
Abstract
Performing cardiac surgery on patients with bleeding diatheses poses significant challenges since these patients are at an increased risk for complications secondary to excessive bleeding. Despite its rarity, patients with factor VII (FVII) deficiency may require invasive procedures such as cardiac surgery. However, we lack guidelines on their pre-, peri-, and post-operative management. As FVII deficiency is rare, it seems unlikely to design and learn from large clinical studies. Instead, we need to base our clinical decision-making on single reported cases and registry data. Herein, we present the rare case of a patient with FVII deficiency who underwent double valve surgery. Pre-operatively, activated recombinant FVII (rFVIIa) was administered to reduce the risk of bleeding. Nevertheless, the patient experienced major bleeding. This case highlights the significance of FVII deficiency in patients undergoing cardiac surgery and emphasizes the importance of adequate and appropriate transfusion of blood products for these patients.
Keywords
Introduction
Factor VII (FVII) deficiency is one of several rare bleeding disorders (RBD). It can be inherited or acquired, and shows the highest prevalence among congenital coagulation disorders with 1 in 500,000 people.1,2 FVII is a vitamin K dependent zymogen involved in the initiation of coagulation in the extrinsic pathway of the coagulation cascade. Circulating FVII and membrane protein tissue factor (TF) build a complex and become activated FVII (FVIIa), which further facilitates hemostasis. FVII has a short half-life (3-6 h) with approximately 1% circulating as FVIIa. 3 Managing patients with FVII deficiency is challenging. FVII can be present in different forms and is potentially detectable by various methods.4,5 Usually, FVII activity is measured in blood plasma, but FVII activity does not correlate with the risk of bleeding. 6 This results in difficulties in assessing the severity of the disease based on FVII activity. For instance, mild deficiencies can lead to major bleeding complications, while patients with severe reduction of FVII activity may never experience bleeding events. 6 Typically, standard hemostatic blood tests demonstrate prolonged prothrombin time (PT) and elevated international normalized ratio (INR) but normal activated partial thromboplastin time (aPTT). 1 Discrepancy between bleeding and low FVII deficiency may also relate to the assay use of TF. FVII variants have been reported to have inaccurate values based on TF from rabbits or bovine sources. 3
Minor surgeries in patients with FVII deficiency seem not to require treatment if there is no history of severe bleeding. 7 Groups have suggested that plasma FVII activity greater than 10% combined with no prior severe bleeding is sufficient in patients undergoing an operation that carries a high risk of major bleeding. 8 In cardiac surgery, the systemic administration of heparin and institution of cardiopulmonary bypass (CPB) create more complexity for the intra-operative and post-operative management of patients with FVII deficiency. Long surgical times and comorbidities that require anticoagulation in these patients further complicate the clinical decision-making. To date, there are no recommendations for patients with reduced FVII activity who undergo cardiac surgery.
Herein, we present the rare and unique case of a patient with FVII deficiency and reduced FVII activity who underwent double valve surgery. In addition to a pre-operative diagnosis of atrial fibrillation, requiring anticoagulation, the patient experienced major post-operative bleeding. Our experience should add to the limited literature on FVII deficiency in patients undergoing cardiac surgery.
Case Report
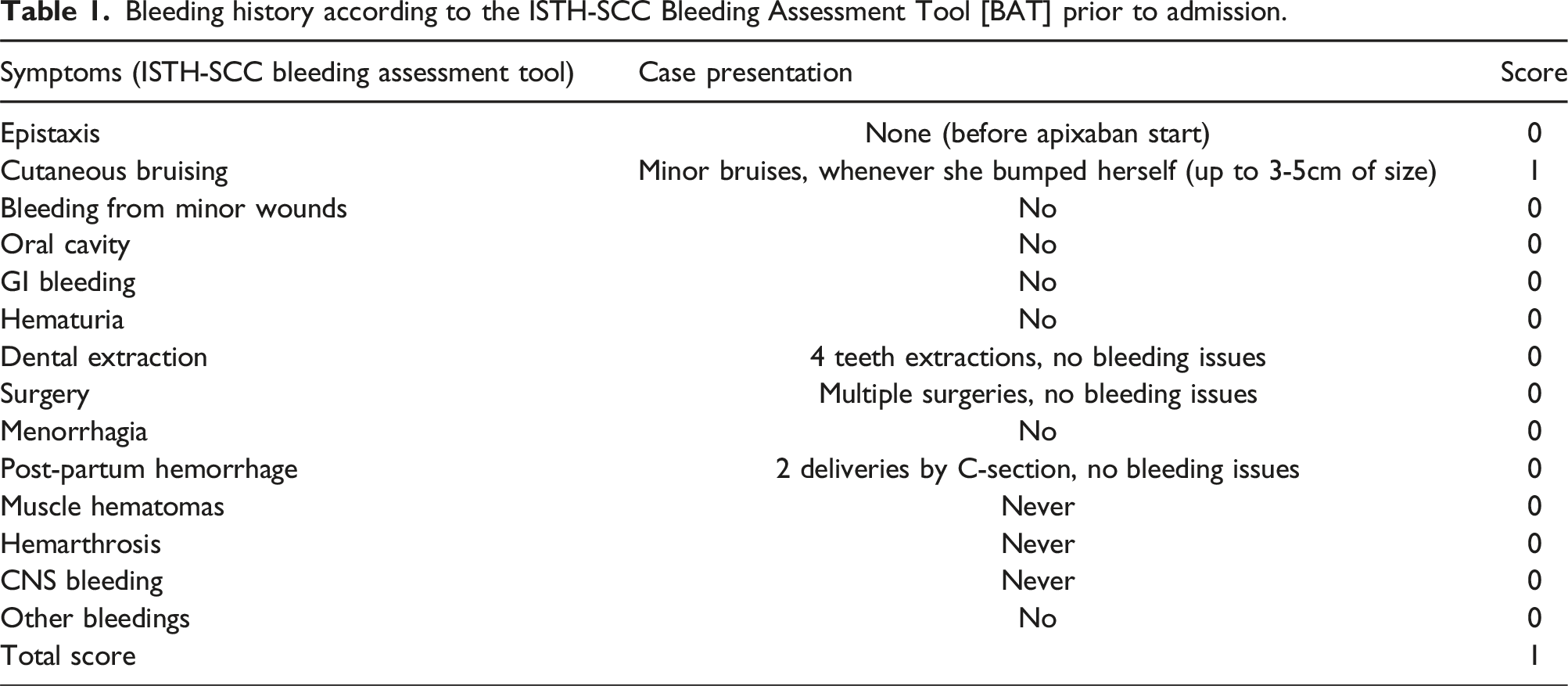
Bleeding history according to the ISTH-SCC Bleeding Assessment Tool [BAT] prior to admission.
Once she was started on apixaban for AF, her INR continued to rise (Figure 1). It reached a maximum of 3.6 a few days before surgery, leading to easy bruises and one episode of epistaxis. Although her apixaban was stopped 72 h prior to surgery, and while she was given Vitamin K and fresh frozen plasma (FFP), the INR was persistently elevated (Figure 1). One day before surgery a FVII activity of 14% and anti-Xa levels of 41 ng/mL were measured (Figure 1). Intra-operatively, 3 doses of activated recombinant FVII (rVIIa) (120 µg/kg for each dose), 2 units of FFP, 1 unit of platelets, four doses of prothrombin complex concentrate (PCC), and five packs of red blood cells (pRBCs) were given (Figure 1). Heparin was given intra-operatively to maintain an activating clotting time greater that 480 s throughout the surgery and the patient underwent mitral valve replacement with a bioprosthetic and tricuspid valve repair. Cross-clamp and CPB times were 79 min and 94 min, respectively. Timeline demonstrating relevant hemostatic blood test measurements including FVII activity and international normalized ratio (INR) as well as presentation of transfusion products. FVII = Factor VII, INR = International normalized ratio, Vit K = Vitamin K, rFVIIa = Recombinant activated factor VII, FFP = Fresh frozen plasma, PCC = Prothrombin complex concentrate, pRBCs = Packs of red blood cells, ICU = Intensive care unit.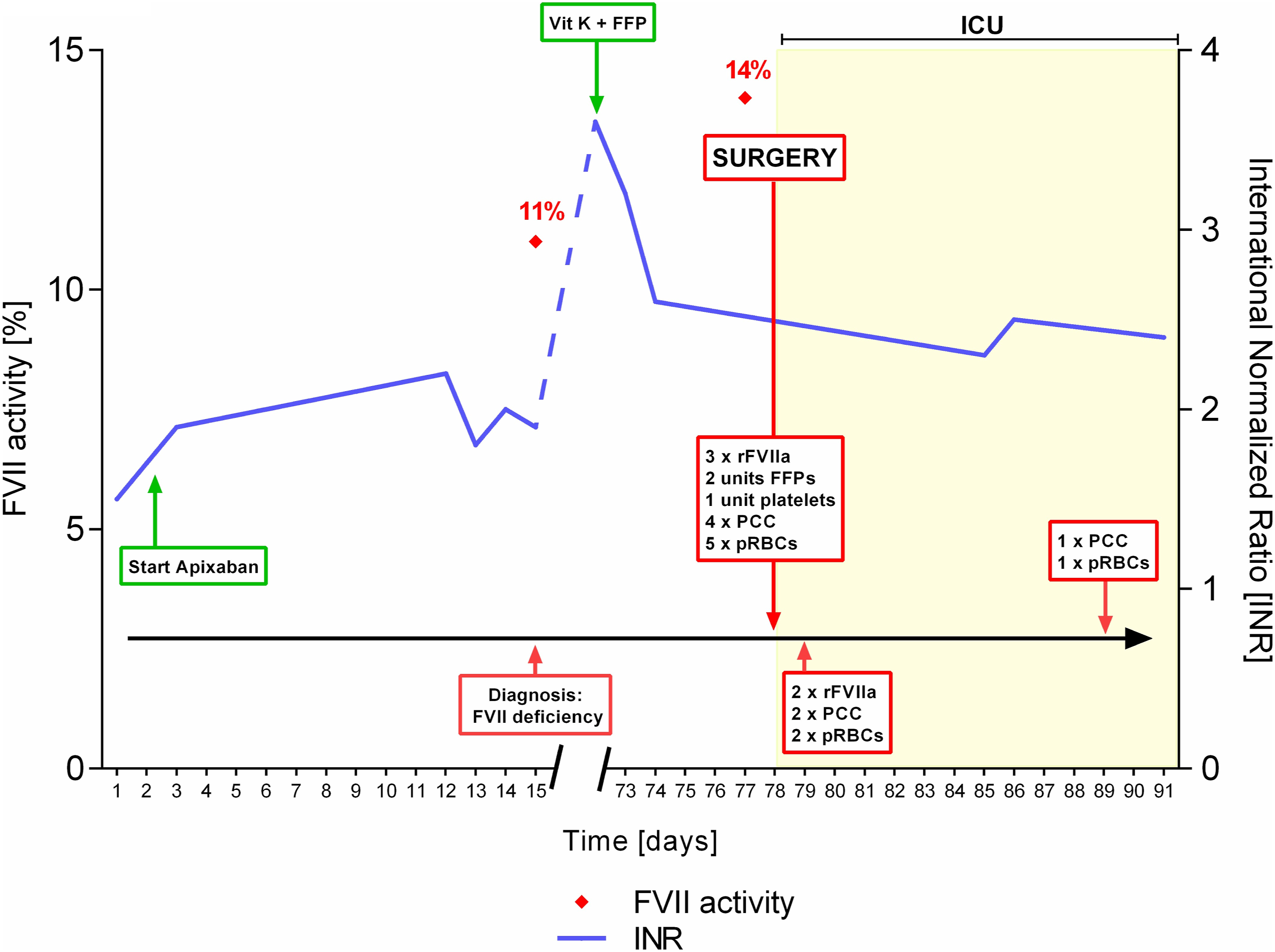
After the operation, the patient had extensive bleeding (approximately 2L in the chest tube reservoir), requiring 2 units of pRBCs, 2 doses of rFVIIa (120 µg/kg for each dose), and 2 doses (each dose was equivalent to 2000 international units) of PCC over the first 48-h after surgery (Figure 1). The patient’s post-operative course was further complicated by respiratory failure secondary to hospital acquired pneumonia, necessitating prolonged mechanical ventilation. The patient was extubated on post-operative day 8. She received 1 unit of pRBCs and 1 dose of PCC on post-operative day 11 (Figure 1). She was discharged to home 17 days after her double valve surgery. On 2-years follow-up, echocardiography shows normal bi-ventricular function, no residual mitral regurgitation, and mild tricuspid regurgitation. She is independent in her activities of daily living. Her medications include apixaban for AF, and bruising easily has been her only hematological symptom.
Discussion
Factor VII deficiency is a rare coagulation defect that increases the likelihood of major bleeding. While there is a correlation between bleeding tendency and FVII levels with severe deficiencies of <1%, FVII activity is not always associated with bleeding in high-risk procedures such as cardiac surgery. Moreover, it is imperative that patients with known or suspected FVII deficiency undergo genetic testing to accurately determine whether FVII deficiency is congenital or acquired. Herein, we present the first description of a combined double valve surgery in a patient with FVII deficiency. This case demonstrates that despite no prior history of major bleeding, pre-operative optimization, and a normal ISTH Bleeding Score, the patient experienced significant bleeding. It is important to emphasize that the patient did not have genetic testing for FVII deficiency and there was no correction in her FVII level with Vitamin K replacement. Her management was further complicated since she required long-term anticoagulation for AF. In addition, given her liver disease, the risk of bleeding due to FVII deficiency was likely worsened by hyperfibrinolysis. Given her bleeding after the operation, the patient may have likely benefitted from 24 to 48 h of rFVIIa infusion post-operatively.
To date, there are no clear recommendations for anticoagulation strategies in patients with FVII deficiency undergoing cardiac surgery. Peri-operative management involves restoring FVIIa using recombinant or plasma derived FVII. Recombinant FVIIa has a rapid effect with peak levels achieved within 5 min and lasting for 4 hours. Plasma derived FVII has a delayed profile achieving peak activity after 60 min and lasting for 6 hours. 3 Generally, the British Committee for Standards in Hematology recommends giving rFVIIa 15–30 µg/kg repeated every 4–6 h with a minimum of three doses for major surgeries in higher bleeding risk cases. 11
Administration of rFVIIa in patients with FVII deficiency is not trivial. There are cases of thromboembolism reported in patients with FVII deficiency who received rFVIIa.12,13 Moreover, thromboembolic events have been noted in 3%–4% of patients with FVII deficiency. 14 Strategies for FVII replacement during cardiac surgery is limited to case reports. The majority of cases received intra-operative FVII replacement; however, there is variability in the use of pre-operative FVII replacement and the duration of FVII replacement post-operatively in the absence of bleeding.15,16 The safety and feasibility of high-risk cardiac surgery in patients with FVII deficiency has been demonstrated in previous cases.17,18 However, due to the rarity of this bleeding disorder, it is unlikely to find robust data and evidence supporting a universal management strategy for patients with FVII deficiency who are undergoing cardiac surgery. Therefore, single cases such as this one and the few other reported ones can be used to offer experiential evidence for managing these patients.
Conclusion
Factor VII deficiency is a rare coagulation defect that can result in serious bleeding complications. In cardiac surgery, long surgical times, the administration of heparin, and the institution of CPB, lead to a higher risk for severe intra- and post-operative bleeding. To date, there are no clear recommendations on the specific care of patients with FVII deficiency that undergo cardiac surgery. For the first time, we discuss the clinical management of a patient with FVII deficiency who received double valve surgery. This case was complicated by severe bleeding despite only mildly reduced FVII activity and adequate pre-operative medical optimization. Although the patient may have been under-treated post-operatively, so it is important to maintain a high level of suspicion for adequate administration of rFVIIa. Our experience can be added to the small body of literature surrounding patients with FVII deficiency who require invasive surgical procedures such as cardiac surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient provided informed consent for the preparation and publication of this case.