
Abstract
Objective: Positive fluid balance in patients on veno-venous extracorporeal membrane oxygenation (VV ECMO) is associated with increased mortality. Drainage insufficiency on VV ECMO is a common occurrence and managed with fluid administration. The use of multi-stage drainage cannulas may result in decreased drainage insufficiency, but it is unclear the effects this may have on patient fluid balance.
Design: A historical cohort study was conducted on adult patients undergoing VV ECMO for acute respiratory failure in femoral-jugular configuration.
Setting: Intensive Care Unit.
Patients: Adult patients undergoing VV ECMO for acute respiratory failure.
Interventions: Cumulative fluid balance in the first 7 days following initiation of VV ECMO was examined. The relationship between cumulative daily fluid balance over the first 7 days and type of drainage cannula was assessed using mixed methods linear regression.
Measurements and Main Results: We included 82 consecutive patients between April 1st, 2020 and September 1st, 2022. 47 (57%) patients were treated with a single-stage drainage cannula. Our final model showed the use of a multi-stage cannula decreased fluid balance by 740 mL/day (95% CI: −1360 to −118, p = .02) compared to patients with a single-stage drainage cannula for the first 7 days.
Conclusions: The use of multi-stage drainage cannulas resulted in improved fluid balance in patients on VV ECMO in the first 7 days.
Keywords
Key points
Introduction
Veno-venous extracorporeal membrane oxygenation (VV ECMO) enables oxygenation and removal of carbon dioxide in patients with acute respiratory distress syndrome (ARDS)1,2 refractory to conventional mechanical ventilation. The use of VV ECMO has increased in the past decade and has been further accelerated with the COVID-19 pandemic.1–3
Conservative fluid management in patients with ARDS improves lung function and decreases duration of mechanical ventilation.4,5 Similarly, positive fluid balance in patients with ARDS on VV ECMO has been associated with increased mortality.6–11 While pharmacologic diuresis is frequently used to facilitate a negative fluid balance, this is often a challenge in patients managed with VV ECMO. Drainage insufficiency, wherein limited pump blood flow and chattering of the drainage cannula, secondary to diuresis, has been shown to impair cannula drainage and disrupt blood flow during VV ECMO.12,13 Drainage insufficiency is often treated with fluid administration, which can conflict with the overall goals to maintain a negative fluid balance.
Drainage cannulas are placed into the central venous system in the superior vena cava or inferior vena cava, typically terminating at right atrium junction.
14
The placement of drainage cannulas is not standardized in their type (single- or multi-stage) or location within the inferior vena cava (IVC).15,16 In recent years, there has been an increased usage of multi-stage drainage cannulas containing multiple sites for venous blood drainage. These multi-stage cannulas allow for less negative pressure drainage compared to single-stage cannulas.
14
In contrast to single-stage cannulas where the maximum negative pressure occurs at the tip, the site of maximum negative pressure in multi-stage cannulas can be greater than 20 cm from the tip.
14
It is unclear if this advantage of multi-stage cannulas translates to improved venous drainage compared to single-stage cannulas as has been shown in vitro studies.
17
Furthermore, it is unclear if the position of the drainage cannula within the inferior vena cava is associated with negative fluid balance in patients with ARDS (Figure 1). Model of VV ECMO cannula position and types of drainage cannula. Panel (A): During VV ECMO venous blood is removed by the drainage cannula which typically terminates at the inferior vena cava-right atrial junction. Panel (B) depicts both a single-stage drainage cannula and its site of venous drainage and a multi-stage drainage cannula.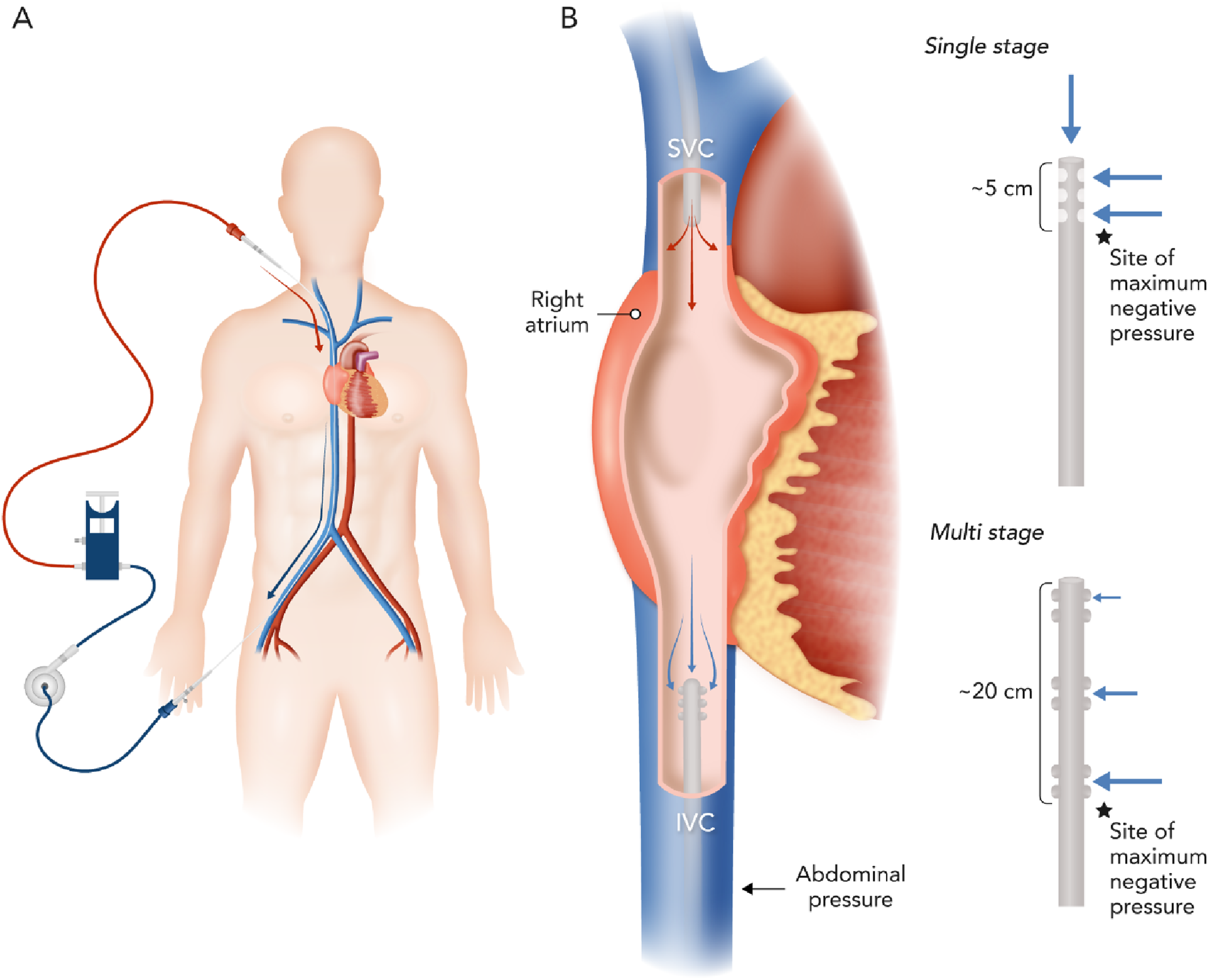
Therefore, we conducted a historical cohort study in patients requiring VV ECMO for ARDS with the central aim of determining the association between cannula type (single- vs multi-stage) in femoral-jugular configuration and cumulative 7-day fluid balance.
Methods
We conducted a historical cohort study of 82 adult patients who received VV ECMO in the Vancouver General Hospital (VGH) Intensive Care Unit (ICU) from April 1st, 2020 to September 1st, 2022. UBC Clinical Research Ethics Board approval was obtained for data collection (H22-03439) on April 18, 2023 (title ECMOcannula) with standards in accordance with the ethical standards of the responsible committee on human experimentation (University of British Columbia) and with the Helsinki Declaration of 1975.
Study setting, management, and population
The ICU at VGH is a closed, 40 bed, mixed medical-surgical unit with a 1:1 nursing to patient ratio and sub-specialty trained intensivists in VV ECMO. On-site perfusion specialists guide ongoing provision of VV ECMO. Cannulation with percutaneous Seldinger technique is guided by ultrasound25 with standardized right femoral vein access (21–27 Fr) and right internal jugular vein (15–19 Fr) return cannulas. Medtronic Bio-Medicus Life Support Femoral Venous Single-stage (50 cm) reference number LS96360-025, Medtronic Bio-Medicus multi-stage (61 cm) reference number CB96345-025 cannulas and Getinge HLS multi-stage drainage cannulas are available to clinicians and among our group there is clinical equipoise regarding the types of cannulas currently used. Drainage cannula size is chosen by clinicians based on patient size and perceived flow requirements. Cardiohelp (Gothenburg, Sweden) or Sorin (London, United Kingdom) ECMO consoles are used. Patients are ventilated on pressure control of 10 cm H2O, a respiratory rate of 10 and a positive end expiratory pressure (PEEP) of 10 cm H2O once VV ECMO is commenced. Fluid management is at the discretion of the treating clinician, but the avoidance of a positive fluid balance is encouraged. Hemoglobin threshold of greater than 80 g/L was maintained. Management is reflective of ELSO recommendations. 3
Consecutive patients greater than 18 years of age undergoing femoro-jugular VV ECMO for hypoxemic respiratory failure from ARDS were included. VV ECMO criteria for hypoxemic respiratory failure are based on randomized control trial and ELSO recommendations.1,2 Patients with bi-caval dual lumen cannulas, patients requiring VV ECMO without ARDS and those receiving veno-arterial ECMO were excluded. Patients on VV ECMO with associated RV failure that were converted to V-VA ECMO were excluded.
Data sources, measurement, and outcomes
In addition to demographic data, the following data was collected using a REDCap (H14-00930) database 18 : VV ECMO-related complications (e.g. CNS injury, bleeding, organ failure, infection, death), circuit complications (e.g. oxygenator failure, air embolism, pump thrombosis), circuit performance details (cannula size, flow rate, sweep gas rate, delta pressure) and clinical physiological parameters (e.g. daily mean arterial pressure, daily fluid balance, Richmond Agitation and Sedation Score (RASS), sedative and vasopressor doses). Cannula positioning based on distance from inferior vena cava-right atrium (IVC-RA) junction in centimeters was assessed by authors ST and DG based on portable supine chest X-ray (confirmed with computed tomography) which is standardly ordered post VV ECMO insertion; this process is shown in E-Figure 2. Daily fluid balance was calculated using all enteral and parenteral intake minus fluid losses (urinary, drainage and renal replacement therapy).
Statistical analysis
Relationship between cannula type and fluid balance univariate analysis
We first plotted the daily cumulative fluid balance for the initial 7 days of VV ECMO for each patient, stratified by single-stage or multi-stage cannula. In order to determine the association between cannula type and cumulative daily fluid balance over the first 7 days, we performed a mixed-effects linear regression of daily cumulative fluid balance and cannula type (dichotomous variable consisting of single-stage and multi-stage), specifying “patient” as a random-effect (STATA command xtreg). To then assess for effect measure modification between cannula type (single-stage or multi-stage) and day of VV ECMO, we a priori included an interaction variable of time (day of VV ECMO) and cannula type.
Relationship between cannula type and fluid balance adjusted analysis
We identified drainage cannula size (categorical variable), and distance of cannula tip from IVC-RA junction, and sequential organ failure assessment (SOFA) score as potential confounders in the relationship between cannula type and 7-day cumulative fluid balance. Thus, we included both cannula size (indicator variable), distance from the IVC-RA junction (continuous variable) and SOFA score (continuous variable) in our final multivariable model. We included an interaction variable of time (day of VV ECMO) and cannula type and an interaction variable of cannula type and distance of cannula tip from IVC-RA junction.
Post-hoc exploratory analysis
Finally, the relationship of cumulative 7-day fluid balance and distance of cannula tip from IVC-RA junction stratified by median distance (4 cm) was explored with univariate logistic regression.
Results
Baseline characteristics and outcomes of patients prior to VV ECMO included in the cohort stratified by type of drainage cannula.
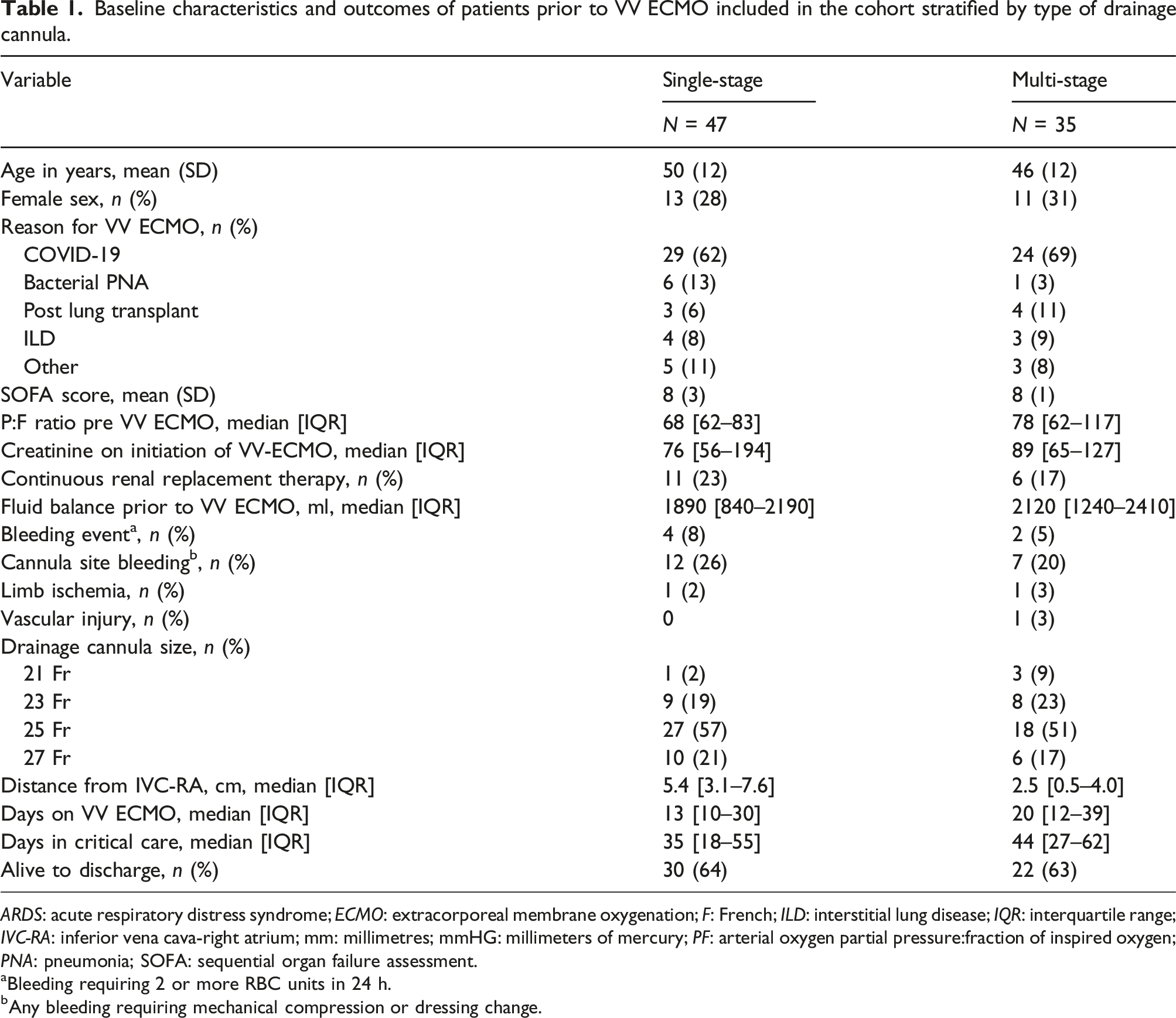
ARDS: acute respiratory distress syndrome; ECMO: extracorporeal membrane oxygenation; F: French; ILD: interstitial lung disease; IQR: interquartile range; IVC-RA: inferior vena cava-right atrium; mm: millimetres; mmHG: millimeters of mercury; PF: arterial oxygen partial pressure:fraction of inspired oxygen; PNA: pneumonia; SOFA: sequential organ failure assessment.
aBleeding requiring 2 or more RBC units in 24 h.
bAny bleeding requiring mechanical compression or dressing change.
The median days (IQR) of VV ECMO was 13 days (10–30) in the single-stage group and 20 (12–39) in the multi-stage group. However, survival to discharge was 64% (N = 30) in the single-stage group and 71% (N = 25) in the multi-stage group (p = .89). Complications of limb ischemia were 2% (N = 1) in the single-stage group and 3% (N = 1) in the multi-stage group.
Relationship between cannula type and fluid balance
The overall 7-day fluid balance was −1150 mL (ml) (IQR −6910 to 3310) using the multi-stage cannula and +2780 mL (IQR 52 to 3930) using the single-stage cannula (Figure 2). There was an interaction between cannula type and day of initiation of VV ECMO (p-interaction = .02). Compared to a single-stage cannula, a multi-stage cannula resulted in −620 mL/day (95% CI: −1160 to −90) more negative fluid balance. Cumulative daily fluid balance trajectories on VV ECMO in patients with single stage and multi stage drainage cannulas. Connected line plots of cumulative daily fluid balance (y-axis) versus time (x-axis) in patients with singe-stage drainage cannula (left panel) and multi-stage drainage cannula (right panel). Each light grey line is an individual patient. The black line is a generated using lowess smoothed curves. p value represents effect measure modification of cumulative fluid balance over time by cannula type indicating a significant decrease in slope in cumulative daily fluid balance for patients with multi-stage drainage cannulas.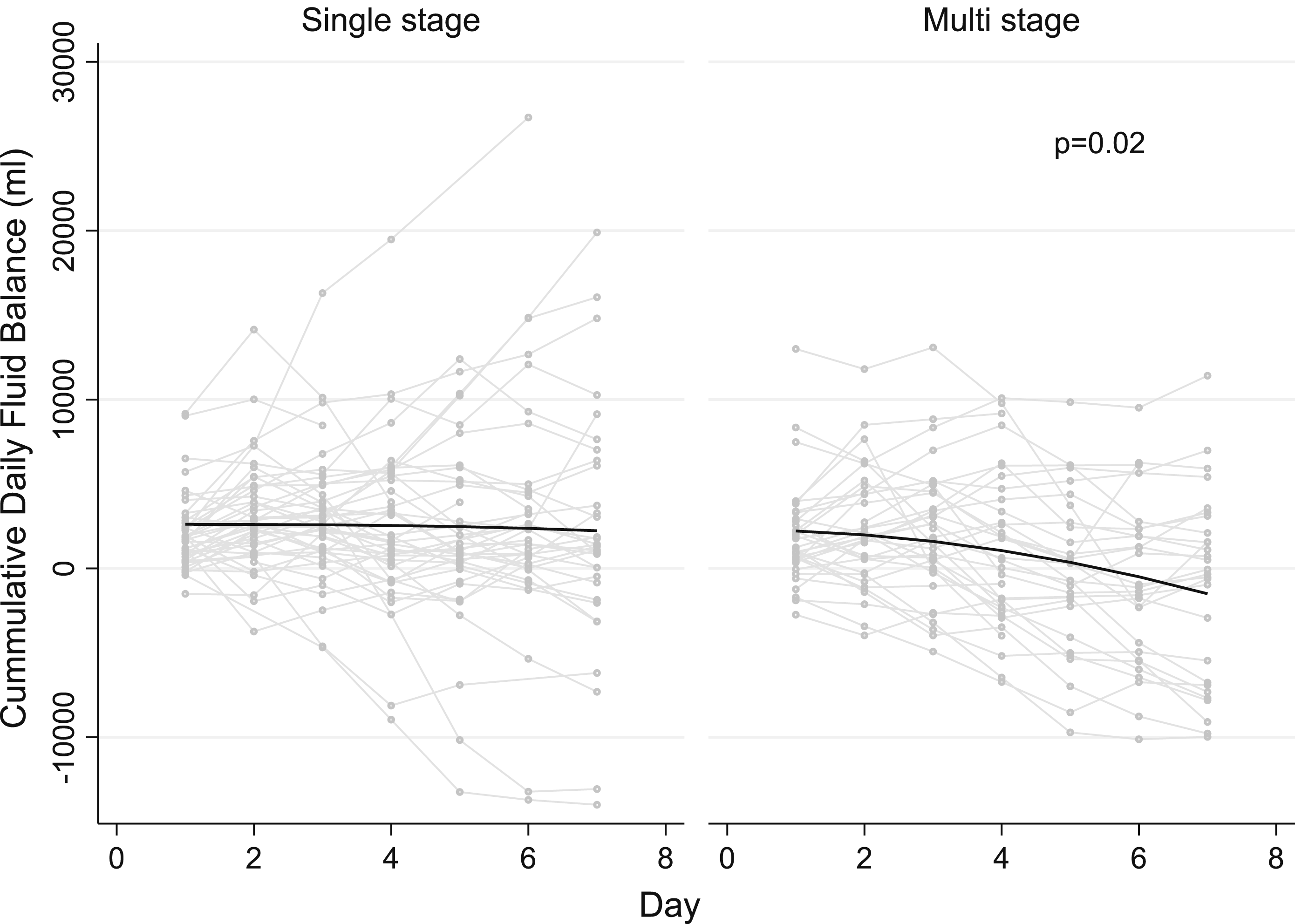
Relationship between cannula type and fluid balance adjusted analysis
Multivariable linear mixed-model after including the distance of the cannula tip from the IVC-RA junction, cannula size and SOFA score with an interaction term with cannula type and time (days) resulted in a fluid balance decrease over time by 740 mL/day (95% CI: −1360 to −118, p-interaction = .02) with the addition of a multistage drainage cannula for the first 7 days. Predicted fluid balances with 95% confidence intervals are presented in Figure 3. Cannula type also showed a statistically significant interaction with distance of cannula tip from IVC-RA junction (p interaction = .01) in our multivariable model. Adjusted daily fluid balance trajectories on VV ECMO in patients with single stage and multi stage drainage cannulas with 95% confidence intervals over first 7 days adjusted for drainage cannula size and distance form inferior vena cava-right atrial junction.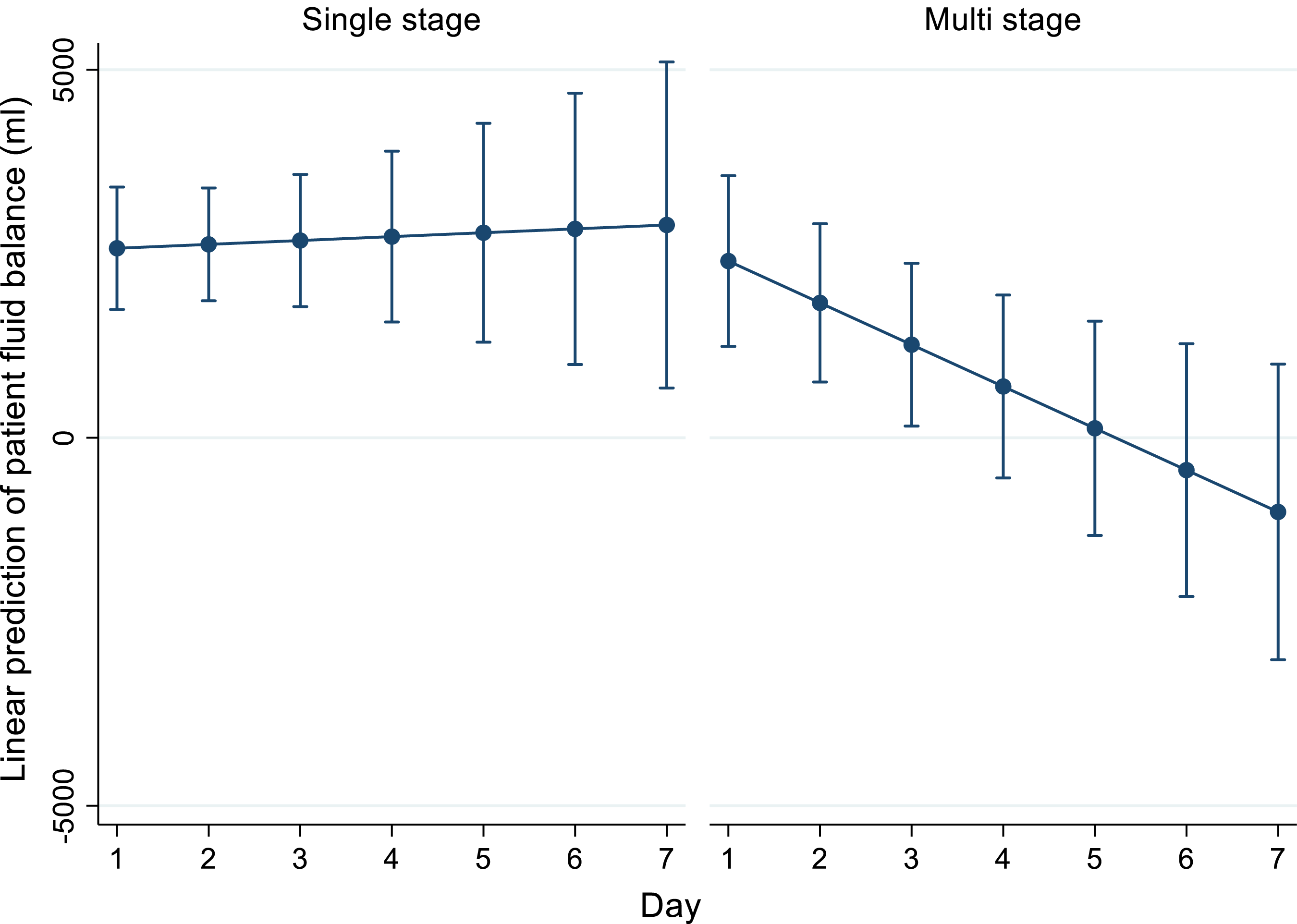
Post-hoc exploratory analysis
E-table 1 presents cumulative fluid balance by cannula type stratified by median distance from IVC-RA junction (4 cm) and E-Figure 1 presents a scatterplot of cumulative 7-day fluid balance in relation to drainage cannula distance from IVC-RA junction in both cannula types. E-Table 2 suggests that in multi-stage cannulas the larger cannulas (27 French) were able to achieve a greater negative fluid balance. We did not find a statistically or clinically significant difference in fluid balance stratified by cannula distance from IVC-RA junction.
Discussion
We present a single center historical cohort study evaluating the effect of VV ECMO drainage cannula type (single-stage vs multi-stage) on patient fluid balance. We observed that multi-stage drainage cannula use was associated with a significant reduction in fluid balance by 740 mL/day (95% CI: −1360 to −118, p-interaction = 0.02) during the first 7 days of VV ECMO. We did not find a significant effect of position of drainage cannula tip from IVC-RA junction in patients’ 7-day fluid balance in patients with single-stage or multi-stage drainage cannulas.
This is the first reported study evaluating the effects of drainage cannula types on patients’ fluid balance during VV ECMO. Chiu and colleagues showed that a positive cumulative fluid balance during the first 3 days of ECMO was independently associated with higher hospital mortality (HR 1.11 [95% CI: 1.03 to 1.20]; p = .009) in severe ARDS. 11 Fong and colleagues also showed that the cumulative fluid balance on day 7 was associated with increased hospital mortality (OR 1.17 [95% CI: 1.06 to 1.29]; p = .001). 13 Previous studies have shown the use of multi-stage cannulas may limit the shear stress applied to blood and improve flow by allowing for less negative drainage pressure. 19 Multi-stage drainage cannulas have been shown to limit recirculation fraction during VV ECMO given the separation of cannula drainage from return blood flow. 15 Our findings show that, after adjusting for size of drainage cannula, distance of cannula tip from IVC-RA junction and SOFA score, the addition of a multi-stage drainage cannula resulted in a fluid balance decrease over time by 740 mL/day (95% CI: −1360 to −118, p-interaction = 0.02) over the first 7 days of VV ECMO. E-Table 2 highlights that increases sizes of multi-stage access cannulas resulted in greater negative fluid balances.
Freckner and colleagues reported various options for positioning of drainage cannula during ECMO based on center expertise; while Fisser and colleagues hypothesize that compared with femoro-jugular configuration, jugulo-femoral configuration may result in more negative fluid balance due to improved drainage flow. 20 Banfi and colleagues recommended placement of the drainage cannula at the inferior vena cava-right atrial junction to allow for optimal drainage while avoiding potential cardiac trauma and recirculation.14,16 Wickramarachchi and colleagues showed that using computational fluid dynamics thrombosis risk varied substantially with variations of single stage cannula but was less evident with multi-stage cannulas. 21 In our cohort we attempted to characterize the effects of a patient’s fluid balance in regard to cannula positioning. We failed to show a clinically significant difference in fluid balance based on cannula distance, but this may be related to our limited sample size and limited variation in cannula distances from IVC-RA junction seen in our cohort. We believe this relationship should be explored in future work.
Our study should be viewed within the context of its limitations. Limitations of this study include our sample size which limits stratification and the fact that it is a single center historical cohort study. Most patients in our cohort presented with COVID-19 which may potentially limit extrapolation. We did not reliably capture daily patient weight, which some centres rely on instead of fluid balance a fluid loss via perspiration from membrane lung was not accounted for. We also did not capture drainage pressure and fluid loss from perspiration via membrane lung which would help to clarify our findings.
Conclusion
The use of multi-stage drainage cannulas in severe ARDS requiring VV ECMO resulted in significant reduction in fluid balance during the first 7 days of VV ECMO compared to single-stage drainage cannulas. We believe this may be clinically significant as a positive fluid balance has been shown to be associated with increase mortality in patients with severe ARDS requiring VV ECMO.
Supplemental Material
Supplemental Material - Impact of drainage cannula type on patients’ fluid balance in venovenous extracorporeal membrane oxygenation: A historical cohort study
Supplemental Material for Impact of drainage cannula type on patients’ fluid balance in venovenous extracorporeal membrane oxygenation: A historical cohort study by Sonny Thiara, Alexander Willms, George Isac, Gordon Finlayson, Hussein Kanji, Kali Romano, Cara Summers, Ryan Hoiland, Mypinder Sekhon and Donald Griesdale in Journal of Perfusion.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
Data available on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.