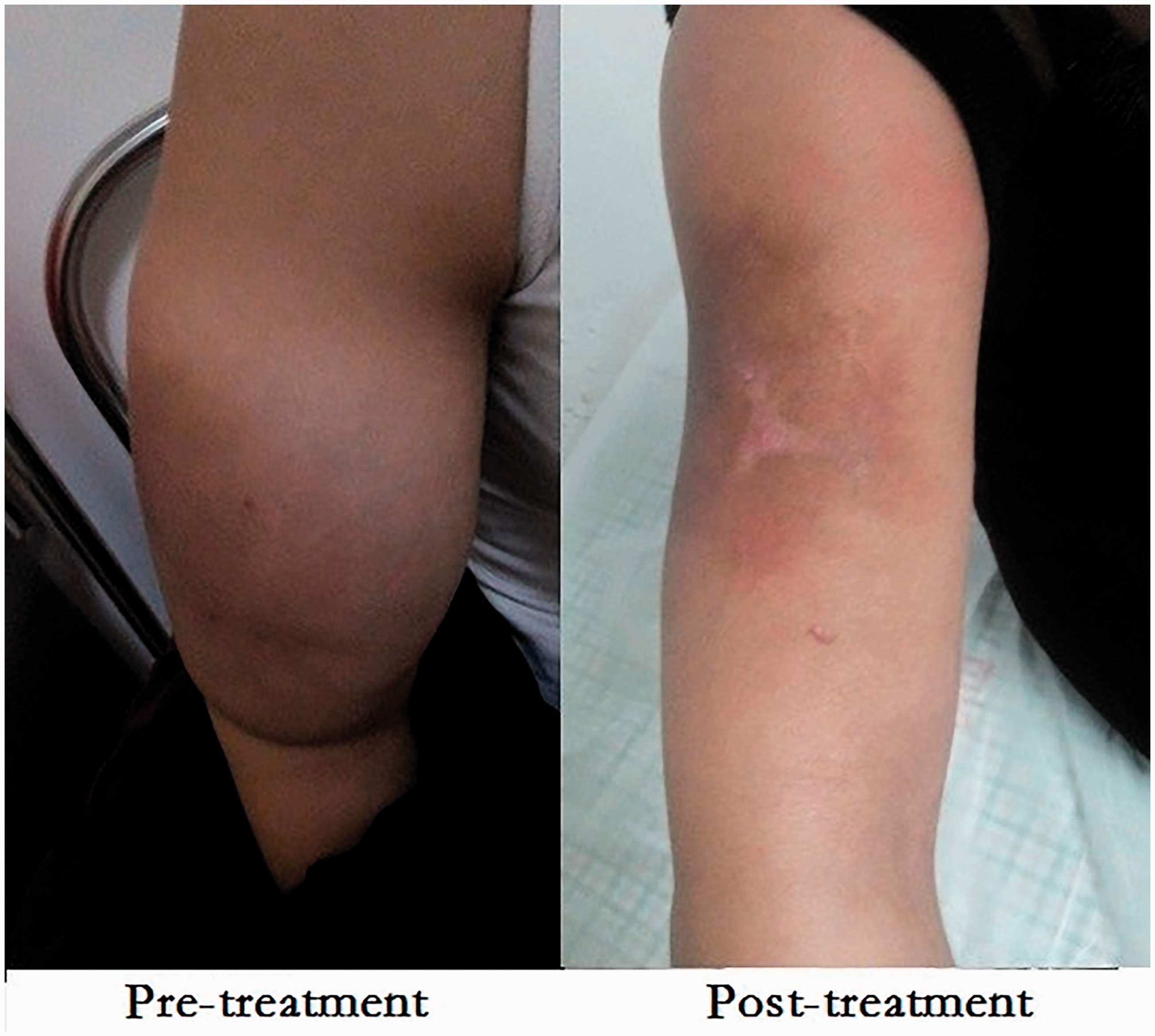
Comparison of clinical findings before and after sclerotherapy. A 23-year-old female patient had a right upper arm mass for 15 years, with swelling of the right upper arm, local surface pigmentation, and tenderness. The mass was treated with polyoxyethylene lauryl ether and Pingyang mildew combined with absolute alcohol. After six months, pain and tenderness were improved and the swelling was improved, without complications. The clinical performance was grade III. The color Doppler ultrasound evaluation was grade III. The MRI evaluation was grade III.
Discussion
VMs are still difficult to cure completely. Multiple long-term treatments and follow-up observations are required, and what is the best monitoring method remains unknown. Previous studies showed that sclerotherapy is an effective treatment method for VMs.17,18 Imaging is mainly used for the efficacy evaluation of sclerosing agents in treating VMs, 19 but some studies also adopted the comprehensive assessment combined with clinical manifestations. 20 No recognized or unified evaluation method and standard exist in China and other countries. Therefore, this study aimed to examine three different methods for evaluating the effect of percutaneous sclerotherapy on limb VMs in a series of patients with a relatively long follow-up. The results showed that after the treatment of VMs with sclerotherapy, the consistency between DUS and clinical manifestations is relatively good. The consistency of MRI with clinical examination and DUS is poor. MRI could be recommended as a secondary choice for imaging follow-up.
During the follow-up in this study, clinical manifestations were found to improve in most patients, and most of them multiple treatments, which is consistent with the literature. 8 The effectiveness of sclerotherapy for VMs is mainly assessed from two aspects: clinical manifestations and imaging. Here, the clinical observation indicated that the symptoms and signs of some patients improved significantly, but this was not true for imaging, especially with MRI. Indeed, according to the clinical manifestations, the proportion of grade IV patients (50%) and the effective rate (97.4%) of sclerotherapy were better, which is consistent with the literature. 22 The total effective rates (grades II–VI) of DUS and MRI were 94.7% and 84.2%, respectively. The rates for grade IV were 34.2% and 10.5%, respectively, and were significantly lower than those of the clinical evaluation. Moreover, the kappa test of consistency also showed that the kappa value of the clinical evaluation and DUS was between 0.4 and 0.75 (0.684), indicating a certain consistency. The kappa value of symptom and MRI evaluation was 0.217, indicating that the consistency between them was poor. The evaluation of curative effect using clinical symptoms and signs was inconsistent with that using imaging, and imaging underestimated the efficacy of sclerotherapy on limb VMs, which was consistent with the study by Glade et al. 19 about the treatment of head and neck VMs using a sclerosing agent.
Compared with imaging, clinical performance is relatively subjective, while imaging is relatively objective. The major aim of treatment is to improve the symptoms, functions, and appearance of VMs. Only monitoring the improvement by imaging is not enough without the improvement in clinical manifestations. At the same time, the presence of clinical symptoms is also an important criterion for treating VMs. Therefore, the improvement in clinical manifestations such as dysfunction and pain is one of the important follow-up methods, which is closely related to the development and prognosis of the disease. 23 Since the clinical examination is the first examination made by the physician before prescribing imaging examinations, clinical examination after the intervention should be the first examination to monitor treatment response.
DUS is important in the whole process of VM treatment. 24 DUS can determine the flow rate, backflow, and other vascular functions of CVM. It provides a dynamic assessment of the blood flow in the VMs. Hence, it is one of the important means in functional and morphological examinations of VMs. 25 Despite being operator-dependent, this examination is fast, inexpensive, and readily available. The present study showed that DUS has a good consistency with the improvement in clinical manifestations. Hemodynamics in the lumen is the focus of CVM, and hence DUS can be used as the preferred way of imaging follow-up. Therefore, DUS is a good, long-term follow-up mode from an economic perspective.
MRI can be used to monitor the treatment effect of VMs. 26 MRI is highly sensitive to the minute changes in soft tissues and can accurately display the lesion, as well as the changes in the lesion size and detect the development and invasion of the disease. On the other hand, MRI generally has a low specificity that is conducive to additional evaluation procedures or false-positive results. 27 MRI evaluation has a poor consistency with the clinical performance evaluation. Its assessment of blood flow is also poor, but it can clearly show the relationship between the lesion and the surrounding tissue and hence still recommended as a secondary follow-up method.27,28 In addition, MRI is expensive and is not readily available in all hospitals.
The clinical manifestations and imaging evaluation results are sometimes inconsistent. Imaging may underestimate the efficacy of sclerotherapy in treating limb VMs. The cause for such a difference between clinical manifestation and imaging evaluation is still not clear. The symptoms of VMs are mostly the formation, expansion, or further oppression of venous masses to the surrounding tissues or nerves, or changes in the skin surface due to venous return obstruction. The most common symptom is pain due to localized intravascular coagulation. 1 After sclerotherapy, the lumen is obstructed, the symptoms and signs are improved, and DUS cannot detect any blood flow. DUS evaluation is less effective than the evaluation of symptoms and signs, probably because the lesion is indeed reduced and the symptoms are improved, but some lesion tissues might remain and cannot be detected by DUS. Nevertheless, DUS will detect any residual blood flow, 29 while MRI can clearly show the scope and involvement of the surrounding tissues.30,31 It has to be noted that the sclerosing agent itself has a signal in MRI, as the original lesion. Hence, MRI immediately after sclerotherapy could lead to false-positive results. Nevertheless, even if MRI remains the gold standard for VM imaging, it is possible that other modalities such as DUS are better for follow-up after sclerotherapy, at least over the short-term after treatment.
The present study has limitations. It was a retrospective study, thus suffering from all the inherent biases. In addition, the sample size was small, and from a single center.
In conclusion, after the treatment of VMs with sclerotherapy, the consistency between DUS and clinical manifestations is relatively good. On the other hand, the consistency of MRI with clinical examination and DUS is poor. Despite MRI being the gold standard for VM imaging, DUS and clinical examination could be better options for follow-up after sclerotherapy, at least over the short term.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fujian Medical University Qihang Fund project [grant number 2017XQ1073].
Ethical approval
This study was reviewed and approved by the Medical Ethics Committee of the First Affiliated Hospital of Fujian Medical University (approval number [2018] No. 111).
Contributorship
THZ carried out the studies and drafted the manuscript. HYC, CC and YCL participated in collecting data, HZ and JCZ performed the statistical analysis and participated in its design. FGC, PFG and YJL helped to draft the manuscript. All authors read and approved the final manuscript.
Acknowledgements
Not applicable.