
Abstract
Objective:
The possible benefits of endovenous saphenous ablation (EVSA) as initial treatment in patients presenting with isolated superficial-vein thrombosis (SVT) and saphenous vein reflux include: (1) definitive treatment of the underlying pathology and (2) elimination of the saphenous vein as a path for pulmonary emboli, which (3) may eliminate the need for anticoagulation.
Methods:
In a ten-year review of 115 limbs presenting with acute isolated SVT, 72 limbs (71 patients) with saphenous reflux were given a choice of two treatments following an explanation of the risks and benefits of each. Group I limbs (n = 41) were treated with office EVSA using radiofrequency or laser with or without thrombophlebectomy if performed within 45 days of diagnosis. Post-treatment anticoagulants were not given. Group II limbs (n = 31) were treated with compression hose and repeat Duplex within one week, with added anticoagulants if SVT extended into the thigh.
Results:
In group I, mean interval from diagnosis to treatment was 13.7 days. One calf deep vein thrombosis was noted. In group II no complications were noted. In late follow-up of group II patients, 12/29 underwent EVSA more than 45 days after initial presentation.
Conclusions:
The safety and efficacy of EVSA and thrombophlebectomy appear indistinguishable from conservative measures and may be offered as initial treatment to patients presenting with SVT and saphenous reflux.
Introduction
Lower extremity superficial-vein thrombosis (SVT) has traditionally been considered a benign condition, but recent studies reveal an appreciable incidence of concomitant deep vein thrombosis (DVT) and nonfatal pulmonary embolism (PE) (collectively, venous thromboembolism (VTE)), requiring anticoagulation.1–4 Less well established is the most effective and cost-beneficial treatment of acute SVT isolated to the superficial venous system. No consensus has emerged despite a number of medical and surgical treatment algorithms and numerous randomized controlled trials (RCTs). 5
One subgroup that might benefit from an alternate approach is patients who have associated reflux in a saphenous vein. Saphenous stripping and great saphenous ligation at the saphenofemoral junction were widely practiced at one time. An RCT comprising only SVT patients with thrombosed varicose veins (VV) and venous reflux compared multiple medical and surgical regimens and showed that stripping resulted in the lowest incidence of thrombus extension and treatment costs. 6 Endovenous saphenous ablation (EVSA) achieves the same goal as stripping, but only one report of three individuals undergoing EVSA for SVT and saphenous reflux has been published to date. 7 The possible benefits of EVSA compared to medical treatment in such patients include: (1) definitive treatment of the underlying pathology and (2) elimination of the saphenous vein as a path for PE, which (3) may eliminate the need for anticoagulation. Concurrent thrombophlebectomy may further relieve pain, accelerate return to full function, and eliminate the need for prolonged compression hose.
Likewise, no study has reported how often patients choose to undergo treatment of saphenous reflux and VV with stripping or EVSA after initial conservative treatment for SVT. Treatment in two stages confounds traditional cost-benefit analysis by neglecting the later expense of treating the underlying pathology.
The goal of this report is to document the previously unreported prevalence of saphenous reflux in a larger series of patients presenting with SVT, assess whether prompt EVSA and thrombophlebectomy is a safe and effective option for treating them, and document the incidence of late EVSA in patients initially receiving medical treatment.
Patients and methods
The charts of all patients in a solo private phlebology practice presenting with acute isolated SVT over a 10-year period (1 June 2002 to 31 August 2012) were reviewed. Individuals with concurrent VTE or whose SVT was attributable to sclerotherapy or EVSA were excluded from further analysis. All patients underwent Duplex ultrasound to rule out DVT, confirm the extent of SVT, and determine the presence of saphenous vein reflux of greater than 0.5 s. Patients were considered to have SVT if thrombus length was ≥3 cm involving surface veins and/or a saphenous vein. Thrombosed varices were considered to be in the distribution of a refluxing saphenous vein if reflux could be traced in a continuous path from the refluxing saphenous vein through superficial varices to the most proximal point of the thrombosed varices. The report further analyzes the subgroup of patients who had at least 6 cm of non-thrombosed refluxing distal (central) saphenous vein amenable to heat ablation and either (1) thrombosed varices in the distribution of a refluxing saphenous vein or (2) SVT involving the saphenous vein. The risks and benefits of (1) definitive treatment, consisting of EVSA with or without thrombophlebectomy, versus (2) conservative measures were discussed with each patient, who could then choose how to proceed. Patients with saphenous reflux and systemic malignancy or who were pregnant in the third trimester were excluded.
Since one goal of the study was to compare the possible risks and benefits of prompt intervention versus conservative treatment, the 45-day period after consultation was defined as the treatment interval within which intervention might have some bearing on the patient’s clinical outcome (i.e. treatment before 45 days would reduce the time an individual needed to take anticoagulants if a policy of universal anticoagulation were in effect). This interval was selected arbitrarily after the review was completed to reflect the similarly defined treatment interval in the recent CALISTO study. 8 Patients who underwent EVSA during the treatment interval were assigned to group I. Patients who selected conservative treatment or who underwent EVSA after 45 days were assigned to group II.
Technique
All procedures were done in the office under tumescent local anesthesia (0.12% Lidocaine without epinephrine) and occasional oral sedation (Ativan 1–2 mg sublingual). EVSA of saphenous vein was achieved using radiofrequency (Closure, ClosurePLUS or ClosureFAST catheter) or laser (940 nM or 1470 nM). If the saphenous vein was partially thrombosed, EVSA was performed only in the thrombus-free segment of saphenous vein central to the thrombus (6 cm minimum). The guide wire was never passed through thrombus. Most EVSA patients also underwent thrombophlebectomy. Anesthesia of thrombosed varices with tumescent anesthesia was readily achieved by thoroughly infiltrating skin tissues deep to and surrounding the veins before anesthetizing the subdermal tissues immediately superficial to them. Ultrasound was used as needed to guide needle placement for tumescent anesthesia, select the optimal incision site for evacuating thrombus, visualize the placement of a small mosquito clamp directly into the thrombosed vein for the purpose of mobilizing tenacious thrombus, and identify large perforators that were potential conduits for unintentionally impelling thrombus into the deep system when superficial thrombus was extracted by gently squeezing surrounding tissues. Once thrombus was extracted, the affected variceal vein itself could usually be avulsed with the aid of a Mueller hook. Incisions were placed to debulk as much thrombus as possible and remove both involved and uninvolved VV. Patients were encouraged to remain active and wear 20–30 mm graduated strength support hose for five days. Post-treatment anticoagulants were not given, and oxycodone tablets (Vicodin 5/500) were given only on request. Patients were usually followed for three months post-treatment, except those who had symptomatic complications or who underwent elective cosmetic sclerotherapy.
Treatment of group II patients generally comprised unrestricted activity, 20–30 mm Hg compression hose for three months, and anti-inflammatory and pain medication as needed. The author’s usual recommendation was to recommend three months anticoagulation with warfarin only if saphenous vein thrombus extended into the thigh or if thrombosed thigh varices were within 2–3 cm of the saphenous vein. The specific anticoagulant (LMWH or warfarin) and duration of its use, however, were usually determined by the referring physician, who often did not follow these guidelines. All patients underwent a follow-up ultrasound study one to two weeks after the initial visit to identify possible thrombus extension. Patients who did not undergo EVSA by the author either in the treatment interval or in the follow-up period through August 2012 were surveyed by letter and telephone to determine whether they later experienced recurrent SVT or other complication of chronic venous insufficiency (CVI), and/or whether they underwent EVSA elsewhere.
The demographics, major co-morbidities, venous history and findings on initial examination, initial treatment, and efficacy outcomes were recorded for groups I and II. The primary efficacy outcomes were death, symptomatic DVT or PE, or significant bleeding in the immediate follow-up period. Since CEAP and VCSS scores were not designed to evaluate acute venous disease, secondary outcome measures, such as pain relief the number of days support hose were worn, were evaluated either subjectively or not at all. The need for re-treatment of the saphenous vein due to saphenous recanalization was recorded, as was the incidence of and reason for EVSA in group II patients after the 45-day treatment interval. Continuous variables were expressed as mean ± SD and compared with the Student’s t test for independent variables. Categoric variables were compared with the Fisher’s exact test or χ 2 . A Kaplan–Meier curve was used to estimate cumulative EVSA (%) in the aggregate of group I and II limbs. A significance level of .05 was assumed for all tests. Statistical analyses were performed using MedCalc for Windows, version 12.3.0.0 (MedCalc Software, Mariakerke, Belgium).
Results
Acute isolated SVT was identified in 115 limbs in 110 individuals (4.5% bilateral). Of these, 76 (66.8%) had reflux in a saphenous vein [great saphenous vein (70), small saphenous vein (4) anterior accessory saphenous vein ≥ 4 mm (2)], all of whose CVI was classified as C2–5. Within the 45-day treatment interval following consultation, 41 limbs underwent EVSA (group I) and 31 limbs (group II) were treated with compression hose and anti-inflammatories, analgesics and/or anticoagulants. Forty-three limbs either did not have saphenous reflux (39), or had reflux but were in the third trimester of pregnancy (3) or had advanced malignancy (1) (Figure 1).
Algorithm for managing patients presenting with isolated SVT.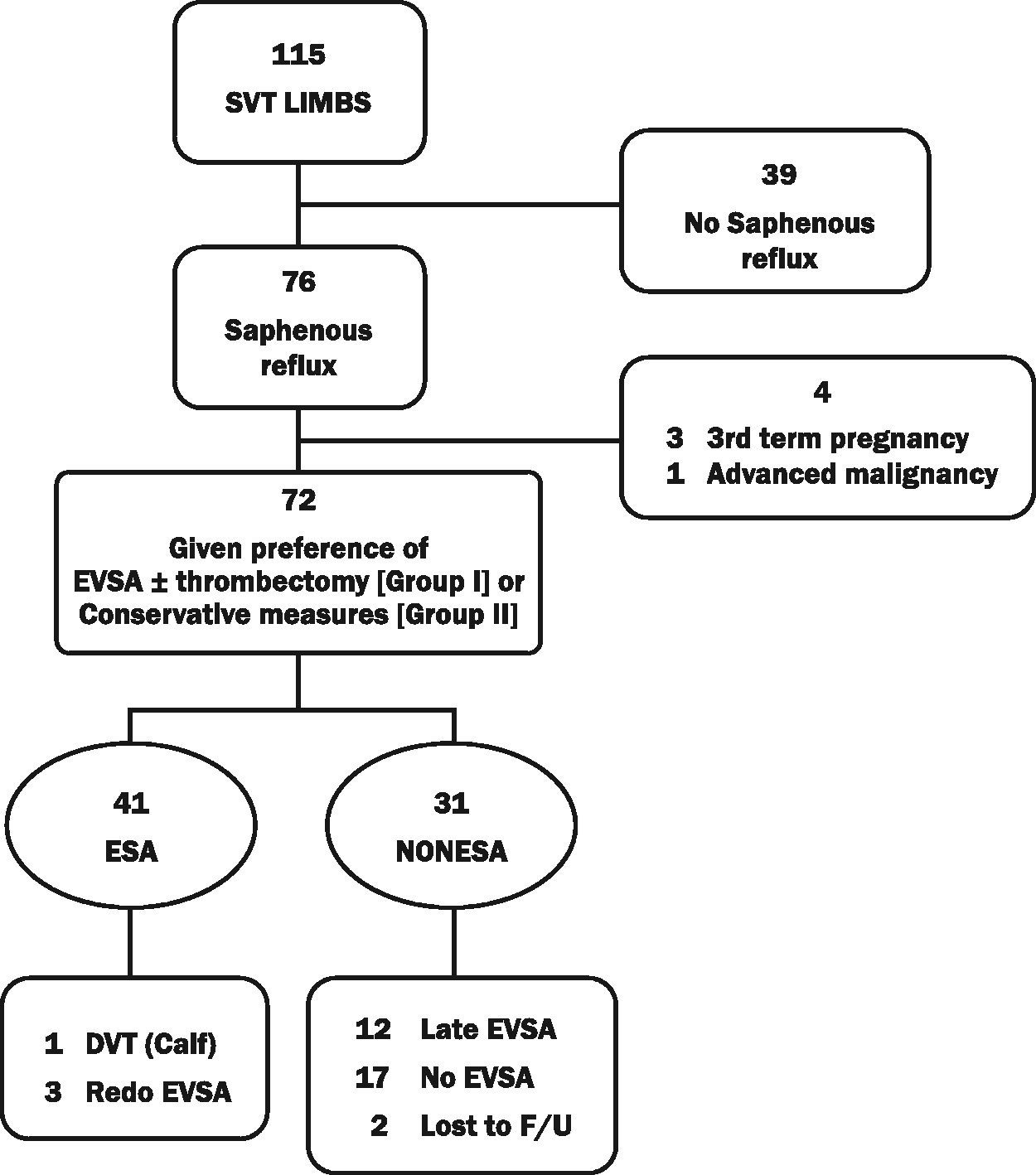
Characteristics of 71 patients (72 limbs) presenting with isolated SVT and saphenous vein reflux.
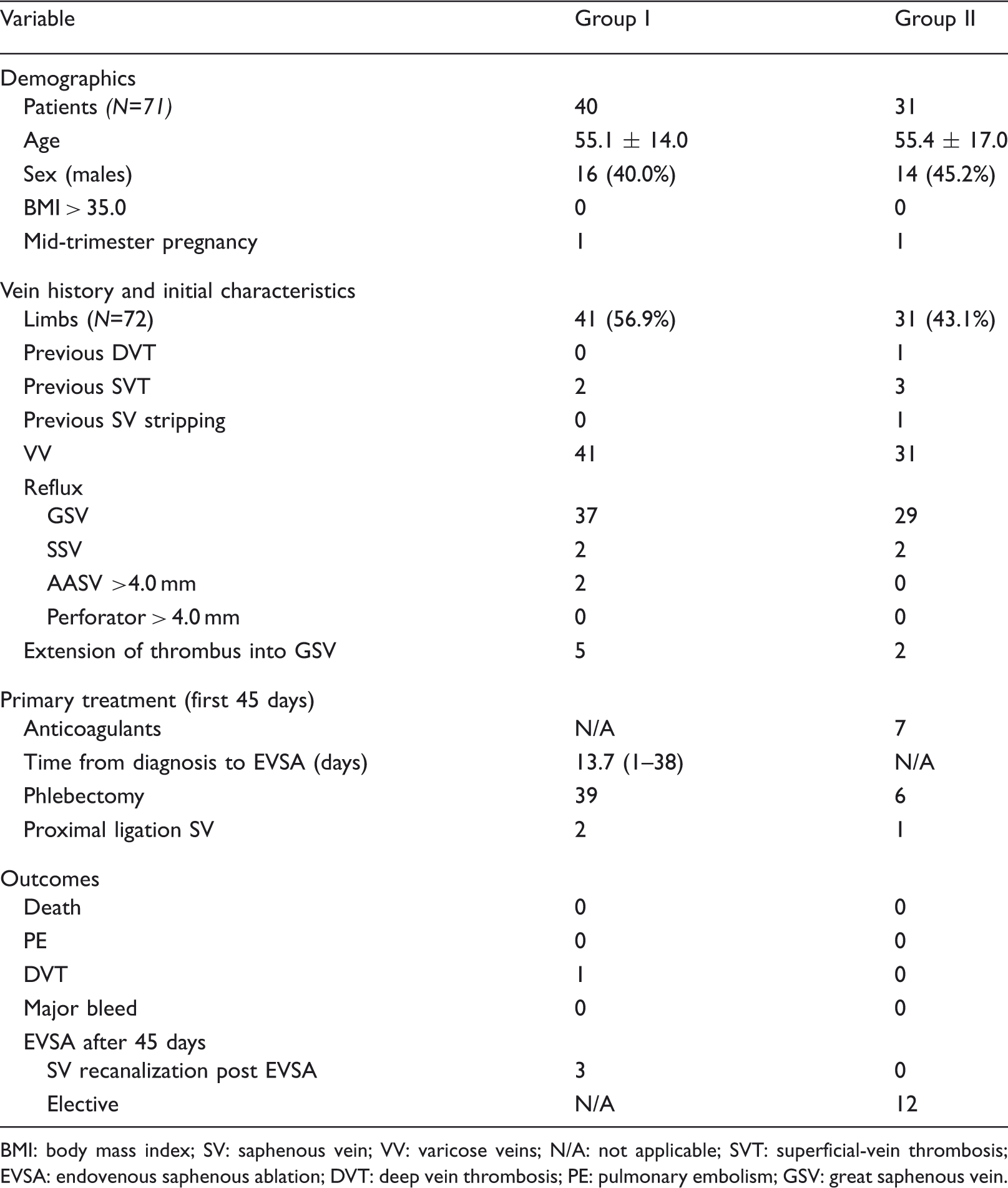
BMI: body mass index; SV: saphenous vein; VV: varicose veins; N/A: not applicable; SVT: superficial-vein thrombosis; EVSA: endovenous saphenous ablation; DVT: deep vein thrombosis; PE: pulmonary embolism; GSV: great saphenous vein.
In group I, mean interval from diagnosis to treatment was 13.7 days (range 1–38). One primary event (transient calf DVT), thought to be a consequence of over-vigorous manual expression of thrombosed veins, was documented early in the series. Three patients (7.9%) had documented recanalization of the great saphenous vein (GSV) and underwent a second EVSA for symptomatic varices in late follow-up ending in August 2012.
In group II, seven patients received anticoagulants and no primary events were noted. Of the 29/31 group II limbs surveyed in August 2012, 12/29 (41.4%) had undergone late EVSA (range 2–80 months). The reasons for delayed treatment were recurrent SVT (2), telangiectasia bleed (1), elective post-partum treatment (1), resolution of insurance issues (3), and elective treatment for symptoms (5). No primary events or late recurrences were noted in this group. Thus, of the 72/115 (62.6%) limbs that were candidates for EVSA at initial presentation, 53/72 (73.6 %) of limbs with saphenous reflux initially assigned to either group I or II eventually underwent EVSA (Figure 2).
Kaplan–Meier estimate of two-year cumulative EVSA in 72 candidate patients presenting with isolated superficial-vein thrombosis. An additional four patients underwent EVSA in years 3–10. SE < 10% through year 10.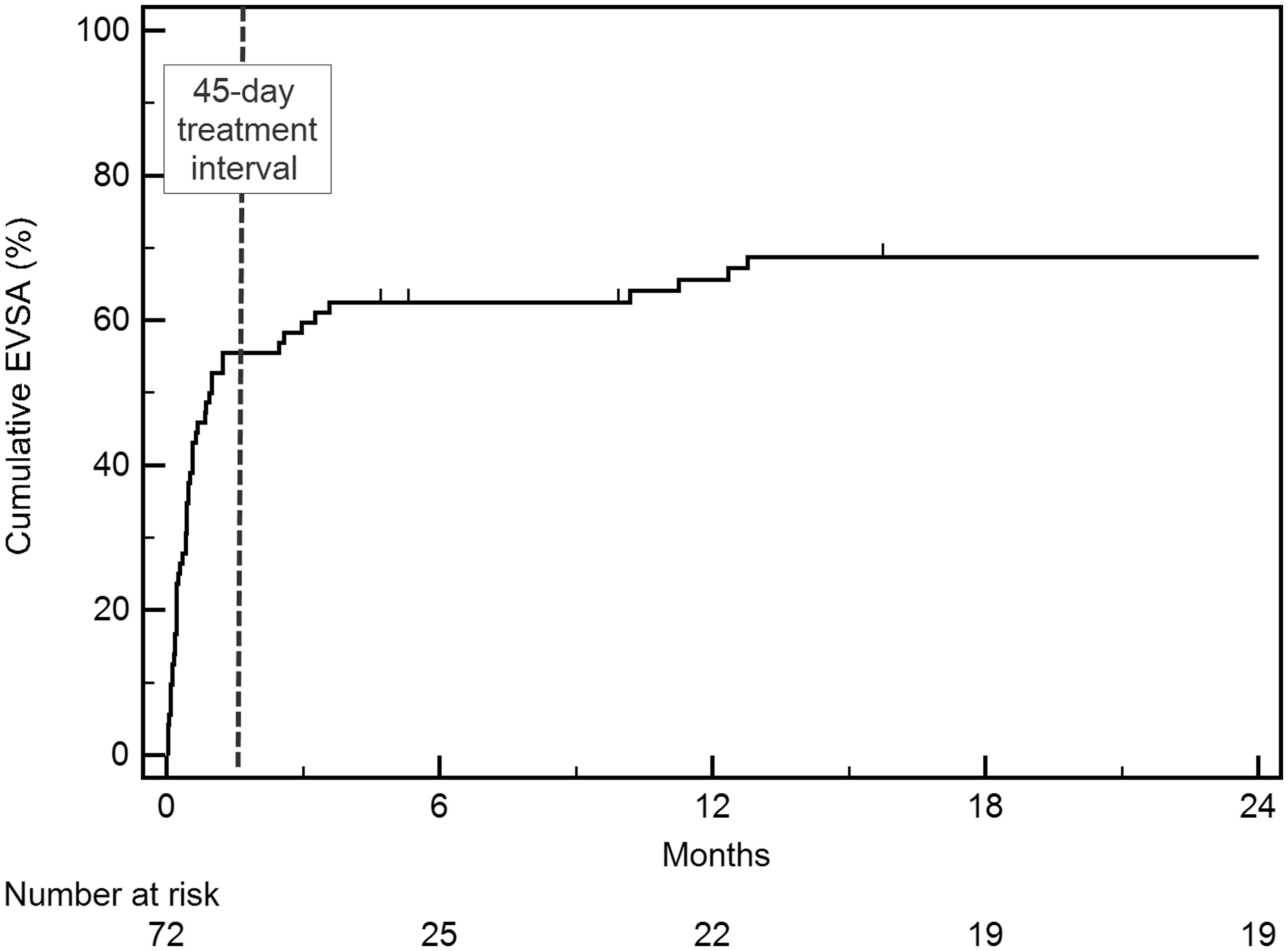
No consistent metric was used to assess the acute pain of SVT or any intervention. All group I patients resumed full activities and/or work within two weeks.
Discussion
In a recently published RCT of 3002 patients with isolated SVT, the benchmark CALISTO study demonstrated that a daily 2.5 mg subcutaneous injection of fondaparinux in all patients produced superior outcomes compared to treatment solely with support stockings supplemented with anti-inflammatory and analgesic medication. 8 The researchers, however, did not stratify patients by risk or consider alternate treatments with other anticoagulants or interventions. Since certain subgroups have been shown to have variable risk for VTE, identifying such patients and tailoring their treatments might provide a benefit that is equal to or greater than a policy of anticoagulation for everyone. 9 For example, previous studies suggest that the need for anticoagulation is greater in subgroups with a relatively higher risk of VTE, such as patients with SVT in the GSV extending above the knee and patients presenting without thrombosed varices.6,9,10
Another potential subgroup for tailored treatment, often reported in the surgical literature before 2000, includes patients whose SVT develops in association with saphenous vein reflux.6,11 Although the incidence of VV is usually reported in 80–95% of individuals presenting with SVT, 8 not all patients with VV have saphenous vein reflux and some patients with saphenous vein reflux present only with saphenous vein thrombosis. There are scant (if any) data on the incidence of immediately treatable saphenous reflux in patients presenting with SVT. This review of either self- or physician-referred patients found the incidence of SVT arising in the distribution of a refluxing axial saphenous vein to be 66.8%, suggesting that saphenous reflux is common in patients presenting with acute isolated SVT. Although underpowered, the study also suggests that EVSA does no harm. Despite the need for intervention, the majority of patients preferred definitive treatment of saphenous reflux to prolonged anticoagulation and support hose. Others elected EVSA later when additional complications or severe symptoms supervened.
Patients who present with SVT and saphenous reflux should be offered an option for EVSA if further experience confirms these results.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Ethical approval
The IRB of Cedars-Sinai Medical Center approved this study (IRB Pro00032943).