
Abstract
Introducion
Renal cell carcinoma (RCC) is one of the most prevalent malignant tumors. It extends up into the systemic veins and right atrium. Surgical extraction of such extensions is usually carried out using cardiopulmonary bypass (CPB) with moderate hypothermic (MH) being frequently applied in order to obtain a clear surgical field. However, due to obvious disadvantages of hypothermia, approaches with mild/normothermia (NT) during CPB have also been established. The current study aims to compare the outcomes of patients undergoing RCC tumor and extensions resection using MH versus NT.
Material and Methods
This is a retrospective, non-randomized study. All patients who underwent RCC tumor and extensions resection for stage III or IV (Staehler) RCC in a single center between 2006 and 2020 were included. During surgery, MH or NT were applied. CPB was realized using aortic and bicaval cannulation. We compared the procedural times, transfusion requirements and postoperative outcomes, respectively between the MH and NT groups.
Results
A total of 24 consecutive patients (n(NT) = 12, n(MH) = 12) were included in the study (median age NT 68.5 and MH 66.5). The study only showed a significant difference in heart-lung machine times (median CPB time NT 45.5 min and MH 110.0 min, p = 0.004). All other results, loss of drainage, administration of blood products, as well as the postoperative course and mortality were comparable in both groups.
Conclusion
The results showed a high perioperative and long-term mortality. The perioperative course was similar after surgery with NT or MH. Therefore, NT which minimizes potential complications of MH should be preferred.
Introduction
Renal cell carcinoma (RCC) is the sixth-most prevalent malignant tumor disease in men and the eleventh-most prevalent one in women. 1 From the 1950s, radical nephrectomy was recommended by Robson et al. Licht and Novick (1993) reported similar results with partial nephrectomy. Partial nephrectomy is the current standard for tumor diameters up to 7 cm recommended by the guidelines by the European association of urology.2,3
RCC is most commonly detected by chance during routine abdominal ultrasound investigations. Currently, it is most commonly classified using the UICC (Union Internationale contre le Cancer) scale and the Staehler classification (Figure 1).3,4 Stage classification – Vena cava thrombus according to Staehler. Own representation.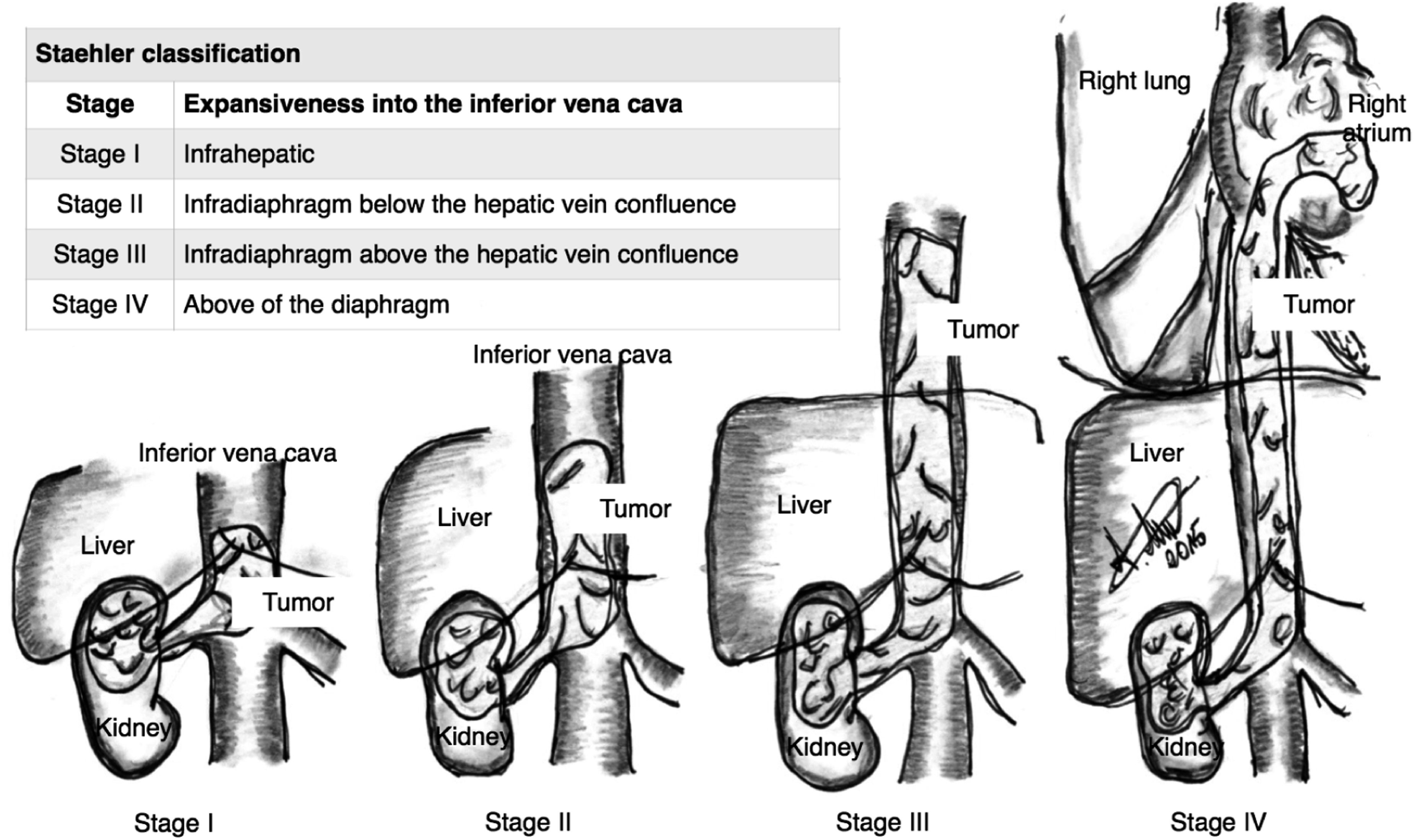
Four to 10 percent of patients initially present with the tumor extending via the renal vein to the inferior vena cava and right atrium. This local extension requires partial or complete excision with or without the use of cardiopulmonary bypass (CPB).2,4,5 A freely floating tumor thrombus level III-IV according to Staehler is mobilized under transesophageal echocardiography (TEE) control by means of a Fogarty catheter through an incision of the gonadal vein from the atrial level to the infradiaphragmal level down to below the hepatic veins and extracted using a Pringle maneuver (Figure 2).
5
If the tumor mass has infiltrated the endothelium of the inferior venae cava (VCI) or right atrium (RA), it can usually only be excised using cardiopulmonary bypass (CPB).
6
Extraction of a Renal cell carcinoma extension from the inferior vena cava using a Fogarty catheter. Own representation.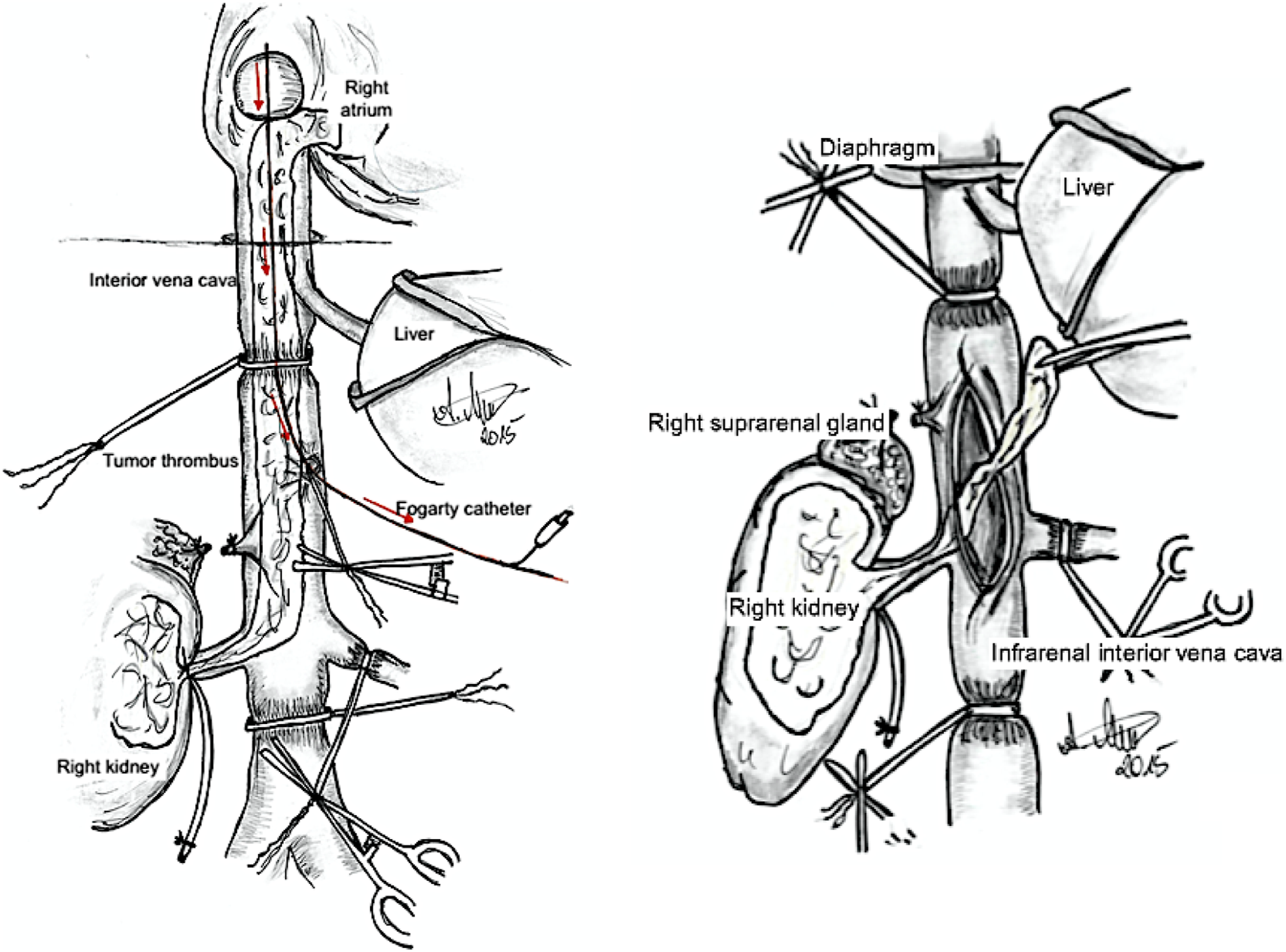
The use of CPB for this purpose is currently discussed controversially: Increased bleeding, platelet dysfunction and mortality have been attributed to CPB with or without the application of hypothermia.
6
However, there are also data showing no association between CPB and adverse events.7–9 The treatment of choice of a RCC is surgical removal and systemic therapy (both neoadjuvant und adjuvant). The best treatment management for the patient is achieved thanks to a therapy algorithm (Figure 3) elaborated by Union International Cancer of Control (UICC).10,11 Therapy algorithm for the treatment of a renal cell carcinoma Union International Cancer of Control.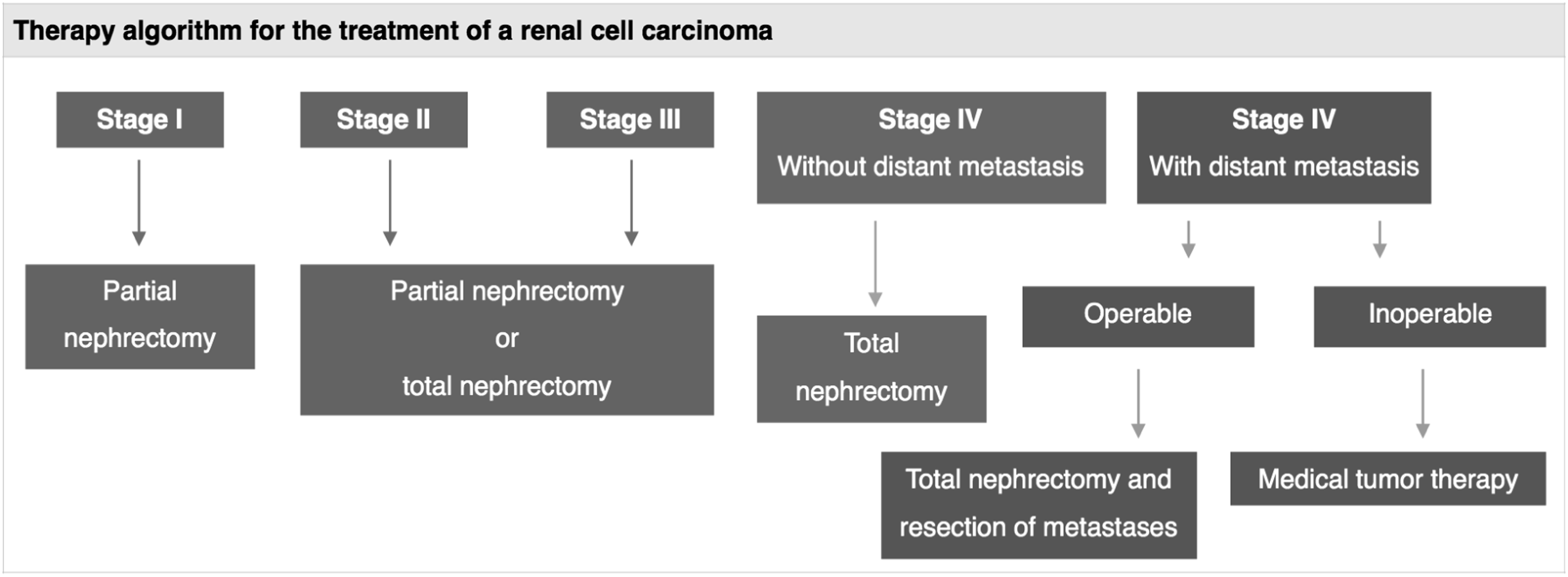
This complex procedure is only possible in an optimized setting and after careful interdisciplinary preoperative planning including urologists, cardiac surgeons, anesthesiologists and perfusionists, respectively. At our clinic, the surgical strategy in the period 2006 to 2020 included moderate hypothermia with circulatory arrest as well as mild/normothermia on the beating heart.
The role of temperature management (moderate hypothermia versus mild/normothermia) during CPB for extraction of RCC for postoperative outcomes and adverse events remains uncharacterized.
This retrospective single-center study aimed at comparing the two strategies with regard to intraoperative parameters (CPB time, blood loss and transfusion requirements) and postoperative outcomes (duration of invasive ventilation, intensive care, lactate production, glomerular filtration rate (GFR), and mortality, respectively.
Material and Methods
This retrospective study was conducted after approval from our institutional review board (approval number S-395/2020, approved in 06/10/2020). For retrospective data analysis, the patients did not require patient information or education about the study. Patients who underwent surgical extraction of stage III to IV RCC with the use of CPB between 2006 and 2020 were included. In case of vena cava (VC) thrombus level IV, a resection is mandatory as for the risk for life-threatening embolism. It is also known, that a cytoreductive nephrectomy can prolong patients life. However, the performance status of the patient and the extent of metastasis have to be taken into account. In patients with limited metastasis and/or good performance status, a surgical removal of the thrombus can prolong patients survival. When performance status is poor or extent of metastasis extensive, we did systemic therapy.
The surgical approach is via a Chevron-Incision. After careful mobilization of the intestines, the affected kidney and its vessels are dissected free. Then, the inferior vena cava (IVC) is dissected free cranially. All tributaries to the IVC are secured and occluded with tourniquets. Then, the kidney, the adrenal gland, the adherent lymph nodes and the renal capsula are resected en bloc. The free-floating tumor extension can be extracted from the IVC using a Fogarty catheter (Figure 2). If this maneuver is assumed to take more than 20 minutes, CPB should be applied in order to prevent abdominal venous congestion.12–14
For excessive tumor extensions reaching the right atrium, an additional median sternotomy is performed. The venous cannulation for cardiopulmonary bypass is conducted using one of the two strategies: 1. Cannulation of the superior vena cava and the infrarenal inferior vena cava. This cannulation allows for occlusion of the venae cava while still maintaining venous drainage. 2. Cannulation of the superior vena cava via the right atrial appendage. This includes venous congestion of the inferior vena cava during tumor excision.
Extraction of the tumor thrombus while the heart is beating is possible in both methods of cannulation.
For the establishment of the CBP would a S5 HLM with a single-system Fusion (S5, Liva Nova, Munich, Germany, Medtronic, Meerbusch, Germany) with a priming volume of 900 ml and a hollow fiber oxygenator was used. Sevofluran anesthesia was maintained during CPB by applying Sevofluran to the CPB circuit. In both strategies, the right atrium is opened longitudinally, and the tumor is resected or pushed digitally into the inferior vena cava in order to resect it from there.
The patients’ data were obtained from institutional records. According to the operative strategy, the patients were either assigned to the mild/normothermia-group (NT-group) or the moderate hypothermia-group (MH-group).
The intraoperative endpoints included duration of perfusion, duration of circulatory arrest, amount of blood loss, amount of transfusion of packed red cells, platelets and fresh frozen plasma, respectively. Postoperative endpoints included duration of invasive ventilation, duration of intensive care unit (ICU) stay, chest tube drainage volume, glomerular filtration rate (GFR) (0 h, 8 h, 16 h und 24 h postoperatively, respectively), serum lactate levels (0 h, 8 h, 16 h und 24 h postoperatively, respectively), and amount of transfusion of packed red cells, platelets and fresh frozen plasma, respectively. Furthermore, 30-days- and 60-days-all-cause-mortality rates were analyzed.
Statistics
The statistical analysis was conducted using SPSS version 27 (IBM, Armonk, USA). Group comparisons were made between the NT-group and the MH-group. The data were tested for normal distribution, Student’s t-test was applied for group comparisons while the Mann-Whitney-U-test was used for comparison of non-normally distributed parameters. Survival functions using Kaplan-Meier-estimations were calculated for both groups and compared using the log-rank test. Statistical significance was assumed for p-values <0.05. Parameters are expressed as medians and interquartile range (IQR), as appropriate.
Results
Twenty-four patients were included in the study. Thereof, 12 patients were attributable to the NT-group and 12 patients were assigned to the MH-group, respectively.
The patient’s characteristic.
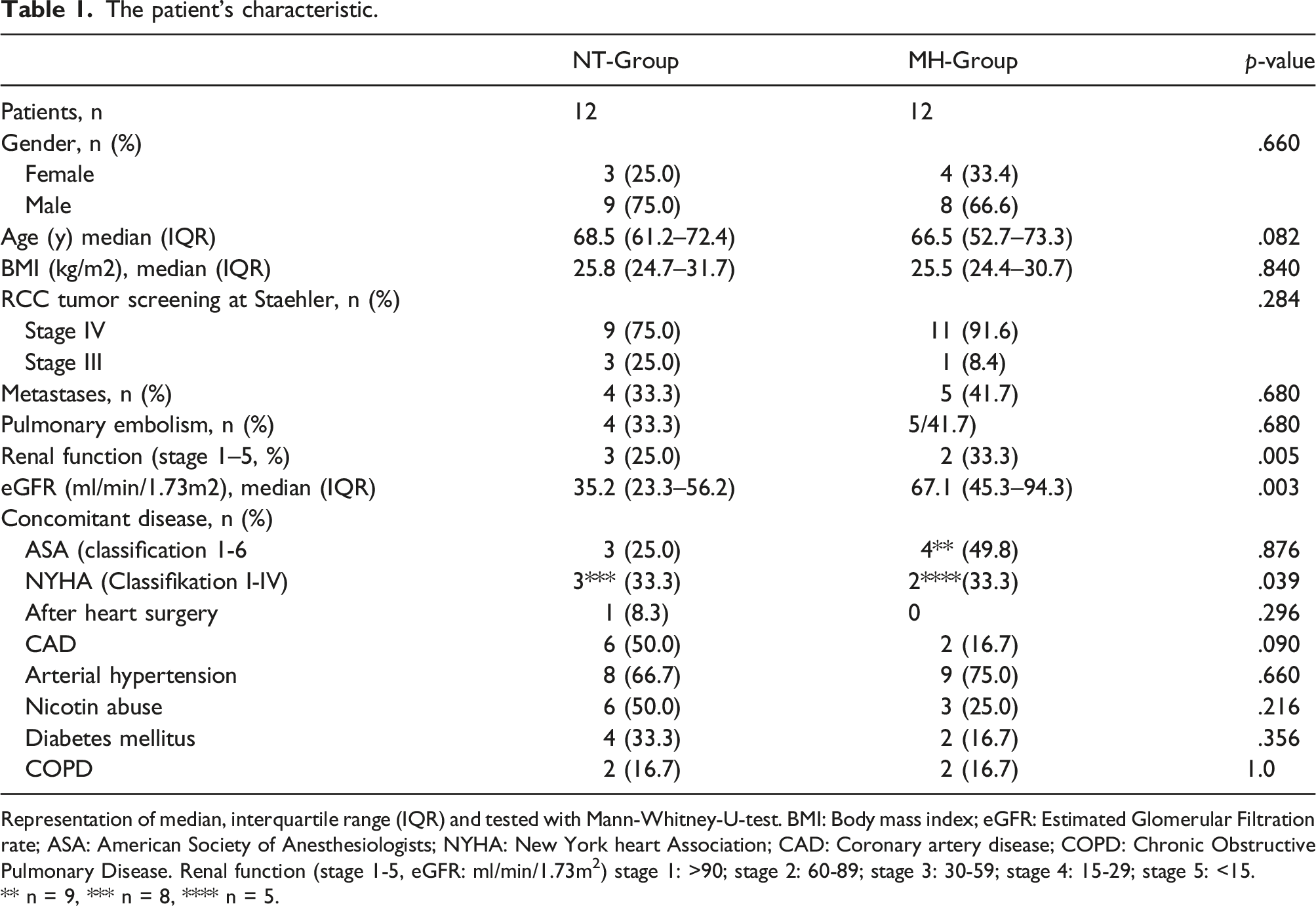
Representation of median, interquartile range (IQR) and tested with Mann-Whitney-U-test. BMI: Body mass index; eGFR: Estimated Glomerular Filtration rate; ASA: American Society of Anesthesiologists; NYHA: New York heart Association; CAD: Coronary artery disease; COPD: Chronic Obstructive Pulmonary Disease. Renal function (stage 1-5, eGFR: ml/min/1.73m 2 ) stage 1: >90; stage 2: 60-89; stage 3: 30-59; stage 4: 15-29; stage 5: <15.
** n = 9, *** n = 8, **** n = 5.
Perioperative features.
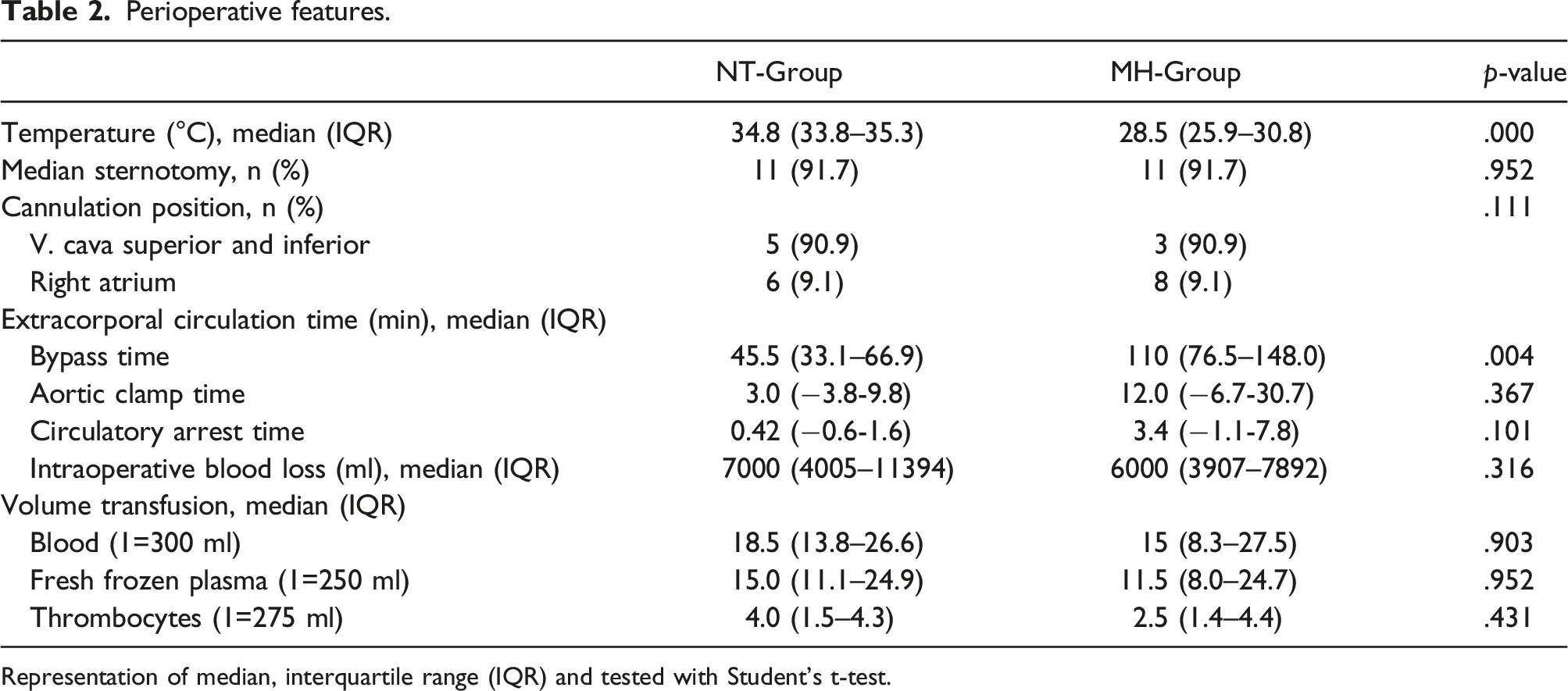
Representation of median, interquartile range (IQR) and tested with Student’s t-test.
Postoperative features.
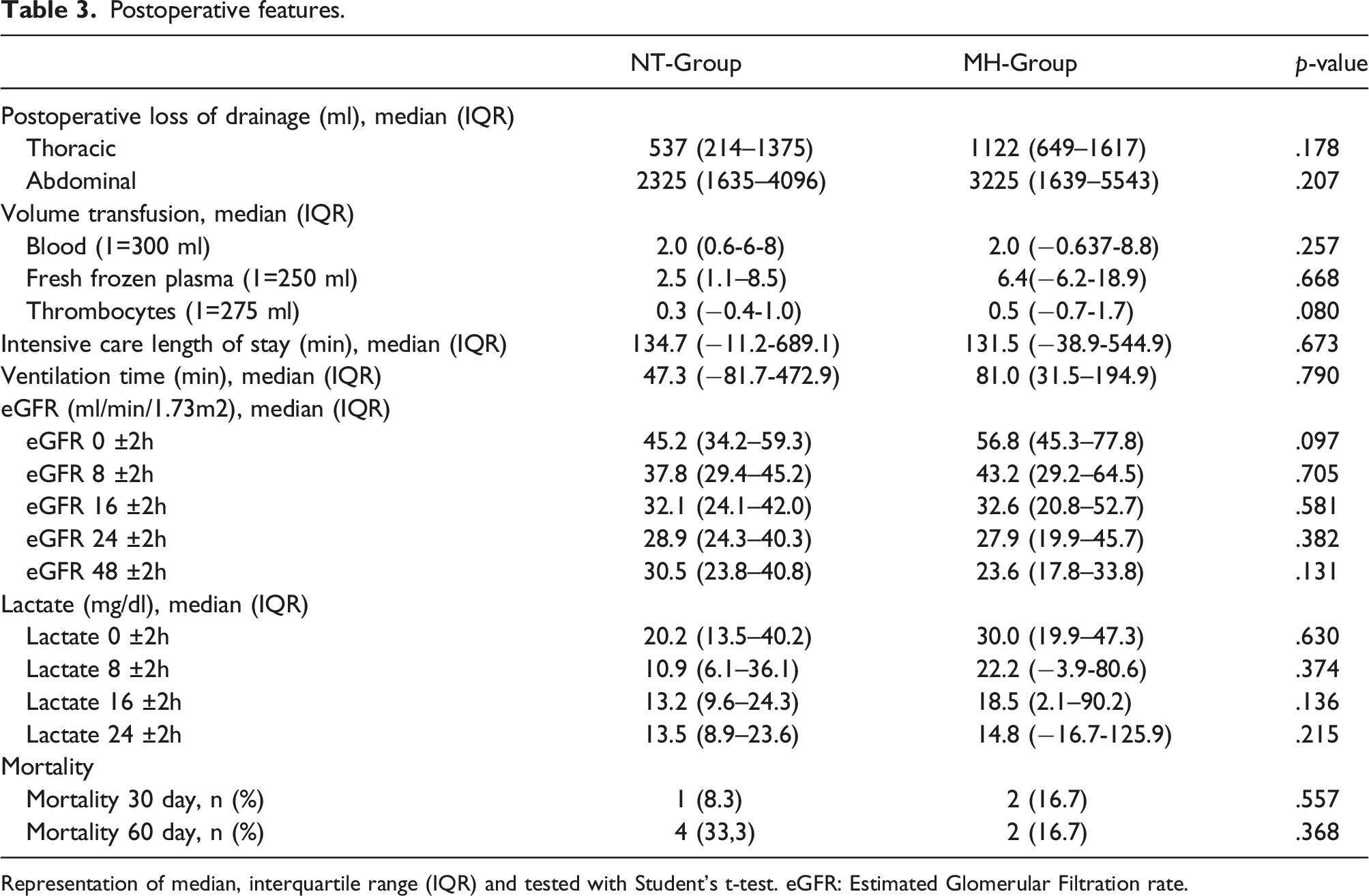
Representation of median, interquartile range (IQR) and tested with Student’s t-test. eGFR: Estimated Glomerular Filtration rate.
The long-term follow up over a median time of NT-Group 3.56 years and MH-Group 5.18 years showed overall survival after one year rates of 58% in both groups, after two years NT-group 42%, MH-group 50% and after five years NT-group 25% and MH-group 42%, respectively with no difference between the groups (Figure 4, log-rank test p = 0.162). Survival functions using Kaplan-Meier estimation of patient’s with renal cell carcinoma with tumor thrombus into inferior venae cava and right atrium until the last follow-up. CI: Confidence interval 95%.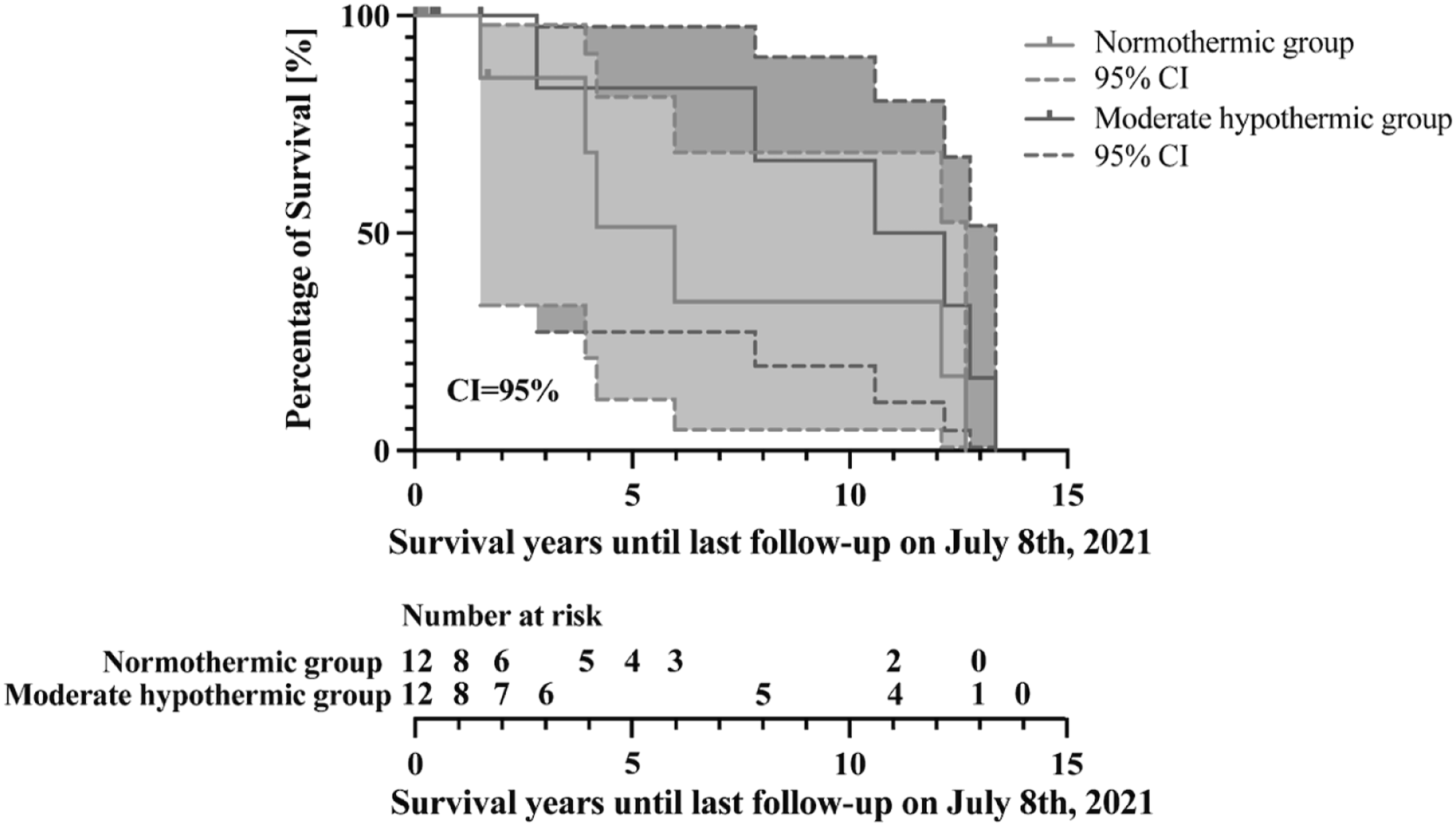
Discussion
This study compared the outcomes of patients with extensive RCC who underwent tumor excision with the use of CPB. We compared two strategies for CPB management. The intra- and postoperative outcomes were comparable for both the NT-group and the MH-group.
As expected, the duration of CPB was longer in the MH-group due to the time needed for cooling and rewarming of the patient.15,16 This is in accordance with previous studies showing an average warming of 0.2°C per minute after cardiac surgical procedures. 17 This also applies to other surgical procedures using moderate hypothermia, such as aortic arch surgery for aortic dissections. With regard to the aortic clamping and the cardiac arrest, the surgical extraction of the tumor material was significantly more complex, which shows the increased clamping time in the MH-group. 18
Blood loss and transfusion requirements were not significantly different between the groups. However, a tendency towards less bleeding and transfusion was seen in the NT-group. This result could be explained by a less pronounced impairment of the coagulatory function in patients who did not undergo excessive cooling and rewarming. 19
The initial postoperative course was comparable in both groups. However, the length of ventilation, chest tube drainage volumes, courses of the GFR in relation to the preoperative values showed a tendency for worse outcomes in the MH-group. Detrimental effects of hypothermia including dysfunction of the plasmatic coagulation and platelets with increased bleeding have been extensively documented.19–22 Furthermore, cooling has been associated to disturbances in the autoregulation of the peripheral vasculature resulting in perfusion deficits and anaerobic metabolism.23,24 The renal function is also well known to be affected by CPB, particularly when hypothermia is applied.22,25 The postoperative durations of mechanical ventilation and intensive care unit stay were comparable in both groups. These parameters are generally strongly dependent on the clinical environment and the course of anesthesiologic management. 26
Surgical therapy of extended RCC is a surgical challenge and associated with an extensive trauma for the patient. Therefore, surgery in this stadium of RCC is sometimes even advised against in order not to shorten the remaining survival time.27,28 The mortality in this study was similar in both groups. The main cause of early mortality was cardiopulmonary failure. In the late course, the causes of mortality were mainly tumor-associated. This is in accordance with previous studies demonstrating similar mortality rates in the mild-term follow-up.29–31
In summary, this is a retrospective study with a very small sample size which precludes any confirmatory conclusions to be derived from our results. However, the data show that with both strategies, hypothermia and normothermic CPB during extraction of stage III-IV RCC, a safe perioperative course can be realized. However, the subsequent high mortality in the long-term warrants further investigation in order to improve the outcome of these severely morbid patients.
From a physiological point of view, the normothermic approach seems to be at least non-inferior to the hypothermic approach. Because normothermia avoids potential risks of deep hypothermia and is associated with shorter CBP duration, we consider it to be the preferred strategy for temperature management of CBP for RCC extraction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.