
Abstract
Introduction
Neurologic complications remain one of the major risks after pediatric cardiac surgery. Cerebral autoregulation (CA) is a physiologic mechanism regulating cerebral perfusion. A dynamic intraoperative evaluation can possibly detect the impairment of the cerebral regulatory function during surgery. The aim of the present study was to evaluate the utility of dynamic cerebral blood perfusion monitoring using cerebral oxygenation index (COx) as CA parameter during pediatric cardiac surgery without cardiopulmonary bypass (CPB) requiring intraoperative cross-clamping of one carotid artery to perform the procedure.
Materials and methods
Prospective intraoperative autoregulation monitoring was performed in 14 children under the age of 1 year requiring elective cardiac surgery with intraoperative cross-clamping of one of carotid artery. Procedures requiring the use of CPB and redo surgeries were excluded.
Results
Impaired CA could be measured during 33.8% of cross-clamping time on the ipsilateral side and 30.1% on the contralateral side. The difference in COx was not significant before (p = 0.7), during (p = 0.29) and after cross clamping (p = 0.63), but a significant difference in COx levels throughout the entire cohort was noted individually. The mean ABP during normal (COx <0.4) CA was 61.8 mmHg (95% CI 60.7 – 62.9) and 62.9 mmHg (95% CI 61.9 – 63.9) for cross clamped and opposite side. During impaired (COx >0.4) CA the ABP values were 58.9 mmHg (95% CI 57.7 – 60.1, p < 0.05) and 56 mmHg (95% CI 54.8 – 57.3, p < 0.05) respectively.
Conclusions
A dynamic intraoperative monitoring of CA during pediatric cardiac surgery is possible and allows to confirm the impairment of autoregulation during cross-clamping of one of the carotid arteries.
Introduction
Improvements in paediatric cardiac surgery have made the therapy of complex lesions possible and reduced dramatically the perioperative mortality. However, neurologic complications still remain one of the major risks in survivors. Despite improvements in surgical, anaesthetic and perfusion techniques the causes are not fully explained and understood. 1 Intraoperative cross-clamping of the carotid artery is required in many procedures and leads to temporary diminished regional brain perfusion which is physiologically compensated by cerebral autoregulation (CA). This homeostatic mechanism minimizes the deviations in cerebral blood flow (CBF) when cerebral perfusion pressure (CPP) changes. 2 A failure in sufficient CA can lead to cerebral ischaemia, oedema or microvascular damage. 1
A dynamic evaluation of cerebral haemodynamic is the key in the elimination of preventable factors contributing to neurological injury. 3 Near-infrared spectrometry (NIRS) is a widely applied non-invasive method that measures regional cerebral oxygen saturation (rSO2). 1 Nevertheless the cut-off values are not clear and the individual results are difficult to interpret. 1 A cerebral oximetry index (COx) has been proposed. The COx is a moving correlation between arterial blood pressure (ABP) and rSO2 and is proportional to changes in CBF. By intact CA tissue oxygen saturation is not passive to ABP and the COx fluctuates around zero. When the autoregulation capacity is reduced, the cerebral tissue oxygen saturation becomes pressure-dependent and the COx approaches +1. 4 The COx has been validated and correlates with transcranial Doppler (TCD) experimental measurements on piglet brains and in adult patients undergoing a cardiac surgery.5,6
The aim of the study was to evaluate the possibility of dynamic CBF monitoring in pediatric patients under the age of 1 year using COx as CA parameter during paediatric cardiac surgery without cardiopulmonary bypass (CPB) and requiring intraoperative cross-clamping of one of carotid artery to perform the procedure and to demonstrate the active and significant changes in CA during the procedure.
Materials and methods
A prospective intraoperative autoregulation monitoring was performed at our centre between 2015 and 2017. Included were all paediatric patients under the age of 1 year requiring cardiovascular surgery with an elective cross-clamping of the one of the carotid arteries. Procedures requiring the use of CPB and redo surgeries were excluded. Written informed consent to participate in this study was obtained from both parents before the procedure. The study was approved by the local ethical committee (Permission-No. 294/2014BO1).
Procedure
All procedures were performed under general anaesthesia and under systemic heparinization with a bolus of 100 units per every kg of the body weight. The surgical correction of aortic coarctation (CoA) was performed through a left thoracotomy. During the procedure a cross-clamping of the left common carotid artery for the time of the anastomosis. The surgical implantation of modified Blalock-Taussig Shunt (BT) was performed through a median sternotomy including a cross clamp of the right common carotid artery for the time of anastomosing the shunt.
An invasive measurement of ABP was performed as standard perioperative care at our institution at the time of the study and blood pressure management was performed exclusively by attending anaesthetist.
Autoregulation monitoring
A direct bilateral cerebral measure of rSO2 with the INVOS system (INVOS 5100C, Somanetics Corporation, Troy, MI, USA) was added to invasive measurement of ABP. The invasive ABP measurements were performed though a catheter in the right radial artery in CoA and in the left radial artery in BT patients. All data were captured online and converted from analog-to-digital via a MPR 1 Datalogger (Raumedic AG, Helmbrechts, Germany) and analysed by ICM + software (Cambridge University Enterprise, Cambridge, UK) so the COx values for both sides could be calculated continuously. Distorted values, mostly from loss of arterial signal due to blood sampling, were removed manually. The COx is an index calculated by a correlation coefficient between rSO2 and ABP. Intact CA leads to no or negative correlation and an impaired CA results in positive increase of the COx value. Lower limit of pressure autoregulation (LLA) was chosen at a value of 0.4, according to former studies. 4 Above that level the CA was interpreted as lost and passive to changes in ABP. The intraoperative values of Cox didn’t influence the course of the surgery and were not available to the clinicians to avoid any confusion.
The course of every surgery was divided into three periods: pre-clamp period (from the surgical incision until clamping), clamp period and post-clamp period (after release of blood flow until the end of the surgery) periods. COx was determined continuously with 10-s intervals.
The values of COx measurements were obtained in real time and recorded for further evaluation.
Statistical analysis
A pressure autoregulation curve was constructed for each patient by binning and averaging both ipsilateral and contralateral COx values according to the average ABP. Lower limit of pressure autoregulation (LLA) was chosen at a value of 0.4, according to former studies. 4 The mean ABP was determined for COx values of below and over 0.4. A composite pressure autoregulation curve was constructed similarly to previous publications by summarizing each subject’s COx-MAP histograms into a mean of means for the entire cohort with equal weight assigned to individual subjects. 4 All obtained data were analysed using SPSS Statistics 26 (IBM Corporation, Armonk, NY, USA). Continuous data are presented as mean (+/− SD) and categorical variables are shown as absolute numbers and percentages. Continuous variables were tested for equality of variances by Levene’s test. Normal distributed variables were compared using the unpaired or paired t test. In other cases, Mann-Whitney U test was performed. Nominal variables were tested with Fisher’s exact test. p values <0.05 were considered as statistically significant.
Results
Characteristics of study population.
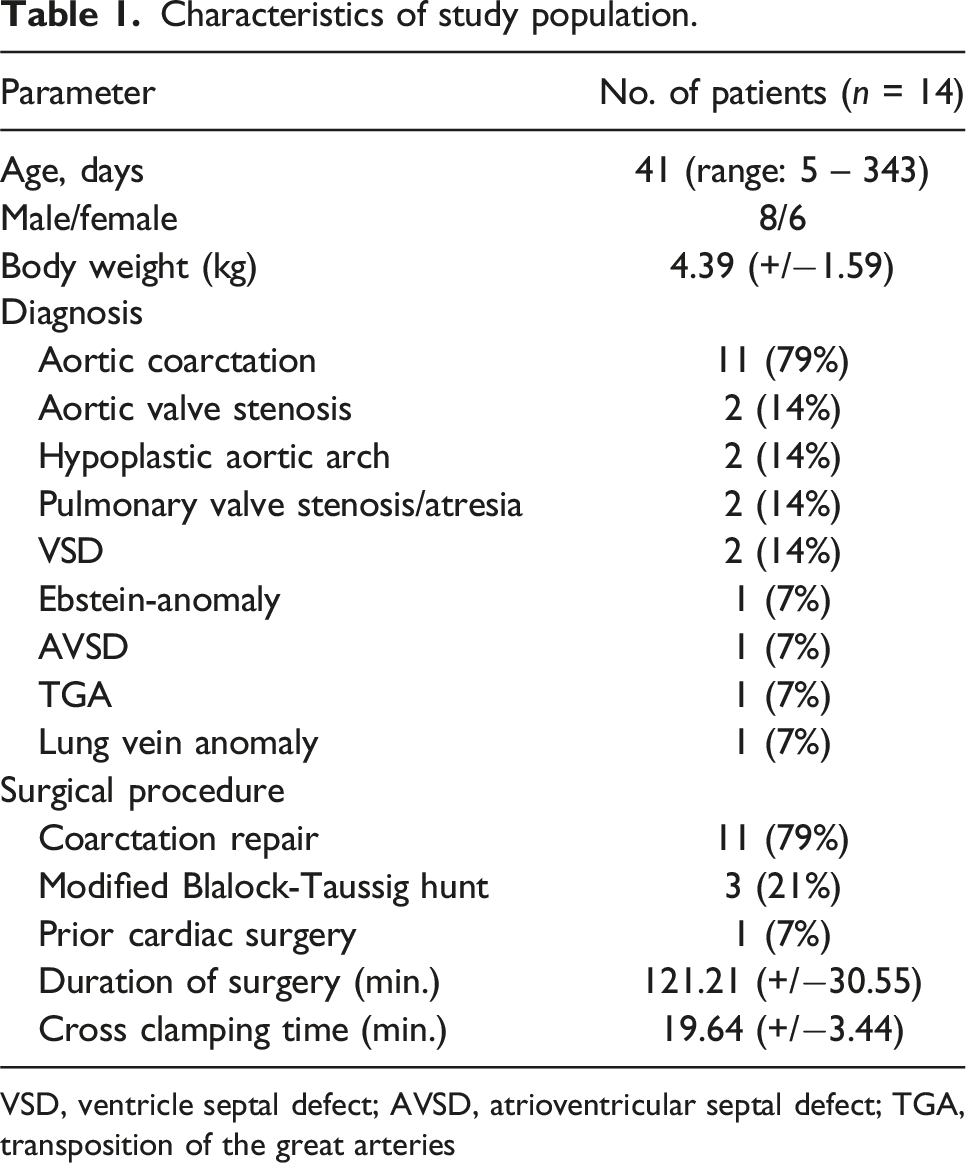
VSD, ventricle septal defect; AVSD, atrioventricular septal defect; TGA, transposition of the great arteries
A beating heart surgery was performed in every case and there was no intraoperative conversion to CPB in any of the patients. No need for urgent postoperative re-exploration or catheter intervention, in-hospital mortality or major bleeding was observed. In one case of coarctation repair a scheduled surgery was performed after arterial switch operation for transposition of the great arteries on elective readmission. We didn’t encounter any neurologic complications in the study population.
Mean ABP for the cohort was 58+/−4 mmHg, 62+/−4 mmHg and 59+/−3 mmHg: before, during and after cross clamping, respectively. Overall results showed no change in rSO2 on the cross clamped side: from 64.3% (95% CI 56.5 to 72.2) to 62.4% (95% CI 54.2 to 70.5, p = 0.8) and no change in rSO2 on the contralateral side from 64.9% (95% CI 56.9 to 72.9) to 72% (95% CI 62.1 to 81.9, p = 0.06) during cross clamping. After release of the blood flow the observed rSO2 returned to 62.3% (95% CI 52.4 to 72.2, p = 0.7) on the declamped and to 63.73% (95% CI 53.5 to 73.9, p = 0.09) on the contralateral side. Observed COx before cross clamping was 0.07 (95% CI −0.05 to 0.18) and 0.03 (95% CI −0.08 to 0.14) on the ipsilateral and contralateral side respectively. During cross clamping the ipsilateral side showed an increase of COx to 0.24 (95% CI 0.11 to 0.37, p = 0.06) and the COx on the contralateral side increased to 0.11 (95% CI -0.05 to 0.26, p = 0.32). After declamping the COx levels fall to 0.14 (95% CI -0.02 to 0.31, p = 0.37) on the clamped side and to 0.1 (95% CI -0.04 to 0.24, p = 0.68) on the opposite side. There was no case of recorded impaired autoregulation that happened bilaterally.
The measurements at the end of the surgery didn’t vary significantly compared to baseline values. The mean rSO2 was slightly reduced by mean of 2% (p = 0.82) on the clamped side and by mean of 1.17% (p = 0.71) on the contralateral side. The difference in COx was +0.07 (p = 0.55) on the ipsilateral and +0.07 (p = 0.40) on the contralateral side. All changes of Cox observed during the cross clamp period were linear.
The values of rSO2 and COx varied between both sides. There was no significant difference in rSO2 before (p = 0.78) and after (p = 0.93) cross clamping, only the difference during cross clamping was significant (p = 0.008) with rSO2 of the cross-clamped side being 13.3 % lower than on the contralateral side. The difference in COx was not significant before (p = 0.7), during (p = 0.29) and after cross clamping (p = 0.63). Mean ABP, rSO2 and COx results for the entire cohort, categorized by surgical stage and clamping side, are shown in Figure 1. Mean ABP, rSO2 and COx results during pre-clamp, clamping and post-clamp period of a cardiovascular surgery.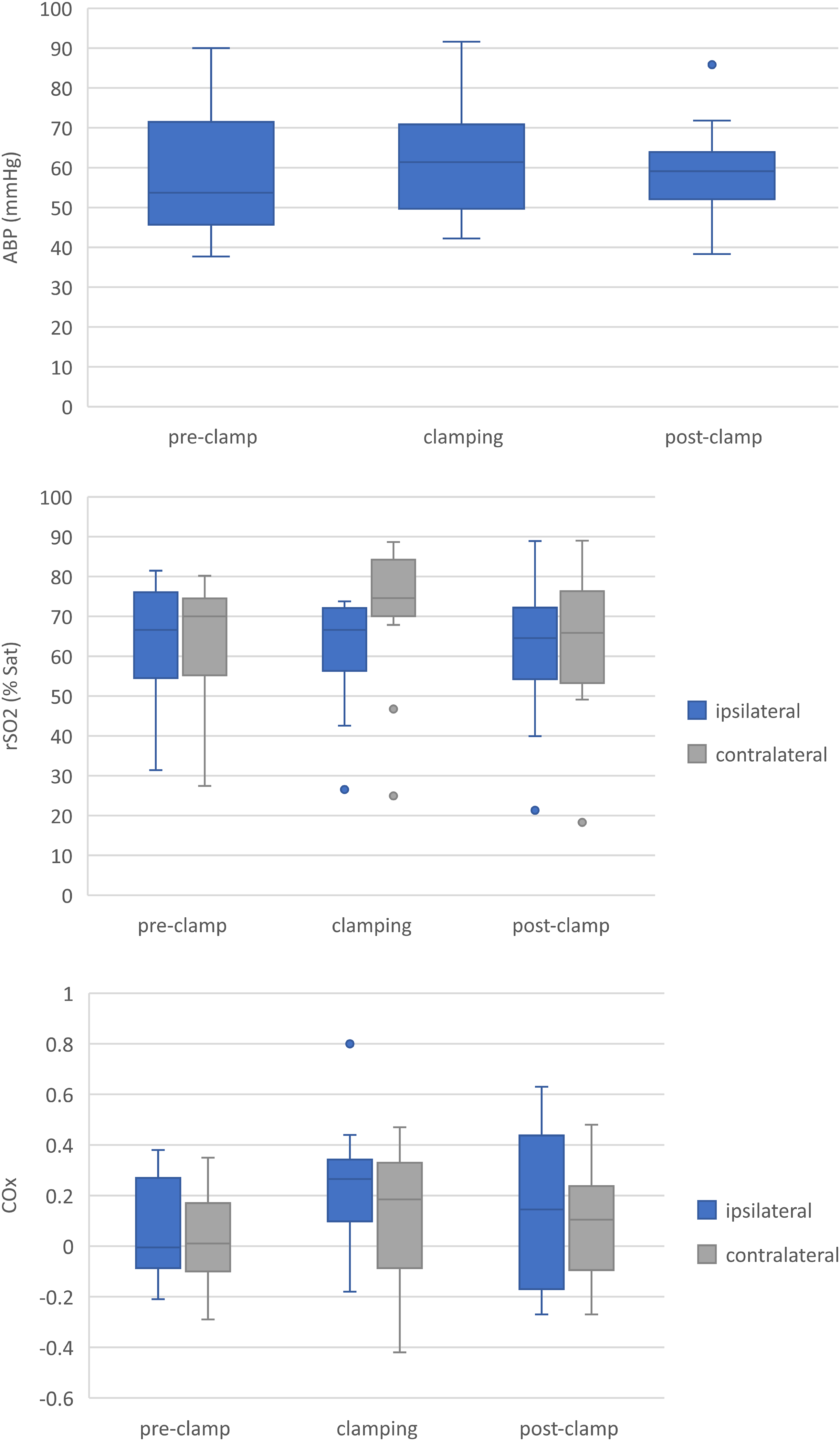
Figure 2 shows a focused individual analysis depicting a significant difference in COx levels throughout the entire cohort. Overall, an impaired autoregulation could be measured during 33.8% of cross-clamping time on the ipsilateral side and 30.1% on the contralateral side. For the cross-clamped side the impaired autoregulation was observed for <25% of the clamping time in 4 (29%) patients and for >50% in 3 (21%) patients. For the contralateral side in 5 (36%) individuals the autoregulation was impaired for <25% of time and for 3 (21%) for >50%. Focused individual analysis of COx levels of entire cohort during cross clamping.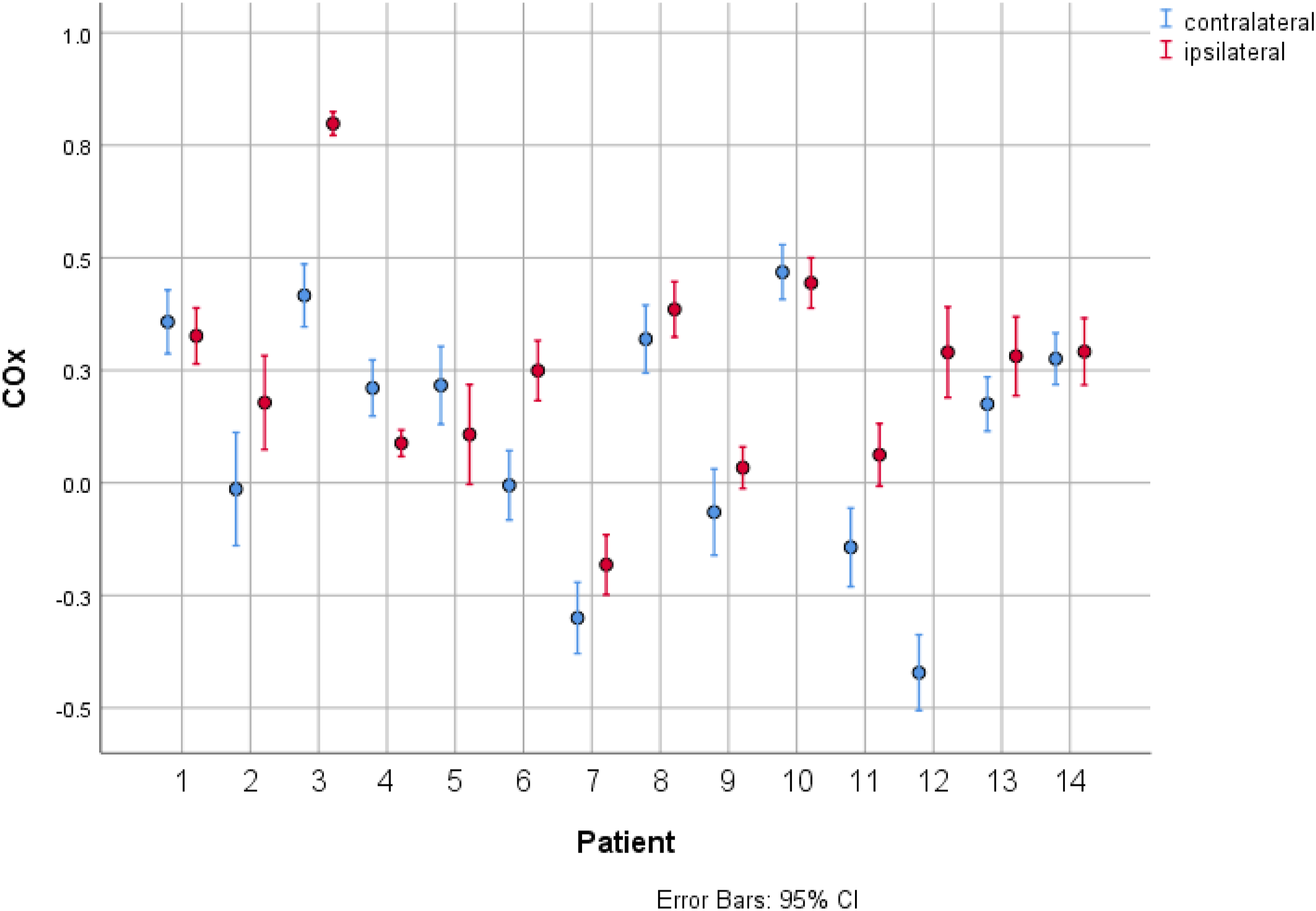
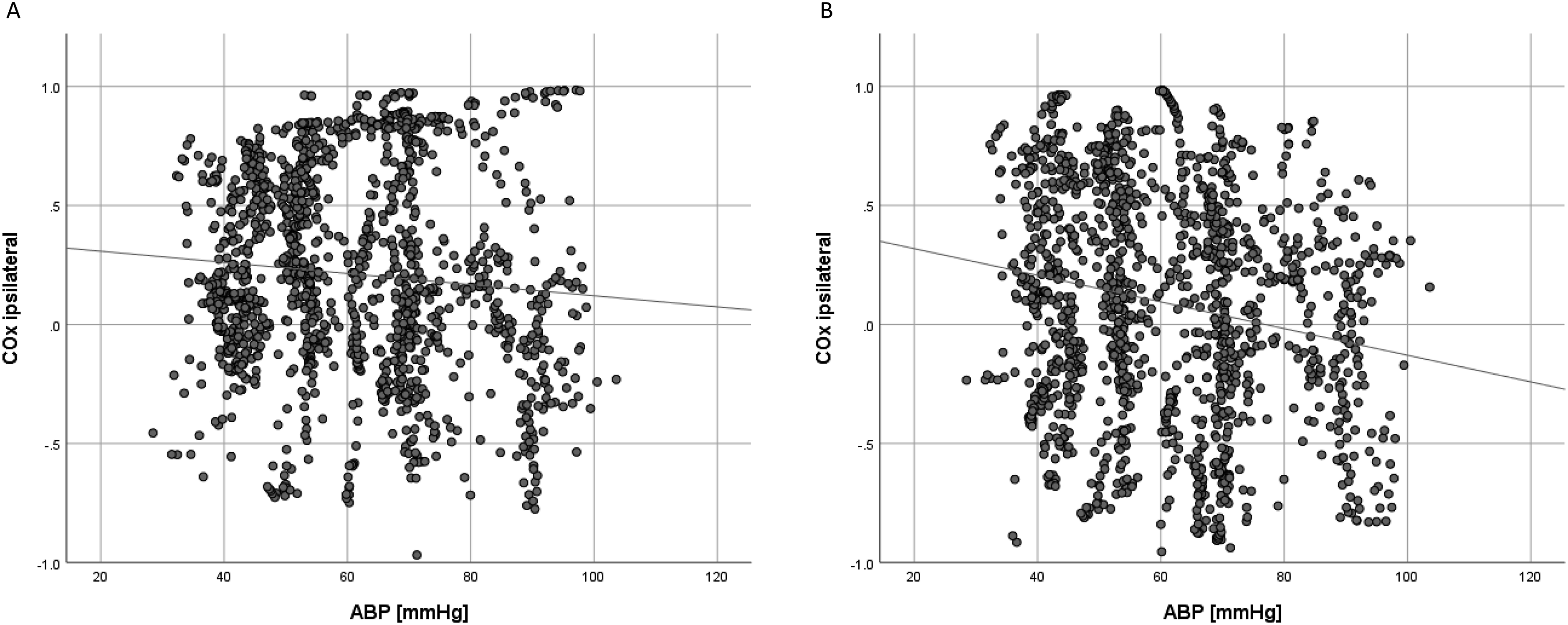
The association of ABP and COx across binned mean values allows the visualisation of the cohort autoregulation curve (Figure 3). The curve shows the impairment of pressure autoregulation with hypotension. The mean ABP during normal (COx <0.4) autoregulation was 61.8 mmHg (95% CI 60.7 – 62.9) and 62.9 mmHg (95% CI 61.9 – 63.9) for cross clamped and opposite side, respectively. During impaired (COx >0.4) autoregulation the ABP values were 58.9 mmHg (95% CI 57.7 – 60.1, p < 0.05) and 56 mmHg (95% CI 54.8 – 57.3, p < 0.05) respectively. There were significant negative correlations between COx and ABP for both sides during cross clamping (Figure 4). The distribution of the COx across binned mean ABP for ipsilateral and contralateral during cross clamping. Correlation between cerebral oximetry index (COx) of ipsilateral (A) and contralateral (B) side and arterial blood pressure. Pearson correlation coefficient r = −0.085; p < 0.05 and r = −0.2; p < 0.05 for ipsilateral and contralateral side respectively.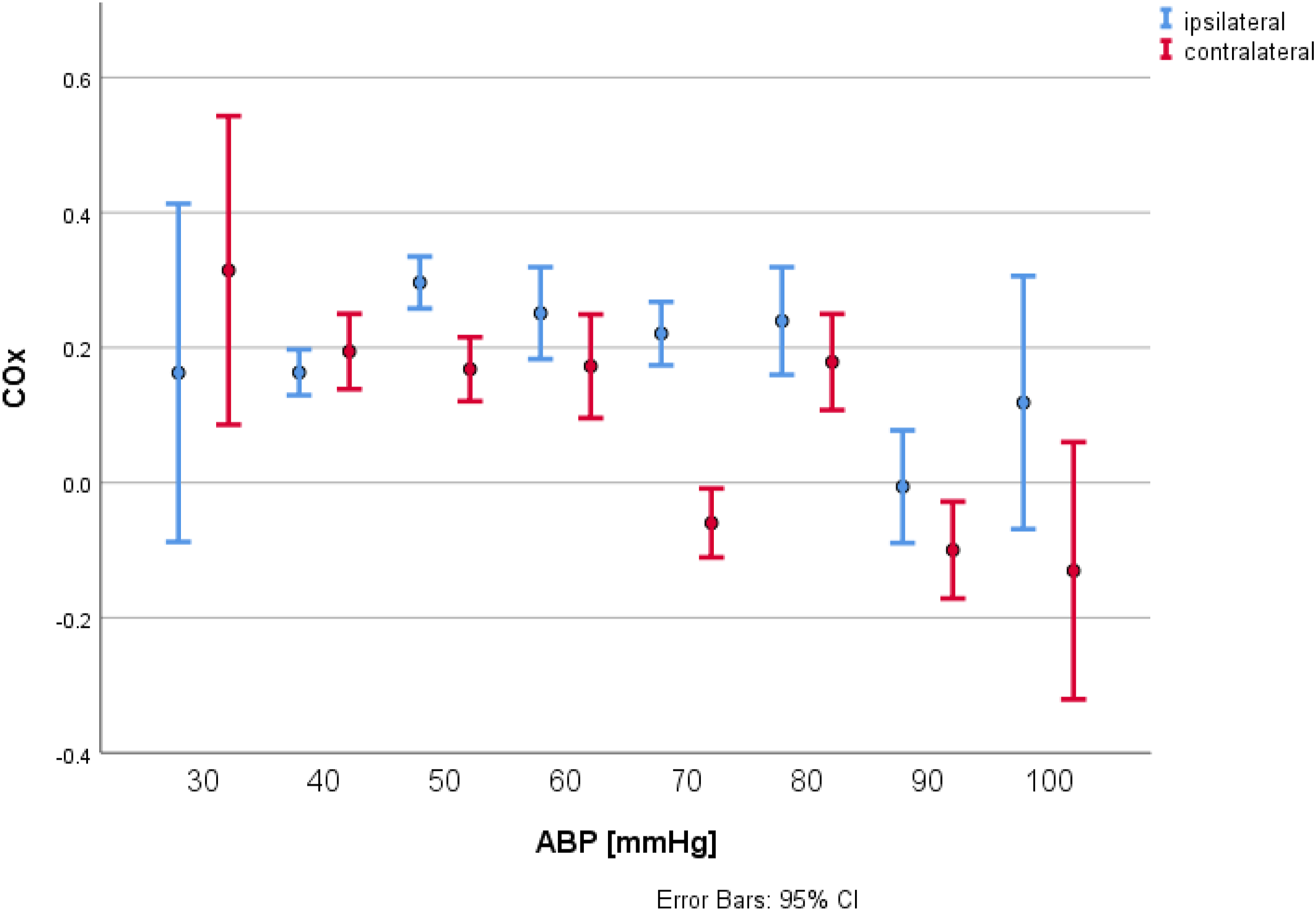
Discussion
COx represents the interaction of rSO2 and ABP and the changes in rSO2 are proportional to changes in CBF.2,4 Thereby, impaired CA leads to passivity of the cerebral tissue oxygen saturation regarding ABP changes and the COx approaches +1. According to former studies a COx threshold of 0.4 is described as a limit of intact autoregulation. 4 The present article reports a method to monitor CA continuously with ABP and NIRS in pediatric patients during cardiac surgery without CPB and shows the blood pressure dependency of the autoregulation during cardiovascular surgery of the infants.
The relationship of the mean COX between cross-clamped and opposite side of the cerebrum varied significantly during the operation, whereas our data showed no significant ipsilateral difference (p = 0.06) regarding autoregulation at baseline, before cross-clamping and at declamping of the carotid artery. The pediatric data analysed by Brady at al. regarding CA in pediatric patients during cardiac surgery with the use of CPB showed a significant relationship between COx and the mean ABP and allowed to calculate an individual CA threshold in 77% of patients at a level of 42+/−7 mmHg. 4 Furthermore, in our study of patients a significant drop in ABP was associated with impaired CA (COX >0.4) on both ipsilateral and contralateral side (p < .05). As shown in Figure 4 a relevant correlation in autoregulation depending on ABP for both sides could be detected.
The feasibility of CA monitoring has been already proven in neurosurgical intensive care patients and after optimization of ABP within the autoregulatory range the outcome could be improved.7,8 In the analysis of Caldas et al. the intraoperative changes in CA could be reported in 17 of 20 studies concerning cardiac surgery with CPB in adult patients. 1 Cerebral hypoperfusion due to impaired autoregulation has been suggested as the mechanism associated with a higher incidence of postoperative delirium, cognitive decline and stroke but the actual results are conflicting.1,9,10
According to our results an effective monitoring of CA depending on online calculation of COx from ABP and rSO2 during cardiac surgery is possible. Previous works tried to find ABP thresholds for optimal autoregulation.4,11 Unfortunately, a threshold value couldn’t be statistically calculated in every patient and was not available in critical moment of the surgery. Hayashida et al. proved, that the autoregulation mechanisms can be immature in children under the age of 4 years and are more likely to have transient cerebral ischaemia caused by acute hypotension during cardiac surgery. 12 Our work elucidates that an impaired autoregulation can be successfully detected and dynamically monitored, creating the possibility to react during a short but vulnerable phase of cerebral malperfusion during cross-clamping of carotid artery, as the COx values at baseline and after cross-clamping didn’t show any significant difference (p = .55 and p = 0.4). Furthermore, a dynamic and on-line monitoring of CA creates the possibility to guide an individual therapy in each individual case and distinguish between volume therapy and pressors. Autoregulation driven blood pressure management may be an instrument, when added to surgical and anaesthesiologic practice, to reduce the risk of neurological complications after cardiac surgery in paediatric patients.
Limitations
The small size of the study population limited the statistical analysis and didn’t allow us to calculate the thresholds of ABP in every patient. Furthermore, we didn’t observe any neurological complications in our cohort, what, apart from potential disastrous implications for patient, could help us better understand the fluctuations of Cox intraoperatively.
Conclusion
A real-time intraoperative monitoring of CA during pediatric cardiac surgery is feasible and allows to confirm the impairment of autoregulation during cross-clamping of one of the hemispheres. Further studies are needed to evaluate the impact of autoregulation loss on perioperative neurocognitive outcome. Further studies to investigate the feasibility of a NIRS/autoregulation driven blood pressure management are also required.
Footnotes
Author’s note
Presented during the 8th World Congress of Pediatric Cardiology and Cardiac Surgery in Washington DC, USA on 30th August 2023.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Study received financial support from the foundation “