
Abstract
The rising application of extracorporeal membrane oxygenation (ECMO) has emphasized the need for consistent and standardized terminology, especially concerning peripheral percutaneous cannulation of the pulmonary artery (PPC-PA). The Extracorporeal Life Support Organization (ELSO) Nomenclature Task Force produced the ELSO Maastricht Treaty for extracorporeal life support (ECLS) Nomenclature to address this challenge. However, adherence to nomenclature recommendations has been poor in publications describing PPC-PA. We aim to describe common nomenclature errors and provide a user-guide for abbreviations that can be used by authors, reviewers, and journal staff to ensure properadherence to standardized nomenclature in publications describing PPC-PA.
Keywords
Introduction
The growing indications for, and use of, extracorporeal membrane oxygenation (ECMO) have spurred innovation in this field. As novel techniques, indications, and devices are presented in the literature, it becomes increasingly important to communicate in a clear and uniform manner. Standardized nomenclature plays a crucial role in facilitating effective communication and collaboration among healthcare professionals and researchers. However, there is growing concern regarding poor adherence to standardized nomenclature,1–3 particularly regarding peripheral percutaneous cannulation of the pulmonary artery (PPC-PA) 1 for ECMO. In this article, we aim to briefly describe PPC-PA, provide a background of standardized ECMO nomenclature, discuss the current scope of the problem of poor nomenclature adherence and potential implications, and provide a guide for clinicians and researchers regarding PPC-PA for ECMO nomenclature and abbreviations.
Peripheral percutaneous cannulation of the pulmonary artery
PPC-PA can be accomplished using either a single-lumen cannula (e.g., Medtronic Bio-Medicus® [Medtronic, Minneapolis, U.S.]) for return or specialized dual-lumen cannulae, such as the ProtekDuo® (LivaNova, London, U.K.) and the Spectrum Dual Lumen Cannula (Spectrum Medical, Gloucester, U.K.), which are specifically designed for placement in the main pulmonary artery (PA) and can be used for both drainage and return. In the context of ECMO, PPC-PA is a critical part of the primary venopulmonary (VP) ECMO mode, 1 hybrid modes for patients requiring enhanced or multiorgan support when a single mode alone is not adequate,4,5 and dynamic strategies for patients with evolving support requirements.6,7
The diverse application of PPC-PA in ECMO, though clinically useful, presents a potential complication if the language employed to describe methods and results lacks standardization, thereby risking a significant hindrance to scientific progress. Aware of the confusion that inconsistent or unclear terminology in the literature can provoke, the Extracorporeal Life Support Organization (ELSO) took a definitive step years ago by initiating the creation of a consensus document on extracorporeal life support (ECLS) nomenclature, effectively addressing these challenges.2,3
Background of standardized extracorporeal membrane oxygenation nomenclature
In 2017, the ELSO Nomenclature Task Force (NTF) convened at the Sixth EuroELSO congress in Maastricht, The Netherlands to unify ECLS nomenclature. The resulting two-part document, the ELSO Maastricht Treaty for ECLS Nomenclature (ELSO Maastricht Treaty), formalizes the nomenclature and abbreviations for ECLS modes and cannulation configurations. The cannulation nomenclature evolves from a basic configuration (level 1) to a highly detailed description, encompassing the location of the cannulated vessel (level 2), the position of the cannula tip (level 3), and cannula size (level 4).2,3 This document serves as a significant milestone in standardizing language in the field. Despite the importance of these recommendations, their adoption has been disappointingly low in academic publications, particularly in relation to ECMO procedures utilizing PPC-PA.
Adherence to standardized nomenclature in the literature
To evaluate the adherence to the ELSO Maastricht Treaty in published manuscripts discussing the utilization of a peripherally inserted percutaneous cannula for ECMO drainage or return in the PA, we performed a systematic search on PubMed. The search spanned from 01 January 2019 to 08 June 2023, and focused on English language articles. Employing a structured approach, we used MeSH terms, textwords, and relevant synonyms to enhance sensitivity. A total of 247 articles were identified, 243 by the database search and four by examination of reference lists in published manuscripts. Using two reviewers, the articles were screened and assessed for eligibility, excluding those with author conflicts, incorrect device or configuration usage, no identification or discussion of oxygenator use, lack of relevance, or classified as commentaries. As a result, 184 articles were excluded, leaving 63 for the final review (Supplementary File).
Overall, the number of publications describing PPC-PA has increased over the specified time period. Among the articles undergoing full-text review, only two (3%) consistently used correct abbreviations and nomenclature to describe PPC-PA as recommended in the ELSO Maastricht Treaty,8,9 and only one of those articles, a case report, referenced the ELSO Maastricht Treaty. 9 An additional two articles (3%) had variable adherence to nomenclature recommendations, but neither cited the ELSO Maastricht Treaty.10,11
The remaining 59 (94%) articles did not adhere to the ELSO Maastricht Treaty in their descriptions of PPC-PA. This non-adherence manifested in various ways, frequently in combination, such as misidentifying the VP ECMO mode, employing incorrect or new terms and abbreviations, and providing inaccurate descriptions of cannulas or their application. The most frequent departure from the recommendations was the use of novel or erroneous terms and abbreviations. Examples of this included the use of abbreviations designated for central ECMO in descriptions of peripheral ECMO, as well as improperly interchanging level 3 and level 4 abbreviations.
Given the widespread non-adherence to the ELSO Maastricht Treaty observed in scientific papers describing PPC-PA, we consider a focused discussion on the correct use of nomenclature, supplemented by a comprehensive guide of examples, to be both urgent and essential. 12
Practical user-guide
Peripheral percutaneous cannulation of the pulmonary artery - configurations and abbreviation examples.
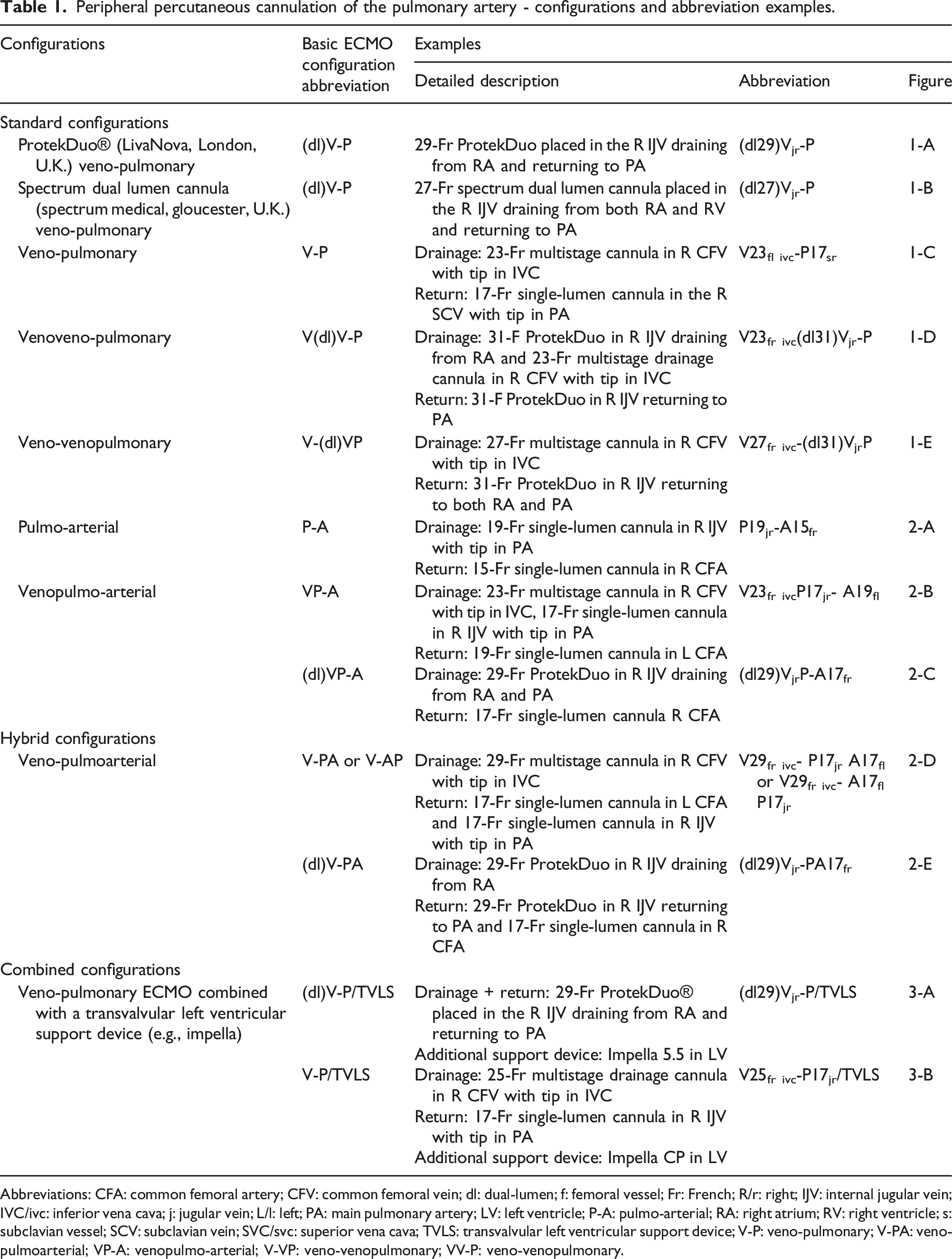
Abbreviations: CFA: common femoral artery; CFV: common femoral vein; dl: dual-lumen; f: femoral vessel; Fr: French; R/r: right; IJV: internal jugular vein; IVC/ivc: inferior vena cava; j: jugular vein; L/l: left; PA: main pulmonary artery; LV: left ventricle; P-A: pulmo-arterial; RA: right atrium; RV: right ventricle; s: subclavian vessel; SCV: subclavian vein; SVC/svc: superior vena cava; TVLS: transvalvular left ventricular support device; V-P: veno-pulmonary; V-PA: veno-pulmoarterial; VP-A: venopulmo-arterial; V-VP: veno-venopulmonary; VV-P: veno-venopulmonary.
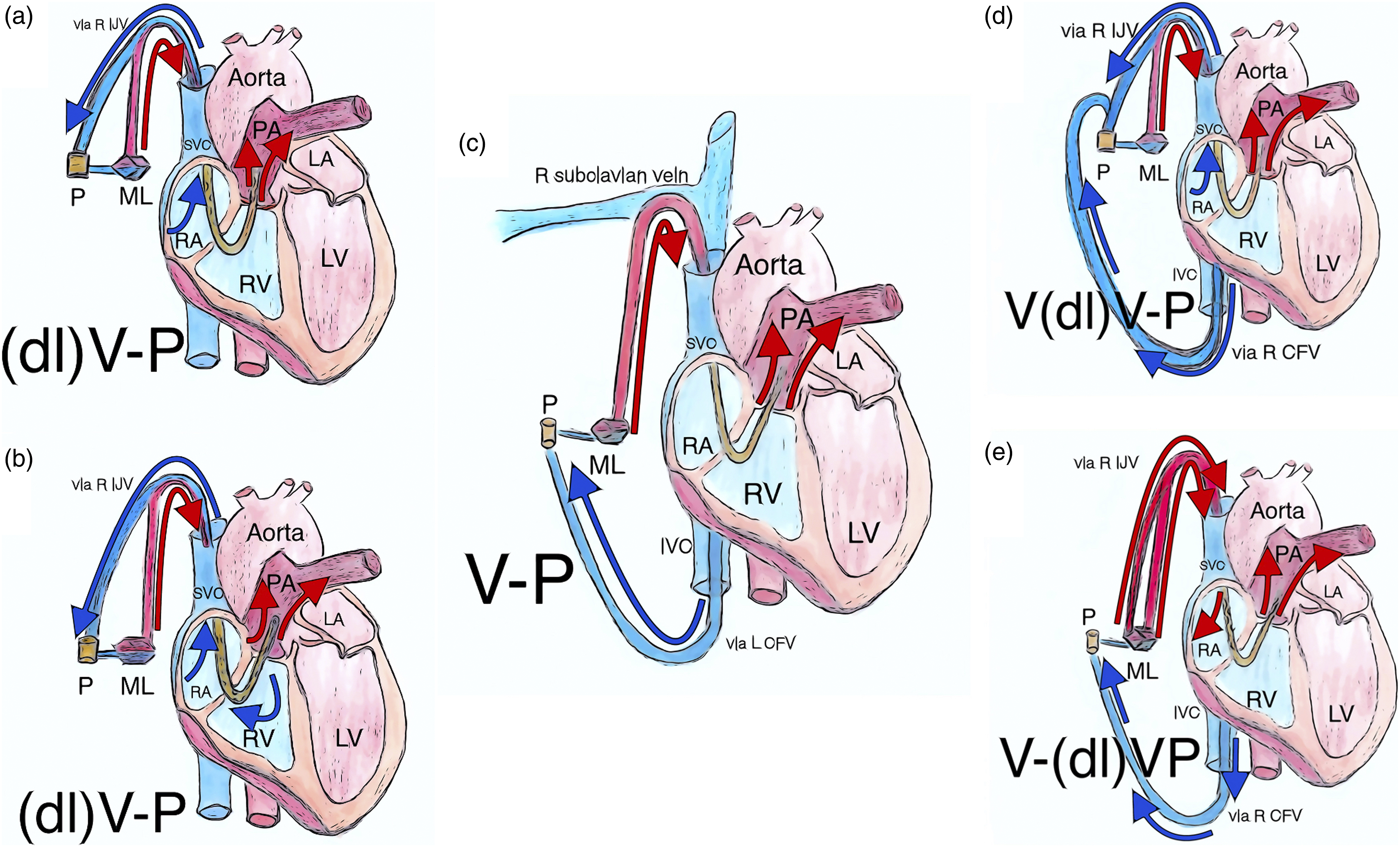
Peripheral percutaneous cannulation of the pulmonary artery - configurations with return to PA (a): veno-pulmonary configuration with ProtekDuo cannula in R IJV with tip in PA, draining RA and returning to PA through separate lumina; (b): veno-pulmonary configuration with Spectrum Dual Lumen Cannula in R IJV with tip in PA, draining RA and RV and returning to PA through separate lumina; (c): veno-pulmonary configuration with drainage via single lumen cannula in L CFV with tip in IVC and return via single lumen cannula in R SCV with tip in PA; (d): venoveno-pulmonary configuration with drainage via single lumen cannula in R CFV with tip in IVC combined with ProtekDuo in R IJV with tip in PA draining from RA and returning to PA through separate lumina; (e): veno-venopulmonary configuration with drainage via single lumen cannula in R CFV with tip in IVC and return via both lumina of ProtekDuo to RA and PA. Abbreviations: CFV: common femoral vein; dl: dual lumen; IJV: internal jugular vein; IVC: inferior vena cava; L: left; LA: left atrium; LV: left ventricle; M: membrane lung; P: centrifugal pump; PA: pulmonary artery; R: right; RA: right atrium; RV: right ventricle; SCV: subclavian vein; SVC: superior vena cava; V-P: veno-pulmonary; V-VP: veno-venopulmonary; VV-P: veno-venopulmonary.
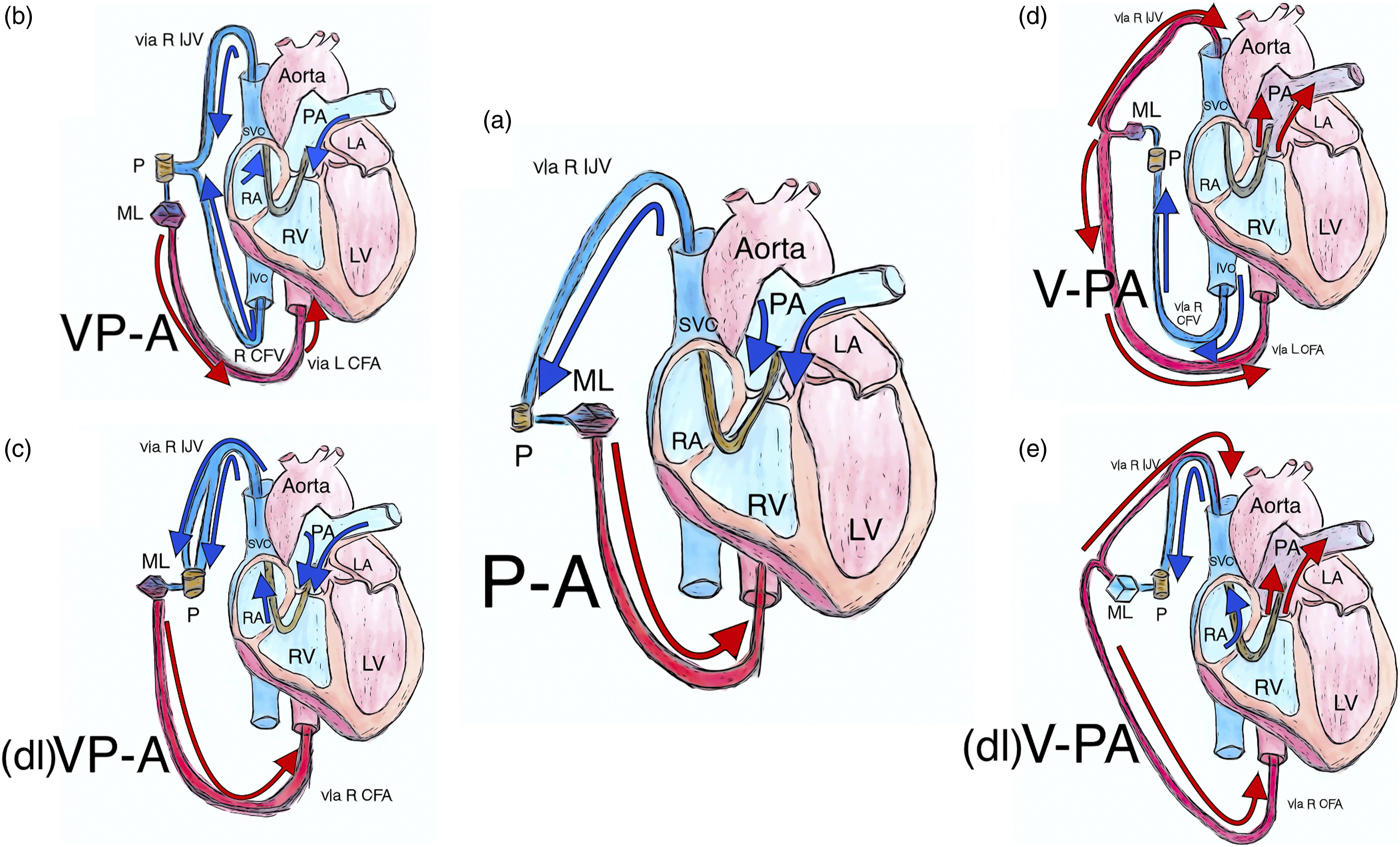
Peripheral percutaneous cannulation of the pulmonary artery - configurations with return to peripheral artery (a): pulmo-arterial configuration with drainage via single lumen cannula in R IJV with tip in PA and return via single lumen cannula in R CFA; (b): venopulmo-arterial configuration with drainage via single lumen cannula in R CFV with tip in IVC combined with single lumen cannula in R IJV with tip in PA and return via single lumen cannula in L CFA; (c): venopulmo-arterial configuration with drainage from RA and PA via both lumina of ProtekDuo cannula and return via single lumen cannula in R CFA; (d): veno-pulmoarterial hybrid configuration with drainage via single lumen cannula in R CFV with tip in IVC and return via separate single lumen cannulae in PA and L CFA; (e): veno-pulmoarterial hybrid configuration with ProtekDuo draining from RA and returning to PA combined with single lumen cannula returning to R CFA. Abbreviations: CFA: common femoral artery; CFV: common femoral vein; dl: dual lumen; IJV: internal jugular vein; IVC: inferior vena cava; L: left; LA: left atrium; LV: left ventricle; M: membrane lung; P: centrifugal pump; PA: pulmonary artery; P-A: pulmo-arterial; R: right; RA: right atrium; RV: right ventricle; SVC: superior vena cava; V-PA: veno-pulmoarterial; VP-A: venopulmo-arterial.
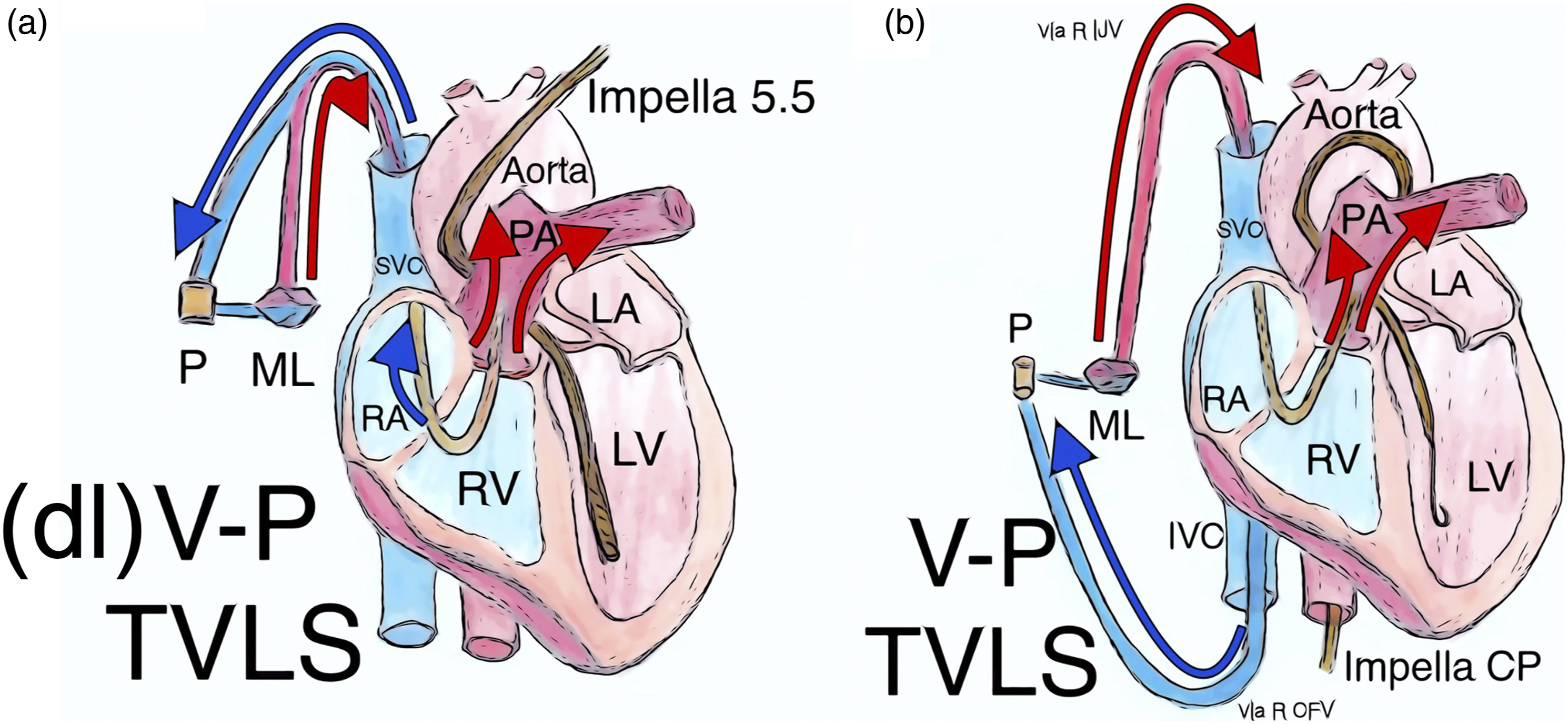
Peripheral percutaneous cannulation of the pulmonary artery – combined configurations (a): Protek Duo cannula in R IJV with tip in PA draining from RA and returning to PA combined with Impella 5.5 TVLS; (b): veno-pulmonary configuration with drainage via single lumen cannula in R CFV with tip in IVC and return via single lumen cannula in R IJV with tip in PA combined with Impella CP TVLS. Abbreviations: CFV: common femoral vein; dl: dual lumen; IJV: internal jugular vein; IVC: inferior vena cava; LA: left atrium; LV: left ventricle; M: membrane lung; P: centrifugal pump; PA: pulmonary artery; R: right; RA: right atrium; RV: right ventricle; SVC: superior vena cava; TVLS: transvalvular left ventricular support device.
Mode
The ELSO has designated VP ECMO as a distinct mode capable of providing both respiratory and right ventricular (RV) support.1,6 Other discrete modes such as venovenous (VV) or venoarterial (VA) should not be used to describe the VP mode. In cases where VP mode is used in combination with VV or VA modes, then the appropriate abbreviations may be combined (Table 1).
Configurations
The VP ECMO mode can be achieved through various cannulation configurations. To represent the level 1 configuration, the abbreviation “V-P” should be used, indicating drainage from a venous source and return to the PA. In peripheral configurations, “P” represents return to the PA. A hyphen, which symbolizes a membrane oxygenator, separates the drainage and return limbs in the level 1 description.1–3,6 The abbreviations “PA” or “RVAD” should not be used for peripheral ECMO configurations, as they are exclusively reserved for central ECMO configurations.1–3 Furthermore, creating new abbreviations to indicate either drainage or return access sites should be avoided. If a specialized dual-lumen cannula is in use, the level 1 configuration can be written as “(dl)V-P” (Table 1).1–3,6
The ECMO configuration can be further specified when level 2 abbreviations are utilized. In instances where multiple cannulas are utilized to create a V-P ECMO configuration, each cannula’s accessed vessel should be included (e.g., V
The cannulation configuration achieves full clarity when level 3 and level 4 abbreviations are included.1–3 When employing two or more cannulas in V-P ECMO, both level 3 and 4 abbreviations can be used to specify the drainage portion, while a level 4 abbreviation is utilized to specify the return portion (e.g., V
Cannulas
Misinterpretations or inaccuracies in the description of cannulas and their functions can sometimes occur. For instance, some authors have referred to the ProtekDuo cannula as a dual-stage cannula, when in fact it is a dual-lumen cannula, with each lumen having a single stage. Conversely, the drainage lumen of the Spectrum Dual Lumen Cannula is genuinely dual-stage, as it drains from two distinct areas, one in the right atrium and one in the RV. Care should be taken to accurately describe cannulas used for ECMO.
Conclusion
Adherence to standardized nomenclature is essential as it ensures clear and unambiguous communication among clinicians and researchers. Our analysis of published manuscripts regarding PPC-PA exposes a significant lack of compliance with the ELSO standardized nomenclature. We believe that this issue urgently needs to be addressed, especially given the increasing use of PPC-PA with the introduction of new cannulas and configurations. The failure to use standardized language not only hinders scientific discourse, but also potentially compromises patient safety. Therefore, we urge clinicians, researchers, and academic editorial teams to familiarize themselves with and insist on the correct use of ECMO nomenclature as detailed in the ELSO Maastricht Treaty. In doing so, we can enhance the quality and clarity of ECMO-related literature, and, in turn, the overall advancement of ECMO technology and patient care.
Supplemental Material
Supplemental Material - Standardized nomenclature for peripheral percutaneous cannulation of the pulmonary artery in extracorporeal membrane oxygenation: Current uptake and recommendations for improvement
Supplemental Material for Standardized nomenclature for peripheral percutaneous cannulation of the pulmonary artery in extracorporeal membrane oxygenation: Current uptake and recommendations for improvement by J Michael Brewer, L Mikael Broman, Justyna Swol Roberto Lorusso, Steven A Conrad and Marc O Maybaue in Perfusion.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Assoc. Professor Broman is a medical advisory board member for EUROSETS, Xenios, and HemoCue. Prof. Lorusso is a consultant for Medtronic, Getinge and LivaNova and medical advisory board member for EUROSETS, all unrelated to this work; all honoraria to the university for research funding. Prof. Maybauer is a consultant for LivaNova and speaker for Abbott, all unrelated to this work
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.