
Abstract
Objectives
Acknowledging lacking of consensus exist in total aortic arch (TAA) surgery for acute type A aortic dissection (AAD), this study aimed to investigate the neurologic injury rate between bilateral and unilateral cerebrum perfusion on the specific population.
Methods
A total of 595 AAD patients other than Marfan syndrome receiving TAA surgery since March 2013 to March 2022 were included. Among them, 276 received unilateral cerebral perfusion (via right axillary artery, RCP) and 319 for bilateral cerebral perfusion (BCP). The primary outcome was neurologic injury rate. Secondary outcomes were 30-day mortality, serum inflammation response (high sensitivity C reaction protein, hs-CRP; Interleukin-6, IL-6; cold-inducible RNA binding protein, CIRBP) and neuroprotection (RNA-binding motif 3, RBM3) indexes.
Results
The BCP group reported a significantly lower permanent neurologic deficits [odds ratio: 0.481, Confidence interval (CI): 0.296–0.782, p = 0.003] and 30-day mortality (odds ratio: 0.353, CI: 0.194–0.640, p < 0.001) than those received RCP treatment. There were also lower inflammation cytokines (hr-CRP: 114 ± 17 vs. 101 ± 16 mg/L; IL-6: 130 [103,170] vs. 81 [69,99] pg/ml; CIRBP: 1076 [889, 1296] vs. 854 [774, 991] pg/ml, all p < 0.001), but a higher neuroprotective cytokine (RBM3: 4381 ± 1362 vs 2445 ± 1008 pg/mL, p < 0.001) at 24 h after procedure in BCP group. Meanwhile, BCP resulted in a significantly lower Acute Physiology, Age and Chronic Health Evaluation (APACHE) Ⅱscore (18 ± 6 vs 17 ± 6, p < 0.001) and short stay in intensive care unit (4 [3,5] vs. 3 [2,3] days, p < 0.001) and hospital (16 ± 4 vs 14 ± 3 days, p < 0.001).
Conclusions
This present study indicated that BCP compared with RCP was associated with lower permanent neurologic deficits and 30-day mortality in AAD patients other than Marfan syndrome receiving TAA surgery.
Keywords
Introduction
The therapeutic regimen has been widely embraced in the worldwide that acute type A aortic dissection (AT-AAD, AAD) should receive emergency surgery due to high mortality and morbidity. Although the survival rate of surgical procedure for acute type A aortic dissection (AAD) had been improved with the development of surgical techniques and hemostasis technology, how to prevent neurologic deficits events was another important goal and a continued topic of controversy because the optimal neuroprotection strategy was not well determined in cardiothoracic surgical community. 1
A consensus had been almost reached that both antegrade and retrograde cerebral perfusion were superior to deep hypothermic circulatory arrest (HCA) in AAD repair. 2 Some studies had attempted to solve the dispute between bilateral and unilateral cerebral perfusion. Piperata et al. advised against the use of bilateral cerebral perfusion due to higher incidence of permanent neurologic deficits (PND). 3 Norton et al. also suggested the right cerebral artery cannulation for its simplicity and effectiveness unless the left carotid artery (LCA) was occluded by thrombosed false lumen. 4 However, these studies were still inconclusive due to lacking of homogeneity on the extent of aortic arch replacement and the clinical etiological classification. Thus, further study on the optimal perfusion strategy in the specific population remained to be determined.
The etiology of the AAD population is comprised of inherited and acquired cause. About 20% of AAD individuals suffered from heritable thoracic aortic disease like Marfan syndrome. 5 The pathological characteristics in this part population was connective tissue disorder. On the contrary, the large part of the population was accounted for unaware or uncontrollable hypertension and aggravating atherosclerosis especially in China. It is likely that the latter has abnormal collateral circulations such as right-left common carotid arteries, right-left external carotid arteries and the circle of Willis due to atherosclerosis on the intima of arteriole, and therefore the blood flow perfusion in left hemisphere could be undermined if only right axillary artery (RAA) was cannulated. In addition, cold shock proteins were also measured on the account of close associations with neurological events after hypothermic circulatory arrest. 6 Here, the present study was to test the hypothesis that bilateral was more optimal than unilateral cerebral perfusion in AAD patients other than Marfan syndrome.
Patients and methods
Study population
This study was a cohort study of retrospectively collected data from consecutively recruited patients between March 2013 and March 2022 at the Cardiac Surgery Department from Sichuan Provincial People’s Hospital and other four assisted institutions operated by one surgeon (Figure 1). Patients receiving total aortic arch (TAA) surgery with antegrade cerebral perfusion (ACP) were included but excluded if Marfan syndrome. The patients were assigned to receive unilateral cerebral perfusion via right axillary artery (RCP) or bilateral cerebral perfusion (BCP) at doctor’s discretion. The study protocol followed the guidelines of the Declaration of Helsinki and local Medical Ethics Committee, and the written informed consent was acquired from the patients and their relatives from all the participating centers (Approval number: 2021-215, by Sichuan Provincial People’s Hospital at 1 March 2021). The primary endpoint of the study was the incidence rate of neurologic deficits events. The secondary endpoints were the 30-day mortality, serum inflammatory response indexes and neuroprotection cytokines. The consciousness was conventionally evaluated in the postoperative hours after withdrawal of sedatives. Computed tomography (CT) or/and magnetic resonance imaging (MRI) were indicated if there were any symptoms on conscious dysfunction or movement disorders. The incidence of permanent and temporary neurologic dysfunction was defined according to the diagnosis standard as previously reported.
7
The study protocol.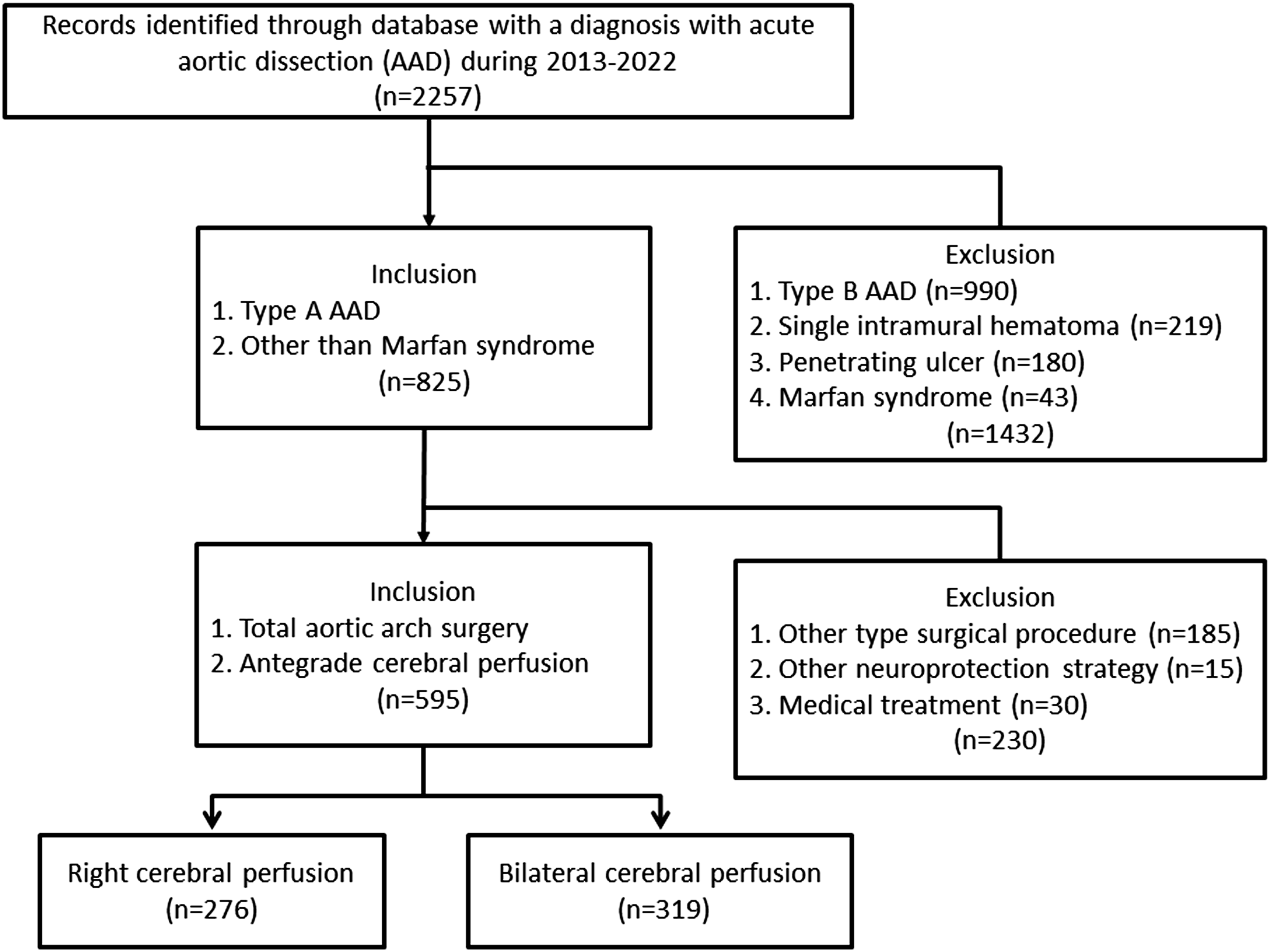
Surgical procedure
The temperature probe was placed for nasopharyngeal and rectal temperature monitoring, respectively. All the procedures were performed by the surgical staffs with same technical support team using a four-branched graft and elephant trunk stent. In brief, during the process of initiating moderate hypothermia after aortic clamping, the proximal end was repaired with one suitable technique according to the damaged condition of aortic valve, valsalva sinus and coronary artery ostium. These reconstruction approaches included Bentall’s, Wheat’s, Carbrol’s, and in many cases, local reinforcement on the aorta with adventitial coat. The endovascular frozen-trunk stent (CRONUS, MicroPort Scientifc Corporation, Shanghai, China) was conventionally implanted into distal anastomosis. The soft edge on the proximal end of stented artificial vessel in combination with outer aortic wall was end-to-end anastomosed to a tetrafurcated graft (Maquet, Rastatt, Baden-Württemberg, Germany). 8
Cerebral artery perfusion
In both groups, femoral artery cannulation and the vena cava drainage was conventionally administered to establish cardiopulmonary bypass (CPB).
9
During HCA period, the flow rate for ACP was 5–10 mL/kg/min for both RCP and BCP with the pressure maintaining around 60 mmHg (50–70 mmHg). The RAA was the routine site for RCP. LCA and left subclavian artery (LSA) was clamped externally near its origin from the aortic arch during HCA. For BCP, two size-suitable arterial cannulas (commonly 16Fr for LCA) was individually cannulated on the normal site of innominate artery and LCA instead of RAA using two antiparallel purse-string sutures with a “Seldinger” technique (Figure 2).
10
Which cannulation strategy was chosen was determined at the surgeon’s discretion on the basis of preoperative CT image. The establishment method of bilateral cerebral perfusion in total aortic arch repair. The femur artery (a) was conventionally used for establishment of cardiopulmonary bypass, bilateral cerebral perfusion was established by two independent size-suitable cannula on innominate artery (b) and left carotid artery (c) using “Seldinger” technique with single one rolling pump.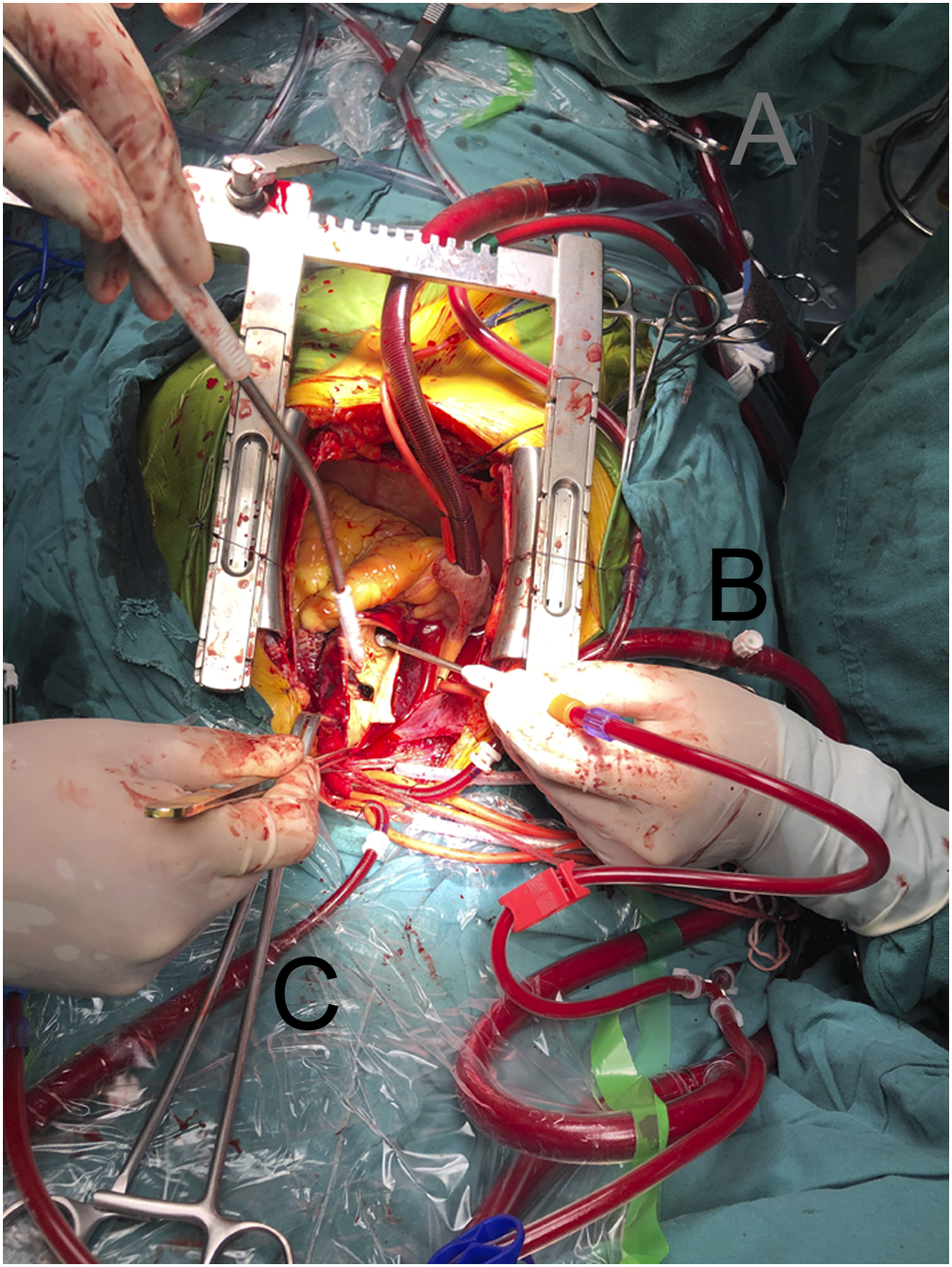
Postoperative clinical outcomes
The operative characteristics such as the time of CPB, aortic cross-clamping (ACC) were extracted from the electronic medical records (EMR). The analysis of 30-day after surgery mortality and neurologic deficits events including permanent neurologic dysfunctions (PND) and temporary neurologic dysfunctions (TND) were performed. The diagnosis of stroke was confirmed under the correlation of the clinical symptoms and neuroimaging evidences. PND was defined as the presence of coma, paraplegia, monoplegia, and hemiplegia. TND was delirium, transient ischemic attack (TIA), confusion and agitation with no positive signs of stroke at CT sacn. 11 The Acute Physiology, Age and Chronic Health Evaluation (APACHE) II score within ICU ward was collected from specialized electronic record at 1 day after procedure. 12
Inflammatory cytokines
Venous blood samples were draw for the laboratory examination, including serum inflammatory response cytokines such as white blood cell, neutrophil, and high sensitivity C-reactive protein (hs-CRP) at the admission time, 12, 24, and 48 hours after procedure. 13 The laboratory test for human cytokines including IL-6 and IL-10 at 24 hours after procedure were also completed.
Cold shock protein analysis
The serum sample of the patients were collected at baseline and 24 hours after procedure for analyzing the levels of cold-inducible RNA binding protein (CIRBP) and cold-shock protein RNA-binding motif 3 (RBM3). Human CIRBP and RBM3 ELISA Kit (Wuhan Fine Biotech, China.) were used as detection and capture antibody, which was based on sandwich enzyme-linked immunesorbent assay technology. 14 Two monocloncal antibodies (the biotin conjugated antibody and tetramethylbenzidine substrates) were used as detection and capture antibody. Samples were prepared and analyzed according to the manufacturer’s instructions. Read the O.D. absorbance at 450 nm in a microplate reader, and then the concentration of target was calculated by the standard curve. These biological assays were completed on the commercial payment to one experienced laboratory technicians who was blind to experimental protocol and sample sequence.
Statistical analysis
Continuous variables were reported as median (1st quartile, 3rd quartile) if distributed non-normally or mean (standard deviation, SD) depending on their adjustment to normality, which was determined by Kolmogorov–Smirnov test. The categorical variables were expressed as absolute numbers (percentage). Statistical analysis between BCP and RCP was performed using Student independent samples t test for normally distributed continuous variables, the Mann-Whitney U non-parametric test for non-normal variables, and χ2 tests (Fisher exact tests if n ≤ 5) for categorical variables. Survival curves of all patients after surgery were estimated using the nonparametric Kaplan-Meier analysis method with Breslow (Generalized Wilcoxon) test. All the statistical analyses were performed using SPSS 25.0 software (SPSS, Inc, Chicago, Ill) and was considered significant at p value of <0.05.
Result
Patient screening and grouping
Baseline characteristics.
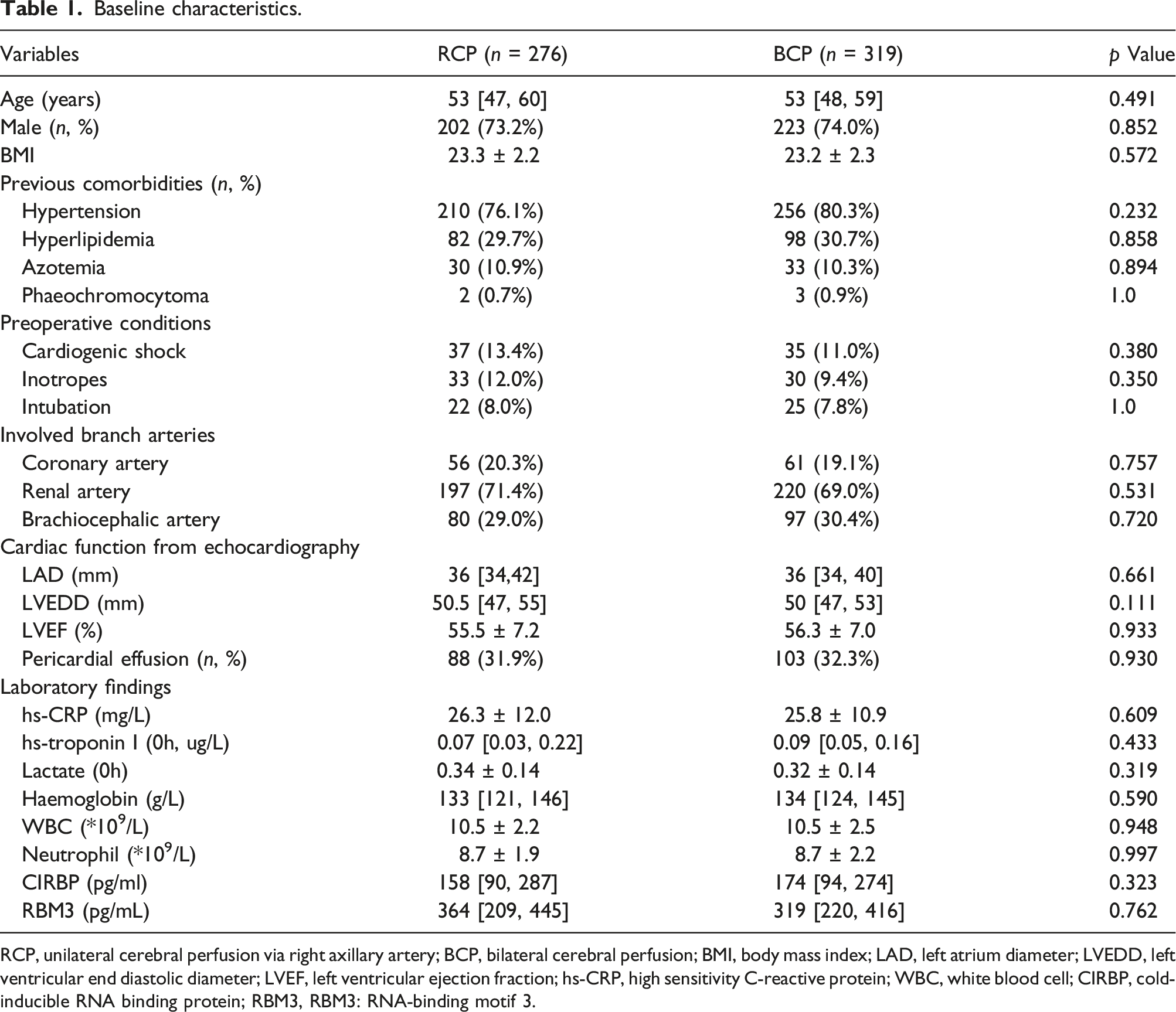
RCP, unilateral cerebral perfusion via right axillary artery; BCP, bilateral cerebral perfusion; BMI, body mass index; LAD, left atrium diameter; LVEDD, left ventricular end diastolic diameter; LVEF, left ventricular ejection fraction; hs-CRP, high sensitivity C-reactive protein; WBC, white blood cell; CIRBP, cold-inducible RNA binding protein; RBM3, RBM3: RNA-binding motif 3.
Intraoperative parameters
Operative characteristics.
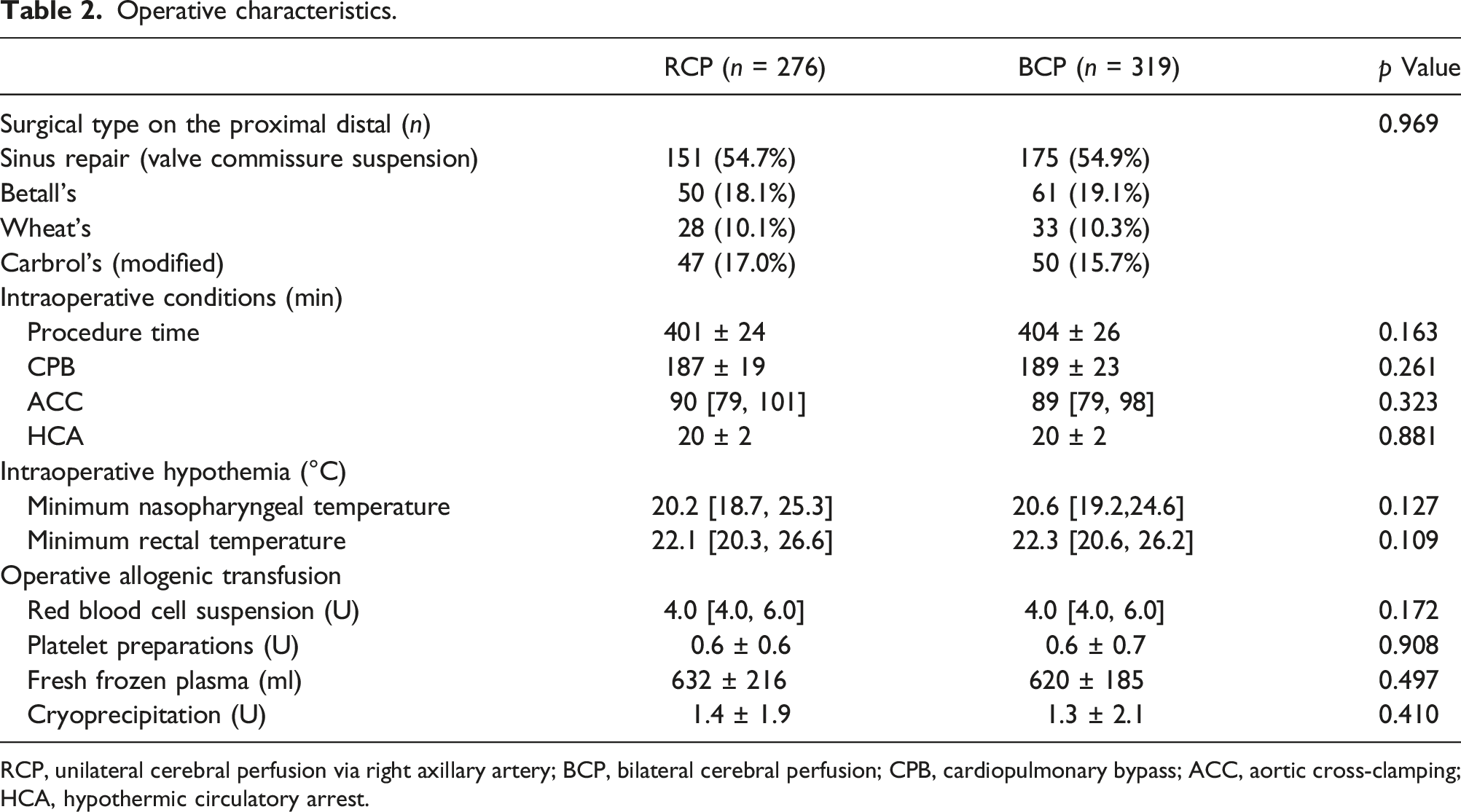
RCP, unilateral cerebral perfusion via right axillary artery; BCP, bilateral cerebral perfusion; CPB, cardiopulmonary bypass; ACC, aortic cross-clamping; HCA, hypothermic circulatory arrest.
Serum levels of hs-CRP, IL-6, IL-10, CIRBP and RBM3
Postoperative inflammation and neuroprotection responses.
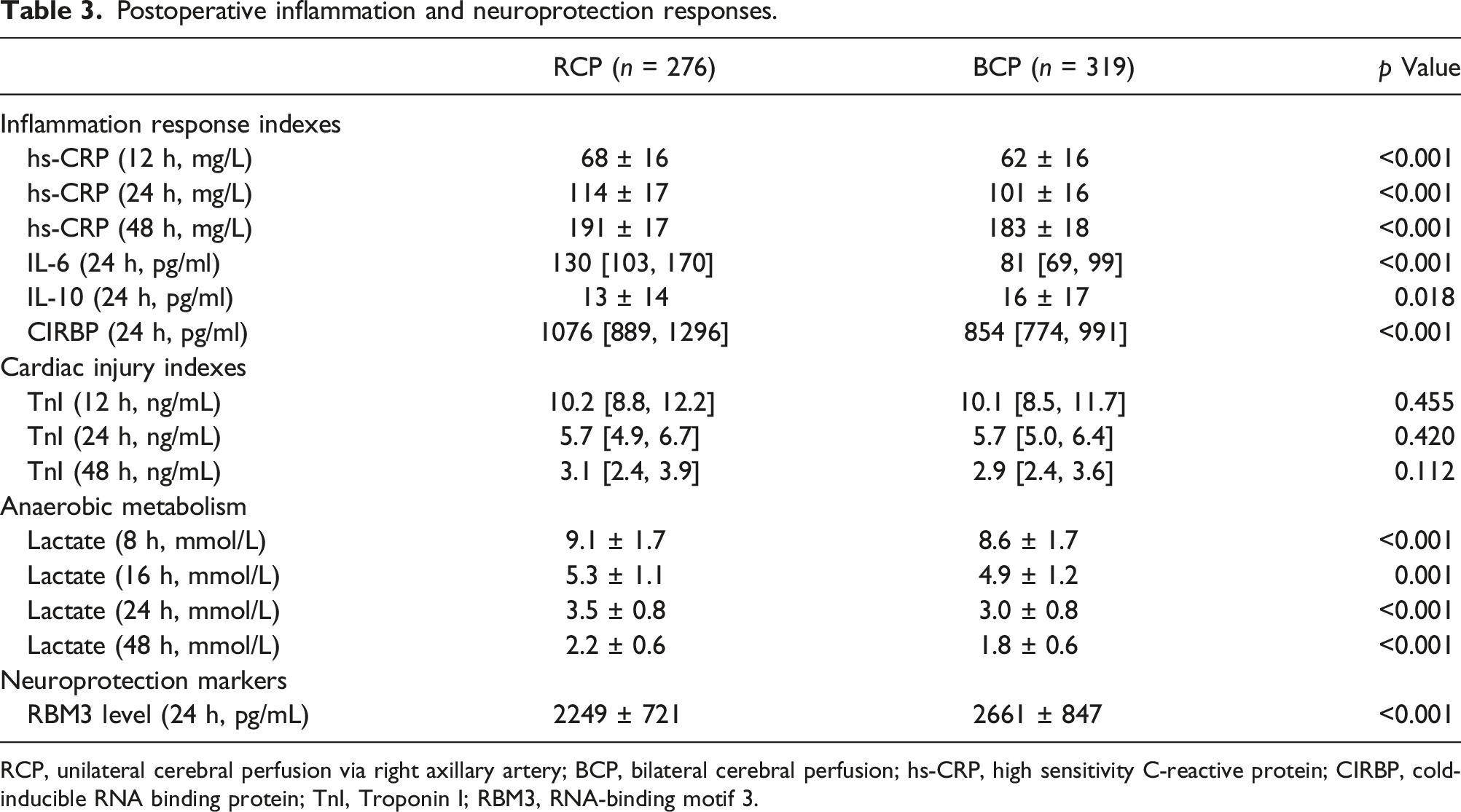
RCP, unilateral cerebral perfusion via right axillary artery; BCP, bilateral cerebral perfusion; hs-CRP, high sensitivity C-reactive protein; CIRBP, cold-inducible RNA binding protein; TnI, Troponin I; RBM3, RNA-binding motif 3.
Postoperative neurological and mortality events
Postoperative clinical outcomes.
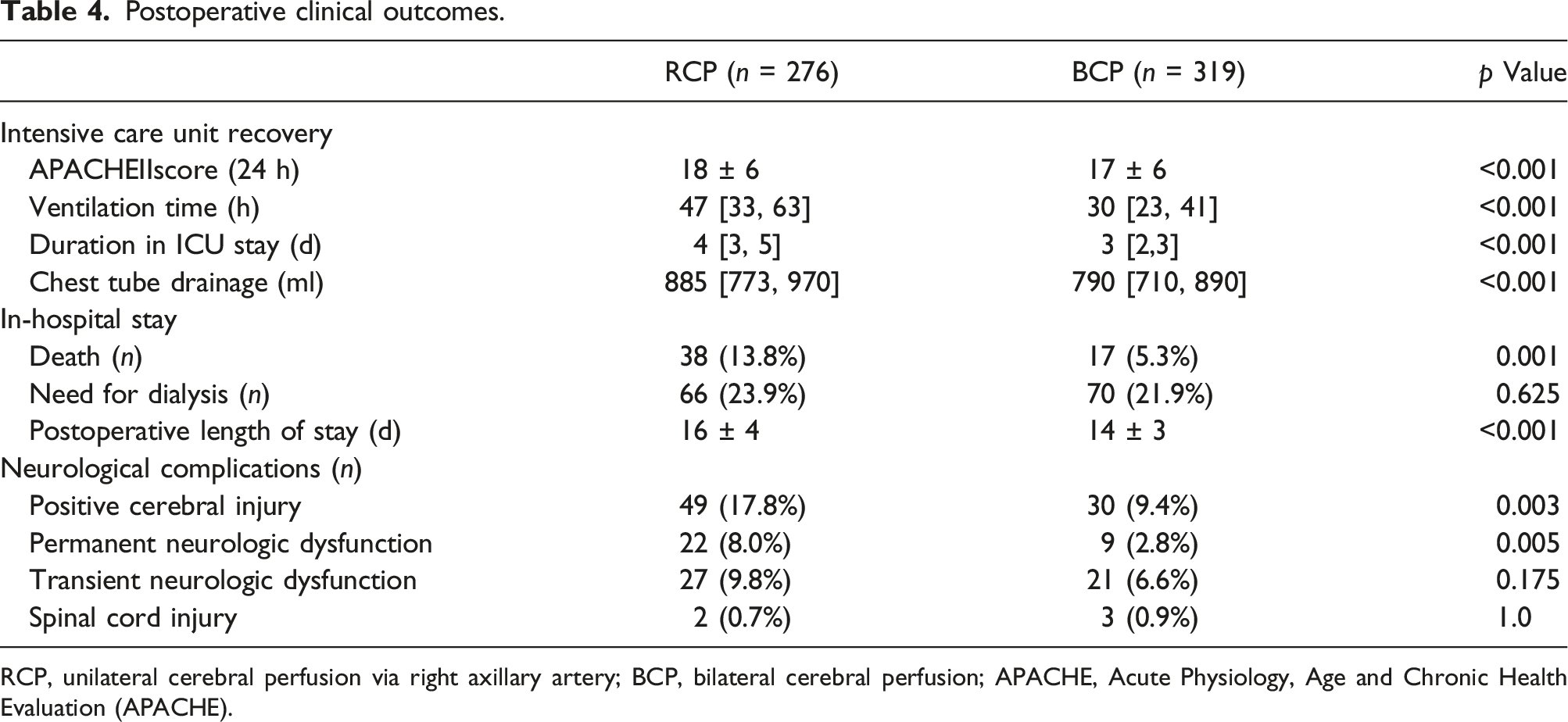
RCP, unilateral cerebral perfusion via right axillary artery; BCP, bilateral cerebral perfusion; APACHE, Acute Physiology, Age and Chronic Health Evaluation (APACHE).
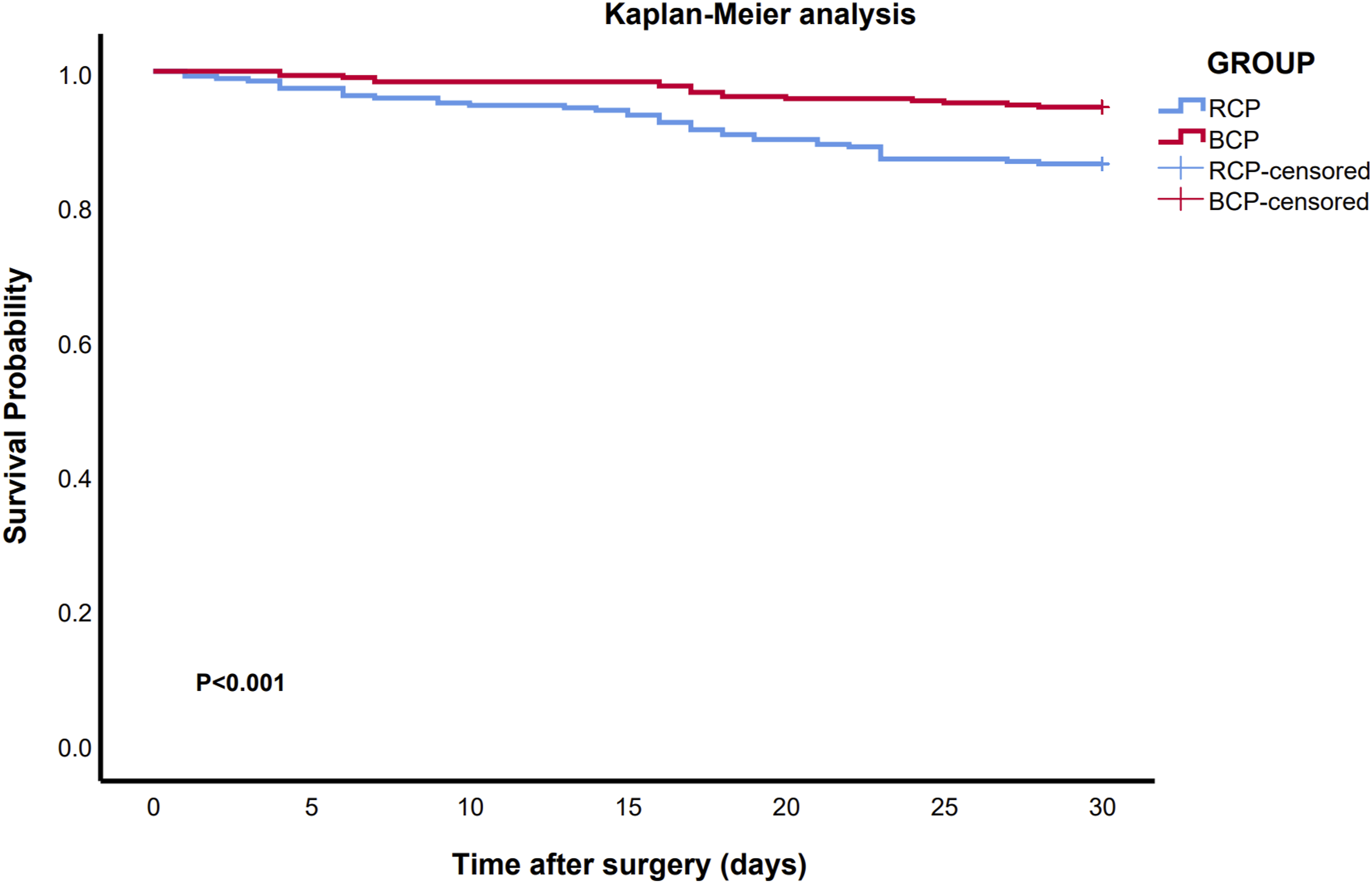
Survival (Kaplan-Meier analysis) of the patients of acute aortic dissection other than Marfan syndrome receiving total aortic arch repair using unilateral cerebral perfusion via right axillary artery (RCP) and bilateral cerebral perfusion (BCP). The 30-day survival rate was higher in BCP group compared with that in RCP group (94.7% vs 86.2%).
Discussion
There are two crucial findings of this study: (1) there was a significantly lower 30-day after surgery mortality and stroke rate after aortic dissection repair procedure with receiving BCP than RCP; and (2) the advantageous results with BCP technique was likely to be accountable for the effect of inflammation alleviation and neurological protection.
The evolution of neurological protection strategies constantly revolutionized in surgical community. HCA provides aortic surgeons with a bloodless operative field while simultaneously protecting the brain and peripheries from ischemic damage via general reduction of metabolism. However, administration of deep HCA resulted in harmful effect on cerebral nerve due to autoregulation loss and decrease in regional oxygen supply. 15 Thus, it seemed that cerebral perfusion was very vital to prevent against death and stroke in AAD repair. 16
Axillary artery cannulation provided a reliable circulatory route for cerebral perfusion. However, the successfully neurological protection via RAA perfusion depends on the complete anatomy of Willis circle of cerebrum which connects the blood circulation between the bilateral cerebral hemispheres. As previously reported from autopsies, the diameter of the communicating arteries in almost above 10% subjects was less than 0.5–1.0 mm, which would undermine left hemisphere perfusion when only RAA cannulation is used. 17 Meanwhile, increased atherosclerotic plaque burden decreased blood flow reserve due to vascular obstruction underneath the arterial wall’s lipid deposits during the RCP process. Therefore, BCP which combines innominate artery cannulation with a supplementary catheter in LCA was aimed to simulate normal ACP and prevent the unequal blood distribution via RCP. 18 About 30% of AAD extended to brachiocephalic branch arteries in our study was similar as Charlton-Ouw et al. reported, 19 which had adverse impact on the flow distribution to some extent. During the management of aortic arch, only the proximal section of the carotid arteries was replaced by the branches of artificial vessel in our management, which differed from the strategy that aggressive replacement of the dissected carotid arteries to its bifurcation. 20 This partial segment replacement strategy potentially leaved more stenosis in bilateral carotid artery.
It had been concluded that modern aortic arch surgery appears safe for stroke prevention with cerebral perfusion not necessitates deep or profound hypothermia in current clinical practice, whether the retrograde or antegrade cerebral perfusion, but the strategy without cerebral perfusion should be dissuaded on the account that no cerebral perfusion had the highest incidence of stroke. 21 Moreover, direct carotid artery perfusion didn’t incur more intracerebral hemorrhage or cerebral infarction. 22 With the introduction of BCP, we also demonstrated the safety of moderate-to-mild systemic HCA (minimum nasopharyngeal temperature: 28°C) without adverse neurological influence including spinal cord injury. 23 Moreover, BCP resulted in better early ICU recovery represented of low APACHE II score, which significantly affected the total hospitalization expenses. 24
Although the protocol was reasonable that an early anastomosis of LCA before the LSA anastomosis for limiting the time of “true” uniform ACP. 25 The HCA and cerebral ischemia potentiated ischemia-reperfusion injury and revoke more neuro-inflammatory responses. 26 A well-established neuroprotection mechanism induced by cooling was that cold shock proteins CIRBP and RBM3 act in a different expression kinetics. 27 CIRBP expression in the blood was elevated at 6 hours after CPB and exerted on detrimental neuroinflammation effects. 28 While, RBM3 protein had a delayed elevation at 24 hours after cooling like hypothermic cardiopulmonary bypass. Moreover, noticeably increased RBM3 was associated with good functional outcome in the stroke patients. 29
A direct comparison between BCP and RCP revealed a significant difference in mortality and morbidity. The outcome indicated that BCP provided satisfactory cerebral protection and avoided unilateral cerebral perfusion-related side effects. We assumed the cause lie in the fact that BCP resulted in satisfactory perfusion pressure and flow circulation because a decrease or increase in the resistance of the right carotid artery could lead to brain mal-perfusion. The greatest advantage of BCP is that the LCA can make up for RCP-induced false cavity hypoperfusion and that LCA can compensate for the insufficient flow of the RCP. Especially for carotid arteriosclerosis, the entrapment of air or small debris in the terminal of an incomplete circle of Willis from RCP cannulation could be washed out by the flow from the LCA perfusion. 30
Study limitations
This study had some inevitable limitations. First, the study was a retrospective observation design on the recruited patients who spanned across 9 years, and then the influence of era bias cannot be excluded such as the advance on laboratory analysis profiles, the rationality of inotropic medication usage, and the unavailability of near-infrared spectroscopy at the early years. Using transcranial cerebral oximetry is helpful to detect the insufficient cerebral perfusion and prevent devastatingly harmful effect. But only clinical evidence of mal-perfusion other than imaging features could always predict in-hospital mortality. Second, this study only represented the result of a multicenter practice but from one surgical technical team. Thus, randomized control trial from multiple surgical teams should be designed to further verify our results.
Conclusions
BCP was associated with lower incidence rate of permanent neurologic dysfunction compared with RCP in AAD patients receiving TAA procedure other than Marfan syndrome.
Footnotes
Author contributions
JQ, HKL, YT and HSS contributed to the conception or design of the work. JQ, WDL, and XJQ contributed to the acquisition, analysis, or interpretation of data for the work. JQ drafted the manuscript. All authors critically revised the manuscript. All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sichuan Science and Technology Program [2021JDJQ0041, 2020YFQ0060], Huanhua Talent for Discipline Backbone of Sichuan Provincial People’s Hospital [SY2022017] and National Natural Science and Technology Foundation of China [81800274].
Data availability
Some or all data used during the study are available from the corresponding author by request.