
Abstract
Introduction
Blood transfusions during paediatric cardiac surgery with (cardiopulmonary bypass) CPB carry increased risks, including infection and immunological complications. This study evaluates blood product use in the Clinic for Paediatric Cardiology and Cardiac Surgery at the Children’s University Hospital following the implementation of a revised blood management protocol from 2020 to 2023.
Methods
A retrospective review of 135 paediatric patients who underwent congenital cardiac surgery with CPB was conducted. Patients were categorized into three age groups: Group 1 (<1 year), Group 2 (1 – 4 years), and Group 3 (>4 years). Data on erythrocyte, fresh frozen plasma (FFP), cryoprecipitate, and platelet use were analysed using the Kruskal-Wallis and Spearman’s rho tests, with significance set at p < .05, and confidence interval (CI) of 95% quoted when applicable.
Results
Erythrocyte use significantly declined over 4 years, with the largest reductions observed from 2020 to 2023 [p < .0001]. Older and heavier patients required fewer transfusions, with a significant inverse correlation between weight and erythrocyte use [Spearman’s rho = −0.29, p = .001]. Platelet use also decreased significantly from 2020 to 2023 [p = .04], while FFP and cryoprecipitate use declined notably over the same period [p < 0.01].
Conclusion
Over 4 years, significant reductions in blood product use were observed, particularly for erythrocytes and platelets. Patients’ age and weight were inversely related to erythrocyte transfusion needs. These trends may reflect improvements in surgical techniques and blood management protocols, with potential benefits for patient outcomes.
Keywords
Introduction
Paediatric cardiac surgery, particularly in patients with congenital heart defects requiring cardiopulmonary bypass (CPB), presents significant challenges due to high intraoperative bleeding risk and frequent need for blood transfusions. Blood management in paediatric patients undergoing cardiac surgery is complex, with risk factors such as patient weight, age, immaturity and an increased tendency for haemostasis activation. These patients also have higher metabolic and oxygen demand along with considerable susceptibility to haemodilution due to the disproportionate size of CPB circuits relative to their smaller blood volumes. 1 The necessity of transfusions, however, is associated with various adverse outcomes, including an increased rate of postoperative complications, such as pulmonary issues, infections, the need for prolonged mechanical ventilation and, an extended hospital stay.2–4 Given these concerns, strategies to minimize transfusion requirements are crucial with emphasis on limiting CPB circuit size and optimizing blood management to approach the goal of bloodless CPB.4–6
Current management practices for paediatric CPB are variable, but there is a notable lack of universally accepted guidelines. Moreover, limitations in the scale and scope of studies addressing paediatric CPB management hinder the development of robust, evidence-based protocols.5,7
Blood product management during CPB involves a multi-stage process, including preoperative, intraoperative, and postoperative strategies. Preoperative measures often focus on minimizing bleeding risk by replacing medications such as aspirin and vitamin K antagonists with low-molecular-weight heparin (LMWH). Intraoperative strategies to reduce blood use in congenital cardiac surgery include minimizing haemodilution, employing advanced venous drainage techniques, utilizing hypothermia and ultrafiltration, optimizing heparin management, and using cell salvage devices. Postoperative management aims to limit blood loss and support recovery through the use of cell salvage devices, administration of antifibrinolytics, and restricting blood draws. 8
To address these challenges, a revised blood management protocol was introduced in 2020. While this study does not analyse the direct impact of individual protocol changes, it evaluates overall trends in blood product use from 2020 to 2023, following the implementation of this updated approach. By assessing transfusion patterns in paediatric cardiac patients undergoing CPB, this study aims to provide insights into the effectiveness of evolving blood management strategies in clinical practice.
Materials and methods
Methods for data collection
This study received approval from the Institutional Ethics Committee. This retrospective study analysed the medical records of all patients who underwent congenital cardiac surgery with CPB at the Clinic for Paediatric Cardiology and Cardiac Surgery in the Children’s University Hospital between 2020 and 2023. A revised blood management protocol was introduced in 2020, and its impact on blood product use was evaluated.
A total of 144 patients were identified; however, nine were excluded due to incomplete data, leaving 135 patients for the analysis. The inclusion criteria encompassed all patients undergoing cardiac surgery with CPB, while the exclusion criteria included patients undergoing cardiac surgery without CPB and those with incomplete data.
The collected data included patient age, weight, aortic occlusion time, total bypass time, and transfusion volumes of erythrocytes, fresh frozen plasma (FFP), cryoprecipitate, and platelets. For a small number of patients, weight at the time of surgery was unavailable and was treated as a missing value in the statistical analysis. To facilitate analysis, the 135 patients were categorised into three different age groups: Group 1 consisted of patients younger than 1 year of age, Group 2 included those between 1 year and 4 years, and Group 3 included patients older than 4 years.
Statistical analysis
Statistical analysis was performed using SPSS. Numerical data were presented as counts and percentages and analysed using Kruskal- Wallis test and Spearman’s rho test. Normality was assessed using the Shapiro-Wilk and Kolmogorov-Smirnov tests before applying the Kruskal- Wallis test. The results showed a significant deviation from normality (Shapiro-Wilk: p < .05) justifying the use of the Kruskal-Wallis test. The statistical significance was set at p- values <0.05. Spearman’s rho test was used to assess the correlation between weight (Kg) and erythrocyte (mL) with a 95% confidence interval (CI) and a significance level of p- value <0.05. Not all collected data were utilized in this study due to constraints within the research framework.
Results
Blood product use trends: This study analysed blood product use during paediatric cardiac surgery with CPB at a paediatric hospital over 4 years from 2020 to 2023. The overall trend demonstrated a significant reduction in the absolute use of blood products. Notably, the median absolute erythrocyte use decreased from 529 mL in 2020 to 269 mL in 2023 [H = 62.775, df = 3, p < .001], These changes are illustrated in Figure 1. The median of erythrocytes used per year in mL.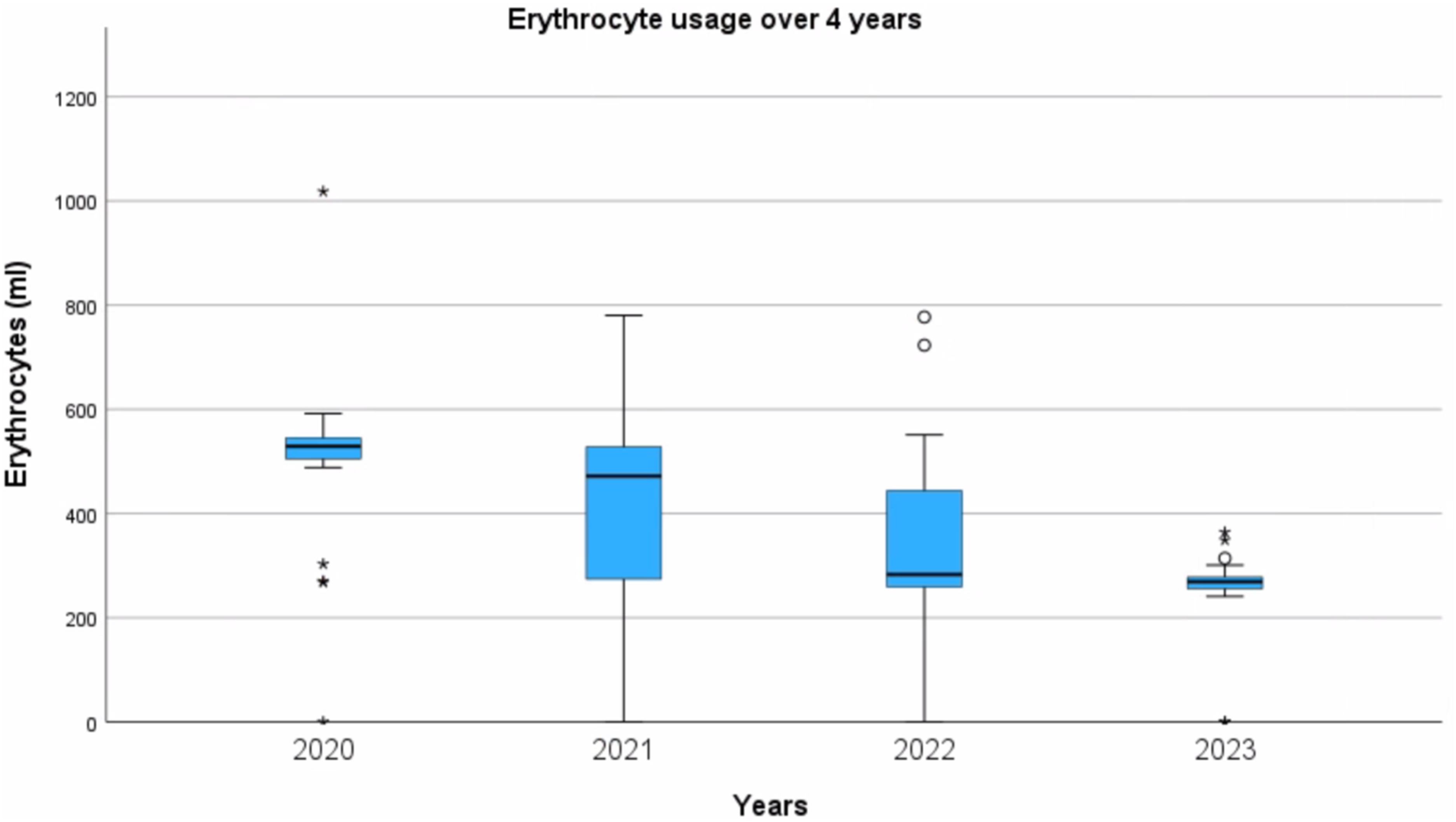
The total erythrocyte use significantly decreased over time. Specifically, there was a significant decrease from 2020 to 2022 [H = 43.770, df = 3, p < .0001] and from 2020 to 2023 [H = 62,775, df = 3, p < .0001]. Additionally, decreases were observed from 2020 to 2021 [H = 27.923, df = 3, p = .018) and from 2021 to 2023 [H = 34.852, df = 3, p = .005].
But no statistically significant decrease absorbed from 2022 to 2023 [H = 19.005, df = 3, p = .33] was seen. Figure 2 presents the distribution of erythrocyte transfusion volumes over the 4 years. The frequency distribution of erythrocyte transfusion volumes (mL) across the 135 cases.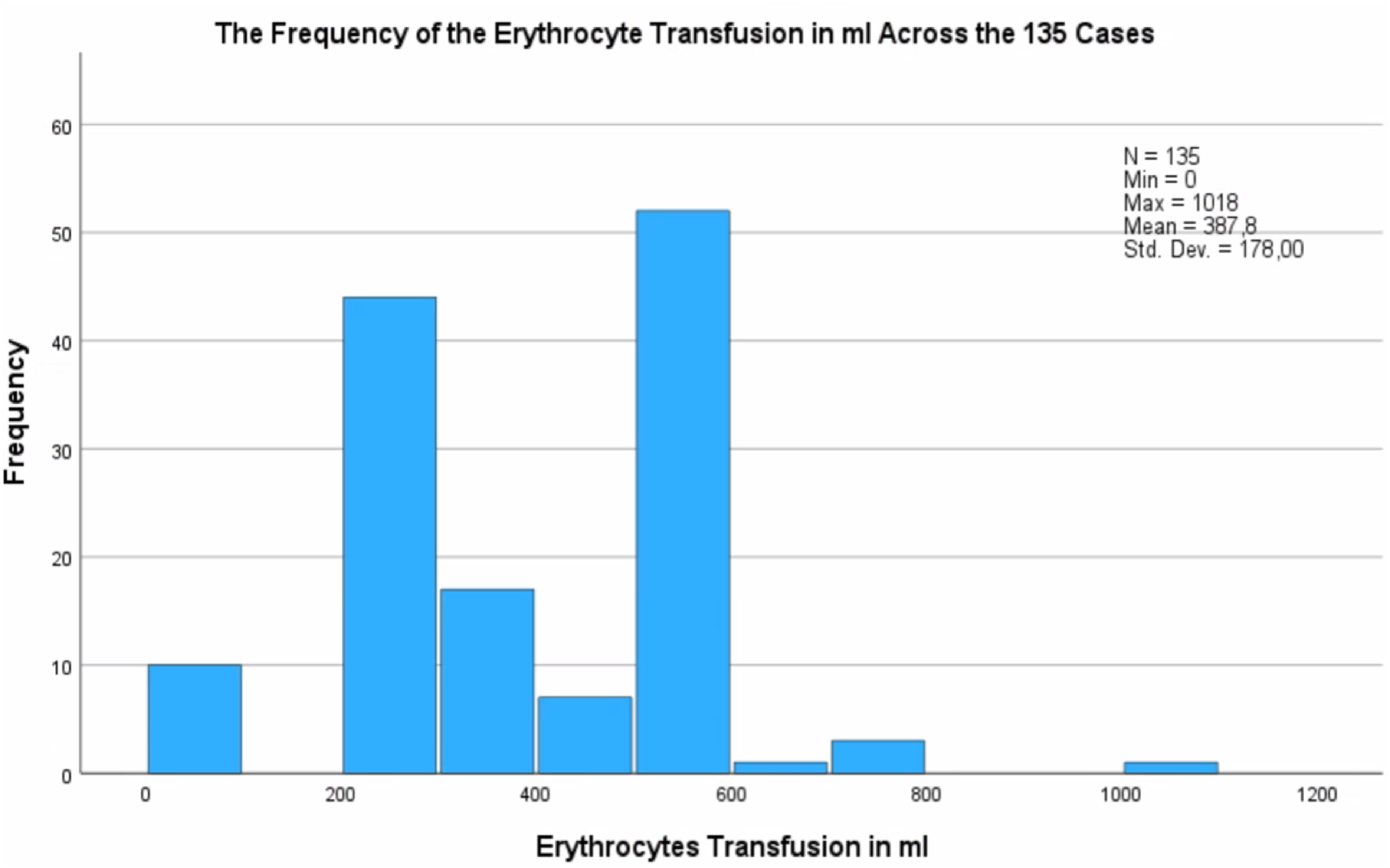
A closer look at erythrocyte use across three age groups revealed a significant difference in transfusion requirements. Patients under 1 year of age (Group 1) required the highest absolute volumes, while older children (Group 3) showed a significant reduction in use [H = 28.618, df = 2, p = .001]. A similar difference was also observed between one- to four-year-olds (Group 2) and children aged four and older (Group 3). Group 3 required statistically significant lower absolute erythrocyte volume compared to Group 2 [H = 40.961, df = 2, p < .0001]. Interestingly, no significant difference was observed between Groups 1 and 2.
A weak negative correlation was found between patient weight and erythrocyte use [Spearman’s rho = −0.29, CI: [-0.443, −0.120], p < .05]. These results suggest that as patient weight increases, erythrocyte transfusion requirements per millilitre decrease, as shown in Figure 3. As depicted in the scatter plot, heavier patients required fewer millilitres of erythrocytes. While these results indicate a statistically significant negative correlations, they do not establish causality for the decrease in erythrocyte use with increasing weight. The erythrocytes in mL per weight per patient.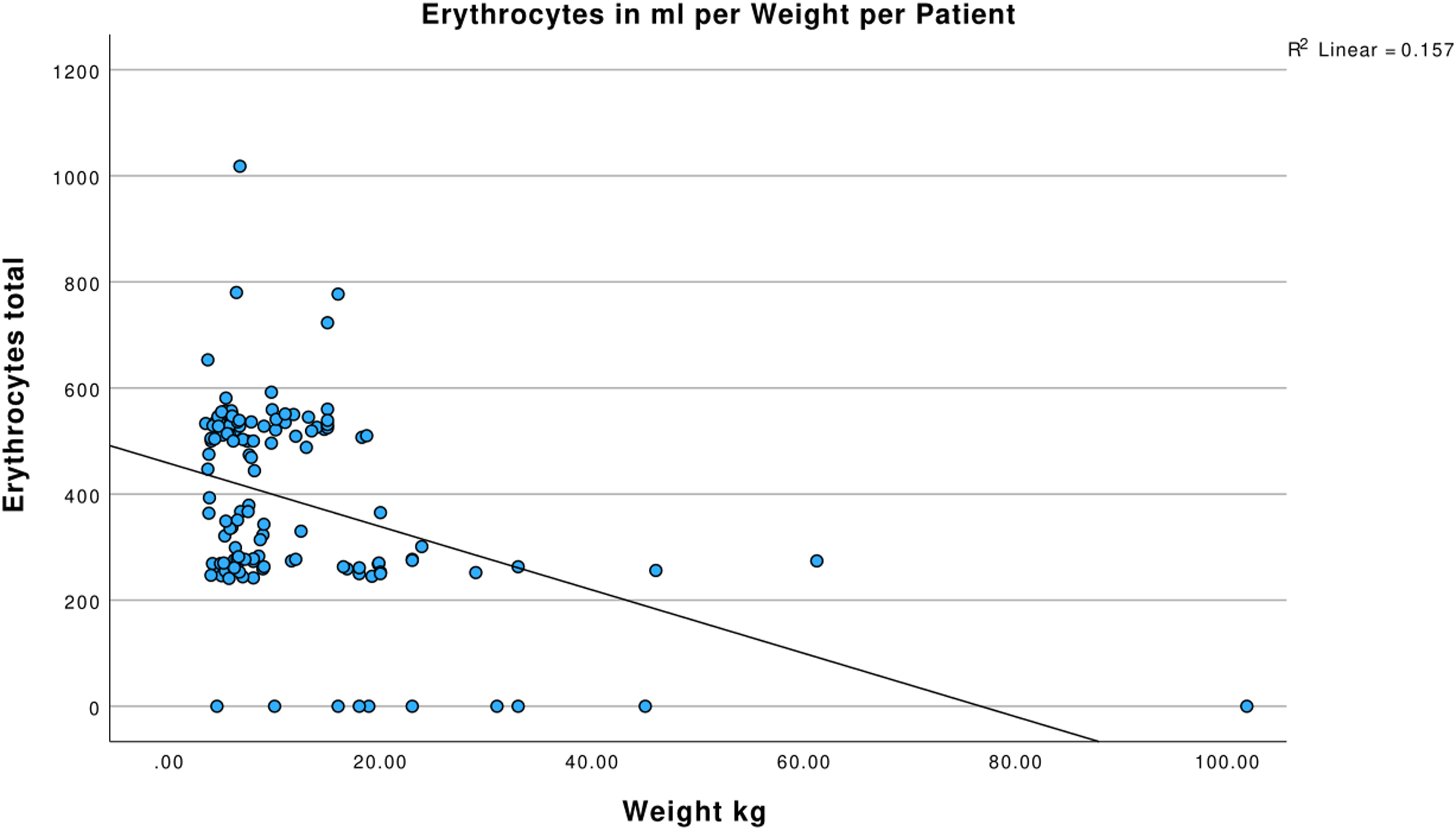
Also, the effect size is relatively weak, indicating that weight alone has a limited impact on erythrocyte use in clinical settings. While smaller patients may require more erythrocytes due to a higher CPB priming volume relative to their blood volume, other factors likely play a more dominant role.
Trends in other blood products showed a decline in their use over the study period. Platelets use significantly decreased from a median of 60 mL in 2020 to 0 mL in 2023 [p = .04].
The use of FFP remained minimal, with a median of 0 mL across all years, although statistically significant variations were observed. A significant decrease from 2020 to 2022 [H = 22,761, df = 3, p = .002] and from 2020 to 2023 [H = 22.167, df = 3, p = .009] was observed.
Median of all blood products used over the year.

Discussion
This study demonstrated a clear trend of reduced blood product use over the 4-year period following the implementation of the revised blood management protocol. A significant reduction was mostly observed in erythrocyte and platelet transfusions.
Additionally, patient age and weight were inversely related to erythrocyte transfusion needs, emphasizing the importance of tailored blood management strategies.
Erythrocyte use during paediatric cardiac surgery with CPB declined significantly. This reduction likely reflects improvements in both surgical techniques and intraoperative blood management strategies. The changes in the blood management protocol implemented in this study included preoperative, intraoperative, and postoperative strategies aimed at reducing transfusion requirements and minimizing associated risks. While the direct impact of individual interventions was not analysed, these changes align with established patient blood management protocols and may have contributed to the observed trends in transfusion reduction.
Preoperative management strategies included stopping aspirin intake 7 days before surgery and, when necessary, switching to low-molecular-weight heparin (LMWH). This adjustment has been associated with a reduced risk of perioperative bleeding while maintaining adequate anticoagulation. 2
Intraoperatively, several measures were introduced to minimize haemodilution and improve coagulation stability. One of the key modifications was reducing the length of CPB circuit tubing, which lowered the priming volume and helped maintain higher haematocrit levels. Studies have shown that reducing priming volume is critical in paediatric CPB, as excessive haemodilution is associated with an increased need for transfusion.3,9
Additionally, targeting a haematocrit level of >28% was achieved through the routine use of osmotic diuretics (Mannitol) at CPB initiation and intraoperative ultrafiltration. Ultrafiltration techniques, particularly conventional ultrafiltration (CUF) and modified ultrafiltration (MUF), were applied in a standardized manner—CUF was used in all cases, while MUF was performed in surgeries where aortic occlusion exceeded 1 hour. These techniques have been widely recognized for their role in reducing postoperative fluid overload, improving haemostasis, and decreasing transfusion needs.1,10
Another intraoperative adjustment was limiting the use of hypothermia. While deep hypothermia has traditionally been used in paediatric cardiac surgery to provide metabolic protection, it is associated with coagulopathy and impaired platelet function, which can increase transfusion requirements. 11
To mitigate this, a normothermic approach was adopted for standard cases (e.g., ventricular septal defect [VSD] repairs), while for more complex cases, body temperature was maintained no lower than 28°C. Finally, the routine use of cell salvage devices was introduced in every operation, facilitating the recovery of autologous erythrocytes and reducing reliance on donor blood. 9
Postoperative strategies focused on minimizing blood loss and optimizing recovery. This included the use of antifibrinolytics, routine application of cell salvage devices, and strict limitations on blood draws. Studies have demonstrated that excessive postoperative blood sampling can significantly contribute to anaemia in critically ill paediatric patients. 12 Sebastian et al. highlighted that implementing restrictive blood draw protocols, in combination with intraoperative blood conservation techniques, can substantially reduce transfusion requirements. 8
Comparing erythrocyte use across different age groups revealed that older, larger, and heavier patients required fewer transfusions. This trend aligns with findings in adult cardiac surgery, where transfusion needs decrease with increased patient size. 6 Hanson et al., in a secondary analysis of a clinical database, found that infants received significantly more erythrocyte and cryoprecipitate transfusions than older patients, regardless of surgical complexity. 13 Similarly, Bohuta et al. reported no significant difference in transfusion requirements between simple and complex cases, further supporting the idea that patient size, rather than procedural complexity, may be a stronger determinant of transfusion needs. 14
However, the broad age range in Group 3 in this study may have influenced the results. Older children typically require fewer transfusions, but variability within the group makes it challenging to draw more precise conclusions.
In addition, Bohuta et al. reported that no significant age-related differences were observed in platelet or FFP transfusions. 14
A weak but statistically significant negative correlation was observed between patient weight and erythrocyte transfusion needs. While heavier patients required fewer transfusions, the small effect size suggests that other factors also play a role. This finding is consistent with previous studies, which have also reported lower transfusion requirements in larger patients.6,8 Similarly, Bohuta et al. observed a decreased need for erythrocyte transfusion in larger patients, reinforcing this association. 14 Some researchers even describe the possibility of performing paediatric cardiac surgery with CPB without blood products in the priming solution, potentially eliminating the need for transfusions in select cases. Boechtter et al. found that this transfusion-free approach is most feasible in larger patients, particularly when minimized CPB circuits are used to reduce priming volume. 9 Likewise, Miyaji et al. reported successful complex, transfusion-free procedures in patients weighing more than 4 kg, where CPB duration and aortic occlusion time—rather than preoperative haematocrit or procedural complexity—were the main determinants of transfusion need. 15
The potential for transfusion-free paediatric cardiac surgery with CPB is becoming increasingly viable, benefiting patients who refuse blood transfusions, such as Jehovah’s Witnesses, and reducing transfusion- related risks. 16 Other factors, such as CPB duration and aortic occlusion time, also influence transfusion needs as mentioned above. 9 Shorter CPB and shorter aortic occlusion time are associated with reduced transfusion needs. 15 However, CPB duration was not considered in this study, which highlights a key limitation.
A significant reduction in FFP, platelets, and cryoprecipitate was observed, aligning with findings by Cholette at al., who reported similar reductions following the introductions of cell saver treatment. 17 While FFP is essential for restoring volume and supporting haemostasis by providing vitamin K-dependent clotting factors, it also carries risks, including transfusion-related acute lung injury (TRALI). 8 Platelets play a key role in clotting but are often depleted during CPB, requiring transfusions guided by laboratory tests and clinical evaluation.
Cryoprecipitate, rich in fibrinogen and Factor VIII, is used to correct low fibrinogen levels, with dosages tailored to body weight. Machovec et al. have found a reduction of in cryoprecipitate transfusion by 50 % due to implementing of checking platelet and fibrinogen blood levels during rewarming phase of CPB.
Platelets play a key role in clot formation but are frequently depleted during CPB, making transfusions necessary. Their use is often guided by laboratory testing and clinical evaluation to minimize unnecessary administration. Similarly, cryoprecipitate, which is rich in fibrinogen and Factor VIII, is used to correct low fibrinogen levels, with dosages tailored to patient weight. Machovec et al. found that cryoprecipitate transfusion could be reduced by 50% by routinely monitoring platelet and fibrinogen levels during CPB rewarming, highlighting the importance of a more targeted transfusion approach. 12
Given the need to limit unnecessary transfusions, fibrinogen concentrate has been proposed as a safer, more concentrated alternative to cryoprecipitate, particularly in fluid-restricted patients. A small prospective study by Gala et al. demonstrated its potential to reduce transfusion requirements while maintaining haemostatic stability. 18
After implementing the revised blood management protocol, the clinical reduction in intraoperative bleeding was observed, though it was not formally analysed in this study. Additionally, a shorter length of stay in both the intensive care unit (ICU) and the hospital was noted, potentially due to faster and improved patient recovery. Harris et al. reported that early extubation was associated with a decreased morbidity, shortened ICU stay and on overall shorter hospital stay. 19 While these findings were not the focus of this study, they warrant further research to establish a more direct link between reduced transfusion requirements and improved recovery times. Whereas Bohuta et al. reported no significant effect on early outcome with decreased blood product use, and also state that more studies are needed for long- term impact. 14
Additionally, reducing transfusion requirements in paediatric cardiac surgery may help decrease complications such as infections, prolonged mechanical ventilation, and other postoperative issues. 4
The limitations of this study include the focus on intraoperative data without considering pre- and postoperative conditions of the patients. Additionally, blood products were administered both via the CPB machine and through venous catheters, with no clear distinction between the venous and arterial volumes of blood products given, unlike other studies that have specifically focused on CPB- related transfusions. 15 This lack of distinction may impact the interpretation of blood product use. And lastly all the limitations that come with a retrospective study.
Further research is needed to explore surgical improvements, patient outcome, and further blood conservation techniques in paediatric cardiac surgery. As paediatric cardiac surgery continues to evolve, emerging guidelines for blood product transfusions - currently under development by European bodies (EACTS, ESPA, EACAIC and EBCP) —will be instrumental in optimising transfusion protocols for paediatric cardiac surgeries with CPB. 6 While patient blood management guidelines for adult cardiac surgery with CPB are already available from EACTS/ EACTA, 20 the growing body of paediatric research holds promise for enhancing transfusion management in children, ultimately improving surgical outcomes in this critical field.
Conclusion
This study demonstrates significant reductions in blood product use, particularly erythrocytes and platelets, over the 4-year study period after implementing the revised blood management protocol. These reductions may also be related to improvements in surgical techniques during paediatric cardiac surgery with CPB. Additionally, patient age and weight were inversely related to erythrocyte transfusion needs, emphasising the importance of customised blood management strategies in different paediatric populations.
Footnotes
Acknowledgements
Edgars Sikora – Radbound University Nijmegen, The Netherlands for the help and advise given during the preparation of the article and Jeļena Perevozčikova - Riga Stradiņs University, Latvia, for helping with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The data sets generated during and/ or analysed during the current study are available from the corresponding author on reasonable request.