
Abstract
Purpose
To explore the life experiences of patients who have been discharged after undergoing extracorporeal membrane oxygenation (ECMO) support.
Design
A qualitative descriptive approach was used.
Methods
Patients who have undergone ECMO support and have been discharged were recruited. Thirteen participants were involved in this study. The data were collected through a semi-structured interview and analyzed using the Colaizzi method.
Findings
Four major themes in life experiences were reported by the participants: changes in physical function, changes in psychological state, active adaptation to daily life, and substantial rehabilitation needs.
Conclusion
Different, continuous, and convenient post-discharge physical and mental interventions, social support, spiritual support, and rehabilitation services should be provided according to the patient’s circumstances. We also call on the government to increase the patient reimbursement rate for ECMO treatment. These measures may help to improve the quality of life of patients.
Introduction
Extracorporeal membrane oxygenation (ECMO) is a type of cardiopulmonary bypass support for critically ill patients, especially those with cardiopulmonary failure who do not respond to standard treatments. 1 From 1989 to 2016, over 22,500 adults were treated with ECMO worldwide. 2 And between 2016 and 2018 in China, 5891 cases were treated with ECMO. 3 Many evidence described the percentage increase in use of ECMO with time. Approximately 6% of the critically ill patients with Middle East respiratory syndrome (MERS) were reported to receive ECMO support in a multicenter retrospective cohort between 2012 and 2015. 4 During very early stage of the coronavirus disease of 2019 (COVID-19) outbreak in Wuhan, 47% required mechanical ventilation and 11.1% required ECMO support in a small cohort of intensive care unit admitted patients. 5 This increase underscores the effectiveness of ECMO. The World Health Organization has recommended ECMO as an adjunct to traditional mechanical ventilation for the treatment of the COVID-19. 4
Despite its efficacy, ECMO is also associated with adverse effects. Patients may also experience persistent psychological symptoms, including anxiety, depression, and post-traumatic stress disorder (PSTD) as well as physical symptoms, such as lower limb ischemia or paresthesia, even after discharge.1,5 These changes may reduce the ability of patients to bring out their potential, and affect their lifestyle and social function, which greatly reduces their quality of life (QoL).6–9
By evaluating the QoL, we can understand the life satisfaction and happiness among the patients determined by the factors of physiological, psychological, social functioning, and spiritual, which could provide information to care teams to improve transitional care strategies. 10 Although previous studies have mainly used a quantitative cross-sectional approach to measure and demonstrate a decrease in QoL in all aspects after ECMO support, the reasons for the decrease are unknown. At the same time, the needs for rehabilitation due to the diseases and complications and residual effects also need to be further understood. We conducted a qualitative study to explore the reasons for changes in quality of life for patients following ECMO.
Methods
Study design
Descriptive phenomenology was used to explore the patients in this post-ECMO study. The standards for reporting qualitative research (SRQR) were followed. 11 The data was collected by the semi-structured interview, and analyzed by the Colaizzi method 12 (item #5 of the SRQR).
Setting and sample
Characteristics of participants (N = 13).
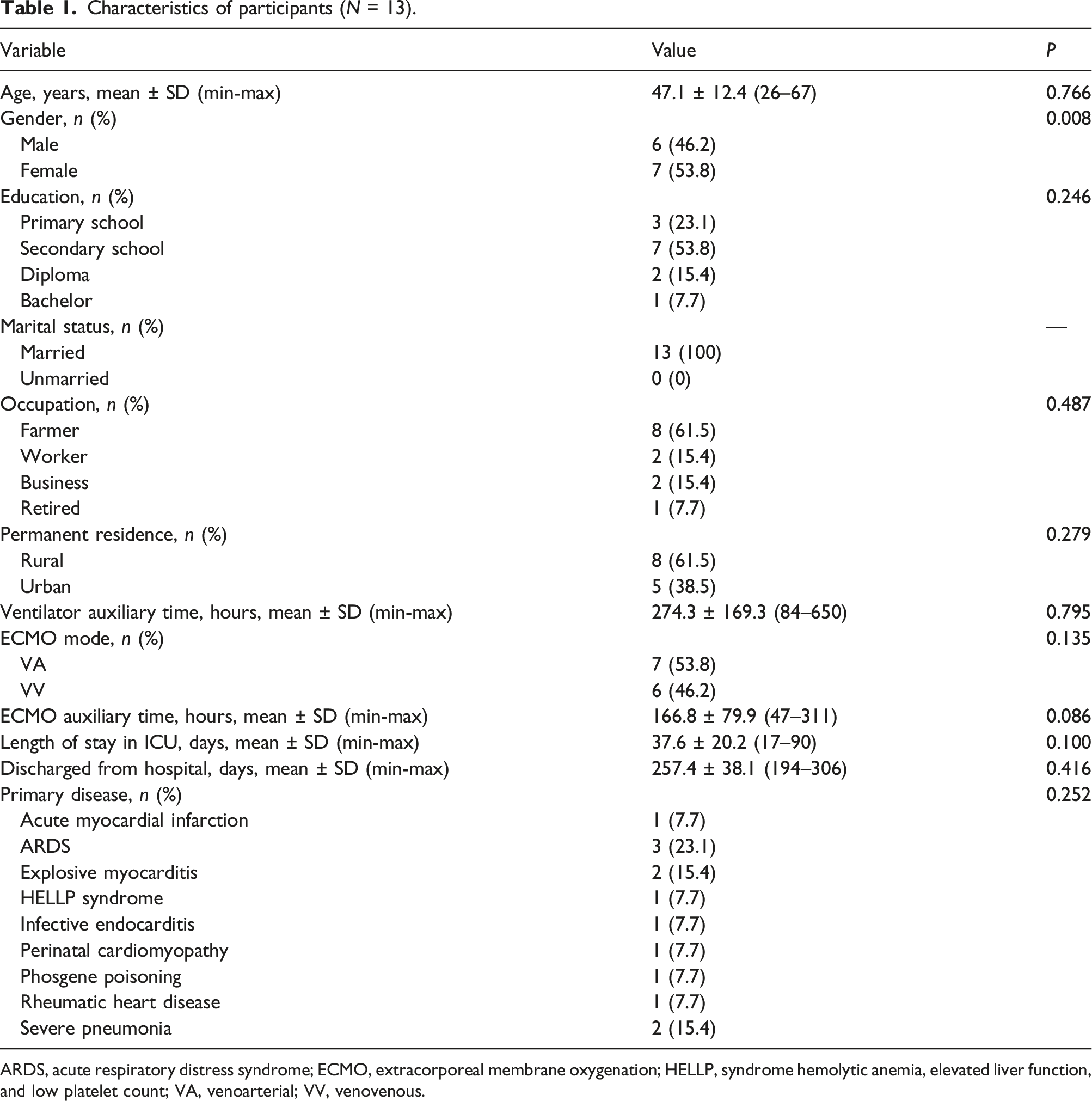
ARDS, acute respiratory distress syndrome; ECMO, extracorporeal membrane oxygenation; HELLP, syndrome hemolytic anemia, elevated liver function, and low platelet count; VA, venoarterial; VV, venovenous.
Ethical considerations
The ethics committee of the hospital permitted the research (No. llsc-20190306). Before the interview, each participant had been informed of the anonymity, confidentiality and freedom to withdraw from the study by the first author. All participants had signed informed consents, which were then encapsulated by the fourth author in opaque bags bearing unique numbers such as E1-E13 and kept in a safe box. The recordings were encrypted and destroyed at the end of the study (items #7 and #9 of the SRQR).
Data collection
The first author, who was also the interviewer, has a bachelor’s degree and is a co-chief nurse. He/She is also the head nurse at the Cardiac Surgery Intensive Care Unit (CICU) of the hospital with 15 years of experience and expertise in the domain of ECMO (item #6 of the SRQR). The second and third authors, both of whom have a master’s degree and are the charge nurses, have been involved in nursing for more than 7 years and, together with the first author, were responsible for data transcription.
Question sets.
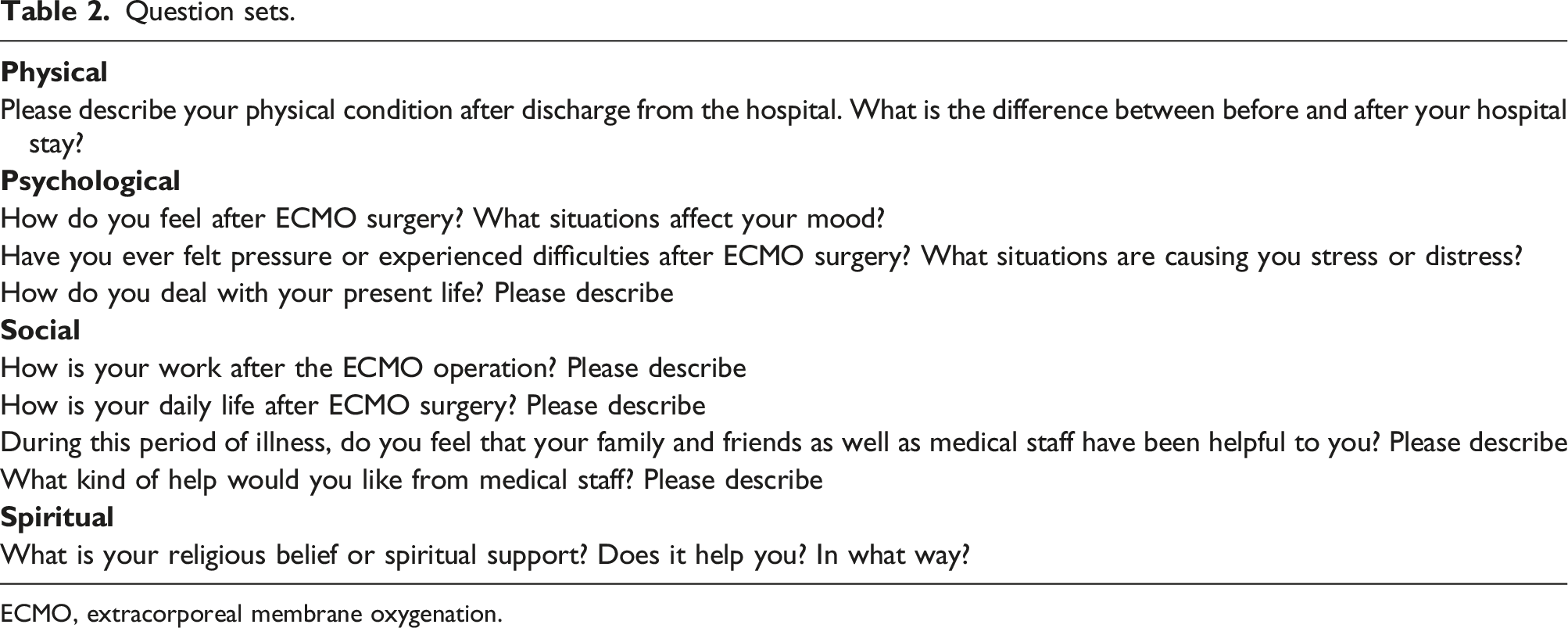
ECMO, extracorporeal membrane oxygenation.
Data analysis
An example of data analysis.
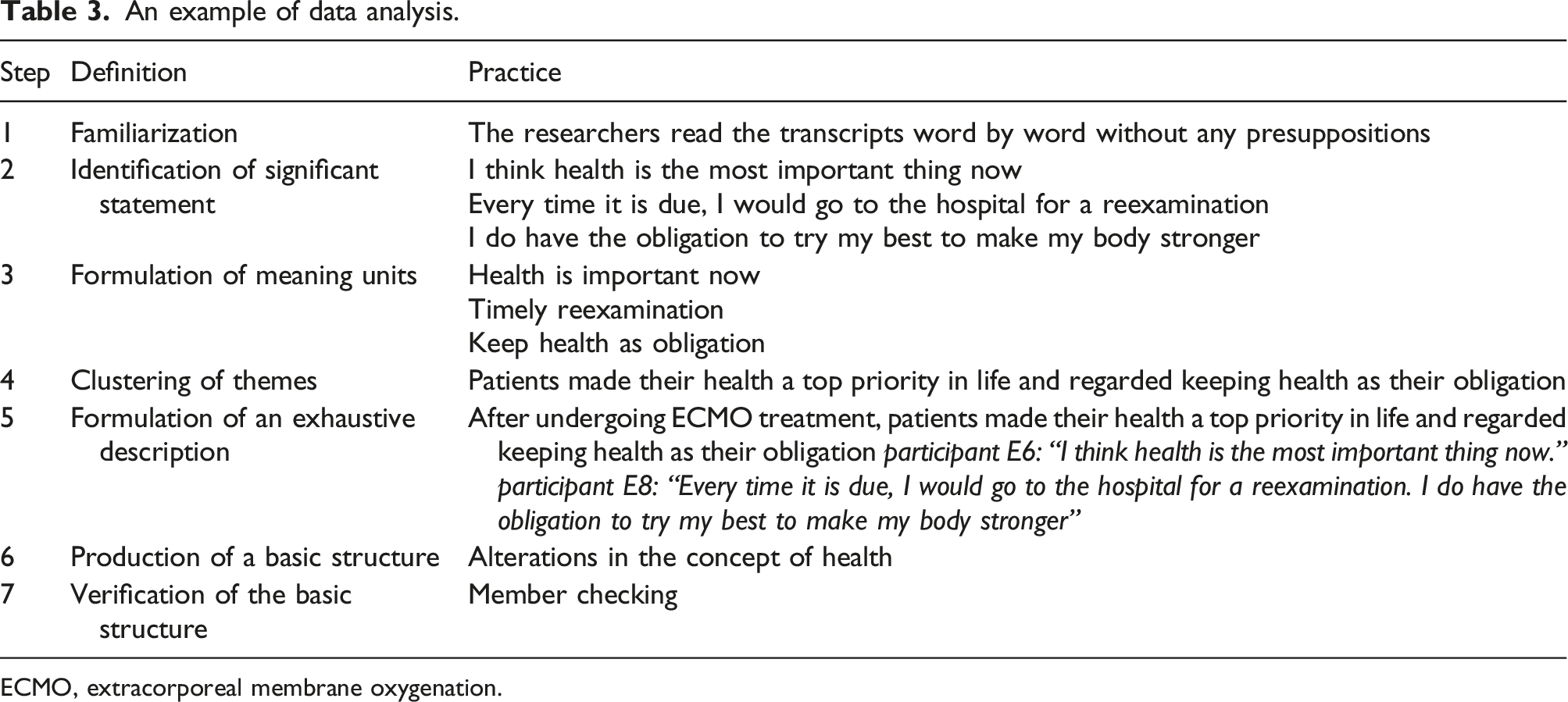
ECMO, extracorporeal membrane oxygenation.
Data rigor and trustworthiness
To ensure rigor, Guba and Lincoln’s
14
guidelines were used. The whole study was guided by a qualitative research expert, who was the fifth author in the study. Thematic saturation was reached after interviewed 12 participants and another participant was included. In the process of data analysis, the interviewer maintained a neutral attitude by using the reflective diaries and strictly followed the Colaizzi method. At each step, the interviewer verified and reached a consensus with at least 2 other researchers. The themes developed in the study were richly described below. Also, the memos and an audit trail were used to maintain transparency. To ensure authenticity and validity, the findings, and analysis of each interview were sent to the corresponding participants for member checking (item #15 of the SRQR). The schematic diagram of the research process was shown in Figure 1. Schematic diagram of research process.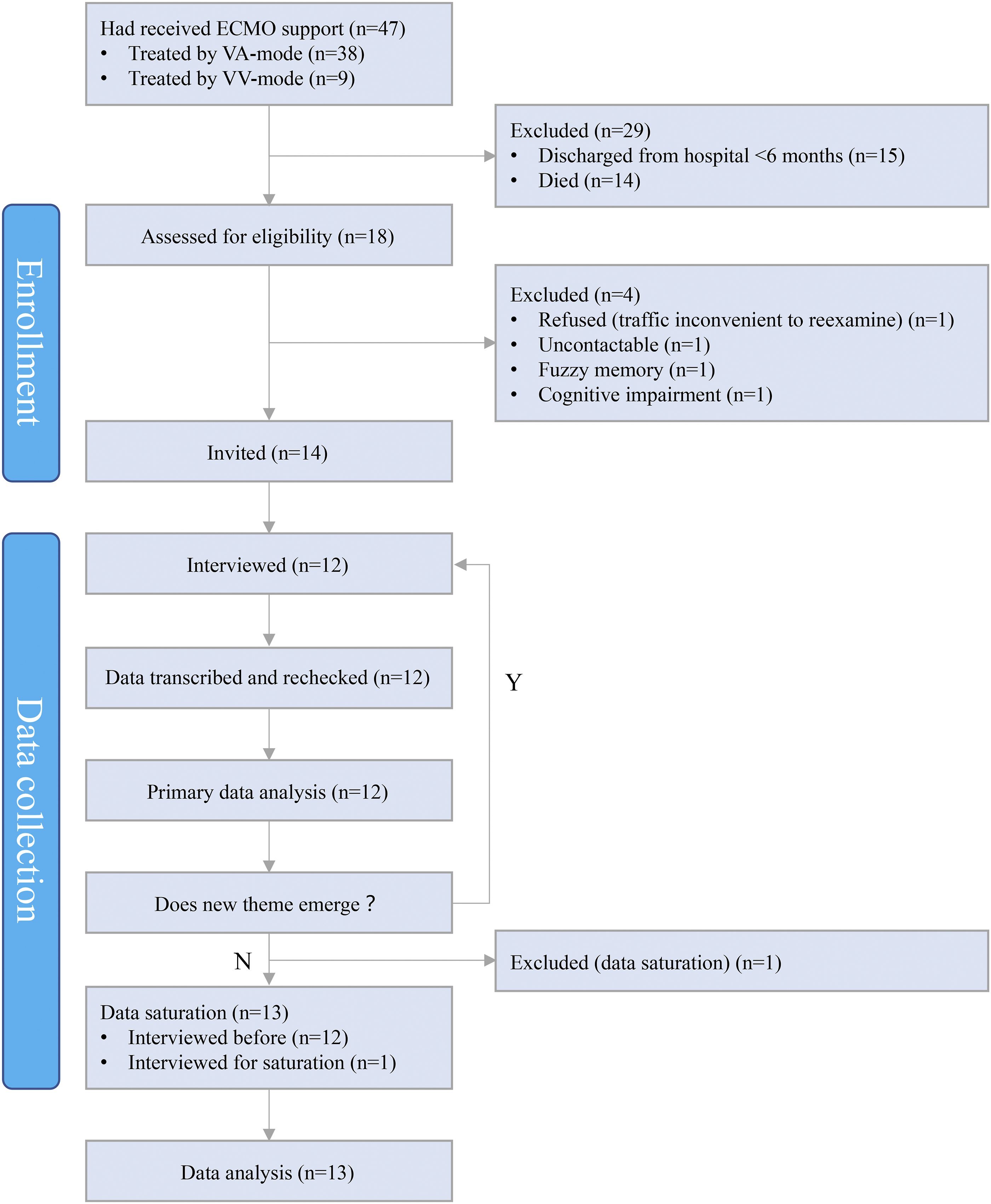
Results
The characteristics of participants were shown in Table 1. The results showed that there was no significant difference between the characteristics and the complications/residual effects except gender (p = 0.008).
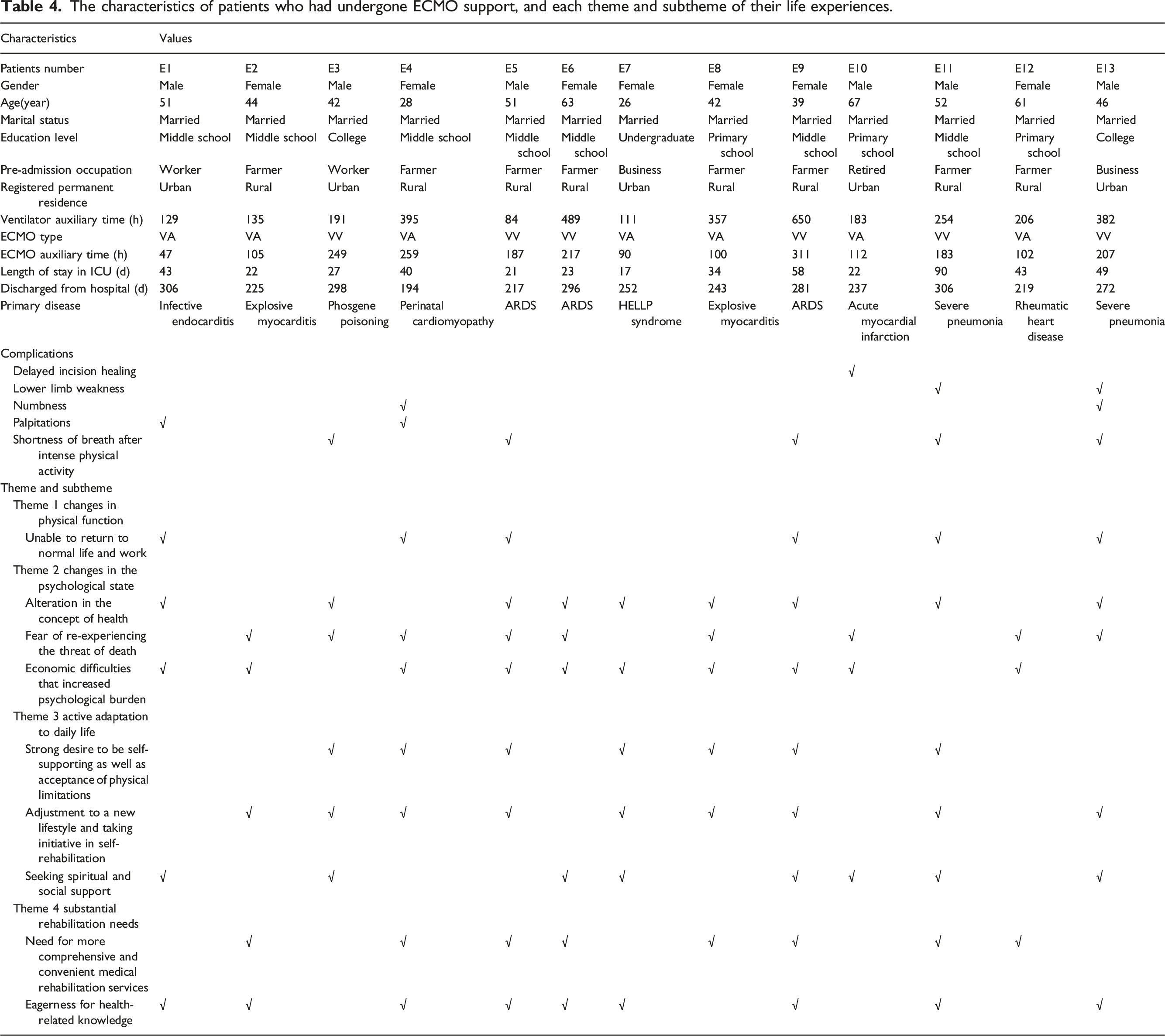
The characteristics of patients who had undergone ECMO support, and each theme and subtheme of their life experiences.
Changes in physical function
After ECMO support, some participants experienced complications and residual effects that lasted up to 6 months after discharge resulting in poor self-care ability, reduced social contact, and an inability to return to work. Totally, it showed that the number of patients occurred complications and residual effects were 8 in Table 4, respectively, E1, E3, E4, E5, E9, E10, E11, E13. Delayed incision healing was 1, lower limb weakness were 2, numbness were 2, palpitation were 2, and shortness of breath after intense physical activity were 5. Furthermore, participants who underwent the venoarterial (VA) mode of ECMO were more experienced delayed incision healing, lower limb weakness, numbness, and palpitations; those who underwent the venovenous (VV) mode of ECMO were more experienced shortness of breath after intense physical activity.
Participant E4: “After discharge, my heart is still not good. Now I seldom go out and stay at home a lot. I feel that I can’t keep up with others’ ideas.”
Participant E11: “Now when I move, I still feel out of breath and my chest is uncomfortable. I don’t know when I can resume physical work, so I want to go out and do something.”
Participant E13: “My right index finger and middle finger are numb and have no strength, so I can’t put on clothes or do anything. So is my right leg, if I squat down it would hurt so much that I can’t stand up, so I have to use a special stool with a hollow on it when going to the toilet.”
Changes in the psychological state
The near-death experiences and heavy financial burden during ECMO treatment not only caused psychological pressure, such as fear and anxiety but also changed participants' health perception after discharge. In this section, three subthemes emerged: alterations in the concept of health, fear of re-experiencing the threat of death, and economic difficulties that increase psychological anxiety. It showed that 9 patients changed their concept of health, 9 were feared of re-experiencing the threat of death, and 10 felt heavy financial burden (see Table 4).
Alterations in the concept of health
After undergoing ECMO treatment, patients made their health a top priority in life and regarded keeping health as their obligation. Additionally, among 9 patients who alternated their concepts of health, the results showed 88.9% had a middle school education or above.
Participant E6: “I think health is the most important thing now.”
Participant E8: “Every time it is due, I would go to the hospital for a reexamination ... I do have the obligation to try my best to make my body stronger.”
Fear of re-experiencing the threat of death
During treatment, 9 participants, aged 28–67 years, with 100–259 h of duration of ECMO or length of ECMO support, experienced the feeling of being close to death. After discharge, they were afraid to recall their resuscitation as it elicited psychological distress.
Participant E3: “I still have a psychological shadow when I work in this company. When my lungs feel uncomfortable, I feel out of breath. This reminds me of the last time I had an accident (phosgene poisoning) and I’m afraid that the same accident will happen again.”
Participant E8: “If I feel uncomfortable, I will go to the hospital for treatment. I cannot delay treatment.”
Participant E12: “I’m so afraid of dying and worry that I’m going to be the same as last time, so I stay at home.”
Financial difficulties that increased psychological anxiety
The consumables used for ECMO are imported and expensive, leading to considerable medical costs for patients. The duration of ECMO or length of ECMO support averaged (153.00 ± 85.69) hours. In Table 4, 60.0% of the 10 patients who felt financial burden lived in rural areas. Additionally, 4 patients could not return to work after being discharged and, therefore, their income declined to result in greater economic pressure on their families.
Participant E5: “I spent a lot of money in the hospital, and it still hasn’t been reimbursed because I have no time to apply for a medical referral certificate. My son borrowed the money from his other relatives and friends for me to see a doctor. What will I do if I can’t pay my bills?”
Participant E6: “I feel very guilty that my son spent so much money on my medical treatment ... So I can’t encumber my son with my illness.”
Participant E10: “My family is under a lot of financial pressure. I had to sell the house to pay for the treatment. Although it was good to save my life, I still hope that I can earn more money to make my life better.”
Active adaption to daily life
After discharge, participants gradually accepted their physical limitations and adjusted to their new lives through self-supporting, rehabilitation, and seeking spiritual and social support. In this section, 7 patients had strong desire to be self-supporting as well as acceptance of physical limitations, 9 patients had adjusted to a new lifestyle and taking initiative in self-rehabilitation, 8 patients were seeking spiritual and social support. Three subthemes emerged: a strong desire to be self-supporting as well as acceptance of physical limitations, adjustment to a new lifestyle and taking initiative in self-rehabilitation, and seeking spiritual, and social support.
Desire to be self-supporting and acceptance of physical limitations
It showed that 7 patients, aged 26–52 years old, had strong desire to be self-supporting as well as acceptance of physical limitations. Participants identified self-belief as a source of strength and support and worked hard to adjust their emotions and accept their physical limitations post-surgery.
Participant E11: “My body is my own. No matter what anyone tells me about being strong or things getting better, I believe the important thing is to cheer myself up.”
Participant E4: “I don’t even think about bad things now. Bodhisattva will bless me to get better every day.”
Participant E9: “I’m the man who has been to hell and back, so I have to be more optimistic, and I believe my body will get better as long as I keep doing exercise.”
Adjustment to a new lifestyle and taking initiative in self-rehabilitation
In Table 4, 9 patients had adjusted to a new lifestyle and taking initiative in self-rehabilitation. Among these participants, 6 were farmers, 2 were in business, and 1 was worker. Participants took the initiative to change their lifestyles and carried out self-rehabilitation through exercise and health care based on traditional Chinese medicine.
Participant E7: “I haven’t been to work for a long time since I can’t do heavy work. I lead a regular life. I eat and sleep on time.”
Participant E2: “I dance in the public square every day. I will go there in the morning and evening and usually exercise for 30–60 min each time.”
Participant E13: “I have been treated with Chinese traditional medicine and it helps me to improve my health by food therapy.”
Seeking spiritual and social support
In this section, 8 participants, among them, 3 were farmers, 2 were workers, and 2 were in business, were seeking spiritual and social support. Participants, all married, believed that their survival was the result of their religious beliefs and willingness to seek medical care, and cited family and friends as sources of spiritual support.
Participant E13: “I believe in the Buddha, and the Buddha has protected me. Maybe you don’t believe me, but the doctor asked me to calm down and I cooperated with him when I was going to die. I just calm myself down by reciting the great mercy mantra in my mind.”
Participant E6: “When I was in the hospital, all my relatives and friends helped me with the hospital expenses. After I was discharged, they often visited me. I was advised to eat more nutritious food and be optimistic about everything.”
Substantial rehabilitation needs
The results, Table 4, showed that 8 participants were in need for more comprehensive and convenient medical rehabilitation services and 9 were in eagerness for health-related knowledge. In the process of seeking rehabilitation, all 10 participants yearned for more comprehensive, convenient medical services and professional health advice because existing medical conditions cannot meet their needs. In this section, two subthemes emerged: the need for more comprehensive and convenient medical rehabilitation services and eagerness for health-related knowledge.
Need for more comprehensive and convenient medical rehabilitation services
The results showed 8 participants who were in need for more comprehensive and convenient medical rehabilitation services were all farmers and lived in rural areas. Participants believed that although they required continued rehabilitation, the current rehabilitation services at the hospital were unable to meet their needs.
Participant E8: “I couldn’t walk around with my leg (pointing at the right leg). I have been to see a doctor several times, but he gave me some vague information on how it can be cured and only said that it might be a nerve injury.”
Participant E2: “My sleeping quality still hasn’t been very good and I felt heartbroken in the middle of the night. The doctor said it is not a physical problem, but maybe a psychological problem. I hope that the hospital can provide me with psychotherapy directly rather than tell me to see a psychologist.”
Participant E5: “We live in a rural area. It is not convenient for us to go to the urban area for a check-up, so I got reexamined in the township health center, and do not know whether it is useful or not.”
Eagerness for health-related knowledge
The results showed that 9 participants were in eagerness for health-related knowledge. Among them, 6 were farmer, only 2 had college education or above, 4 were treated by VA mode of ECMO and 5 were VV, 6 were suffering complications and residual effects of ECMO support. Participants wished to continue to receive professional health advice after discharge.
Participant E2: “I would like to know how I can sleep well.”
Participant E7: “I was able to get rid of such a serious disease last time. I am most grateful to the doctors and nurses for their skills. Now I would like to know how to give birth to a baby safely.”
Participant E13: “I have thought about how to improve my body by myself and I hope that the doctor can tell me some professional methods.”
Discussion
In Table 1, the significance between the gender and complications/residual effects was inconsistent with previous studies.5,7,9 This may be related to the small sample size, which needs to be expanded.
The lives of patients after ECMO support are plagued by complications and residual effects. Six months after discharge, patients still suffered from physical and mental complications/residual effects associated with ECMO treatment, as previously reported.15,16 The participants who underwent the VA mode of ECMO reported lower extremity symptoms, possibly because the femoral arteriovenous catheter used in the VA mode is more likely to result in lower limb ischemia and affect lower limb muscle nerve function. 1 Additionally, some patients who underwent the VV mode of ECMO complained of shortness of breath after intense physical activity, which may be related to incomplete recovery from the primary disease affecting lung function. Therefore, medical staff should pay attention to physical and mental complications and residual effects in patients after ECMO support and provide better long-term care after their discharge.
Post-ECMO patients are under substantial pressure
Participants’ stress was mainly associated with fear of death, increased financial burden, and the difficulty of returning to work. In this study, most patients experienced the threat of death in ICU and expressed fear of death, which is consistent with Tramm et al’s. 5 study. Fear of death may be related to the experience of resuscitation in the ICU. Several studies have shown acute stress during resuscitation can harm patients' mental health, such as endotracheal intubation and mechanical ventilation, as well as the use of psychotropic drugs for analgesia and sedation, which could easily cause symptoms of PTSD within a year of discharge, such as fear, avoidance, and overreaction.17–19 Additionally, the increased financial burden and difficulty in returning to work also contribute to the substantial pressure faced by patients after discharge. An investigation revealed that multiple factors contributed to increased financial pressure on patients after ECMO support, including the cost of ECMO treatment, a low percentage of medical reimbursement and, in some cases, the inability to continue working after discharge. 20 Therefore, medical staff should provide psychological interventions that will have maximum effectiveness based on the stress for each patient. Additionally, we appeal to the government to provide more medical insurance support for ECMO consumables to relieve the financial burden on patients.
The patients’ adoption of positive attitude toward life after ECMO, along with multiple sources and types of support, are essential for their recovery
Most participants exhibited a positive coping style and adapted to life after discharge. This may have been promoted by traditional Chinese cultural aphorisms, such as, “Those who survive a catastrophe are bound to have good fortune” and “it’s better to stay alive than to die”. As previous studies have reported, most discharged patients were satisfied with their survival and believed that nothing is more important than their health. 8 The reason may be that the patient feels awe for life after experiencing such a serious disease. Additionally, the participants coped with discomfort using exercise and traditional Chinese medicine, as in the cases of patients with chronic diseases.21,22 Based on our data, we suggest that doctors and nurses should make full use of patients’ positive attitude in rehabilitation by providing more comprehensive professional knowledge of rehabilitation, including various symptoms, recommending different methods of self-directed exercise, and advice on dietary choices. We also found that multiple sources and types of support like medical treatment, nursing, rehabilitation, psychological care were beneficial to the health of patients after ECMO support, this is in agreement with previous work indicating that support from friends and family has positive effects on patient’s health and recovery.23,24 Most patients acknowledged that faith played an important role in their survival. Religious belief is an expression of spirituality, of which Buddha is one interpretation25,26; this can help a patient regain meaning in his or her life during their illness and increase their confidence that it can be overcome. 27 In addition to encouraging social support from ECMO patients’ family, friends, and fellow patients, medical staff should provide spiritual care according to patient’s cultural and religious needs.
Patients who have undergone ECMO support have a strong desire for post-discharge rehabilitation services and are eager for professional rehabilitation knowledge
After being discharged from the hospital, patients were faced with a variety of daily life challenges and changes to their health. Accordingly, they expressed a strong desire for professional support, hoping it could help to solve their health problems and allow them to recover as quickly as possible to alleviate their difficulties, which is consistent with Chen et al’s 1 study. The patients after ECMO treatment still require ongoing medical services after discharge for functional rehabilitation training and mental health guidance. 28 However, the rehabilitation needs of some participants were not being met, such as lack of specific psychological rehabilitation strategies and health education, traffic inconvenience in reexamination. Hence, medical personnel should strengthen post-discharge rehabilitation support for ECMO patients. Moreover, given the inequality between urban and rural medical resources, efforts should be made to provide convenient and high-quality rehabilitation guidance and aid to all patients.
Limitations
Given the relatively homogeneous patient demographics (e.g. all were married with a relatively low educational level), a prudent interpretation of the results in this study is necessary. In addition, cultural and ethnic differences may play a pivotal role in the life experience of these patients thus the generalizability of this study may be limited. Overall, further large-scale multicentre studies are warranted to obtain more comprehensive data on the postoperative lives of ECMO patients.
Conclusion
We identified significant changes in four major themes of life experience after ECMO support, reflecting the real-world situation in our Chinese population and providing reference value for race-specific solutions. We suggest managers should provide detailed plans of comprehensive nursing care, including enacting different intervent 6-12 mouths based on primary disease and ECMO mode, focusing on patients with mental health problems, providing social and spiritual support from many aspects, providing professional guidance and convenient rehabilitation. Also, we appeal to the government to increase the patient reimbursement rate for ECMO treatment. These may help improve the QoL of patients after ECMO support.
Supplemental Material
Supplemental Material - Post-discharge experiences of patients with extracorporeal membrane oxygenation support: A qualitative study
Supplemental Material for Post-discharge experiences of patients with extracorporeal membrane oxygenation support: A qualitative study by FengZhen Wang, YuHao Zhang, ShuJing Wu, HongYing Xie, DongMei Lin, XianMin Wen, ZhiSheng Duan, YuFeng Lu, ZiYou Liu, Shuo Hu and Jian Liu in Perfusion
Footnotes
Acknowledgements
The authors thank the participants of this study.
Author Contributions
(I) Conception and design:Wang FZ and Zhang YH. (II) Administrative support:Wu SJ and Xie HY. (III) Provision of study materials or patients:Lin DM and Wen XM. (IV) Collection and assembly of data:Duan ZS and Lu Y. (V) Data analysis and interpretation:Liu ZY, Hu S and Liu J. (VI) Manuscript writing: All authors. (VII) Final approval of manuscript: All authors
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Gannan Medical University (grant no. ZD201829).
Data availability statement
Data supporting the results reported in this article can be found in the Results section.
Ethical considerations
The Ethics Committee of the First Affiliated Hospital of Gannan Medical University permitted the research (No. llsc-20190306).Written informed consent was obtained from all participants.
Consent
All participants provided written, informed consent before participation. Audio data of participants were stored on a computer with a secure password during the study period. All files were deleted after the study to protect the privacy of the participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.