
Abstract
Introduction:
Aortic arch reconstruction surgery represents a challenge for the medical personnel involved in treatment. Along the years, the perfusion strategies for aortic arch reconstruction have evolved from deep hypothermic cardiac arrest to antegrade cerebral perfusion with moderate hypothermia, and recently to a combined cerebral and lower body perfusion with moderate hypothermia. To achieve a lower body perfusion, several cannulation strategies have been described. In this study, we investigated the feasibility of utilizing an arterial sheath introduced in the femoral artery to achieve an effective lower body perfusion.
Methods:
We included patients who underwent an aortic arch reconstruction surgery with a lower body perfusion, from January 2017 to June 2019. To achieve a lower body perfusion, a three-way stopcock was connected to the arterial line, where one end was connected to the central cannulation for cerebral perfusion and the other to an arterial sheath that was introduced through the femoral artery. A total of 25 patients were included. Peri- and postoperative lactate and creatinine levels and signs of malperfusion were recorded.
Results:
During the reperfusion phase, after selective perfusion ended none of the patients showed a significant increase in lactate, creatinine, and liver enzyme levels. After 24 hours, there were no signs of an acute kidney injury, femoral vessel injury, or limb malperfusion.
Conclusion:
These findings show that a sufficient lower body perfusion through an arterial sheath placed in the femoral artery for aortic arch reconstruction can be achieved. This approach caused no complications related to the arterial sheath during the early postoperative period and is an easy way to maintain perfusion of systemic organs.
Introduction
Neonatal aortic arch surgery represents a challenge not only for the surgeon but also for the perfusionist, cardiac anesthesiologist, and intensivists because of the complexity of the surgery, long cardiopulmonary bypass (CPB) time, deep hypothermic cardiocirculatory arrest (DHCA) and/or selective antegrade cerebral perfusion (ACP) which may lead to intra- and postoperative complications.1–3 With the use of ACP, an improved brain protection can be achieved, accompanied by a strategy using moderate hypothermia for organ protection to decrease lactate levels, length of stay in the intensive care unit (ICU), and acute postoperative kidney injury.1,2,4 It has been previously published that with this strategy, the lactate levels are lower when compared with DHCA alone, what might be due to collaterals that ensure a certain perfusion of the lower body. 4 Recently, centers around the world have described different techniques to cannulate the descending aorta during aortic arch surgery to ensure renal and splanchnic perfusion.5–7 These techniques have shown to reduce end organ damage in the lower body, leading to even shorter ICU stay, lower lactate levels, and a lower risk for kidney injury.2,7–9 The aforementioned techniques range from an infradiaphragmatic cannulation to a left thoracotomy or even a direct cannulation during arch reconstruction through the anastomosis.6–8 These techniques, while effective, require manipulation and extensive preparation in order to reach the aorta at the desired cannulating segment and may lead to vessel or organ injury and increases surgery time.
At our center, we have been implementing a different technique to ensure lower body perfusion (LBP) with ultrasound guided cannulation of the femoral artery using intra-arterial vascular sheaths. When the aorta is cross-clamped, and hypothermia implemented, ACP and LBP are begun and maintained through the duration of the aortic anastomosis. The purpose of this study was to determine the feasibility of cannulating the femoral artery to introduce vascular sheaths and to determine if it is a safe technique of achieving LBP and determine if a sufficient perfusion was obtained during this time.
Methods
Patient selection process
We retrospectively included all pediatric patients from January 2017 to June 2019 who underwent aortic arch surgery at the Tübingen University Hospital. Patients underwent surgeries such as the Norwood procedure, Damus–Kaye–Stansel Anastomosis or an aortic arch reconstruction due to hypoplasia of the latter either as first or redo surgery. All surgeries were performed by the same surgeon. Patients in which a LBP was not instated and patients who were transferred to the ICU with extracorporeal support (extracorporeal membrane oxygenation (ECMO)) were excluded.
Vascular sheath implantation and perfusion strategy
The arterial sheaths were percutaneously cannulated by two experienced congenital cardiac anesthesiologists during the induction of anesthesia. Direct visualization of the femoral vessels by ultrasound was used during the implant process. The size of the arterial sheaths was determined according to the weight of the patients.
During the surgery, a polytetrafluoroethylene (PTFE) shunt was anastomosed to the truncus brachiocephalicus through which the aortic cannula would be inserted for the ACP; then the aorta was cross-clamped and moderate hypothermia (28-30°C) was achieved for reconstruction, a combined ACP and LBP were instituted through an arterial line connected to a high-flow three-way stopcock (Figure 1). The flow rate was 50-80 mL/min, depending on the blood pressure and oxygen saturation, for the duration of the aortic reconstruction. After the completion of the reconstruction, the neo-aorta was cannulated, and a full body perfusion was instated. During the surgery, the bilateral cerebral and visceral perfusion was monitored using near-infrared spectroscopy (NIRS) (Medtronic/Covidien INVOS™, Minneapolis, MN, USA and Masimo O3® Regional oximetry, Irvine, CA, USA). Arterial blood gases (blood gas analysis (BGA)) were regularly drawn. During the reperfusion period, lactate levels were closely monitored to determine if the LBP was effective. Lactate as well as creatinine levels were monitored during the ICU stay as markers of splanchnic and renal ischemia.
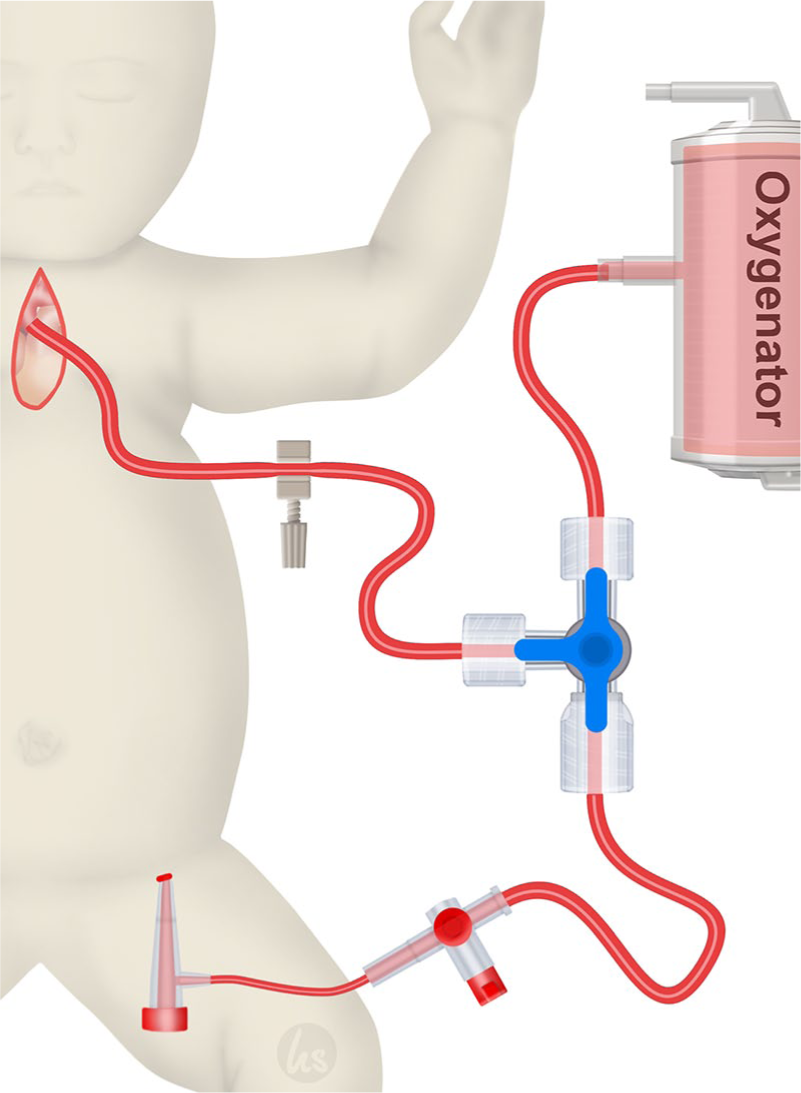
Extracorporeal circulation through a combined strategy with antegrade cerebral perfusion (ACP) and lower-body perfusion (LBP). LBP is being administered through an arterial sheath in the femoral artery.
After the surgery ended, lower extremities were examined and compared for signs of possible ischemia caused by the arterial sheath. After sheath removal at the ICU, the patients were examined at least three times daily for clinical signs of malperfusion (changes in skin color, extremity temperature, and recapillarization time).
Statistical analysis
All statistical analyses were performed using the SSPS 23.0 (IBM Corporation, Armonk, NY, USA) software. Normal distribution was checked using the Kolmogorov–Smirnov test. Continuous variables are reported as means and standard deviation if distributed normally. Not normally distributed variables are reported as median and interquartile ranges. Normally distributed variables were compared using the student t-test and not normally distributed variables were compared using the Mann–Whitney U-test. Ordinal variables are reported as absolute values and percentages where applicable.
Ethics approval
Approval for this retrospective study was obtained from the local institutional review board and ethics committee of the University of Tübingen (461/2019BO2).
Results
Patient cohort
There was a total of 25 children who met the inclusion criteria. Six children had to be excluded due to ECMO support (n = 4) and non-implementation of a LBP (n = 2); this left a total of 19 patients who met the inclusion criteria.
Of the 19 patients who met the inclusion criteria, 17 patients underwent an aortic surgery for the first time and 2 patients had a re-do surgery due to stenosis of the aortic arch after reconstruction at an earlier age. These two patients can be regarded as outliers, given the fact that they underwent a surgery at newborn age and received the re-do surgery over a year later. The rest of the patients had a comparable age, weight, and gender at the time of surgery (Table 1).
Patient characteristics, surgeries, and intraoperative strategies.
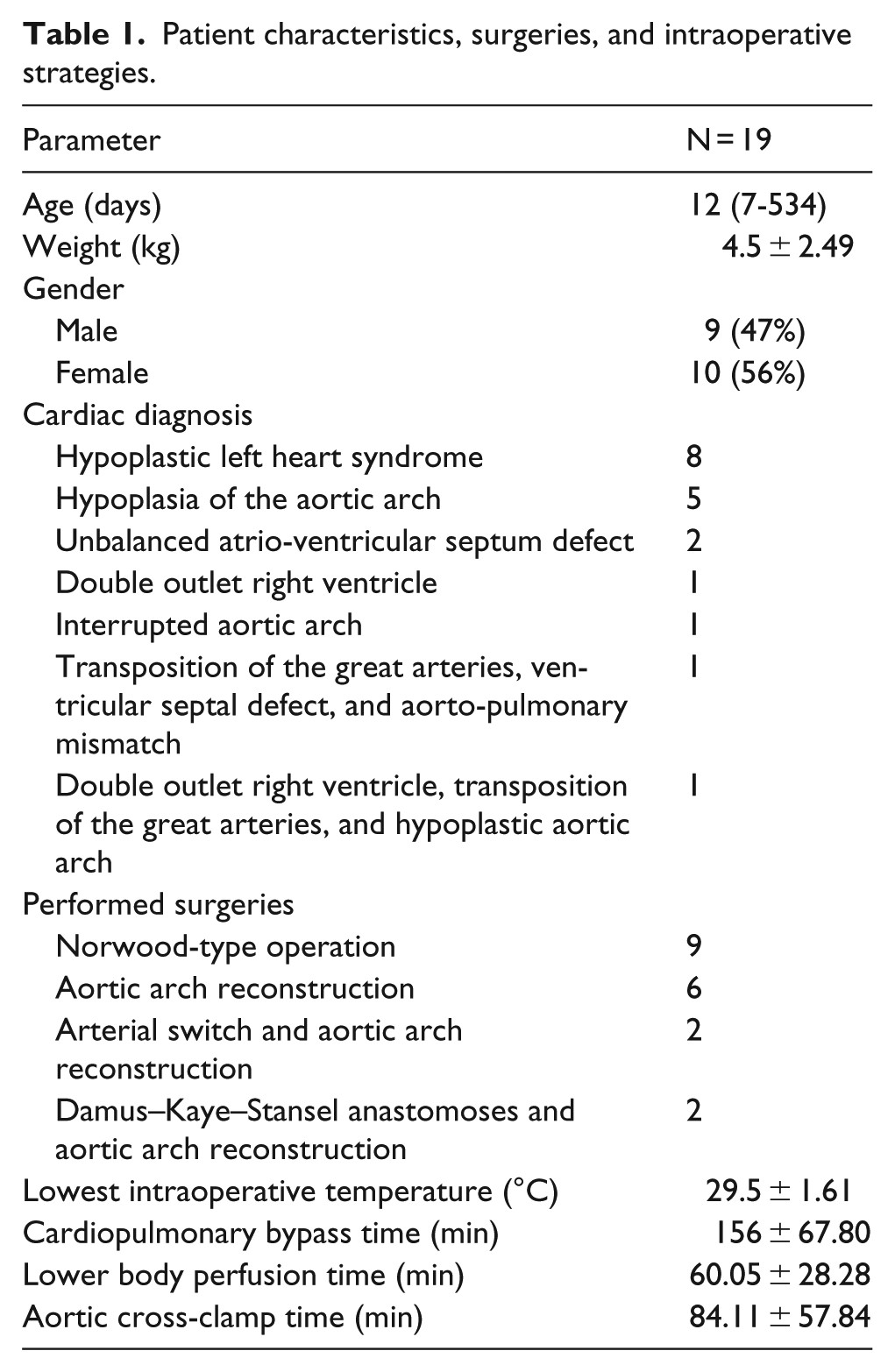
The CPB time, temperature, and lactate levels during reperfusion were comparable between the patients, in patients undergoing a re-do surgery the operative times were longer, due to the adhesions found in the situs, values are seen in Table 1.
All the patients underwent a reconstruction of the aortic arch, either as a main procedure or as part of a complex procedure. There were four different surgeries performed in these patients, including a Norwood type surgery, aortic arch reconstruction, Damus-Kaye-Stansel anastomoses and aortic arch reconstruction, and transposition of the great arteries and arch reconstruction (Table 1).
For patients weighing between 3 and 5 kg, a 3F Cook Medical Micropuncture set was utilized, this sheath has an outer diameter of 1.3 mm; for patients over 5 kg, a 4F Terumo arterial sheath was implanted. In n = 13 patients, the arterial diameters were documented. The arterial diameters ranged from 1.2 to 3.9 mm, the smallest patient in the presented cohort weighed 2.3 kg and had a femoral artery diameter of 1.4 mm. For this reason, a 20G Vygon Leader Cath cannula was introduced and utilized for the LBP. One of the patients who underwent a re-do surgery was 419 days old and had a larger femoral artery diameter so a 5F Terumo sheath was utilized for the LBP. The distribution of sheaths used in patients is shown in Table 2.
Vascular sheaths used and femoral diameters.
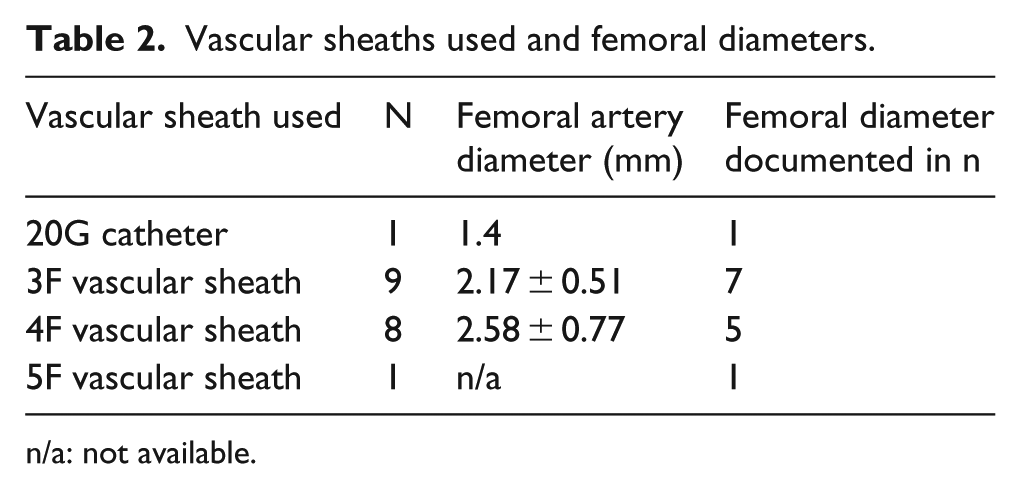
n/a: not available.
Pre- and 24-hour postoperative creatinine, liver enzymes, and intraoperative lactate were recorded and compared, results are shown in Table 3. There was no significant difference between creatinine, aspartate aminotransferase (ASAT), lactate dehydrogenase (LDH), and lactate in the pre- and early postoperative phase. Alanine aminotransferase (ALAT) was significantly lower in the early postoperative period. This supports an adequate perfusion of the abdominal organs and the lower extremities during the surgeries.
Creatinine, liver enzyme and lactate levels in the clinical course.
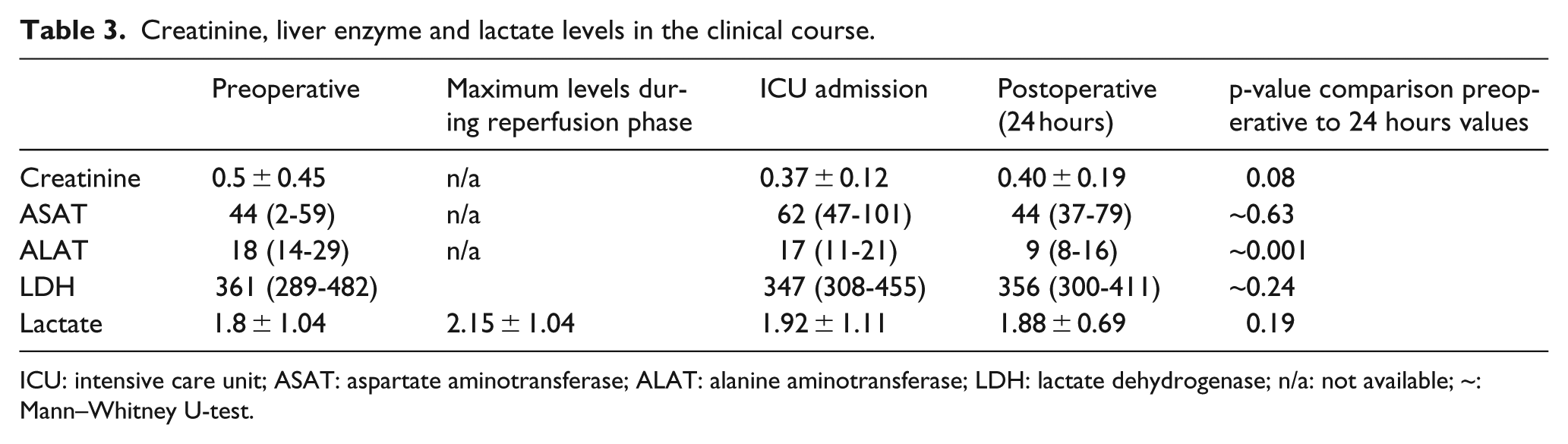
ICU: intensive care unit; ASAT: aspartate aminotransferase; ALAT: alanine aminotransferase; LDH: lactate dehydrogenase; n/a: not available; ~: Mann–Whitney U-test.
Upon completion of the surgery, the arterial sheaths were left in place and the patients were transferred to the ICU. At the ICU, the sheaths were explanted as soon as possible; 11 of the 19 (58%) patients had the femoral sheath for 24 hours or less. During the stay, the lower extremities were examined for signs of malperfusion and/or hematoma caused by the arterial sheath (please see methods section). Out of the 19 patients who underwent surgery with LBP, none of them showed signs of malperfusion or stenosis caused by the arterial sheaths during the entire hospital stay.
Discussion
Selective ACP is the method of choice for improved cerebral perfusion and protection; combined with moderate hypothermia, it has been used as a standard technique for aortic arch reconstructions in neonates. Although the postoperative results have improved compared with DHCA alone, there is still a certain degree of acute kidney injury (high creatinine levels) and elevated lactate levels can be seen in the reperfusion phase intraoperatively and postoperatively at the ICU.7–9 The lactate level reflects the amount of lower body ischemia due to circulatory arrest in this situation. Avoiding lower body and splanchnic ischemia might improve patients’ outcomes as organ dysfunction is avoided. To address this problem, different approaches have been developed in an attempt to improve the splanchnic and renal perfusion through cannulation of the descending aorta, femoral artery, or umbilical artery.5,7–9 These studies have shown an improvement of the renal function, lactate levels and ICU length of stay when compared with mild hypothermia and ACP.5–7,9 However, only one group has published an LBP approach utilizing a different cannulation site than the descending aorta either by the use of the umbilical or femoral artery utilizing a 3.5F (n = 9 patients) and 3F (n = 4 patients) arterial sheath, respectively. 5 The patient cohort which underwent surgery with LBP showed improved renal function, implying an adequate perfusion using both approaches; 5 by avoiding any degree of acute kidney injury the morbidity and mortality at the ICU is reduced.10,11 After confirming that a splanchnic and renal perfusion is of benefit to the patients, we decided to focus on the safest approach to it. Like mentioned earlier, although the operative techniques to cannulate the descending aorta are effective, an aortic cannulation may lead to complications like bleeding or injury of adjacent structures. For this reason, we decided to focus on the approach through the femoral artery using arterial sheaths.
Femoral artery access and pressure monitoring is a standard approach in children undergoing congenital cardiac surgery, and ultrasound-guided cannulation of the small femoral vessels is performed routinely. Therefore, the same access site can be used for LBP. Our data show that the use of vascular sheaths, when tailored to the size of the femoral vessel, is a safe procedure. This approach, therefore, represents an easy approach for LBP allowing the reduction of cannulas and perfusion lines in the surgical situs. The low intraoperative lactate levels during reperfusion after cross-clamping (mean 2.15 ± 1.04 mmol/L) and constant levels of creatinine values and liver enzyme levels compared with preoperative values show that an efficient splanchnic and renal perfusion was achieved. For the reported cohort insertion of arterial sheaths represented no vascular or puncture-related complications whatsoever; in most patients, the removal of the sheath occurred within the first 24 hours after surgery. Some patients had prolonged stay at the ICU because of accompanying diagnoses. These patients had the arterial sheaths for a prolonged time in situ to enable arterial blood pressure monitoring and in case an emergency ECMO implantation was necessary to have a quick arterial access.
Limitations
Our data are limited because we can only report on a small cohort of patients undergoing surgery at a single center. In this cohort, it is also not possible to detect all complications of femoral access with vascular sheaths. Long-term follow-up needs to be performed to identify whether the children develop femoral artery stenosis. As the aim of this study was to determine the feasibility of achieving a sufficient LBP using a femoral arterial sheath, the impact it had on the early and late postoperative period were not investigated.
Conclusion
In our experience, the use of arterial sheaths for LBP during neonatal aortic arch reconstruction surgery is a safe procedure. It enables an improved splanchnic perfusion compared with ACP alone which allows for the surgeries to be performed in a moderate instead of deep hypothermia. LBP has been previously shown to result in shorter reperfusion and mechanical ventilation times; it may also reduce the ICU length of stay. In order to have better data, a study with a bigger cohort should be performed. Due to the rarity of the diseases for which this technique is indicated, it is difficult to find a patient pool large enough; a multi-center approach could provide a greater number of patients in need of aortic arch surgery in whom an LBP may be performed. As intraoperative results with low lactate levels are encouraging, it has yet to be determined whether this translates into improved patient outcomes.
Footnotes
Acknowledgements
We would like to thank personnel from the heart surgery, anesthesia, perfusion and pediatric cardiologists and intensivists who were involved in the treatment of the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.