
Abstract
Objective
Delayed neurocognitive recovery (dNCR) remains a common complication after surgery and the incidence of it is determined 30–80% after cardiac surgery with cardiac bypass (CPB) in eldery patients. Many researchers have identified that neuropsychological complications emerge from insufficient cerebral perfusion. Relative cerebral hyperperfusion also disrupts cerebral autoregulation and might play a significant role in dNCR development. The aim of this study is to determine hyperperfusion in the middle cerebral artery during CPB influence to dNCR development and brain biomarker glial fibrillary acidic protein (GFAP) impact in diagnosing dNCR.
Designs and methods
This prospective - case control study included patients undergoing elective coronary artery bypass grafting or/and valve surgery with CPB. For cognitive evaluation 101 patients completed Addenbrooke’s cognitive examination - ACE-III. To determine mild cognitive dysfunction, cut - off 88 was chosen. Mean BFV was monitored with transcranial Doppler ultrasonography (TCD) and performed before surgery, after induction of anaesthesia, during CPB and after surgery. Preoperative BFV was converted to 100% and used as a baseline. The percentage change of cerebral blood flow velocity during CPB was calculated from baseline. Patients with decreased blood flow velocity were included for further investigation. To measure glial fibrillary acidic protein, blood samples were collected after anaesthesia induction, 24 and 48 h after the surgery. According to the ACE-III test results, patients with relative hyperperfusion were divided into two groups: with Delayed neurocognitive recovery and without dNCR (non‐dNCR group).
Results
101 patients were examined, 67 (69.1%) men and 29 (29.9%) women, age 67.9 (SD 9.2) Increased percentage of BFV was determined for 40 (39.60%) patients. There were no differences in sex, haematocrit, paCO2, aortic cross-clamping or CPB time between the two groups. Percentage change of BFV was 105.60% in the non-dNCR group and 132.29% in the dNCR group, p = .033. Patients who developed dNCR in the early post-surgical period were significantly older, p < .001 and had a lower baseline of BFV, p = .004. GFAP concentration significantly increased in the dNCR group 48 hours after surgery, compared to the non-dNCR group, p = .01.
Conclusions
Relative hyperperfusion during CPB may cause dNCR. Elderly patients are sensitive to blood flow velocity acceleration during CPB. GFAP concentration increased 48 h after surgery in dNCR group but did not have any connection with risk factors.
Keywords
Introduction
Cardiovascular disease (CVDs) is society’s biggest health problem. According to World Health Organization data from 2019, an estimated 17.9 million people died from CVDs in the world. While these types of diseases are often successfully treated through medication, frequently surgery is required to ensure a healthy and functioning heart. 1
Delayed neurocognitive recovery (dNCR) remains a common complication after surgery and the incidence of it is determined 30–80% after cardiac surgery with cardiac bypass (CPB) in eldery patients. 2 Many researchers have identified that neuropsychological complications emerge from insufficient cerebral perfusion.3,4 Cerebral hyperperfusion may also trigger a few neurological and neurosurgical conditions. Hyperperfusion syndromes cause increased blood pressure, vasodilatation, breakdown of the blood-brain barrier, and the development of cerebral oedema. 5 Hyperperfusion and its effects on dNCR have been observed and described during cardiac surgery with CPB in several studies.6,7
The glial fibrillary acidic protein (GFAP) is a specific biomarker of astrocytes and is detected only in the central nervous system. GFAP is a monomeric filament protein found in the astroglial skeleton and is a specific marker of brain damage. 8 Elevation in plasma has been reported in adults with traumatic brain injury, stroke, or after cardiac arrest.9,10 It is widely used and a promising biomarker in research after cardiac surgery and may help to identify dNCR.
The aim of this study is to determine hyperperfusion in the middle cerebral artery during CPB influence to dNCR development and brain biomarker GFAP impact in diagnosing dNCR.
Materials and Methods
The prospective observational study was performed for 101 patients, undergoing elective cardiac surgery with CPB. This study was conducted at the Department of Cardiothoracic and Vascular Surgery in the Hospital of Lithuanian University of Health Sciences Kauno Klinikos from April 2018 to April 2019. The study was approved, and permission was obtained from the Kaunas Bioethics Committee (Nr BE-2–3) and the Institutional Review Board (NCT03641833). All of patients signed participation in the research agreement. Patients with anamnesis of neurocognitive diseases, using agents affecting the central nervous system, multiple organ dysfunction syndrome, deficiency, carotid artery atherosclerosis with a reduction in artery diameter ≥50%, urgent or re-surgery, younger than 18 years were excluded from the study.
The cognitive functions were assessed for all patients 1 day before surgery and 7–10 days after surgery. Test for cognitive evaluations was chosen according The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). 11 The DSM-5 does not specify tests and their quantity to assess patients' cognitive functions. However, it is recommended to use tests that assess one or more specific cognitive functions, such as complex attention, memory, perception. It is advisible not to tests such as MMSE or MOCA, as they do not assess specific cognitive functions. ACE-III matches all requirement. It evaluates cognitive functions widely and provide broad assessment of cognitive domains.
The Addenbrooke’s cognitive examination (ACE- III) was chosen for cognitive evaluation. It is a comprehensive test, which assess cognitive functions and consists of five parts: assessment of focus and orientation, memory, language, verbal fluency, and spatial perception. The maximum score is 100 points, with a higher score reflecting better cognitive functions. The test is sensitive to cognitive dysfunction and dementia. Dementia is defined as a patient scoring 82 points or less. Cognitive impairment is diagnosed by scoring less than 88 points. A cut - off 88 points was chosen during the study. Cut of point was chosen acording ACE-III and M-ACE Administration and Scoring Guide and recommendations after adaptation in Lithuanian language.
12
According to the ACE-III test results, patients with relative hyperperfusion were divided into two groups: with dNCR (dNCR group) and without dNCR (non‐dNCR group). Study flow is shown in Figure 1. Study design and patient flow. MCA, Middle Cerebral Artery; BFV, Blood Flow Velocity; CPB, Cardiopulmonary Bypass, GFAP, Glial Fibrillary Acid Protein, ACE-III, Addenbrooke’s Cognitive Evaluation III.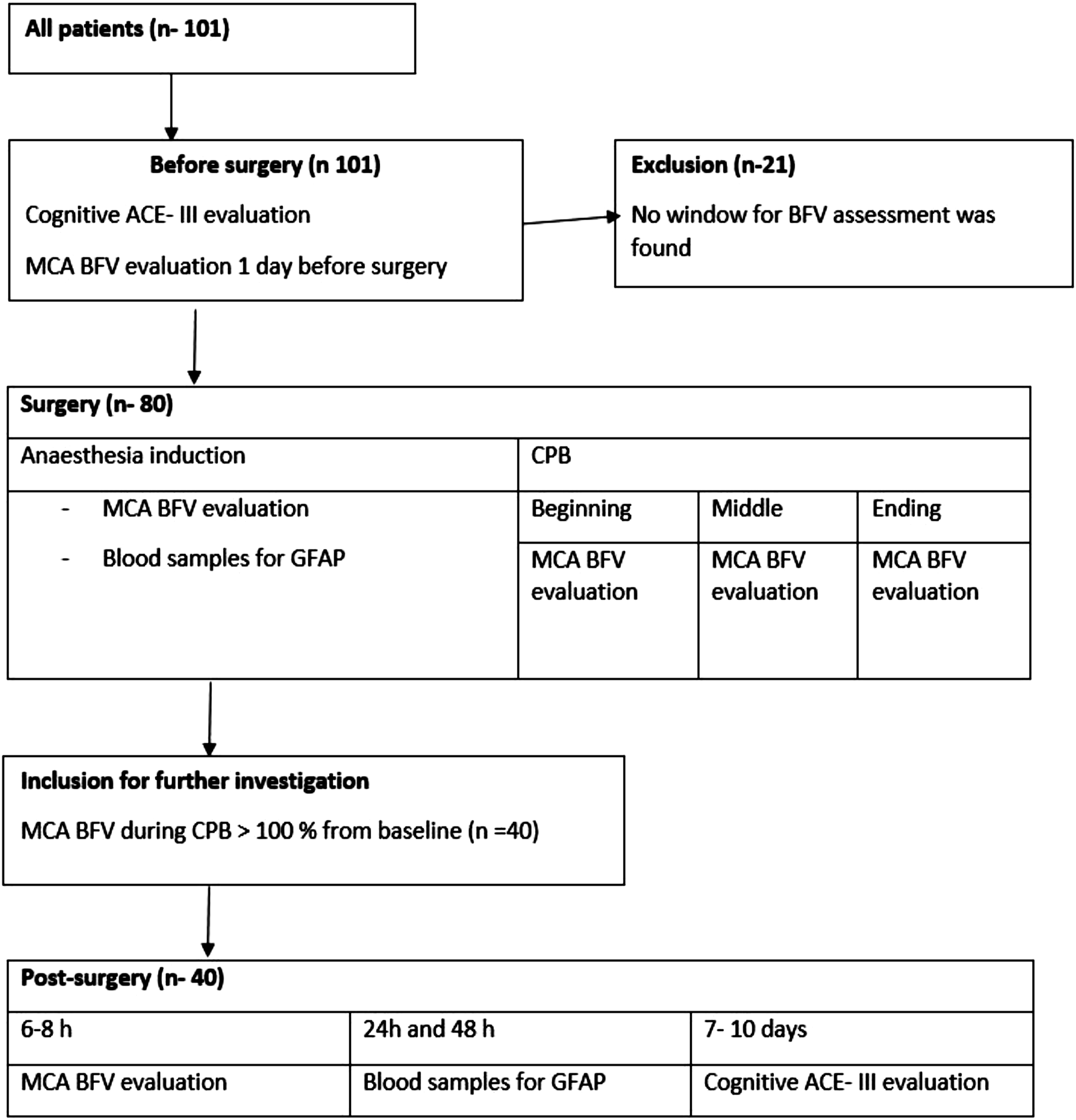
Perioperative period
All patients received of 1–2 mg oral clonazepam for premedication.
Standard endotracheal anaesthesia was applied. Induction was performed with fentanyl 1–2 μg/kg i. v.; propofol 2–2.5 mg/kg i. v.; rocuronium 0.5–0.7 mg/kg. Anaesthesia was maintained with sevoflurane (MAC 1–2%) and fentanyl (10–12 μg/kg) for analgesia. Lungs were ventilated with a supply of oxygen/air 50–60%. Middle sternotomy section and standard technique for anastomosis formation and valve surgery were performed. The CPB circuit was filled with 1200–1500 mL of Ringer’s acetate crystalloid solution and 10,000 IU of heparin. The CPB was established using a roller pump, Stockert III”, and hollow‐fiber membranous oxygenator „Compactflo D703” (Dideco, Mirandola, Italy). After full CPB support, pump flow was maintained at a cardiac index of 2.4 L/min/m. The myocardium protection was achieved using cold (2–4°C) St. Thomas solution according to clinical protocol. The surgeries were performed in mild hypothermia (32°C–34°C).
Vital signs monitoring included: electrocardiogram, heart rate, invasive arterial blood pressure, pulse oximetry, oesophageal and body core temperature, central venous pressure, urine output.
Cerebral perfusion and transcranial doppler ultrasonography technique
Normal function of the central nervous system depends on a constant and adequate supply of oxygen, glucose, and uninterrupted blood flow. The main mechanism of brain vessels autoregulation is changes in vascular lumen (dilation and constriction). There are a number of factors that can lead to vascular dysregulation. Transcranial Doppler ultrasonography (TCD) does not provide information about direct blood flow because the flow velocity of red blood cells are affected by the diameter of the blood vessels. The change in velocity measured by the TCD reflects changes in blood flow. There was a significant correlation between changes in cerebral blood flow (using 133Xe clearance) and changes in MCA flow velocity. 13
Sonara transcranial Doppler device was issued by, “Natus Neurology Incorporated”; Wisconsin, USA and delivered European authorized representative “Natus Europe GmbH” in 2013. This device was used for TCD technique. 2 MHz transducer was used for investigation and a temporal window was chosen for middle cerebral artery (MCA) blood flow velocity evaluation. Patients were excluded from the study if the window was not found, or the signal was not clear. The mean flow velocity was evaluated 1 day before surgery, after induction of anaesthesia, and at the beginning, middle and ending during CPB and post-surgery in operating room. The average of three bilateral measurements during CPB was used for calculation. All measurements were performed by the same operator. Preoperative BFV was converted to 100% and used as a baseline. The percentage change of cerebral blood flow velocity during CPB was calculated from baseline. It was included only these patients, which blood flow velocity were >100 proc. from baseline for further investigation
Glial fibrillary acidic protein
Blood samples for GFAP were collected after anaesthesia induction, 24 and 48 h after surgery. The samples were analysed by an enzyme‐linked immunosorbent assay kit and designed for the quantitative measurements of GFAP. Measurements were made according to the ABCAM (United Kingdom) manufacturer recommendations.
Statistical methods
The normality of the data was assessed with Kolmogorov–Smirnov or Shapiro–Wilk tests. Data distributed non normally, and were expressed as median (min, max). For nonparametric statistics, groups were compared by Mann–Whitney U‐test. Spearman correlation analysis was performed to determine the association between two variables (age and ACE - III test results after surgery; age and MCA BFV during CPB). The statistical analysis was performed using IBM SPSS Statistics software (v. 23.0 Chicago, IL, USA). Statistical tests were two‐sided, with p < 0.05 considered significant.
Results
ACE – III test results after surgery.

ACE – III, Addenbrooke’s Cognitive Examination-III, dNCR, Delayed Neurocognitive Recovery.
Data was distributed non normally and presented as the median (Q1-Q3). p – value – Mann Whitney test.
Characteristics of study population.
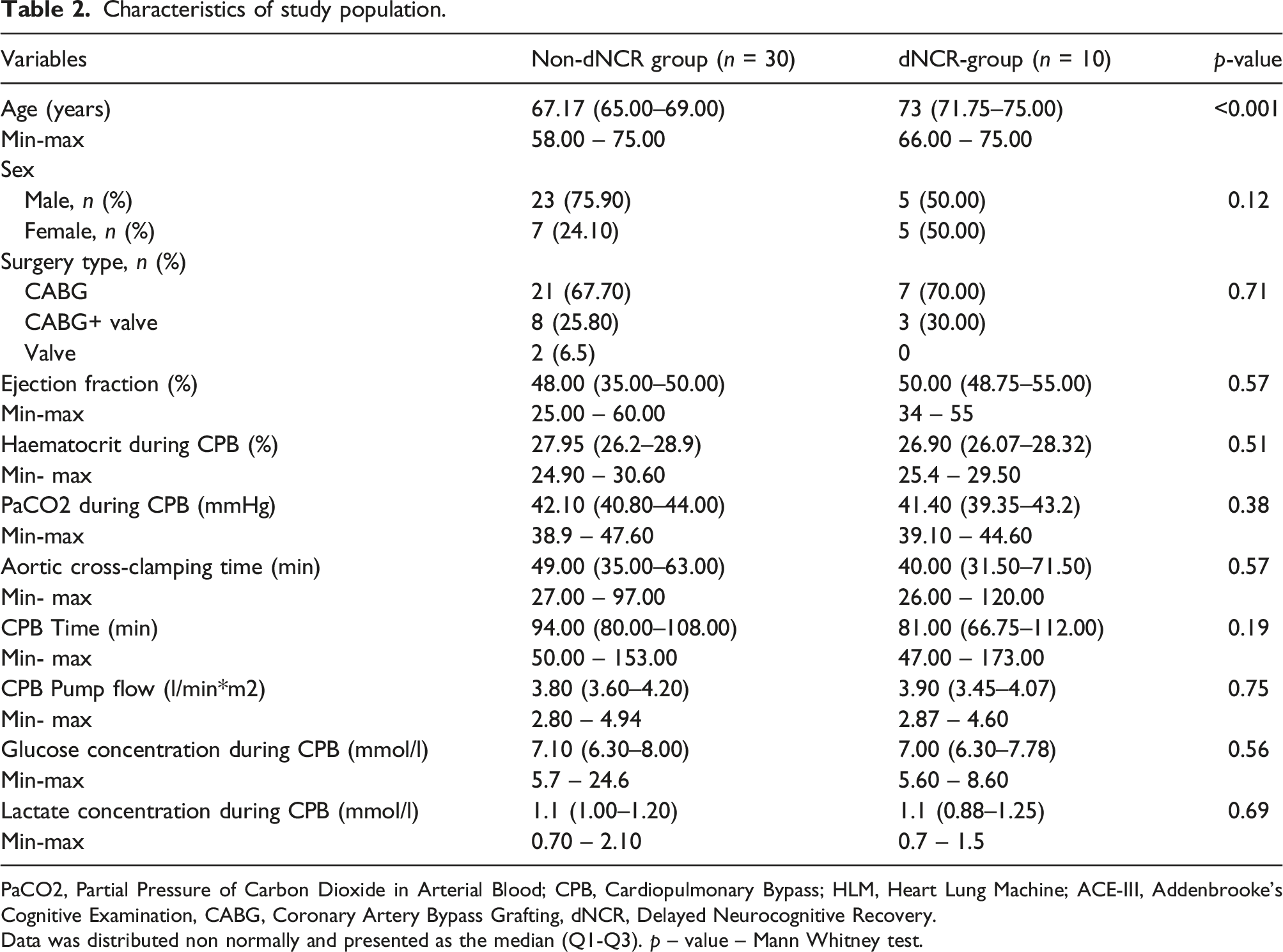
PaCO2, Partial Pressure of Carbon Dioxide in Arterial Blood; CPB, Cardiopulmonary Bypass; HLM, Heart Lung Machine; ACE-III, Addenbrooke’s Cognitive Examination, CABG, Coronary Artery Bypass Grafting, dNCR, Delayed Neurocognitive Recovery.
Data was distributed non normally and presented as the median (Q1-Q3). p – value – Mann Whitney test.
Middle cerebral artery blood flow velocity changes during surgery.
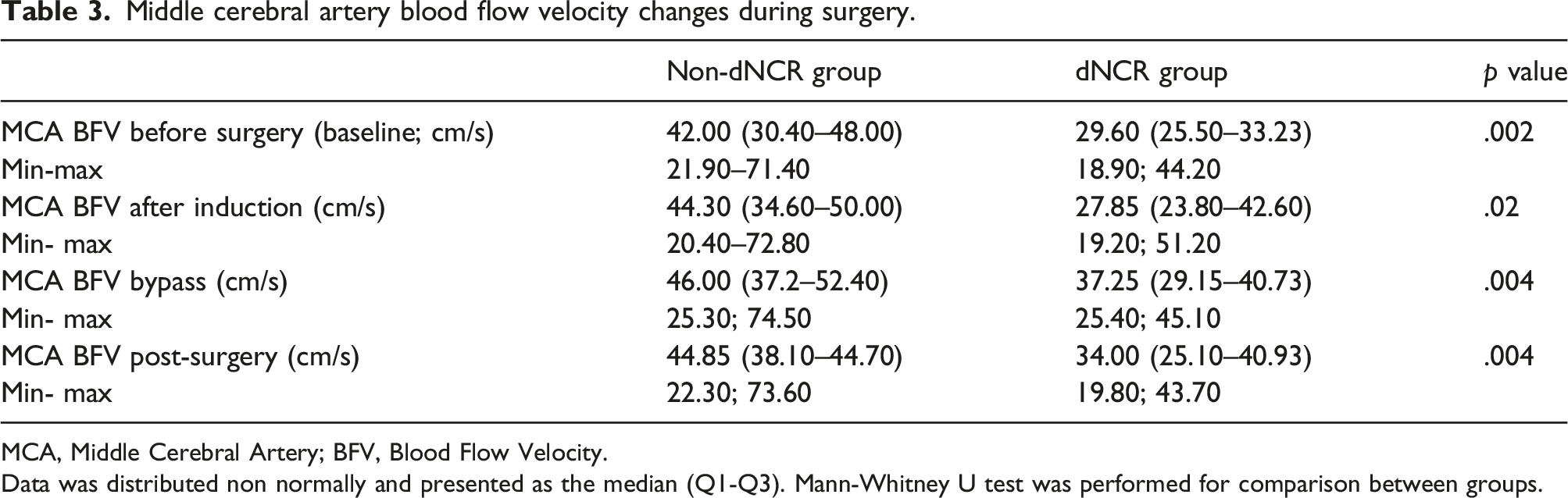
MCA, Middle Cerebral Artery; BFV, Blood Flow Velocity.
Data was distributed non normally and presented as the median (Q1-Q3). Mann-Whitney U test was performed for comparison between groups.
Percentage change of BFV was 105.60% (Q1 101.89- Q3 120.82; min 100.21- max 148.02) in the non-dNCR group and 132.29% (Q1 102.87–139.28; min 101.34- max 150.26) in the dNCR group, p = .033 (Figure 2). Percentage changes of BFV in non-dNCR and dNCR groups. MCA, Middle Cerebral Artery; BFV, Blood Flow Velocity; dNCR, Delayed Neurocognitive Recovery.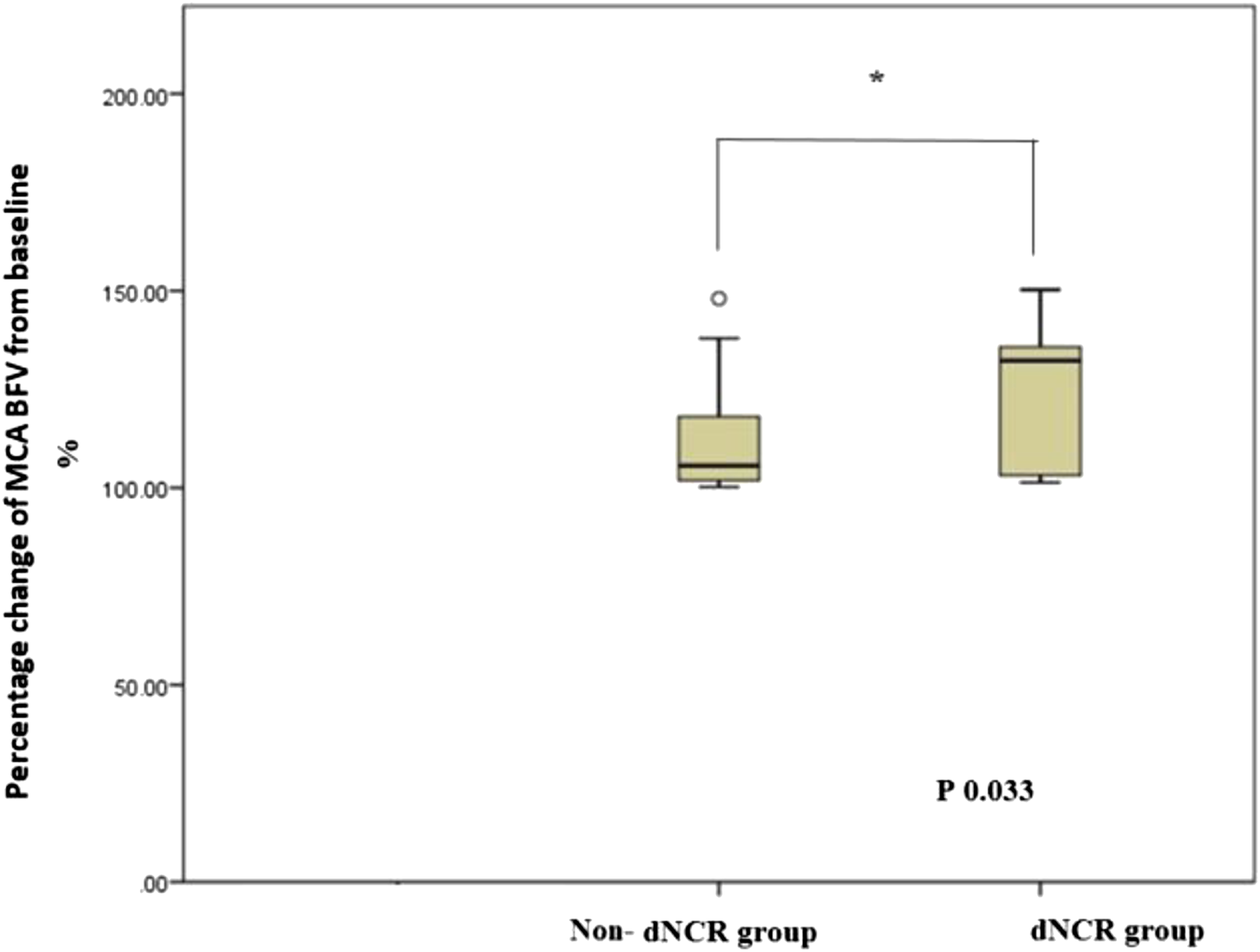
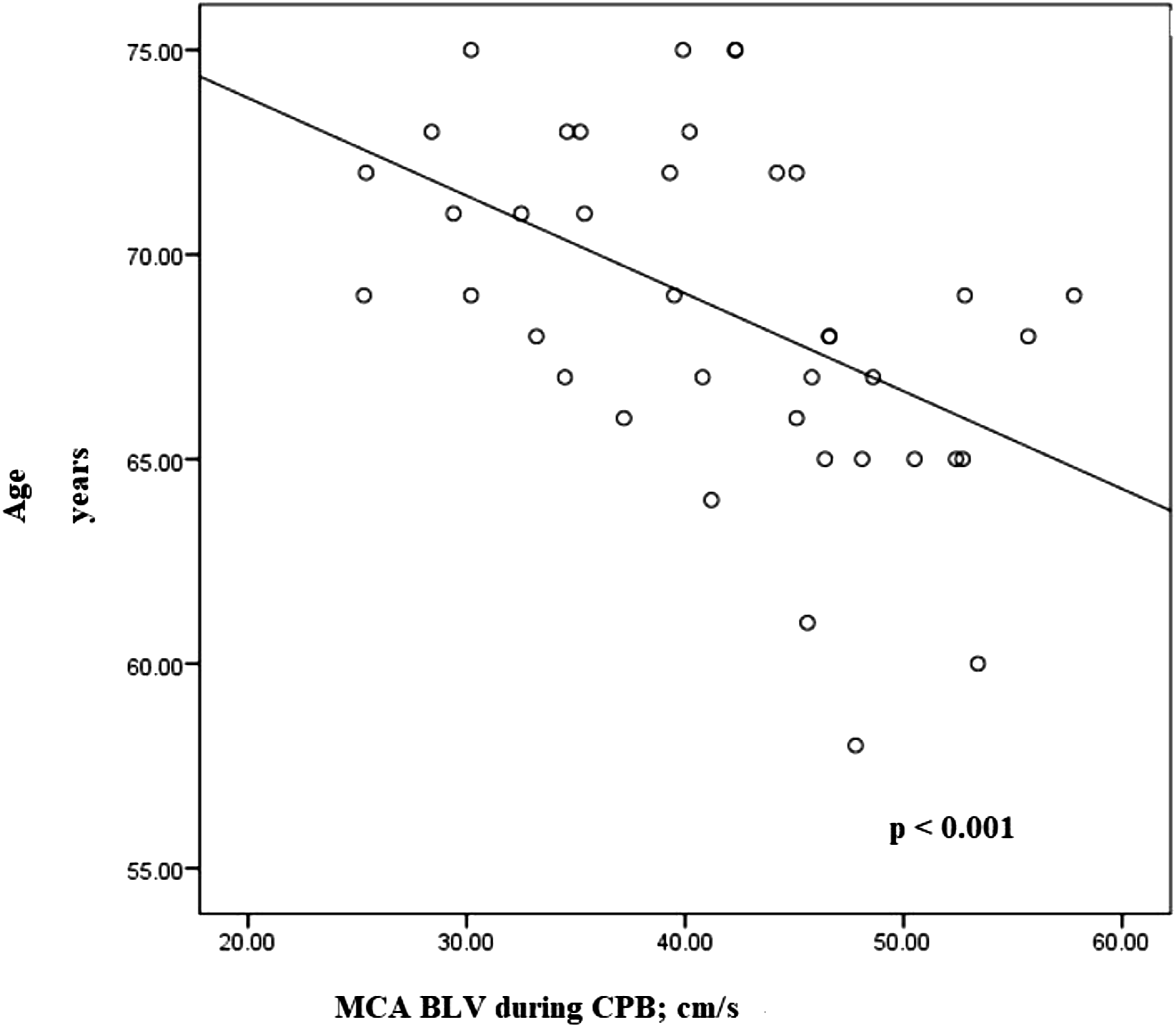
The relationship between patients age, ACE-III test results and MCA BFV were assessed. Spearman correlation analysis revealed that age had negative moderate correlation with ACE-III test results after surgery (Spearman r −0.597, p < .01) and negative moderate correlation with MCA BFV during CPB (Spearman r −0 .529, p < .01) (Figure 3 and Figure 4). Relation analysis of age and the patient postoperative ACE-III score in both groups. ACE–III, Addenbrooke’s Cognitive Examination III. Relation analysis of age and the MCA BFV during CPB in both groups. MCA, Middle Cerebral Artery; BFV, Blood Flow Velocity; CPB, Cardiopulmonary Bypass.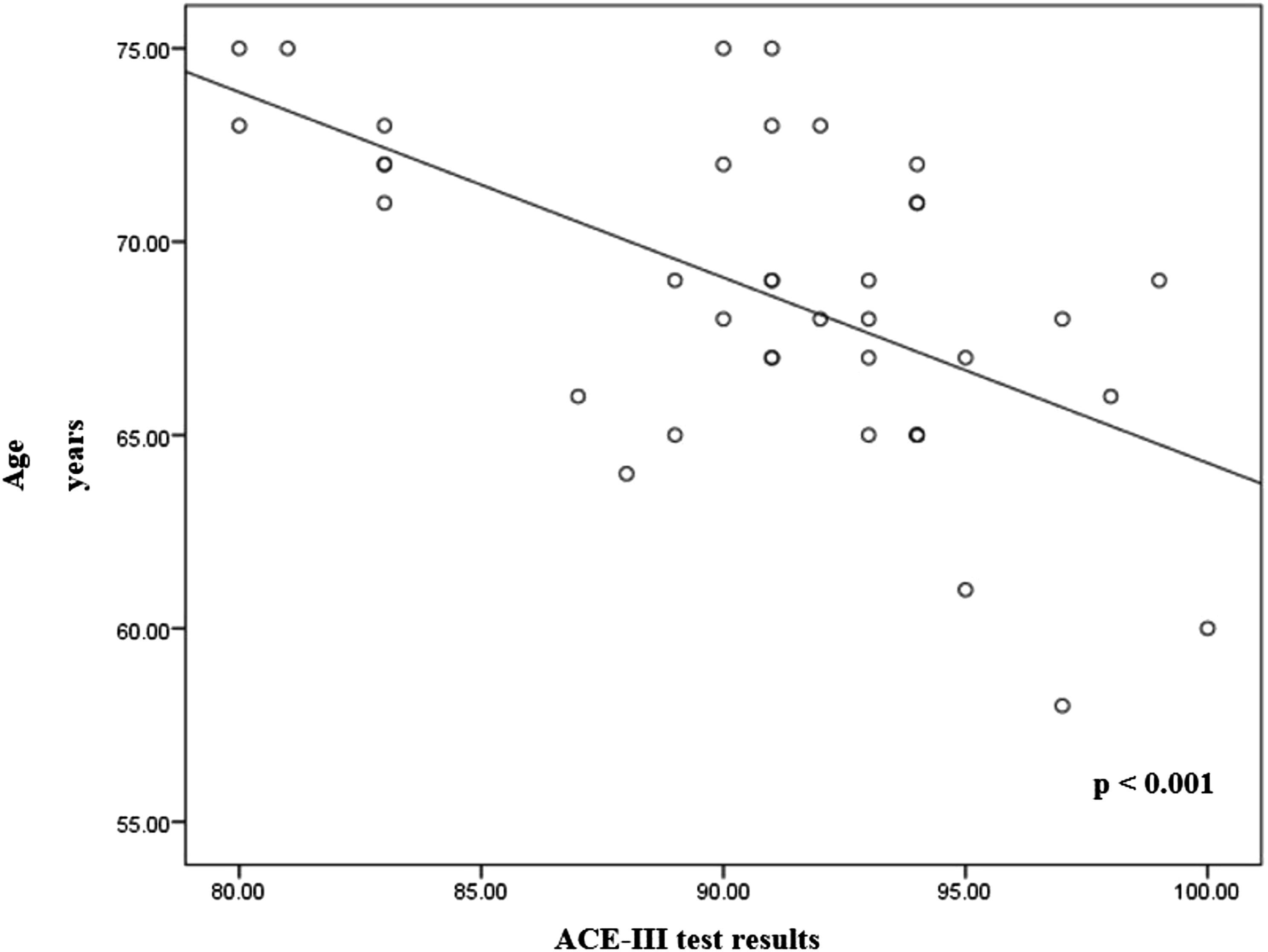
GFAP concentration in blood after anaesthesia induction, 24 and 48 hours after surgery.

GFAP, Glial Fibrillary Acidic Protein.
Data was distributed non normally and presented as the median (min; max). Mann-Whitney U test was performed for comparison between groups.
Discussion
It was established, that the most important factors in developing dNCR are older age and middle cerebral artery blood flow velocity changes during bypass surgery, based on this study. MCA BFV and brain damage biomarker GFAP were compared in two groups of relative hyperperfused patients: with and without dNCR.
Analysis of the dNCR development after cardiac surgery usually focuses on hypoperfusion of the cerebral arteries. Since the blood flow becomes non-pulsed during CPB and a fixed blood flow is transmitted through the CPB device, only indirect indicators can predict whether brain perfusion during CPB is sufficient. However, perfusion of the brain due to various pathophysiological mechanisms is not the same for all patients. It was sought to find out the effect of hyperperfusion on the recovery of neurocognitive functions after cardiac surgery. We found that patients with dNCR in the early post-surgical period were significantly older and had a lower baseline of BFV compared to non-dNCR group. Older age might be the most important factor in decreased blood flow velocity. According to the literature, one of the main factors that may affect the MCA blood flow velocity is age.14,15 It has been found to reach ∼24 cm/s in neonates, ∼100 cm/s in 4–6-year-old children, and only ∼40 cm/s in approximately 70 years old patients. 14 This is because atherosclerosis increases the systemic stiffness of blood vessels in elderly patients. Other age-related factors include co-morbidities leading to increased sensitivity of the central nervous system to medications used during surgery, decreased reserve of cognitive functions, and undiagnosed “silent” brain disease before surgery.16,17 Our results are also confirmed by other researchers: in a study by Thudium M., post-surgical delirium was found in 27% of patients after cardiac surgery, of whom as many as 67% were diagnosed with cerebral hyperperfusion during CPB. 6 Percentage change from baseline MCA BFV was 90 (±21) % in the no-postoperative delirium group vs. 112 (±32) % in the postoperative delirium group (p = .01). These results are very similar to ours, which confirms that relative hyperperfusion has a significant role on the occurrence of the neurological damage. Thudium also stated that duration of cerebral hyperperfusion was highly significantly related to the development of postoperative data. It was not monitored duration of relative hyperperfusion in this study and this is one of this study limitation.
Schmidt also found an increase in the speed of the middle cerebral artery during CPB. 18 Eldery patients have comorbidities, structural changes in cardiovarcular, pulmonary and other systems, are more sensitive to drugs. 17
Cardiopulmonary bypass may affect degree of hyperperfusion. As it is known CPB pump flow is calculated according to height and weight. Cerebral autoregulation maintains constant cerebral blood flow than mean arterial pressure is sufficient. But unfortunately, it is not suitable for all patients. As it was found in this study, some patients already had decreased ACM BFV before surgery. Relative hyperperfusion was determined for these patients during CPB and it was associated with negative neurological outcomes, then CPB pump flow was calculated according to the formula. So, the effect of relative hyperperfusion increases in patients with reduced preoperative BFV.
There are many risk factors to dNCR development, but it was not found any correlations with comorbidities, medications during surgery, CO2, haematocrit, lactate concentration, glucose level, pump flow, ejection fraction, extubation time during surgery. These results could be obtained due to a small sample. Further investigation should be conducted with bigger sample size.
Glial fibrillary acidic protein is widely used as a biological marker in various clinical studies. It was found increased concentrations of GFAP 48 hours after the surgery in the dNCR group patients in this study. An association between an increase in GFAP concentration and delayed neurocognitive dysfunction following cardiac surgery has also been identified in various clinical studies not only in adults but also in neonatal populations.19,20 Other investigation had found a correlation between an increase in GFAP and age. 21 GFAP is known to increase due to microglial activation, a neuroinflammatory response, and increased oxidative stress that results in more intense GFAP transcription. 21 During cardiac surgery, all the listed mechanisms of neuronal damage occur under the influence of various risk factors, such as CPB. Elderly patients are especially susceptible to such neuronal damage, and it was in them that our study found dNCR and an increase in GFAP after cardiac surgery.
Despite the results obtained, we understand that age is an uncorrected pre-surgical risk factor, it is appropriate to identify groups of patients with a higher risk of dNCR. As it has been established that the structure of grey and white brain matter is restored in the elderly during the training of cognitive functions, we suggest using cognitive training exercises with these patients prior to the surgery. 22 We also recommend monitoring MCA BFV during surgery and individualise CPB strategies.
Great attention should also be paid to factors that we can adjust during the surgery. Statistically significant difference was not found between paCO2, haematocrit, or groups of other factors in this study.
There were several limitations in the study. We conducted the study in only one hospital and examined a relatively small group of patients. The TCD sensor was fixed to the patient manually, therefore monitoring was performed only at selected stages of the surgery. By fixing the sensor with the help of a helmet, it would be possible to monitor changes in cerebral blood flow throughout the surgery. In addition, monitoring was applied only during the surgery and did not continue in the intensive care unit, although possible post-surgical disorders that were not recorded may have contributed to a post-surgical increase in the concentration of biomarkers in the brain injury and dNCR. Another limitation is small sample, which was determined by the number of patients treated in our hospital. Nevertheless, we think that this topic in important and worthy interest. To highlight the role of hyperperfusion, a larger study should be performed. This leads to better patient’s neurocognitive recovery after cardiac surgery.
Conclusions
Relative hyperperfusion during CPB may cause dNCR. Elderly patients are sensitive to blood flow velocity acceleration during CPB. GFAP concentration increased 48 h after surgery in dNCR group but did not have any connection with risk factors. The use of GFAP to diagnose dNCR is promising, but large sample research should be performed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.