
Abstract
Introduction
Deep venous stenting has gained increasing interest. More flexible venous stents are thought to gain superior clinical outcomes. This research evaluated the patency and clinical outcomes between more rigid stents and more flexible stents.
Material and methods
The Venous Clinical Severity Score, Villalta, complication rates and patency rates were evaluated. The more rigid stents included the Sinus XL, the Veniti VICI and the Sinus Obliquus. The flexible group included the Zilver Vena or the Sinus Venous stents.
Results
Differences in Venous Clinical Severity Score (p = 0.09) and Villalta score were found (p = 0.28). Tapering (0 versus 5, p = 0.03) and bad alignment were found (0 versus 5, p = 0.03). The rigid stents showed patency rates of 80, 86 and 92% compared to 88, 96 and 98% in the flexible group.
Conclusion
Dedicated venous stents show good patency outcomes and clinical results. Tapering and bad alignment between connecting stents are more frequently seen in more rigid stents.
Introduction
Deep venous stenting, to treat post-thrombotic obstructions or iliac vein compression, has gained increasing interest during the past couple of years.1–4 First, patients could only be treated with stents developed for the arterial system. However, the underlying pathology to treat patients with arterial problems differs tremendously from patients with deep venous obstructions. 5 The arteries differ in haemodynamics and show more shear stress, smaller vessel diameters and mainly need to overcome the negative effects of atherosclerotic plaques.6–8 On the contrary, venous pathology mainly needs to focus on overcoming high inward forces due to arterial counter pressure and post-thrombotic scarring of the vessel wall. 9 For this reason, it is likely that stents developed for arterial pathology are not ideal for the venous system. Even so, these stents show post-intervention complications like kinking or fracturing which can result in loss of patency.10,11 Due to this stent-related reduction of patency there was need for the development of dedicated venous stents.
These dedicated venous stents show favourable features like larger diameters, higher radial force, higher crush resistance and higher flexibility. Because there is low shear stress in the venous system, intimal hyperplasia is less likely to develop and stents mainly need to prevent the occurrence of collapsing. The Sinus venous stent (Optimed, Ettlingen, Germany) is one of the available dedicated venous stents and has a segmental design with a high flexibility due to only two small connections between the closed cell designed segments. Additionally, the Zilver Vena stent (Cook, Bloomington, IN, USA) is available with an open cell design focussing on high flexibility. On the contrary, the Sinus XL, Sinus Obliquus (Optimed, Ettlingen, Germany) and Veniti VICI (VENITI Inc., St Louis, MO, USA) are available. These stents have a geometry focussing on a high radial force. Bench testing of all the mentioned stents shows the favourable physical properties of all those stents.
Previous research showed favourable outcomes in small, short-term follow-up groups with patency rates of 83% up to 10 months in a Sinus Obliquus cohort. 12 In our dedicated tertiary referral centre, a cohort of patients with deep venous obstruction have been treated with flexible venous stents. Currently, most subjects are stented with the Zilver Vena or Sinus Venous stent. Previous analysis showed very favourable outcomes for this Sinus Venous stent, with patency rates of 92–100% after 12 months. 13 Since there are multiple options in the selection of stent type, the question is which type has the best favourable outcome. A comparison between different types of dedicated venous stents has never been performed before. Moreover, one of the main questions is which characteristic is superior in the prevention of stent collapse.
Consequently, the aim of this research was to evaluate the patency and clinical outcomes in patients treated with more rigid stents compared to the more flexible stents.
Methods
This study focussed on the stent-related and clinical outcomes in flexible versus more rigid stents.
All patients, treated between March 2012 and July 2015, with uni- or bilateral placed stents were analysed. Patients with a deep venous thrombosis (DVT) less than 12 months before treatment were excluded as natural recanalization and clinical improvement might still occur. Even so, patients with a combination of multiple stent types were excluded to receive a homogeneous outcome.
Demographics and baseline characteristics like age, gender, coagulation disorders and history of DVT were collected. Before treatment, all subjects experienced complaints of oedema, pain or venous claudication interfering with daily activities.
Regarding these complaints, the Venous Clinical Severity Score (VCSS), Villalta score and venous claudication were analysed. Venous claudication was scored positive when patients experienced onset or worsening of pain during (mild) exercise, which subsided during rest, especially when sitting or lifting the leg.
Every patient had a thorough preoperative evaluation of the deep venous system by both duplex ultrasound (DUS) and magnetic resonance venography. By means of these imaging techniques, the extent and severity of post-thrombotic changes or venous compression could be analysed. Based on these images, in combination with a multiplane phlebography, iliac vein compression was considered as being positive, when the common iliac vein gave a lumen reduction of ≥50% in combination with visualized collaterals and clinical complaints. Flow division and intraluminal synechiae were considered as signs for post-thrombotic obstruction. When no post-thrombotic changes were found, patients were included in the iliac vein compression group (iliac vein compression syndrome).
Patients with post-thrombotic changes were subdivided into the percutaneous treated group (post-thrombotic syndrome) or the hybrid treated group (extended post-thrombotic syndrome). A thorough description of recanalization, stent technique and the allocation into subgroups has been described previously. 14 After the stent procedure, a cone beam CT or multiplane phlebography was performed to evaluate the stent configuration and the venous flow through the stented iliofemoral tract.
Stent type
In this paper, two subgroups were created based on the flexibility characteristics of the stents. The more rigid stents included the Sinus XL (Optimed, Ettlingen, Germany), Veniti VICI (VENITI Inc., St Louis, MO, USA) and the Sinus Obliquus (Optimed, Ettlingen, Germany).
Since the rigid stents were used in fewer patients, we searched for a matched control group treated with the Zilver Vena (Cook, Bloomington, IN, USA) or the Sinus Venous stents (Optimed, Ettlingen, Germany). The matching was based on age, gender, underlying pathology for treatment and number of deployed stents and resulted in inclusion of 102 subjects.
Postoperative regimen
After the interventional procedure, all patients received rivaroxaban or Coumadin therapy for a minimum of six months with a target INR range between 3 and 4. A full therapeutic dose of tinzaparin was administered after the intervention to bridge the period until target range was obtained. In general, the patients who were treated by a percutaneous procedure were discharged the next day. The majority of patients who were treated by a hybrid procedure could be discharged after 3–7 days. Before discharge, all subjects received a DUS to assess patency of the stents.
Subsequently, standardized follow-up was planned at two and six weeks, 3, 6 and 12 months after the intervention. During this follow-up, a DUS was performed to analyse stent patency and the occurrence of complications, no IVUS was used. Besides this, the clinical complaints were evaluated and expressed in the VCSS, Villalta score and presence or absence of venous claudication. The complications which were being scored included stenosis of the stent or vein segment distal or proximal to the stent (of any degree), occlusion of the stent, fracture of the stent, compression (of any degree), kinking, tapering or bad alignment between connected stents. Compression was scored as any indentation of the stent due to external compression, most notably caused by the right common iliac artery.
When the suspicion arose that fracture or kinking of the stent occurred, an abdominal X-ray was performed in three directions.
Statistics
Normality of statistical distributions was measured by the Shapiro–Wilk test. When performing a survival analysis, a log-rank test was used to investigate the differences in primary patency (PP), assisted patency and secondary patency (SP) between patients treated with flexible stents and patients treated with more rigid stents. PP was defined as having patent stents without an additional intervention during follow-up. Assisted primary patency (aPP) was defined as subjects needing an additional intervention because of a stenosis or near occlusion. Whenever occlusion occurred somewhere during the follow-up, this was taken into account in the SP group.
Chi square tests were used to compare the flexible stents with rigid stents with respect to the scored complications. A Fisher’s exact test was used whenever an expected count less than 5 was seen. A repeated measures analysis was performed for VCSS and Villalta scorings at baseline and 12 months post-treatment to obtain the clinical differences after treatment and the effect of treatment group. Repeated measures analysis was corrected for baseline measurements and patency. A regression analysis was performed using the difference of post-treatment with respect to pre-treatment scores of VCSS and Villalta to control for the effects of age and gender as well.
A significance level of 0.05 (two sided) was used. All data were analysed by IBM SPSS statistics v23.0 (IBM Corporation, Armonk, NY, USA).
Results
Between March 2012 and July 2015, 305 patients were treated for post-thrombotic changes or iliac vein compression syndrome. Of these patients, 54 received more rigid stents. Since three of them were lost to follow-up and did not have a 12-month post-procedure duplex control, these subjects were excluded. A matched control group of 51 patients with flexible venous stents were combined.
Table 1 shows the demographics of the included 102 subjects. There were no statistically significant differences in age, gender, number of stents or reason for treatment.
Demographics of included subjects.
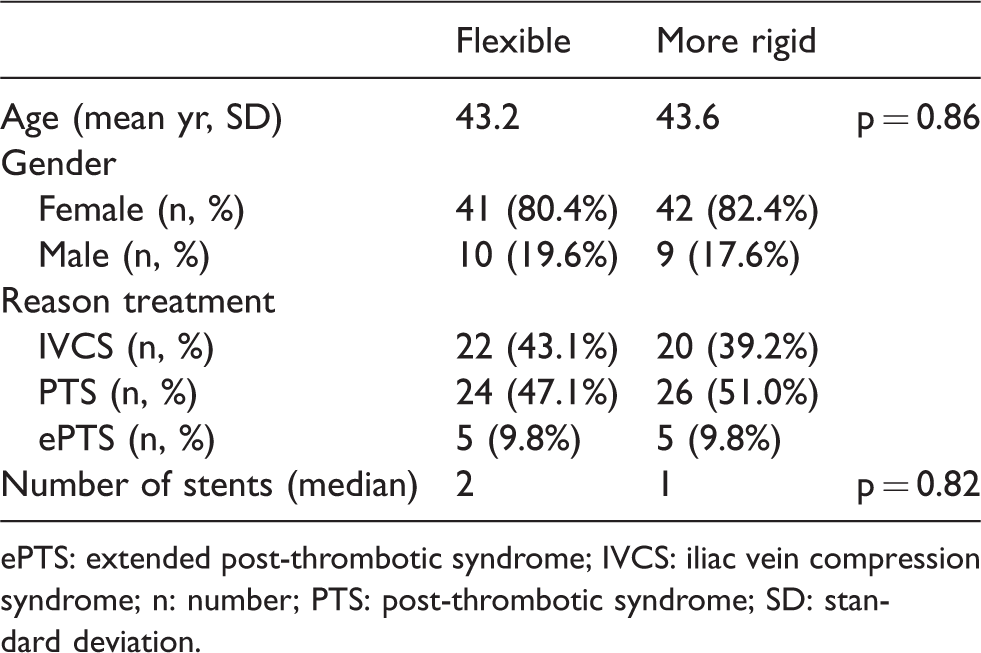
ePTS: extended post-thrombotic syndrome; IVCS: iliac vein compression syndrome; n: number; PTS: post-thrombotic syndrome; SD: standard deviation.
Clinical outcome
Before treatment, the VCSS, Villalta and venous claudication were scored. Since scoring of clinical data was performed at the grace of the consulting physician, these data were not available for all included subjects. Figures 1 and 2 show the differences between evaluated scores. All post-treatment scores were analysed 12 months after the first intervention.
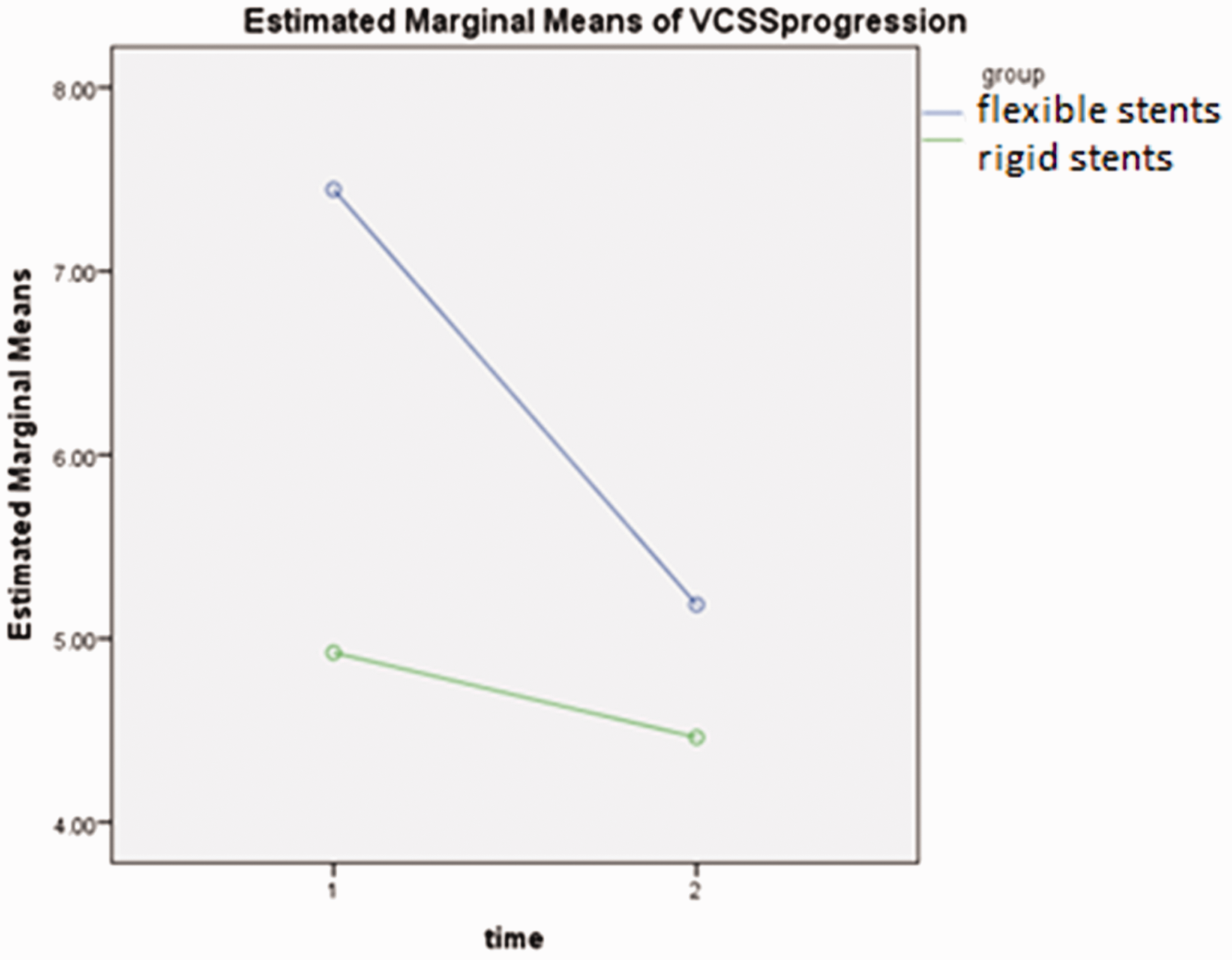
Estimated means of VCSS before and after treatment. VCSS pre- and post-stent treatment, F (1 by 38 df) = 6.89, p = 0.01 with a nonsignificant group effect of F (1 by 38 df) 3.007, p = 0.09. Based on N = 69.
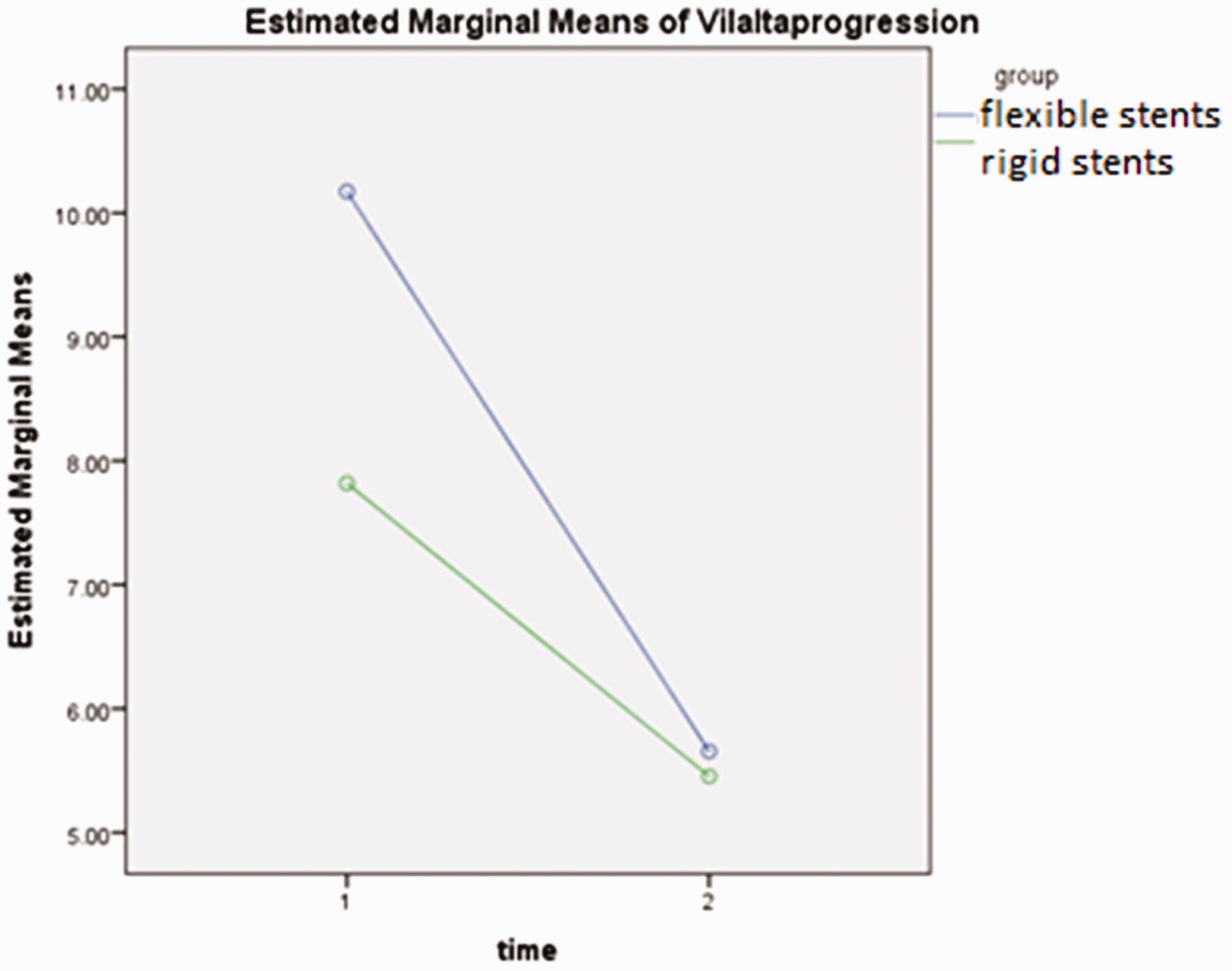
Estimated means of Villalta before and after treatment. Villalta score comparing pre- and post-treatment outcomes (F (1 by 38) = 12.18, p <0.01 with a nonsignificant group effect of F = 1.193 (1 by 38 df), p = 0.28. Based on N = 68.
A significant difference in VCSS was found with respect to pre- and post-stent treatment, F (1 by 38 df) = 6.89, p = 0.01 with a nonsignificant group effect of F (1 by 38 df) 3.007, p = 0.09 (Figure 1). The Villalta score was found to be significantly different as well comparing pre- and post-treatment outcomes F (1 by 38) = 12.18, p < 0.01 with a nonsignificant group effect of F = 1.193 (1 by 38 df), p = 0.28 (Figure 2).
Before treatment, 49 of 95 (48.0%) patients suffered venous claudication. After treatment, 9 out of 73 (8.8%) subjects stated that there were still complaints related to venous claudication. In the flexible stent group, VC was present in 63% of patients before treatment and 8% after treatment (p = <0.01). In the rigid group, VC was present in 33% of cases and 10% after treatment (p = 0.009).
After a period of 12 months, 34 (72.2%) patients in the more rigid stent group and 26 (55.3%) subject in the flexible stent group did use any kind of anticoagulation. This difference was not statistically significant (p = 0.09).
When analysing the stent-related complications, we noticed a statistically significant difference in the occurrence of tapering (0 versus 5, p = 0.03) and bad alignment between connecting stents (0 versus 5, p = 0.03). Table 2 shows the results of the stent-related complications based on DUS. The occlusion rate, stenosis rate, compression and kinking were not significantly different between the types of stents. A fracture of the stent could not be shown in any of the subjects.
Complications of stents.
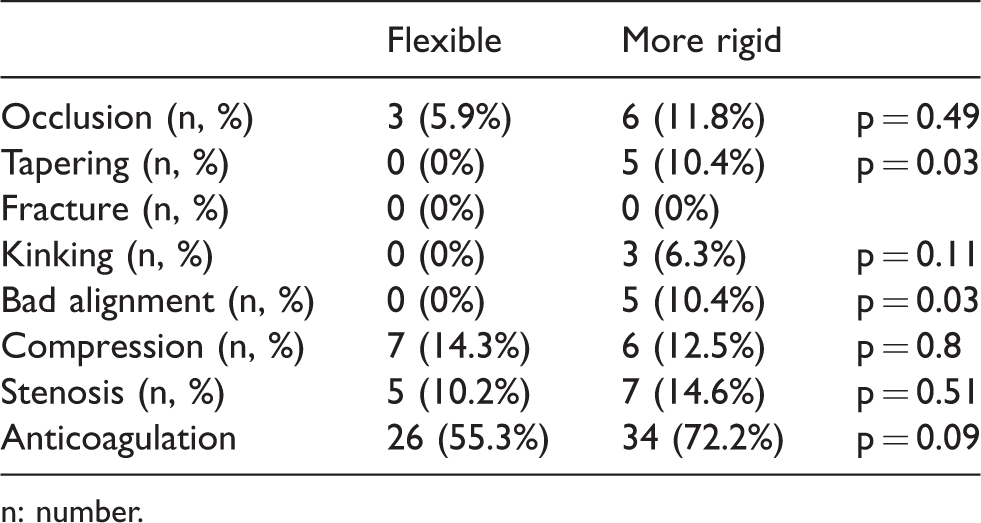
n: number.
Patency outcome
Figure 3 shows the PP rate of both groups. The more rigid stents showed a PP of 80%. In contrast to this result, the flexible stents showed a PP rate of 88% after 12 months (Figure 3(a)). The aPP of the rigid stents was 86% compared to 96% in the flexible group (Figure 3(b)). SP rates were 92 and 98%, respectively (Figure 3(c)).
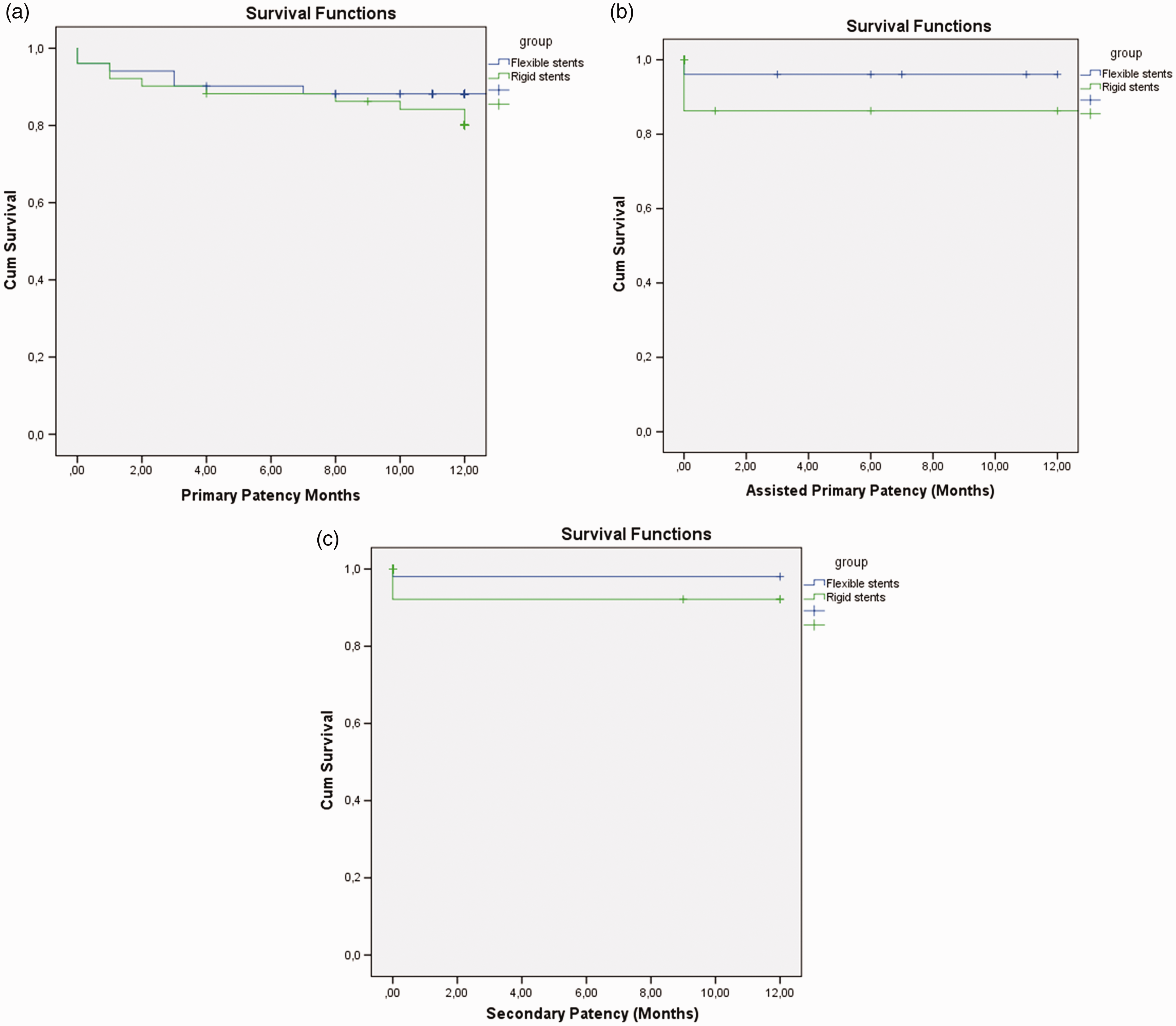
(a) PP of flexible (88%) versus rigid (80%) stents, (b) aPP of flexible (96%) versus rigid (86%) stents and (c) SP of flexible (98%) versus rigid (92%) stents.
Since the length of follow-up of patients in the more rigid stents was more extensive, the graphs were discarded after 12 months.
Discussion
This paper analysed the stent-related complications and clinical outcomes in multiple stent types in the venous system. The more rigid stents were compared to the flexible venous stents. Although the patency rates were not significantly different (PP 80% versus 88%, aPP 86% versus 96% and SP 92% versus 98%), some discrepancies have been found.
Due to a matched control group, it might be expected that the differences found are encountered due to stent-related issues. In order to analyse the number of stent-related complications, it was important to emphasize on the number of stents deployed. When deploying multiple stents, there is always a stent–stent overlap which is more prone to result in stent-related complications like bad alignment between connecting stents or stenosis. Since the number of stents was one of the criteria the matching was based on, this could not have been a statistically significant difference (p = 0.82). However, the number of tapering and bad alignment between connecting stents in the rigid stent group did show a statistically significant (p = 0.03) difference. Since the tapering or bad alignment could result in a new outflow obstruction, it might be expected that new interventions will be necessary. Consequently, the performance of these new interventions leads to loss of PP and accounts for higher numbers of subjects included in the aPP group. Moreover, the results of this article did show that complications like tapering or bad alignment resulted in differences in aPP.
On the other hand, the identified stent-related problems might prompt the physician to extend the anticoagulation more often. Ideally, a stent should be realigned with a new endothelial layer in several months, without stent material sticking into the lumen of the vein, necessitating prolonged anticoagulation to prevent thrombosis of the stents. Normally, when the stent is patent without any complication, the anticoagulation can be stopped after 3–6 months. After this period, the stent is likely covered by an endothelial layer. 11 However, when kinking or compression is present, the blood flow through the stent is altered and the use of anticoagulant medication is thought to be of more importance to overcome a stent occlusion. Surprisingly, no statistically significant difference in the use of anticoagulation therapy between both groups was found (p = 0.09). This could have been related to the small number of subjects analysed. Even so, the duration of follow-up could have been a confounding factor explained by the fact that complications like tapering can result in the continuation of anticoagulation in order to preclude stent occlusion. Moreover, when the blood flow through the stent is compromised, anticoagulation therapy can even be necessary lifelong. Analysis of the anti-thrombotic therapy use after multiple years should be performed in future research to exclude this overlapping period. Another possible explanation is the fact that the underlying number of DVTs was not taken into consideration. In the Dutch guidelines for prevention and treatment of thrombosis, it is stated that it should be considered to keep patients with a recurrent DVT on lifelong anticoagulation therapy. To notice, if these factors resulted in confounding, future research should take this into account as well.
Although not all analysed complications or scorings were statistically significant, we did notice some differences. The most important factor contributing to the decision which type of stents one should use is the clinical relevance of the identified stent-related complications. We did not find a clinically significant difference after one year between both groups. Therefore, future research should be performed to analyse this more thoroughly since this can contribute to anticoagulation-related complications.
Since this research has some limitations, a few recommendations for future research can be implicated. Like mentioned earlier, a large group of subjects with longer follow-up and a standardized anticoagulation regimen would be more ideal to investigate stent-related problems over time. Moreover, as DUS is a subjective and investigator-dependant imaging technique which results in a 2D perspective it hinders accurate and reproductive imaging. Ideally, a 3D image would be more appropriate to take notice of the stent-related complications. Imaging modalities like computed tomography, phlebography or even abdominal X-rays are recommended to analyse the 3D results in prospective trials. At last we should mention that there could have been a learning curve bias which could have led to some differences in outcome as the most flexible stents were used in a later stage.
Conclusion
Dedicated venous stents show good patency outcomes and clinical results. Tapering and bad alignment between connecting stents in the venous system are more frequently seen in more rigid stents. Future research should indicate if these results significantly influence clinical outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CHA Wittens received consultancy fees from Angiocare, Medi, OptiMed, Vascular Insights, IQ, Brand Group, and research funds: BTG, OptiMed, Olympus, Bayer, AB medica, Angiocare, Philips, Cook, Boston Scientific.
Ethical approval
This research was approved by the ethical committee of the Maastricht University Medical Center METC 16-4-225.
Guarantor
N/A.
Contributorship
TMAJV: study design, data collection, data analysis, writing; MAFW: data collection, critical review in writing; CHAW: study design, data collection, critical review data analysis in writing.
Acknowledgements
N/A