
Abstract
Introduction:
Historically, perioperative hemoglobin monitoring has relied on calculated saturation, using blood gas devices that measure plasma hematocrit (Hct). Co-oximetry, which measures total hemoglobin (tHb), yields a more comprehensive assessment of hemodilution. The purpose of this study was to examine the association of tHb measurement by co-oximetry and Hct, using conductivity with red blood cell (RBC) transfusion, length of stay (LOS) and inpatient costs in patients having major cardiac surgery.
Methods:
A retrospective study was conducted on patients who underwent coronary artery bypass graft (CABG) and/or valve replacement (VR) procedures from January 2014 to June 2016, using MedAssets discharge data. The patient population was sub-divided by the measurement modality (tHb and Hct), using detailed billing records and Current Procedural Terminology coding. Cost was calculated using hospital-specific cost-to-charge ratios. Multivariable logistic regression was performed to identify significant drivers of RBC transfusion and resource utilization.
Results:
The study population included 18,169 cardiovascular surgery patients. Hct-monitored patients accounted for 66% of the population and were more likely to have dual CABG and VR procedures (10.4% vs 8.9%, p=0.0069). After controlling for patient and hospital characteristics, as well as patient comorbidities, Hct-monitored patients had significantly higher RBC transfusion risk (OR=1.26, CI 1.15-1.38, p<0.0001), longer LOS (IRR=1.08, p<0.0001) and higher costs (IRR=1.15, p<0.0001) than tHb-monitored patients. RBC transfusions were a significant driver of LOS (IRR=1.25, p<0.0001) and cost (IRR=1.22, p<0.0001).
Conclusions:
tHb monitoring during cardiovascular surgery could offer a significant reduction in RBC transfusion, length of stay and hospital cost compared to Hct monitoring.
Keywords
Introduction
Perioperative monitoring of hemoglobin (Hb) and hematocrit (Hct) often relies on point-of-care blood gas and laboratory analyzers, utilizing co-oximetry or conductivity technologies. Using multi-wavelength spectrophotometry, co-oximetry adds valuable information for the clinician by providing measurements of total hemoglobin (tHb) and the breakdown of four hemoglobin moieties, oxyhemoglobin, deoxyhemoglobin, carboxyhemoglobin and methemoglobin. 1 On the other hand, conductivity utilizes electrical conductance for the determination of plasma Hct. While the Hct conductivity method is accurate in many clinical situations, it relies upon an algorithm that assumes normal blood protein levels. Among hospitalized patients, there are many conditions in which blood protein levels are abnormally low or high. One of the most extreme forms of controlled hemodilution occurs during cardiopulmonary bypass (CPB) when blood is hemodiluted, which substantially lowers serum protein levels and renders falsely low Hct measurements which may result in unnecessary red blood cell (RBC) transfusion. 2 On the other hand, the measurement of tHb by co-oximetry is not affected by the dilution of blood proteins and results in more consistent measurements of hemodilution during CPB.1,2
Previous studies have shown a systematic relationship between RBC transfusion and poor outcomes among patients undergoing major cardiovascular procedures.3–6 Incremental risks for post-operative complications, including sepsis and pneumonia, have been linked to the increased intubation time associated with RBC transfusion.7–9 Perioperative RBC transfusion has also been associated with the development of acute kidney injury during cardiac surgery as a result of increased inflammation, which may lead to tissue oxidative stress. 10 The relationship between mortality and RBC transfusion in cardiac surgical patients is less clear.11–13 However, increased rates of complications associated with RBC transfusion have been shown to have a direct effect on treatment cost due to longer hospital stays and resource utilization intensity.3,6,14
To date, no studies have examined the relationship between the methods of hemoglobin monitoring, the risk of RBC transfusion and comparative levels of resource utilization. Therefore, we examined the association of the measurement of tHb by co-oximetry and Hct by conductivity with RBC transfusion, length of stay (LOS) and total inpatient discharge costs.
Methods
A retrospective cohort study using the Vizient Health System database, a nationally recognized and representative administrative database that provides billing details from approximately 400 hospitals across 43 states in the United States,13–15 was conducted using January 2014 to June 2016 discharges.
The study population consisted of patients aged ≥18 years who were hospitalized for either coronary artery bypass graft (CABG) or valve replacement (VR) surgical procedures, as defined by the International Classification of Disease Category (ICD-CM) versions 9 and 10. Patients who underwent both CABG and VR procedures were analyzed and compared as separate cohorts. Finally, all patients were classified into two study cohorts (tHb and Hct) based on the two types of hemoglobin monitoring technologies. These monitoring cohorts were identified using a combination of detailed billing records and Current Procedural Terminology version 4 (CPT-4) codes 85014 (Hct) and 85018 (tHb). Patients who had both monitoring technologies performed were excluded from the analysis because it was unknown which test was the primary driver for the decision to administer a RBC transfusion.
The primary outcome of interest in this retrospective analysis was in-hospital RBC transfusion risk. RBC transfusion was identified using hospital billing records and constructed as a binary variable. Secondary outcomes included the assessment of resource utilization by examining total inpatient discharge cost and hospital LOS. Cost was defined as the total cost of the hospitalization encounter derived by applying hospital-specific cost-to-charge ratios (CCR) developed from the publically available Medicare Cost Reports (MCR) collected by the Centers for Medicare and Medicaid Services (CMS) to the summarized discharge level cost for each patient encounter. This cost represents the total cost to the hospital to provide care to each patient during their hospital stay.
Factors that could affect the risk of RBC transfusion, as well as the baseline health characteristics of the patient population, were also included in this analysis. Patient level demographic variables, including age and gender, were captured, as well as encounter-specific variables, such as source of admission, discharge status and LOS. Age was reported as both a continuous variable and in 10-year increments. Patient comorbidities were identified using the Charlson-Deyo version of the Charlson Comorbidity Index, a method of categorizing comorbidities of patients based on ICD-CM diagnosis codes found in administrative data.15–16 Both the score and individual comorbidities were included in the analysis; the higher the score, the more likely the predicted outcome will result in mortality or higher resource use.
Additional cardiovascular-specific comorbidities and complications were added to mitigate potential confounding of the RBC transfusion risk. These included measures of volume depletion (dehydration, vomiting), evidence of severe anemia (intravenous (IV) iron treatment), severe trauma and burns and the presence of severe bleeding during or after surgery. Other surgery-related complications were identified in the analysis, including hypertension, acute renal failure and polycythemia vera. Finally, cardiovascular procedures were subdivided based on whether the patients had on-bypass or off-bypass procedures. All additional comorbidities and complications where defined using (ICD-CM) versions 9 and 10.
Hospital-specific variables were also collected, including the number of beds, teaching status and geographic regions. For analysis, bed size was converted to standard categories similar to those reported by the American Hospital Association Annual Survey of Hospitals. These variables were used to control for geographic- and service-based variation in cost and resource utilization among the hospital service providers.
Unadjusted bivariate descriptive analyses were performed, comparing the baseline population characteristics and RBC transfusion, cost and LOS between the tHb- and Hct-monitoring cohorts. Chi-squared tests were used to test for significant differences between the patient populations for categorical variables. Fisher’s exact tests were used for low cell counts. Analysis of variance was used to test for significance in continuous variables with Mann-Whitney U tests used for non-normal distributions.
Multivariate regression techniques were utilized to isolate the effect of hemoglobin-monitoring type and control for other key factors that may increase the RBC transfusion risk, cost and LOS between the monitoring cohorts. RBC transfusion risk was compared using logistic regression methods. General linear methods (GLM) were used to model the LOS and cost utilization variables. Log transformations (negative binomial for LOS and gamma for cost) were applied to the resource utilization variables to adjust for the skewed distributions common among these types of data.14,17
Significance levels for the model parameter estimates were set at 0.05. All data analysis and statistical models for this study were generated using SAS/STAT software Version 9.4 of the SAS System (SAS Institute Inc., Cary, NC).
Results
The study population included 18,169 patients who underwent cardiovascular procedures with Hct-monitored patients accounting for 66% of the patient population. Patients monitored with Hct were more likely to have a dual CABG and VR procedure (10.4% vs 8.9%, p=0.0069). As expected, both cohorts were primarily male, with the Hct cohort slightly older than the tHb cohort (age 65.9 versus 65.0 years, p<0.0001).
More than half of the tHb group (51.1%) were treated in a major teaching facility compared to 13.1% of the Hct group (Table 1). In addition, tHb-monitored patients were more likely to be treated in facilities with 500 or more beds (51.3% vs 30.0%, p<0.0001) (Table 1).
Population Demographics and Characteristics.
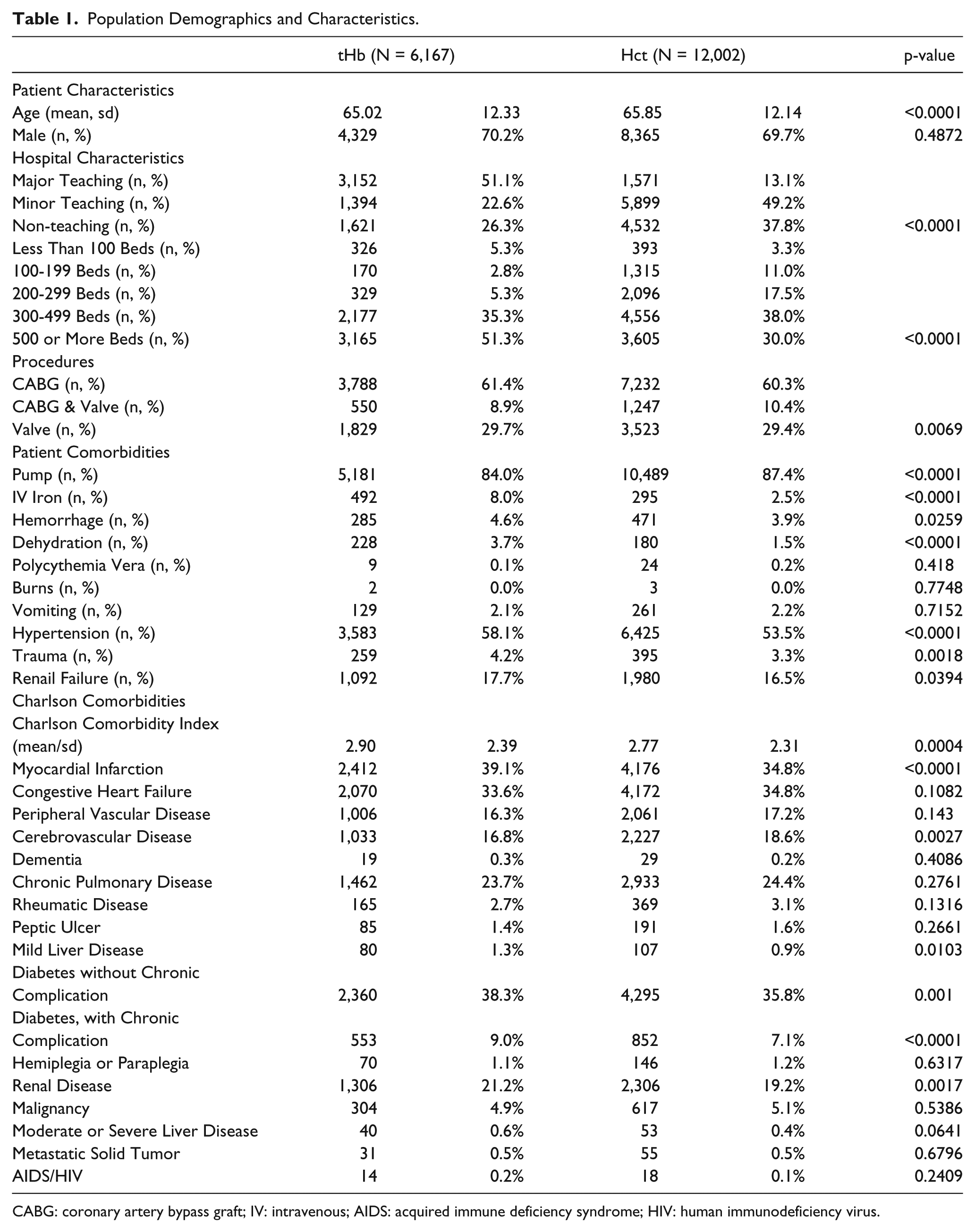
CABG: coronary artery bypass graft; IV: intravenous; AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus.
The Charlson Comorbidity Index score was higher for the tHb than the Hct group (2.90 vs 2.77, p=0.0004) with the most common comorbidities, including diabetes mellitus, myocardial infarction, congestive heart failure, and chronic pulmonary disease (Table 1). tHb-monitored patients were more likely to be administered intravenous iron (8.0% vs 2.5%, p<0.0001) and have diagnoses of trauma (4.2% vs 3.3%, p=0.0018), renal failure (17.7% vs 16.5%, p=0.0394), severe bleeding (4.6% vs 3.9%, p=0.0259) and dehydration (3.7% vs 1.5%, p<0.0001) (Table 1). Hct-monitored patients were more likely to have on-pump procedures (87.4% vs 84.0%, p<0.0001) than tHb-monitored patients (Table 1).
Red Blood Cell Transfusion Risk
The unadjusted RBC transfusion rate was higher in patients monitored with Hct (20.9% versus 18.9%, p=0.0014) compared to patients monitored with tHb (Table 2). After controlling for patient and hospital characteristics, as well as patient comorbidities, patients monitored with Hct had a 26% increased risk for RBC transfusion (OR=1.26, CI 1.15-1.38, p<0.0001) compared to patients monitored with tHb (Table 3). Other factors significantly increasing RBC transfusion risk included on-pump procedures (OR=2.30, CI 2.01-2.63, p<0.0001), diagnosis of trauma (OR=1.84, CI 1.37-2.47, p<0.0001), renal failure (OR=1.67, CI 1.52-1.85, p<0.0001), severe bleeding (OR=1.67, CI 1.26-2.20, p<0.0001) and administration of intravenous iron (OR=1.26, CI 1.06-1.51, p<0.0001) (Table 3).
Outcomes by Monitoring Type.
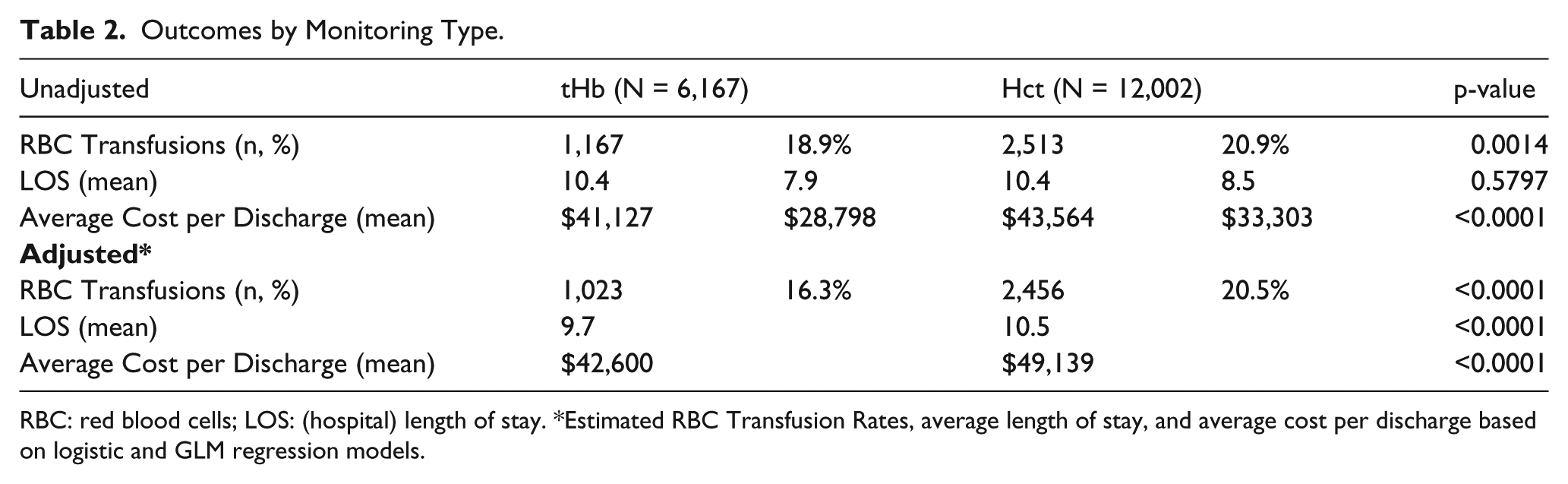
RBC: red blood cells; LOS: (hospital) length of stay. *Estimated RBC Transfusion Rates, average length of stay, and average cost per discharge based on logistic and GLM regression models.
Red Blood Cell Transfusion Risk Regression Results.
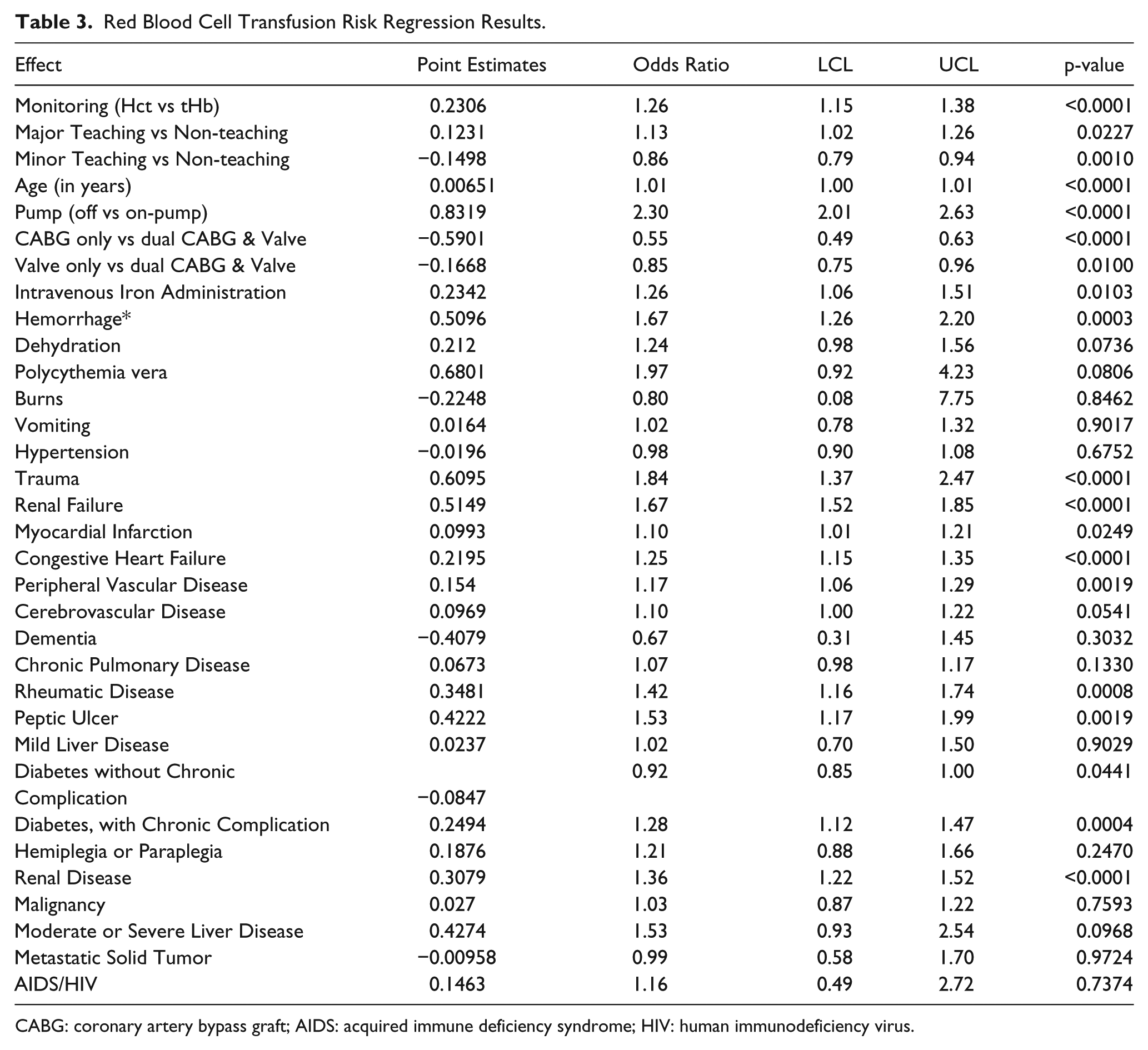
CABG: coronary artery bypass graft; AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus.
Hospital Length of Stay
The unadjusted average LOS was similar between the two groups (10.36 days for tHb vs 10.43 days for Hct, p=0.5797); however, patients monitored with Hct had an 8% increased risk for longer LOS (0.79 days, IRR=1.08, p<0.0001) compared to patients monitored with tHb, after adjusting for hospital characteristics, patient characteristics, patient comorbidities and RBC transfusion (Tables 2&4). RBC transfusion was a key driver of increased LOS (IRR = 1.25, p<0.0001), as were severe bleeding (IRR=1.60, p<0.0001), renal failure (IRR= 1.53, p<0.0001) and hemiplegia/paraplegia (IRR=1.40, p<.0001) (Table 4). Patients administered IV iron had longer LOS (IRR=1.28, p<0.0001), as did patients treated in major teaching facilities (IRR = 1.10, p<0.0001) (Table 4).
Length of Stay Regression Results.
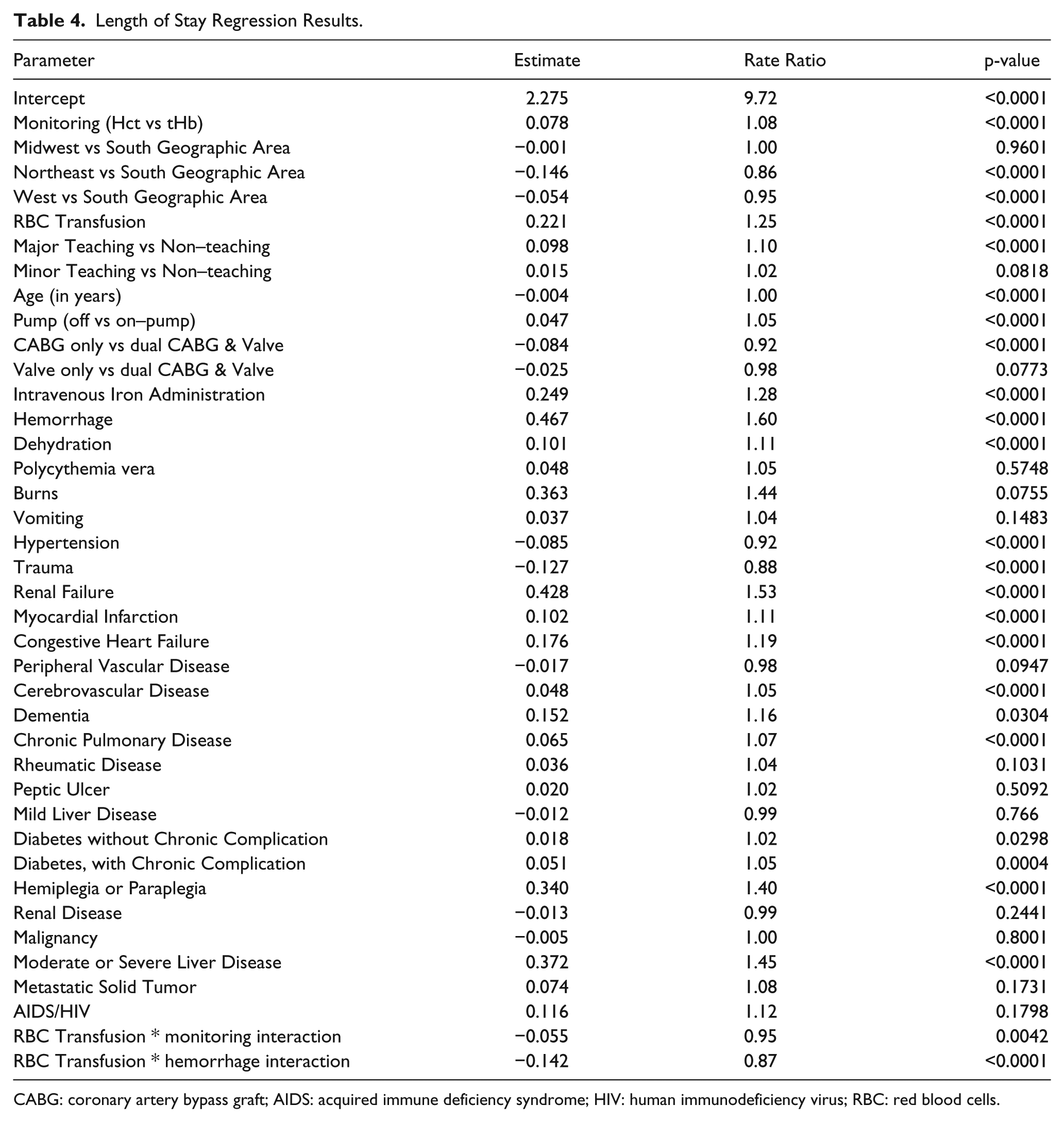
CABG: coronary artery bypass graft; AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus; RBC: red blood cells.
Total Inpatient Cost
Patients monitored with Hct had higher unadjusted costs of care ($43,564 vs $41,127 USD, p<0.0001) compared to patients monitored with tHb (Table 2). After controlling for the effect of RBC transfusion and LOS, as well as patient and hospital characteristics, Hct-monitored patients had an estimated 15% increased risk for higher hospital costs ($6,539 per discharge) (IRR = 1.15, p<0.0001) than those monitored with tHb (Tables 2&5). In addition to RBC transfusion (IRR=1.22, p<0.0001), patients with burns (IRR=1.72, p=0.0056), severe bleeding (IRR=1.41, p<0.0001) and severe liver disease (IRR=1.24, p<0.0001) had higher costs of care (Table 5). Patients treated in major teaching facilities (IRR=1.13, p<0.0001) also had higher costs of care (Table 5).
Cost Regression Results.
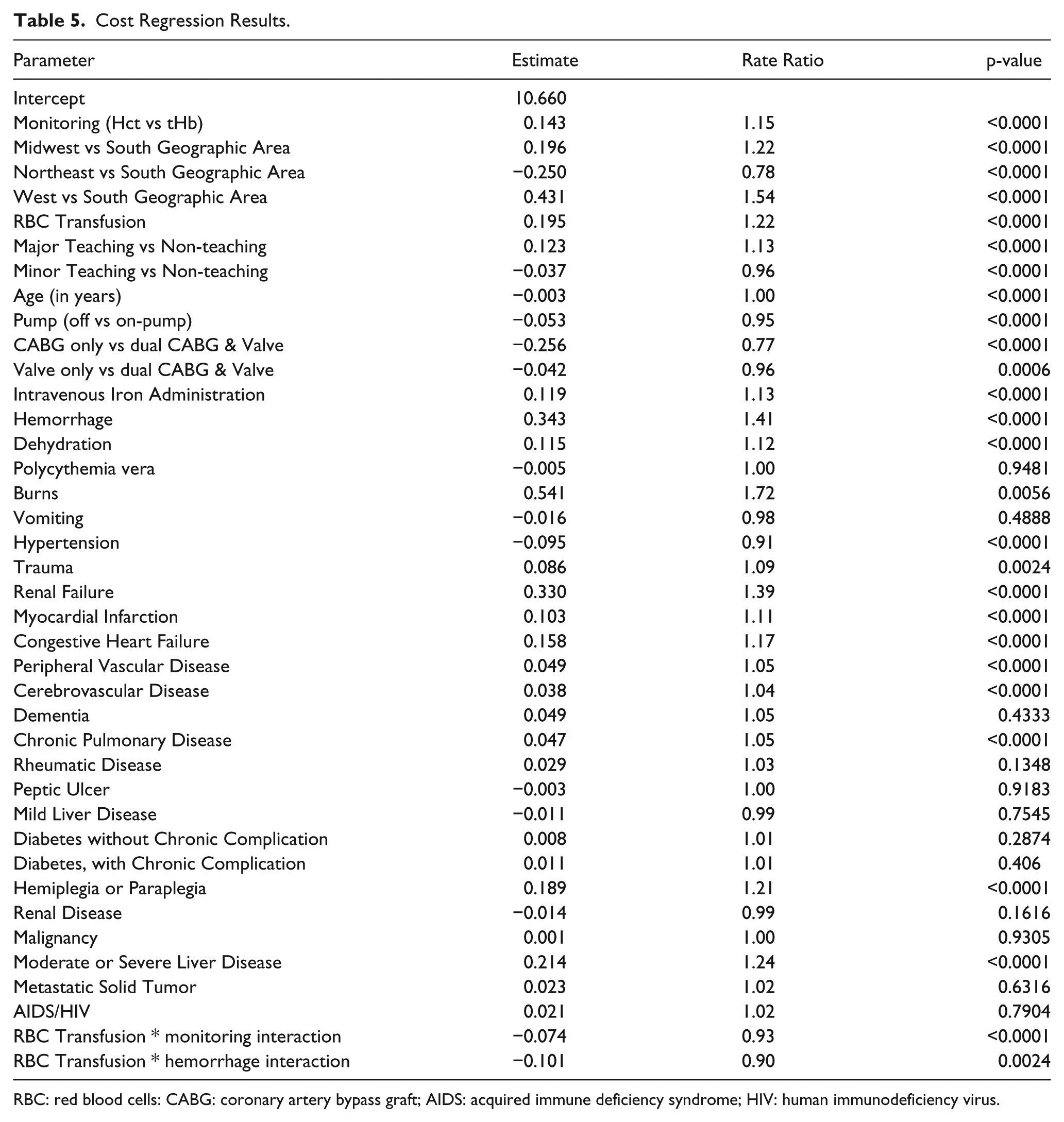
RBC: red blood cells: CABG: coronary artery bypass graft; AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus.
Subgroup Analysis
To examine potential bias associated with unmeasured heterogeneity across the surgical sub-populations, sensitivity analyses were performed. Multivariate regression analyses for each of the study outcomes were conducted separately for the CABG, VR and dual CABG and VR populations. In both the CABG (OR 1.47, CI 1.28-1.67, p<0.0001) and dual CABG and VR (OR 1.53 CI 1.17-2.01, p=0.0030) surgical populations, the Hct cohort had a significantly higher RBC transfusion risk compared to the tHb group. The RBC transfusion risk among Hct-monitored patients who underwent VR was higher than the tHb group (OR 1.07, CI 0.91-1.25, p=0.4177). However the results were not statistically significant.
Sensitivity analyses for the utilization outcomes mirrored the overall population analysis. Costs in the Hct cohort were predicted to be significantly higher than the tHb cohort for CABG (IRR = 1.15, p<0.0001), VR (IRR = 1.16, p<0.0001) and dual CABG and VR (IRR =1.17, p<0.0001). Similarly, the Hct cohort had longer LOS estimates for CABG (IRR = 1.09, p<0.0001), VR (IRR = 1.06, p=0.0076) and dual CABG and VR (IRR = 1.09, p=0.0117) when compared to the tHb cohort.
Discussion
This study demonstrates lower RBC transfusion risk, hospital LOS and cost for cardiovascular surgery patients when tHb is measured compared to Hct. Sensitivity analysis that isolated the individual surgical populations confirmed these results with the exception of the VR population. This variance may be explained by the increased likelihood of RBC transfusion among VR patients unrelated to hemoglobin monitoring.18,19 Given the tHb cohort had a higher occurrence of severe bleeding, it is unlikely that bleeding was the cause of increased RBC transfusion in the Hct cohort.
Reduction in resource utilization as measured by LOS and total hospital cost followed the lower RBC transfusion risk rates in the tHb cohort. These results were confirmed in the surgical sub-population sensitivity analyses and are consistent with other published data which have demonstrated significant reductions in LOS and/or cost associated with lower RBC transfusion rates.14,18 The economic impact of unnecessary RBC transfusion imposes a significant burden on this patient population. Estimated incremental hospitalization costs associated with blood product transfusion range from $4,408 USD for intraoperative transfusion to over $10,000 USD for post-operative transfusion.20,21 Similarly, estimates from this study show a possible increase risk for costs associated with Hct testing of approximately $6,539, an increased risk for LOS of 0.79 days with Hct testing and an increased risk for RBC transfusion of 26% with Hct testing.
Though not measured in this study, it is likely that reductions in transfusion-associated complications accompanied the reduction in RBC transfusion in the tHb population.4,22 It has been well described that a reduction of post-operative complications can significantly reduce overall hospitalization costs and reduce LOS amongst cardiac surgery patients.14,23
It should be noted that these results suggest only a strong association between tHb monitoring and a reduction of RBC transfusion in this population and do not imply causation. It is likely that other factors combined with the use of the tHb for hemoglobin monitoring play a role in the reduction in the need for RBC transfusion. Although many of the clinical factors that can increase the risk for RBC transfusion, such as on-pump bypass, anemia, renal failure, hypertension, dehydration and severe bleeding, were controlled for in the regression models, other factors, such as length of surgery and hospital transfusion protocols, were not able to be measured and controlled for in the regression analysis.
Given the large sample size, the demographic and geographic diversity of the patient cohort and the clinical capabilities of the study hospitals, these results can be considered representative of treatment patterns within the United States. However, there are some limitations of this study that warrant mention. The data source is subject to those limitations known to be associated with the use of large scale administrative data, including inconsistent coding and billing practices and incomplete records.24,25 The study was also limited to the inpatient hospital setting and did not account for the full continuum of care. Finally, this study does not account for the presence of any procedural differences (e.g. priming volumes, circuit sizes), variances in bleeding vigilance by physicians or hematologic expertise, hospital protocols designed to minimize RBC transfusion, variance in provider RBC transfusion thresholds or programs designed to minimize intraoperative blood loss.26,27
Nevertheless, these findings suggest that tHb monitoring during cardiovascular surgery could offer a significant reduction in the need for RBC transfusion, as well as measurable reductions in LOS and hospital cost compared to Hct monitoring. Given that this study is the first to document these associations, additional studies across varying data sources and study populations is warranted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this analysis provided by Instrumentation Laboratory, Bedford, MA.