
Abstract
Introduction
The treatment of a chronic type B aortic dissection can be challenging and need a precise and multidisciplinary planning.
Materials and Results
A 62-year-old man presented to our hospital with acute aortic thrombosis on chronic thoracoabdominal dissection with bowel and kidney ischemia. He was submitted to urgent open surgical treatment with replacement of thoracoabdominal aorta and reimplantation of celiac trunk, superior mesenteric artery and right renal artery. During the intervention the visceral perfusion was provided with a modified Gott shunt; while the lower limb perfusion was provided by an existing right axillo-femoral and femoro-femoral bypass. The patient had a favorable course and did not report any complications.
Conclusion
The ideal management strategy of complex post-dissection conditions has to be tailored on the single patient’s features to provide the maximal efficacy and safety. If the endovascular treatment is not viable, open surgery represents a valid option.
Introduction
Chronic type B dissection is a complex condition, characterized by high risk for late aorta-related events and reinterventions with high morbidity and mortality rates. Treatment strategies vary from open repair to total endovascular and hybrid options and must be tailored on specific aortic and patient’s features.
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Case report
A 62-year-old man presented to our hospital with acute abdominal pain, severe hypertension, and oliguria. 10 years before he had an acute type A aortic dissection with acute lower limb ischemia, treated with ascending aorta replacement and right axillo-femoral and femoro-femoral bypass. 6 years after that event, he required emergent embolization of the left renal artery for rupture of the vessel with retroperitoneal hematoma.
On arrival, he underwent a CT-angiogram which documented a residual aortic dissection extending from the arch to the thoracoabdominal aorta with aneurysmal dilatation of the arch (55 mm) and complete thrombosis of a dilated false lumen (FL) with near total occlusion of the true lumen (TL) at the hiatus and malperfusion of the superior mesenteric artery (SMA) and the right renal artery (RRA) (Figure 1(a) and (b)). Moreover, the CTA scan documented the presence of a pseudoaneurysm of the ascending aorta, measuring 6 cm, close to the distal anastomosis of the previous surgical graft. Volume rendering reconstruction of the pre-operative CT-angiogram. (b). Detail of celiac trunk and superior mesenteric artery originating from a near occluded true lumen.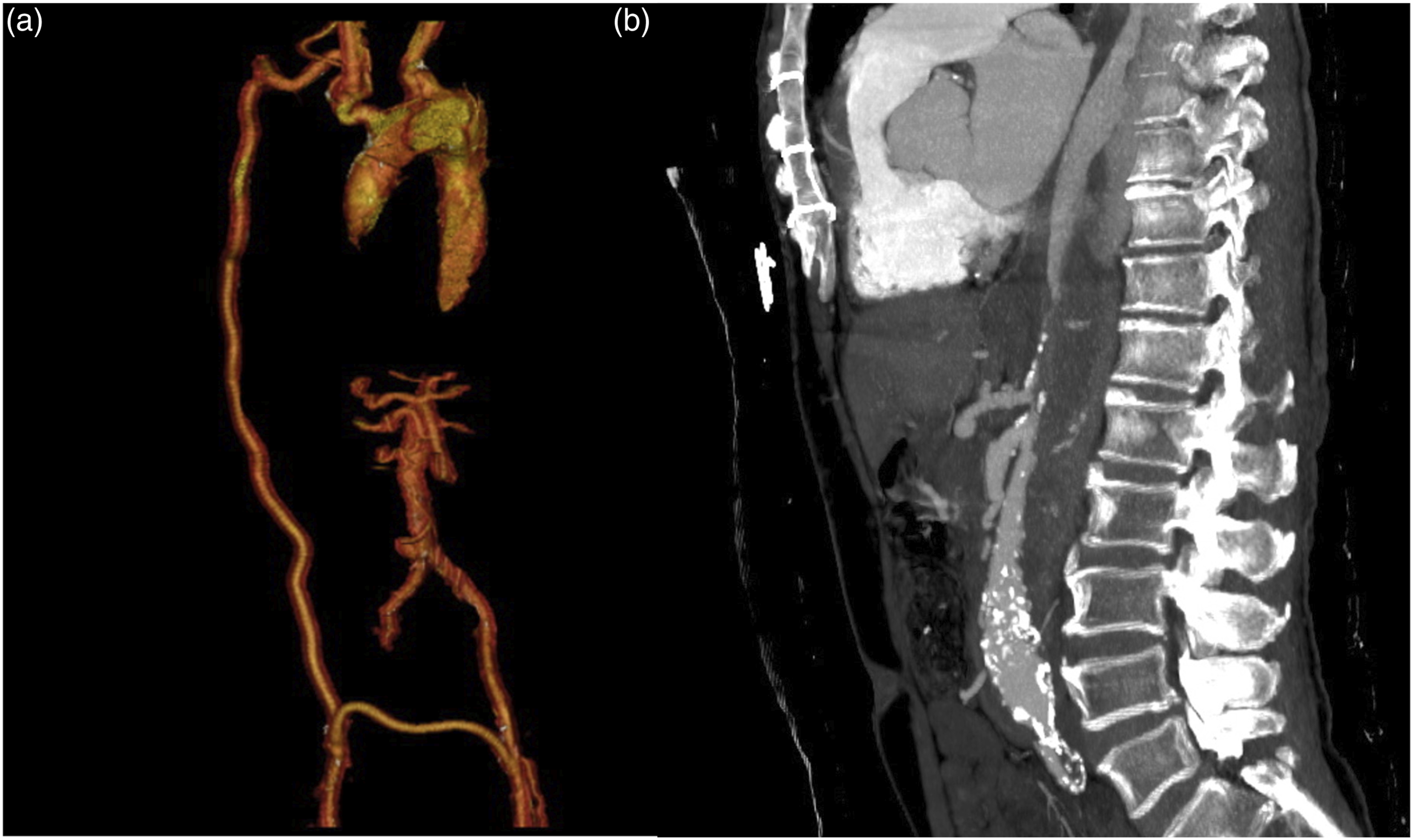
After multidisciplinary discussion, given the absence of a suitable outflow for direct arch repair nor a suitable access to the arch from the femoral arteries for a possible endovascular solution, decision was made to offer the patient an open thoraco-abdominal repair. The intervention was performed with cerebrospinal fluid drainage and single lung intubation. The surgical access was a thoraco-phreno-laparotomy at the sixth intercostal space. We opted for a partial radial phrenotomy. We dissected the descending thoracic aorta, the infrarenal aorta, the celiac trunk (CT), the superior mesenteric artery (SMA) and the right renal artery (RRA).
During the intervention, the visceral perfusion to CT and SMA was ensured with a modified Gott shunt anastomosed to the left axillary artery, whilst distal perfusion was maintained through the right axillo-bifemoral bypass. The RRA was perfused with Custodiol® solution (Figure 2(a) and (b)). Schematic representation of visceral, kidney and lower limb perfusion strategy with modified Gott shunt (for celiac trunk and superior mesenteric artery), Custodiol solution (for right renal artery) and right axillo-bifemoral bypass (for lower limbs). (b). Intraoperative image of the visceral and renal perfusions.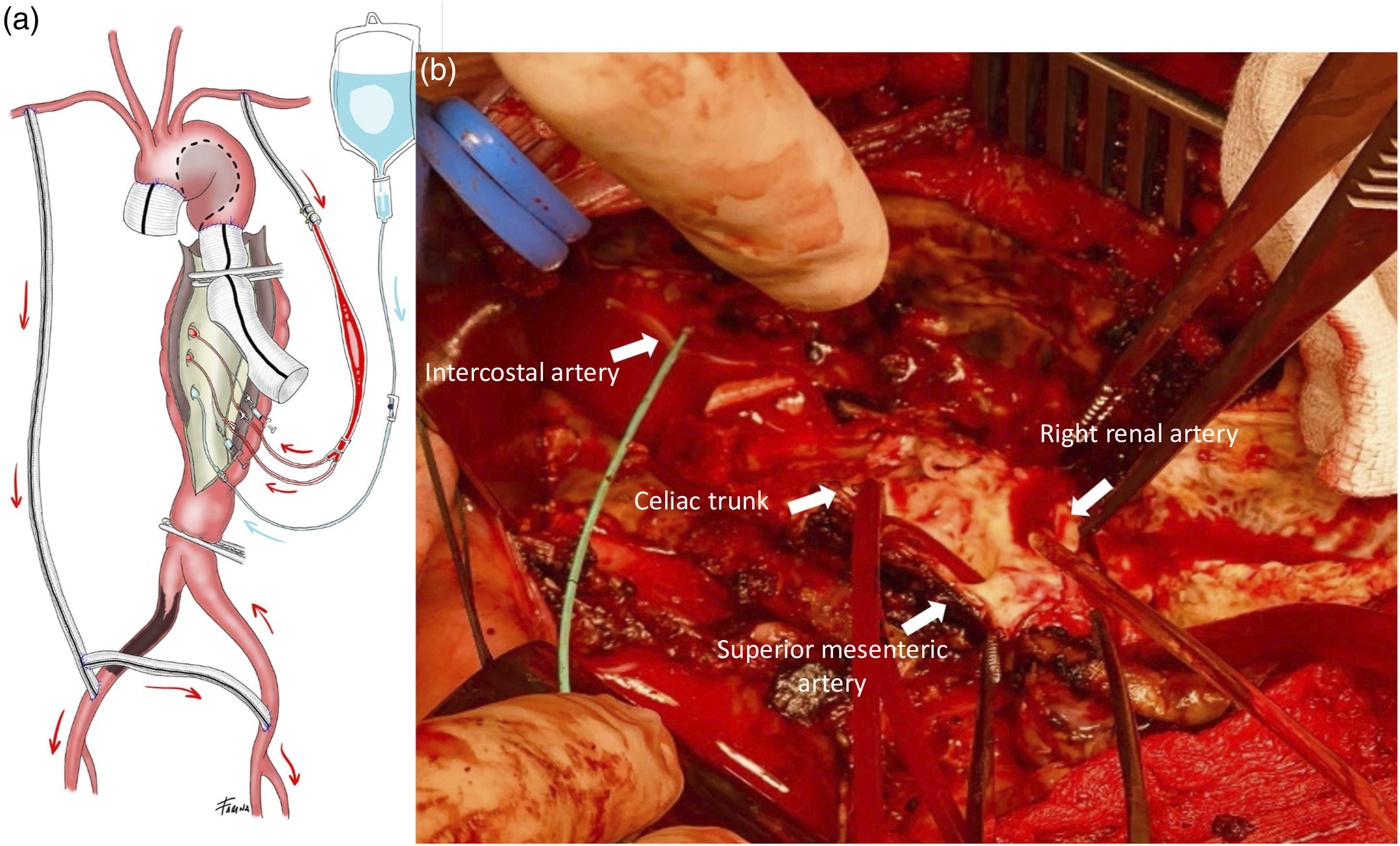
After aortic cross-clamp, the aorta was opened revealing a thick solid thrombus in the FL crushing the TL (Figure 3). The thoraco-abdominal aorta was replaced with reimplantation on a single patch of CT, SMA and RRA. A large intercostal artery was reimplanted through a short bypass. Thick and layered thrombus removed from the false lumen.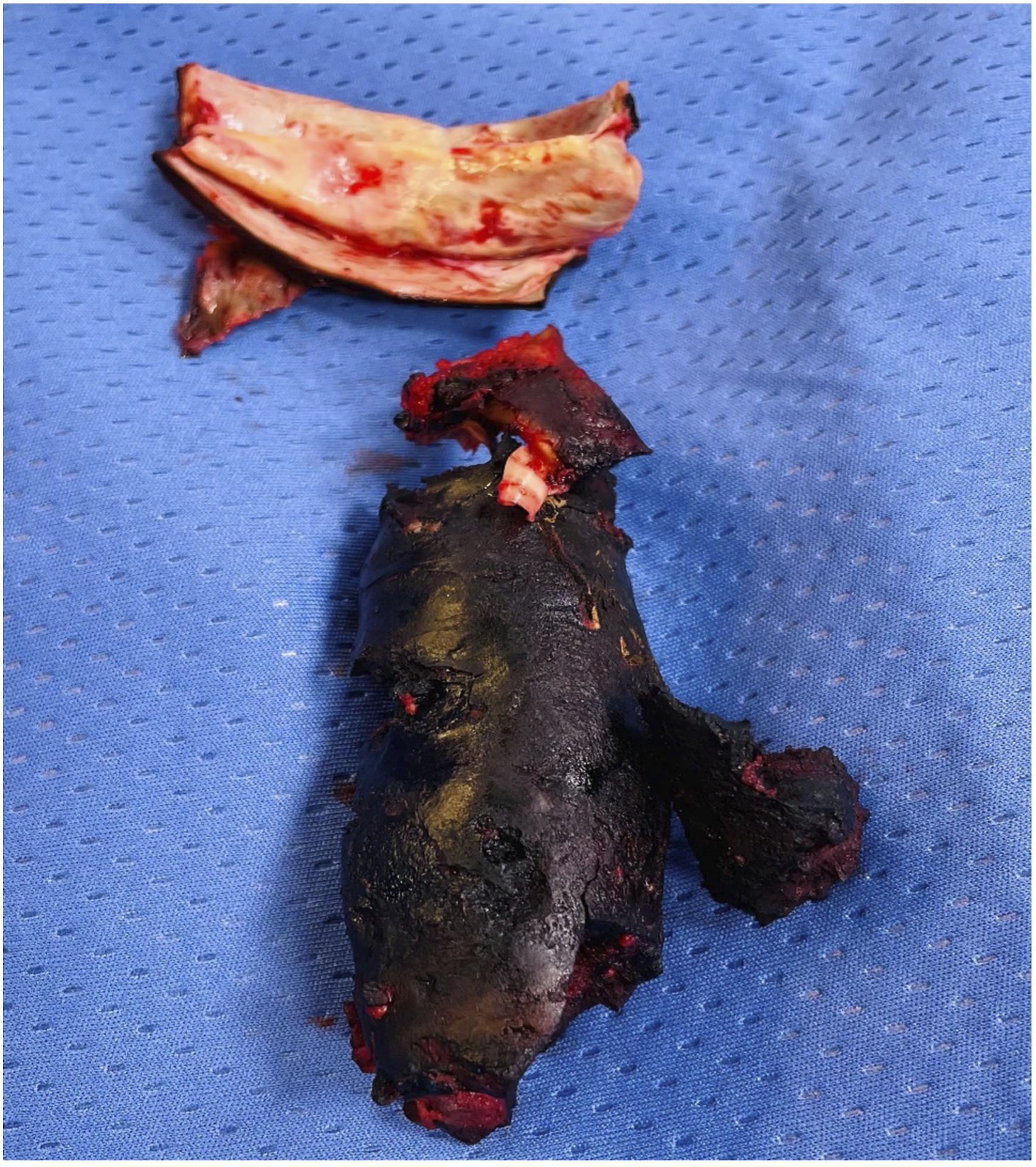
The patient had a favorable post-operative course with resolution of symptoms and no spinal nor visceral ischemia.
The post-operative CTA scan showed patency of the aortic graft, the visceral vessels and the intercostal bypass; the ascending aorta pseudoaneurysm was totally thrombosed, probably for the reduction of the mechanical stress on sutures, that was secondary to persistent high values of blood pressure (Figure 4). Reimplantation of an intercostal artery through a short Dacron graft.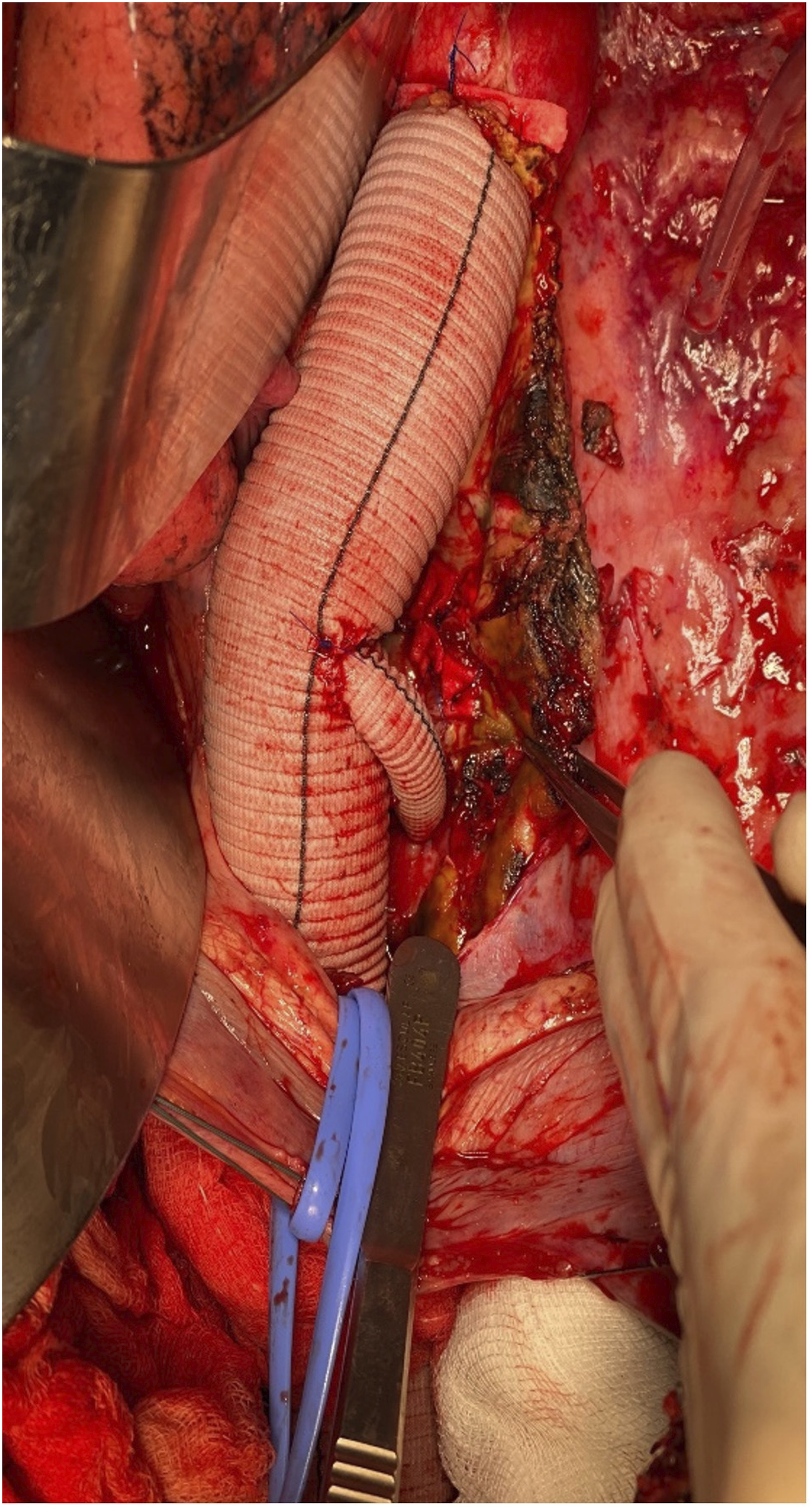
At 6-months follow up the patient was completely asymptomatic and did not present any sign nor symptoms of visceral and spinal ischemia. The CTA-scan confirmed the post-operative findings (Figure 5). Volume rendering of post-operative CTA showing thoracoabdominal aortic replacement with reimplantation of celiac trunk, superior mesenteric artery, right renal artery and a large intercostal artery.
Discussion
Open thoracoabdominal aortic repair is a challenging option, often characterized by high morbidity and mortality. The most important postoperative complications are paraplegia and renal failure. 1
LeMaire et al. report major adverse outcomes in 15.9% of procedures, including the 8.4% that resulted in early mortality. 2
In our case, the patient was undergoing multivisceral malperfusion due to the compression of the true lumen by the false lumen. Endovascular treatment was not suitable because of the absence of both retrograde and antegrade access in the context of the compression of the true lumen.
During the open repair, one of the main issues is the prevention of visceral ischemia due to proximal cross-clamping. Many distal aortic perfusion systems can be used: deep hypothermia, left heart bypass, femoro-femoral extra-corporeal circulation, selective methods such as side branches from the distal aortic perfusion line.
In this case we adopted a temporary passive arterial shunt between the left axillary artery, celiac trunk, and superior mesenteric artery. The main advantage is the immediate organs perfusion after the aorta is opened and the avoidance of a heavy systemic anticoagulation Moreover, the anesthesiologic management was more physiological, since the passive shunt eliminates the necessity for the pump to determine the pressures, the filling volumes, cardiac return with possibility to act in presence of real vital parameters.
Renal protection was provided by a histidine-tryptophan-ketoglutarate solution (Custodiol; Dr Franz-Kohler Chemie GmbH, Bensheim, Germany), whose composition should reduce the cellular swelling, toxicity, and damage caused by intraoperative ischemia. Tshomba and Kahlberg et al. performed a prospective comparative study on the use of 4°C Custodiol versus 4°C Ringer Lactate and showed that Custiodiol provides better protection against ischemic renal injury, reducing acute kidney injury incidence and improving perioperative trend of eGFR despite the longer total renal ischemic time. 3
As far as spinal cord injury is concerned, reported incidence varies from 16% to 31%.4,5 Several techniques are available for spinal cord protection, such as intraoperative and postoperative cerebral spinal fluid drainage (adopted in this case), pharmacologic protection, moderate hypothermia,, atrio-femoral bypass, direct renal, visceral, or epidural cooling, hypothermic circulatory arrest.
The reimplantation of intercostal arteries is still a matter of debate. Safi et al. affirm that reimplantation of patent thoracic intercostal arteries T11 and T12 is indicated; while reimplantation of T9 and T10 lowers the risk of late neurologic deficit, probably by decreasing the spinal cord’s vulnerability to changes in blood and cerebrospinal fluid pressure in the days after surgery. 6 On the other side, after comparing thoracic and thoracoabdominal aortic surgery with versus without intercostal artery reimplantation, Wynn et al. show that intercostal artery reimplantation does not produce a statistically significant reduction in SCI, even in the highest-risk patients. 7
In this case, after identification of a good caliber intercostal artery and evaluation of its run-off, we decided to reimplant it on the Dacron graft with interposition of another Dacron prosthesis. This procedure not significantly prolonged the intervention, and the intra-operative Duplex scan was satisfying.
Our patient did not report any peri-operative organ damage. We believe that visceral and renal perfusions and spinal protection played an essential role, probably in association with the existing axillo-femoral bypass that ensured a minimal retrograde perfusion.
Conclusion
Chronic aortic dissection implies a high risk for late aorta-related events and reinterventions, and the ideal management strategy must be tailored on the single patient’s features to provide the maximal efficacy and safety.
This experience suggests that in complex post-dissection states where endovascular treatment does not ensure a complete efficacy, open surgery represents a valid option, if performed in experienced centers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.