
Abstract
Objectives
This study assessed the effectiveness and patient experience of the ClariVein® endovenous occlusion catheter for varicose veins from a large single-centre series in the UK.
Methods
A total of 300 patients (371 legs) underwent ClariVein® treatment for their varicose veins; 184 for great saphenous vein (GSV) incompetence, 62 bilateral GSV, 23 short saphenous vein (SSV), 6 bilateral SSV and 25 combined unilateral great saphenous vein and SSV. Patients were reviewed at an interval of two months post procedure and underwent Duplex ultrasound assessment. Postoperative complications were recorded along with patient satisfaction.
Results
All 393 procedures were completed successfully under local anaesthetic. Complete occlusion of the treated vein was initially achieved in all the patients, but at eight weeks’ follow-up, there was only partial obliteration in 13/393 (3.3%) veins. These were all successfully treated with ultrasound-guided foam sclerotherapy. Procedures were well tolerated with a mean pain score of 0.8 (0–10). No significant complications were reported.
Conclusions
ClariVein® can be used to ablate long and short saphenous varicose veins on a walk-in–walk-out basis. Bilateral procedures can be successfully performed, and these are well tolerated as can multiple veins in the same leg. Early results are promising but further evaluation and longer term follow-up are required.
Introduction
Minimally invasive endovenous techniques such as ultrasound-guided foam sclerotherapy (USGFS), radiofrequency ablation (RFA) and endovenous laser therapy (EVLT) have revolutionized the management of primary varicose veins in the UK. Compared with conventional surgery (high ligation, stripping and phlebectomies), the number of endovenous operations performed has escalated during the past decade in the UK with doubling of procedures between the period of 2007 and 2008 alone. 1 These methods have been enthusiastically adopted because of the proposed benefits including fewer complications, quicker return to work, improved QoL scores, reduced need for postoperative analgesia and improved cosmetic outcome. Furthermore, the National Institute of Clinical Excellence (NICE) 2013 guidelines recommends the use of endovenous thermal ablation techniques (RFA and EVLA) as first-line treatment for truncal vein reflux. 2
A recent systemic review and meta-analysis of randomized clinical trials showed that although USGFS seemed inferior to surgery, primary failure and recurrence rates with RFA and EVLT were comparable to surgery but with the added bonus of reduced complications such as wound infection, haematoma and shorter return to work. 3
Tumescent anaesthesia is currently required for both types of endothermal ablation technique and carries the risk, albeit rare, of thermal-related complications such as neuralgia, skin burn and prolonged pain.4,5 The insertion of tumescence itself can also be painful and cause complications.
The ClariVein® occlusion catheter system (Vascular Insights, Madison, CT, USA) is a relatively new minimally invasive approach to induce closure by a combination of endovenous mechanical damage to the endothelial cells and chemical injury with a liquid sclerosant infusion. It has the advantage of eliminating the need for tumescent anaesthesia and the risks of heat-related injury to the surrounding tissue and structures (no heat is used). It has been shown to be safe and efficacious in its initial trials6,7 not only for the great saphenous vein (GSV) but also for the short saphenous vein (SSV).8,9 Procedure times and intra/postprocedural pain scores have been shown to be significantly better than for RFA and EVLA.10,11
This study assessed the effectiveness and patient experience of this new endovenous treatment not only to target incompetent GSV but also SSV and bilateral procedures and multiple veins, from a high-volume centre in the UK.
Methods
Study design
A set protocol was constructed and adhered to in order to evaluate endovenous mechanochemical ablation (MOCA) with the patented single-use, disposable ClariVein® system at a single private hospital in East Anglia, UK. Ethical approval was gained from the internal hospital board, and data were collected prospectively onto a secure computer database.
Patients were either fee-paying individuals or held private health insurance. They underwent examination and duplex ultrasound evaluation by one consultant vascular surgeon with a large endovenous experience. The assessment included evaluation of GSV/SSV reflux, clinical, aetiological, anatomical and pathophysiological elements (CEAP) classification 12 and previous venous procedures. The study period was from January 2011 to January 2015.
Reflux was determined at the saphenofemoral (SF)/saphenopopliteal (SP) junction in the lying and standing position using the Valsalva manoeuvre or manual distal compression with rapid release, respectively. Reflux as documented by ultrasound was defined and considered significant as retrograde flow of > 0.5 s.
Inclusion criteria were:
Age >18 years old. C2–C6 varicose veins (CEAP Class 1 patients were excluded). Primary GSV or SSV incompetence. Patients who had GSV/SSV diameters of 3 mm to 12 mm in the lying position.
Patients were consented for ClariVein® being a new technique under study and that they were participating in this study. All the patients received a procedure-specific information leaflet, which explained the technique including risks and side-effects as well as a description of alternative techniques.
Patients were excluded from having this procedure if they were pregnant, lactating, allergic to sclerosant, had previous truncal varicose vein treatment, peripheral arterial disease (ABPI < 0.8), history of deep venous thrombosis, previous thrombophlebitis, which have recanalized and were incompetent, anticoagulation with warfarin and if their GSV/SSV were severely tortuous. Patients who did not want to be treated with ClariVein® were routinely offered treatment with EVLA. A total of 1052 patients opted for EVLA in the same time period.
ClariVein® technique
The ClariVein® catheter has been previously described.
6
In brief, it combines two methods of action:
Mechanical agitation of the vessel endothelia by a rotating catheter tip. A sclerosant drug sprayed from the tip of the catheter as it is withdrawn to ensure maximal effect.
All procedures were performed under local anaesthetic consisting of ultrasound-guided above knee saphenous nerve block (20 ml Xylocaine, bupivacaine mixture) supplemented with further local injections to avulsion sites (administered prior to prepping and draping) by a single surgeon (MEG). The saphenous nerve block used was an ultrasound-guided above knee subsartorial nerve block inserted just above knee level where the saphenous nerve leaves the femoral artery and vein to pass underneath the sartorius muscle to become superficial next to the GSV at the knee level. Therefore, the saphenous nerve block only anaesthetises from the knee down to enable lower medial leg phlebectomies to be performed painlessly. It does not anaesthetise the thigh where GSV MOCA is performed nor does it anaesthetise the posterior calf when the SSV MOCA was performed.
No tumescent anaesthesia, sedation or antibiotics were required. All the patients were positioned supine with the leg slightly flexed and abducted to enhance access to both the GSV and the SSV. This position was particularly advantageous for combined GSV/SSV procedures.
A Seldinger technique was used to introduce a short micropuncture 5Fr introducer sheath into either the GSV or SSV under ultrasound guidance and flushed with saline. The phlebectomies were performed first under saphenous block and the wounds closed with tissue glue. The ClariVein infusion catheter tip was inserted through the sheath and the tip of the dispersion wire positioned 10 mm distal to the SFJ or SPJ. The sheath was withdrawn to just beyond the puncture site so as to prevent activation of the probe within the sheath. Wire rotation was activated for a few seconds to induce spasm of the proximal vein. With the wire continuing to rotate, infusion of the sclerosant was started simultaneously with catheter pullback. The activated catheter, which is connected to a 9 V battery-motorized handle, was steadily withdrawn at 1 cm every 7 to 10 s. The sclerosant used was 2.0% liquid sodium tetradecyl sulphate (STD). The sclerosant volume used was determined by vein diameter and treatment length. The sclerosant was delivered using the approved method of compressing the syringe attached to the handle, which conveys the sclerosant to the end of the catheter just proximal to the rotating angulated wire. The volume of sclerosant used was not predetermined but adjusted on a case-by-case basis by continuous duplex monitoring of the mechanical and chemical effect to ensure spasm and collapse of the vein, while not exceeding the safe dose of sclerosant. Generally, 0.1 ml–0.2 ml of sclerosant is injected every 1 cm pullback on the catheter.
Vein diameter was determined by duplex ultrasound measurement from the widest part of the treated vein in the supine position excluding the first 2 cm of vein and any localized venous blowouts. Treatment length was calculated from the graduated markings on the catheter.
A completion duplex ultrasound was performed after the procedure to confirm the patency of the common femoral vein and the deep venous system. The time taken to complete the procedure was noted. Subcutaneous heparin was not routinely given before or after the procedure.
A full length compression stocking was applied to the treated limb(s) from the foot to the groin followed by Cestra™ compression bandages over the stocking. The compression stocking used was Struva 23™ – 23 mmHg graduated pressure from ankle to upper thigh. The Cestra™ bandages were applied over the stocking to provide extra support, haemostasis and absorbance of any bleeding and allow the patient to undertake immediate exercise consisting of a 15-min walk and then rest in the waiting room for another 15 min. The patient was then checked by a nurse and allowed home with instructions to undertake at least a 15-min walk twice a day for one week. Bandages were removed by the patient at three days postprocedure and compression stockings removed at three weeks. The patients were instructed to take paracetamol and/or ibuprofen medication for discomfort if needed.
Outcome and follow-up
Patients were asked to document the level of peri and postprocedural pain endured on a 100 mm visual analogue scale. A follow-up visit at two months was arranged and an ultrasound study and clinical exam were performed. Postop duplex includes colour and spectral Doppler in addition to B-mode. Colour duplex scan was performed scanning the full length of the treated vein testing for compressibility and reflux. A successfully obliterated vein was solid with no visible lumen and could not be compressed, and there was no flow on colour duplex and Valsalva. A partially obliterated vein still had a partial lumen, which could be compressed; Doppler showed some flow but not necessarily reflux on Valsalva. Some of these veins had an unsealed mid-section usually without reflux, those with an unsealed proximal section extending to a patent SFJ usually did show reflux. Unsealed mid-sections often sealed spontaneously unless there was a large tributary feeding into it, unsealed proximal LSV always needed UGFS.
Occlusion and vein wall changes were documented along with the patient completing a 10-point scale satisfaction score (10 being most satisfied).
Statistical analysis
Continuous variables are reported as mean and standard deviation and categorical variables as absolute number and percent, unless stated otherwise. Continuous data were compared using the Student t test or Mann-Whitney U test for parametric and non-parametric data, respectively. Categorical data were compared using the Chi-square or Fisher exact tests. Statistical significance was assumed at p < 0.05. The statistical analyses were performed using Statsdirect 2.7.8 (Statsdirect Ltd, Altrincham, UK).
Results
Based on the above protocol, the study included 300 consecutive patients of which 207 were females (69%). The mean age was 58 ± 13 years. They were treated between 1 January 2011 and 31 January 2015. All were diagnosed with either unilateral or bilateral symptomatic GSV/SSV incompetence or a combination of unilateral GSV and SSV incompetence.;184 (61%) were treated for GSV incompetence alone, 62 (21%) for bilateral GSV, 23 (8%) SSV, 6 (2%) bilateral SSV and 25 (8%) combined unilateral GSV and SSV (see Figure 1). There were 393 sets of GSV/SSV treated in 371 legs. All the patients had concomitant phlebectomies. The CEAP classification (C2:C3:C4:C5–C6) for this group was 209:129:25:8, respectively. All treated veins showed occlusion on ultrasonography immediately after ClariVein® treatment. No major adverse events were observed, i.e. no deep vein thrombosis (DVT), nerve injury, skin necrosis, infection or pigmentation. Transient superficial phlebitis was noted in 13/300 (4%) patients, the majority of these (8/12) came from those who had a unilateral GSV procedure (see Figure 2). One bilateral GSV patient experienced phlebitis on both legs. Phlebitis was treated with a course of anti-inflammatories, and these patients did not need to attend further for follow-up.
ClariVein® procedures performed. ClariVein® outcome by complication and occlusion rate.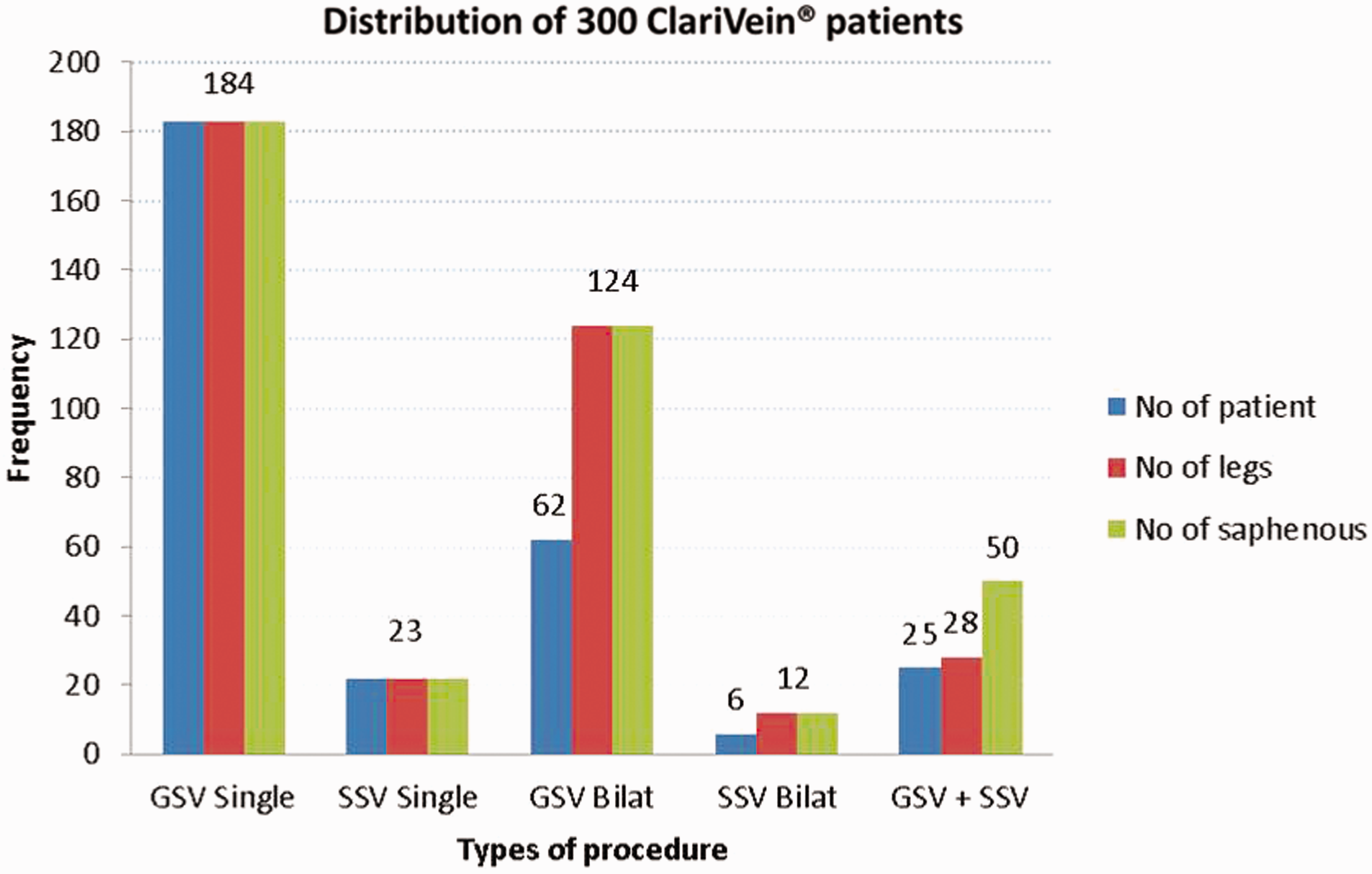
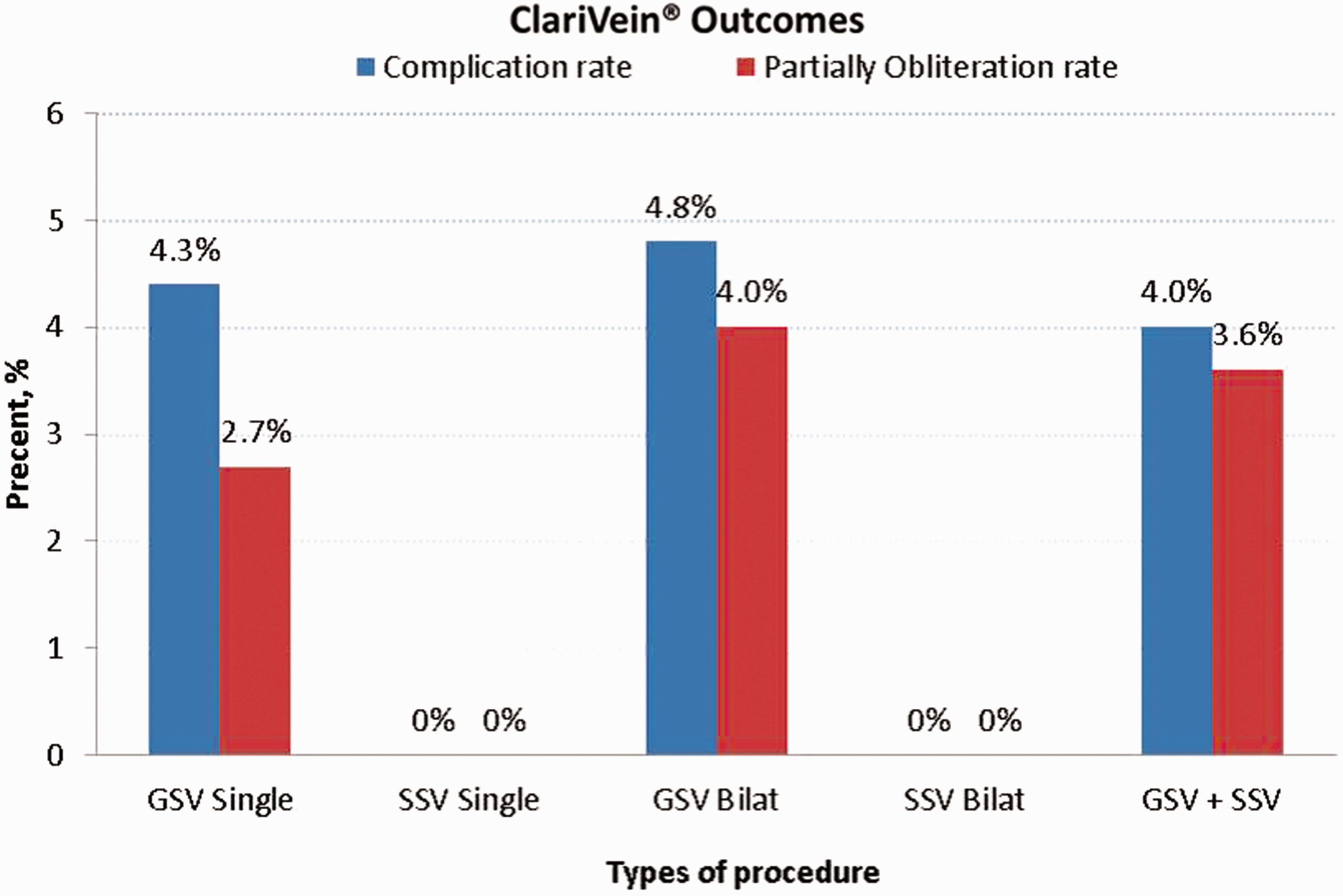
The complication rate per patient had no significant association (p > 0.05) between unilateral (9/207, 4.3%) and bilateral or combined GSV/SSV (4/93, 4.3%). There was also no difference in the complication rate between ablating the GSV (12/333; 3.6%) compared to SSV (2/60; 3.3%). Most of the phlebitis was noted along the line of the treated GSV rather than its tributaries. In all the cases, this was mild and self-limiting and responded to several days of over the counter paracetamol and non-steroidal anti-inflammatory tablets (ibuprofen).
The mean length of GSV obliterated was 40.0 ± 10.3 cm compared to 21.7 ± 7.3 cm for a SSV (mean difference = 18.3 cm, 95% CI 16.0 to 20.6 cm, p < 0.001). A mean volume of 7.6 ± 2.1 ml of sclerosant was used per GSV treated and 4.0 ± 1.5 ml per SSV treated (mean difference = 3.7 cm, 95% CI 3.2 to 4.1 cm, p < 0.001). The mean volume used in a bilateral GSV procedure was 13.3 ± 2.4 ml, bilateral SSV procedure was 7.8 ± 2.4 ml and combined unilateral GSV and SSV was 10.6 ± 2.2 ml (p < 0.001). The average diameter of GSV and SSV treated was 6.4 ± 1.4 mm and 5.0 ± 0.9 mm, respectively (mean difference = 1.3 mm, 95% CI 1.1 to 1.6 mm, p < 0.001).
Mean procedural time for a unilateral ablation was 27 ± 6.2 min and a bilateral procedure 39 ± 5.5 min, both included the phlebectomies.
At eight weeks’ follow-up, the GSV was completely occluded in 322/333 (97%) veins and SSV completely closed in 60/60 (100%) veins. The 11 target veins that were partially sealed were completely obliterated with one course of UGFS at this follow-up visit with no complications. No additional complications were observed either clinically or detected with duplex ultrasonography. Eight of 11 (73%) GSVs that had recanalized were noted to have done so within the first 8 cm from the SFJ. There was no relationship between the initial diameter of the veins and recanalization at two months.
All procedures were very well tolerated with a mean pain score of 0.8 (range 0–3) on a 10-point scale, documented immediately afterwards. In fact, 269 (90%) patients did not report any pain immediately after treatment was finished.
Bilateral procedures had similar immediate pain scores to those who had unilateral procedures. After six weeks, median patient satisfaction of the treatment was 9 (IQR 9–10).
Discussion
This study is the largest UK single experience to date with the ClariVein® occlusion catheter system. Three previous studies4,7,13 limited the ClariVein® catheter to GSV incompetence. The first results was described in 29 patients (30 GSVs) and resulted in occlusion rates of nearly 97% after eight months, with minimal periprocedural complications. 4 This was followed up with a study from the Netherlands which reported an initial technical success rate of 100% in 25 patients (30 GSVs) but dropped to 87% complete occlusion at six weeks. 7 This may have been down to the use of a weaker sclerosant solution (1.5% versus 2.0%) and the shorter follow-up interval.
The third paper mentioned above describes data from the same Dutch group mainly comparing perioperative pain and early QoL scores after RFA and MOCA. 13 The group do not mention whether this is the same group of patients from their initial study, and there is no documentation of venous seal rate. The first prospective observational multicentre report on the efficacy of MOCA in selected patients with lower extremity chronic venous disease was described by Bishawi et al. 14 The population (126 patients) in this report was significantly older, and the BMI was higher compared to published studies using endothermal techniques. Again, the procedure was limited to the GSV and reported high occlusion rates at one week, three and six months (100%, 98% and 94%, respectively), comparable to the endothermal procedures in spite of the older population and the higher BMI. There was significant clinical improvement after treatment as shown by the marked reduction in the CEAP class and the VCSS.
Our results are comparable (initial occlusion rate 100% with 94% completely sealed at eight weeks’ follow-up) but differs that it includes treatment of both incompetent GSV and SSV, bilateral and multiple vein procedures.
It is important to note that the number of truncal veins treated at one sitting or the type of vein treated (GSV or SSV) had no association with developing a complication, although the incidence of this was low and may represent a type II error.
All patients were done as day-case procedures on an intention to treat basis and none had to be admitted as inpatients, which suggest this form of endovenous ablation can be safely performed for bilateral procedures and treatment of more than one vein in the same leg on a walk-in–walk-out basis. Furthermore, it seems an ideal form of treatment for SSV incompetence, where the sural nerve can be very close to the SSV and run the risk of thermal injury during RFA/EVLA. It can also be combined with phlebectomies during the same procedure under local anaesthetic. This is in keeping with a recent study showing that MOCA was a safe, feasible and efficacious technique for treatment of SSV insufficiency. One-year follow-up shows a 94% anatomic success rate and no major complications. 8
Transient phlebitis was the only common minor complication to have been noted (4%) – patients should be warned about the risk of phlebitis in advance, especially if the truncal vein is very superficial and advised of the measures to treat it, i.e. compression and NSAIDs. This is a low-incidence rate comparable to previous studies with MOCA and RFA and lower than if foam or liquid sclerotherapy were used.9,15,16 A lower incidence of superficial phlebitis following MOCA may be due to less energy required to seal the vein with ClariVein® compared to endothermal methods. Less trauma or perforations of the vein may also play a role in this aspect.
There were no major adverse events; specifically no DVT was encountered, even without prophylactic low-molecular weight heparin being used. We believe that combined compression with stocking, bandage and immediate exercise are important to prevent periprocedural DVT. With no adverse events, our findings based up to two months of follow-up suggest that the ClariVein® procedure is safe not only for GSV ablation but also for bilateral cases, multiple veins in the same leg and for SSV incompetence.
The justification of using 2% rather than 1.5% STD was that each STD solution also contains other chemicals to stabilize the STD to maintain its effectiveness. Dilution of 3% with saline may potentially dilute these stabilisers and may reduce the effectiveness of the STD. Dilution of the 3% STD with 1% STD (50:50) maintains the same concentration of stabilisers, maintains the pH at 7.9 and helps maintain the stability of the solution. Currently, there is no consensus on what strength of STD is ideal for MOCA. When adhering to safe-dosage levels, sclerosants with higher concentrations potentially limit the extent of treatment especially for multiple veins ablated at the same sitting. Currently, there is a RCT being performed looking at the ideal Polidocanol (Aethoxysklerol®, Kreussler Pharma, Wiesbaden, Germany) liquid dosage for ClariVein®, although preliminary results suggest that if the sclerosant is used in a microfoam format, this has proved less effective in ablating the truncal vein. 17
The recommended maximum single treatment dose of STD should not exceed 10 ml of 3% strength (30 mg/ml STD product sheets). A 10 ml treatment with 3% STD delivers a total dose of 300 mg. An equivalent dose of 2% STD would enable 15 ml to be used. We have shown that it is safe to utilize up to this dose of 2% STD for multiple veins and enable bilateral procedures to be performed. Although we would not recommend exceeding this dose, data from Australia have suggested that even higher doses of up to 15 ml of 3% STD – used to treat larger diameter varicose veins – have no apparent adverse effects. 18 Convenience should not be ignored when a new technology is assessed. Elimination of injecting tumescence may save time. We report a mean 27-min and 39-min treatment times for a unilateral and bilateral procedure (either GSV or SSV), respectively (including phlebectomies). In comparison, a single GSV treatment (approximately 40 cm) with EVLT combined with phlebectomies takes around 35 min 19 nearly as long for a bilateral MOCA procedure described in this series.
The satisfaction score at eight weeks is high and very few patients complained of pain immediately postprocedure. This did not matter whether it was a unilateral or bilateral ablation. van Eekeren et al. 7 showed similar degree of patient satisfaction and very low pain scores in their pioneering MOCA manuscript. 7 Reasons for these include, MOCA is performed without tumescent anaesthesia, and there is no potential risk of thermal-related injuries to surrounding nerves or tissues. On the other hand, scaling back on the anaesthesia (no tumescence) introduces a risk to the heart of minimally invasive treatment namely periprocedural or postoperative pain. This was not borne out in this study, and the level of pain experienced was lower than that experienced after EVLT and RFA, although these procedures were performed at the time under general anaesthetic and not using modern day local anaesthetic techniques. 20 The benefit though may well be the elimination of pain caused by insertion of the tumescence itself, which is known to be higher than during the treatment. 21 Recent QoL studies showed that MOCA is associated with significantly less postoperative pain, faster recovery and earlier work resumption compared with RFA.11,13
Limitations of the study include the fact that this is a single surgeon’s experience with no independent assessment of success and no element of control albeit large and varied, with a limited follow-up period (two months). Randomized trials with a prolonged follow-up protocol are clearly indicated to compare closure rates directly with other endovenous modalities including catheter-directed foam sclerotherapy, especially as most recanalizations with other techniques will occur during the first year after treatment. These trials should look at other aspects such as cost savings associated with the use of the ClariVein® device, which are not yet reported but will definitely play an important role in acceptance of this new technology as a treatment option especially in the current economic downturn. There is no hardware to buy and upkeep and the technique can be performed on an outpatient basis, thereby reducing overhead and procedural costs.
The MARADONA trial 22 (Mechanochemical endovenous Ablation versus RADiOfrequeNcy Ablation in the treatment of primary GSV incompetence) has been designed to directly compare the anatomical and clinical success rate at one year compared to RFA and is hoping to recruit 230 patients in each group (460 patients in total). The MESSI Trial will look at similar endpoints for the SSV. 23
Conclusions
The ClariVein® device is safe and efficacious to ablate long and short saphenous varicose veins on a walk-in–walk-out basis. The procedure can be expanded to bilateral procedures and multiple veins in the same leg, which are well tolerated. There is a high satisfaction rate, and periprocedural pain is low. Early results are promising, but further evaluation and longer term follow-up are required in the form of randomized controlled and cost-effectiveness studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vascular Insights provided MEG with initial training in the ClariVein® technique.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.