
Abstract
Sourcing and including the views of children in speech and language therapy aligns with Articles 12 and 13 of the United Nations Convention on the Rights of the Child. This research explored the perspectives of 30 children (3;9–8;7 years) with childhood apraxia of speech regarding their experiences of Dynamic Temporal and Tactile Cueing intervention. Children lived in the United States or Australia and had engaged in one of three intervention studies exploring: delivery by their parent or speech and language therapist; delivery in high or low dose; and delivery in massed or distributed format. Children shared their perspectives of intervention through drawing a picture of themselves during intervention, describing their drawings, and identifying emojis responding to questions about intervention. Five focal points were identified in the drawings: Place (73.33%: environment, intervention materials, and transitions), People (73.33%: body parts and facial expressions, relationships and connection, and sense of self), Activity (20.00%: words, talking, and listening), Emotion (53.33%: positive and negative), and Not Talking (6.67%). Many participants felt happy about ‘speech practice’ (☺ 62.50%) and who did speech practice with them (☺ 62.50%) but were divided in how they felt about the number of times (☺ 33.3%) and the length of time (☺ 29.17%) of speech practice. Children's perspectives can be considered when designing and delivering intervention.
Keywords
I Introduction
For many years, speech and language therapists (SLTs) have been aware of the need to consider the perspectives of clients as a core element of evidence-based practice (Dollaghan, 2007; Roulstone, 2015; Sackett et al., 1996, 2000). However, in practice, particularly for those working with children, sourcing, hearing, and acting upon children's perspectives has presented challenges (Lundy, 2007). In recent years, the need to include children's perspectives in decision-making has received strong endorsement (Lyons et al., 2022; Mahony et al., 2024; McCormack et al., 2010; Roulstone & McLeod, 2011), and a number of researchers have created or recommended a range of methods and tools to enable SLTs to do so (e.g. McCormack et al., 2022; McLeod, 2004; Merrick & Roulstone, 2011) drawing on the concept of the ‘hundred languages of children’ (Malaguzzi, 1998). In addition to the range of methods available, an attitude of openness is also required. As Lyons and colleagues (2022) remind us, children have many ways of communicating and so ‘employing curiosity, empathy and creativity…will enable us to be more open and responsive to new perspectives and to move beyond the limitations of current practice’ (p. 547). All of this aligns with Articles 12 and 13 of the Convention on the Rights of the Child (United Nations, 1989). Very young children can reflect on and talk about their own and others’ emotions and by middle childhood gain insight that others may have different thoughts and feelings (Bretherton et al., 1986; McDevitt et al., 2020 for a review). However, Lundy (2007) also reminds us that an openness to sourcing and hearing children's voice is insufficient. She encourages us to consider also how children's perspectives may be given ‘due weight’ by providing an ‘audience’ and ‘influence’ (p. 927).
II Listening to children in clinical activities
With a renewed commitment to listening to children, and in a spirit of identifying how children's voices can have influence in practice, we might consider the range of clinical activities during which their voices may be heard. A relative strength within the research and practice space is the sourcing of child perspectives as a component of assessment (McCormack et al., 2019). Asking children about their talking to help inform an understanding of their communication strengths and needs is enabled through a range of tools (e.g. the KiddyCAT – Vanryckeghem & Brutten, 2007; SPAA-C – McLeod, 2004; drawing talking – McCormack et al., 2022; McLeod et al., 2025; narrative inquiry – Lyons & Roulstone, 2018). Data from these assessments can be triangulated with evidence gathered from other sources to help clinicians and families make clinical decisions about intervention targets and approaches. However, during and after intervention, it is also important to source and hear children's voices to understand the client/consumer experience as a core element of evidence-based practice (Dollaghan, 2007; McLeod et al., 2023). Gathering the perspective of children during intervention can help measure client progress, monitor client satisfaction and factors influencing engagement and success, and enable adjustment to goals or approaches to ensure they meet child and family needs. Gathering children's perspectives after intervention can be a helpful form of outcome measurement but also help identify the factors that facilitated (or hindered) the achievement of outcomes; that is, the ‘active’ ingredients (Baker et al., 2018).
III Outcome measurement
Despite funding and policy often requiring outcomes to be measured to demonstrate intervention effectiveness and/or the need for ongoing services, the question remains of what outcomes (and whose) should be measured. Roulstone (2015) summarised work undertaken through the Better Communication Research Program in the UK which gathered information from parents and children regarding the outcomes they value. In essence, she reported, ‘parents value changes in their child's communication that lead to functional changes for the child’ (Roulstone, 2015: 214) such as in social inclusion or independence. She found that children valued having fun and their achievements, particularly outside of school life or communication activities. Roulstone questioned whether these outcomes typically were considered within intervention research. Similarly, other researchers (Baker et al., 2022; McCormack et al., 2025) have identified a current lack of research exploring social participation outcomes. A challenge seems to be the lack of tools. Given the nature of participation outcomes, self-report or report by significant others via checklists/interviews would seem to be the most appropriate to use, but few of these exist. There are even fewer examples of tools for evaluating experience within speech and language therapy. Yet, self-determination theory (Deci & Ryan, 1985) tells us that a therapeutic relationship that is warm and structured and supports autonomy can increase client motivation and lead to positive outcomes in speech and language therapy practice (Haerens et al., 2021). Thus, sourcing and understanding children's experiences of intervention could be key in identifying factors that contribute to good outcomes.
IV Components of intervention and the active ingredients
Baker et al. (2018) reviewed empirically supported speech intervention and created a taxonomy of phonology treatment elements, to help researchers, among others, to identify the ‘elements that deserve greater scrutiny’ (p. 910), due to their role in supporting/driving intervention success. These include Goal (area of focus; characteristics of the target; linguistic context of the stimulus; goal progression strategy), Teaching Moment (antecedent event; response; consequent event), Context (agent; venue, session format; resources; activities), and Procedural Issues (intensity; training; evaluation). The relative importance of some elements has been explored further in empirical studies, such as those focused on questions of dosage (Baker, 2012; Cummings et al., 2021; Zeng et al., 2012). However, the importance of elements from the client's perspective is lacking. Exploring the clients’ experience of intervention might help to highlight the elements they consider most necessary and shed light on how we design and deliver intervention that may support their autonomy, increase motivation, and succeed in positive social participation outcomes. Some researchers have explored patient experience in other paediatric settings but often with children school-aged and above (McLeod et al., 2023; Merrick & Roulstone, 2011; Owen et al., 2004; Pennington et al., 2020; Simkin & Conti-Ramsden, 2009; Van Poucke et al., 2025). These studies have identified while many children enjoy attending speech and language therapy (e.g. activities and rewards), and their relationship with their SLT, they have mixed emotions about the time and timing of intervention (e.g. during school time), and peer perspectives (e.g. embarrassment). The voice of children in speech and language therapy settings is limited; in particular, the voice of young children with unintelligible speech.
V Context
This research was funded by the Once Upon a Time Foundation to consider the perspectives of children with childhood apraxia of speech (CAS) about intervention. The children had all participated in other research studies exploring the effectiveness of Dynamic Temporal and Tactile Cueing (DTTC, Strand, 2020) when delivered in three different forms. The first study compared outcomes for high versus low dose intervention (Iuzzini-Seigel et al., 2023) whereby children received either twice weekly intervention for 12 weeks (low dose) or four intervention sessions per week over 6 weeks (high dose). The second compared massed versus distributed intervention whereby children received either 1-h of intervention three times per week (distributed) or one 3-h intervention session once per week (massed) across 8 weeks of intervention. The third study compared SLT versus parent-supported intervention with children in the parent-supported intervention completing home practice with their parent(s) three times per week in the treatment phase and six times per week post-treatment.
Following completion of their intervention, the children and their families were invited to participate in the current research study. Intervention for the three DTTC studies previously had been provided by community-based SLTs and the intervention research teams who collected data before, during and 1, 4, and 12 weeks after intervention. Whole word accuracy was the outcome measure for the DTTC studies considering segmental, phonotactic, and suprasegmental accuracy (Iuzzini-Seigel et al., 2023). An exploration of SLT and parent perspectives of delivering the intervention was also undertaken with a small sample who participated in the dosage study (Thomas et al., 2025). The current independent research is focussed on the children's perspectives about engaging in the DTTC intervention.
VI Aims
The overarching aim of this study was to explore the perspectives of children with CAS regarding their experiences of DTTC intervention as conveyed through their drawings.
VII Method
1 Ethical approval
Ethical approval for this study was acquired through the Australian Catholic University Human Research Ethics Committee (Ethics application number 2023-3256H). Information about the study was provided to participants online and through printed information. Parents provided written informed consent before their child completed the study. Child assent was obtained from the children prior to participating (Merrick, 2011; McCormack et al., 2022).
2 Participants and recruitment
Participants were recruited through purposive sampling via the children's community-based SLTs involved in the three DTTC studies. Their SLTs shared a printed flyer and the online information and consent form. Inclusion criteria for eligibility in the current study were (a) participation in one of three DTTC studies, (b) submission of written parent consent forms, and (c) child assent to participate in the current research. Participants were reimbursed for participating in the current research by receiving a small payment.
The three DTTC studies involved 106 children (some of these children were ineligible because they had completed the intervention research prior to recruitment for the current research commencing; as such, they could not receive information about this study from their SLT). There were 34 parents who completed the consent forms for the current study. There were two families who were unable to schedule a time to complete interviews. One child did not provide assent for participation and was withdrawn on that basis. One child and family completed the data collection for the study, but then withdrew. Consequently, there were 30 children who completed both phases of the current study.
The 30 participants had a primary diagnosis of CAS. They ranged in age from 3;9 to 8;7 years (M = 5;6 SD = 2;3) and there were 22 males (73.33%) and 8 females. The participants all spoke English and lived in the United States (n = 28) and Australia (n = 2). Each participant was in one of the three DTTC intervention studies: either in the dosage RCT (n = 19, 63.33%), block intervention study (n = 5, 16.67%), or the parent intervention study (n = 6, 20.00%). Half were in the control group (n = 15, 50.0%), 10 were in the intervention group (n = 10, 33.33%), and the remainder were unsure which group they were in (n = 5, 16.67%).
3 Research team: Positionality
The six-member research team in the current study consisted of five English-speaking SLTs and one multilingual clinical psychologist, all of whom have experience in researching children's perspectives of communication. One SLT lived in the United States and had extensive experience working in the education system and the remaining research team lived in Australia.
4 Instruments
This study used three child-friendly techniques to gain children's perspectives: drawing, visual emoji scales, and interviews.
The Sound Effects Study Drawing Protocol (McCormack et al., 2022) was adapted to support children to express their views about their DTTC intervention. In the current study, the participants were asked to ‘draw a picture of yourself during speech practice’ then answer questions about their experiences and perspectives. They were given two opportunities to draw, first with a parent, then with a researcher (with parent present). The second drawing was elicited if the child wanted to complete a second drawing or the first one was not available as a digital upload. The five stages of the Sound Effects Study Drawing Protocol (McCormack et al., 2022) was adapted for the current study: (a) Preparation (b) Drawing/Observing, where the child draws and the parent/SLT/researcher is quiet, (c) Responding/Discovering, where the adult asks the child to describe the drawing, (d) Identifying, where the researchers identify key focal points, and (e) Summarising insights from the child to inform practice.
5 Data collection
A two-phase process was used to collect data. Phase one of the study involved seeking consent from parents and ensuring that families had materials (markers, paper, and directions). Instructions and a short training video were available and directed parents to ask the child to draw a picture of them doing DTTC using the materials provided. After completion of the drawing, parents asked their child specific questions about the drawing and completed a response form. The child's drawing and parent response form were submitted digitally to the research team and parents could send a video of the child completing the drawing. All drawings were received and no participants elected to make a second drawing during the online interview. Demographic information was collected, regarding the children's age, interests, diagnosis, participation in DTTC research, location, and time since research DTTC ended, if they had ceased intervention before the data collection for the current study commenced.
Phase two of the study involved an online interview with the child and parent conducted by a member of the research team. The interviews began with rapport building as the interviewer explained that the child and parents would be helping others learn about DTTC or ‘speech practice’, confirmed demographic information with the parent, sought child assent for recording of the interview, and the child's selection of a pseudonym. Next, the researcher shared the image of the child's drawing onscreen and asked a series of open-ended questions about the drawing/artefact submitted in Phase one. A series of emojis were shown onscreen with labels being provided by the interviewer (e.g. happy, in the middle, sad, and I don’t know or make up your own feeling). An on-screen laser pointer was used to highlight each emoji. Participants responded verbally and if participants pointed to the emoji on screen the parent verbally indicated which emoji was selected. The examiner's initial description of the emojis was ‘Here's my pointer. OK, so this one's happy, this one's in the middle and this one's sad. This one's for a feeling that's not on the screen’. Children were asked two questions and asked to indicate the way they feel to answer each question. The first emoji question was ‘How do you feel about the way you talk?’ The second emoji question was ‘How do you feel about your speech practice with [SLP]?’ Follow-up prompts included: ‘What would you call that feeling?’ ‘Why did you choose that feeling?’ ‘What made you feel [participant's response]?’ ‘Can you tell me how you feel about the way that you talk?’ were used in an attempt to gather additional information. The following is an excerpt from an interview demonstrating the use of initial prompts and follow-up questions as well as creation of a new feeling response by a participant: Researcher: So this face is happy. This face is in the middle. This face is sad and Child (P30): “Mad” Researcher: “Mad? OK. And you can make up your own face if you want. You can make up your own feelings. OK? Researcher: How do you feel about the way you talk? Is it one of those or a different one? OK, how do you feel about the way you talk? Is it one of those or a different one? Child (P30): In the mid. In the middle? Researcher: In the middle? Child (P30): Yeah. Researcher: OK. And why do you say, why did you pick in the middle for talking? Child (P30): I have cough a lot. A lot of times. Researcher: Oh, you have to cough. OK. You have to cough a lot of times. OK. And how do you feel about speech practice with Miss XXX? Child (P30): mmmm Good. Good. I. Good. Mother: Which face? Good? Researcher: Good. Oh, I think you're making up a new one. Right? You're making up your own word. Child (P30): Yeah.
The interview continued with a discussion about DTTC speech practice including questions such as ‘Tell me about your speech practice?’ and questions asking what participants liked and didn’t like about going to speech practice (these data are analysed in a subsequent paper). A question was added to ask about the specific treatment condition, if the condition was disclosed to the researchers.
Throughout the interview, parents were asked to clarify unintelligible comments. At the conclusion of the interview, parents were offered an opportunity to share any additional information and the recording was ended. The interviewer thanked participants and explained they would be sent a copy of the transcript and invited to make changes or provide clarification, and the interviewer then answered any questions. Recordings of each interview were uploaded to a secure server for transcription and deidentification. Participants were given the opportunity to review the transcripts prior to analysis and make edits as needed.
6 Data analysis
The children's drawings and descriptions of their drawings from Phase one and two of the study were considered together by the research team. First the drawings were displayed on a large table. The research team considered each drawing, read the descriptions then identified focal points or ‘…what our attention focuses on in the picture’ (Furth, 2002: 32). The key points were written on a whiteboard. Then the team determined overlapping concepts by comparing the list with the six focal points from the Sound Effects Study with the current study: (a) body parts and facial expressions, (b) talking and listening, (c) relationships and connection, (d) positivity, (e) negativity, and (f) no talking (McCormack et al., 2022). By going back and forth between the drawings and the categories, five main focal points with subpoints were identified (Table 1). Triangulation among team members and different sources of data enhanced credibility. Next each drawing and explanation was analysed and key focal points were identified (as many as appropriate per drawing). Finally, the children's responses were collated regarding questions about how they feel about their speech, speech practice, how many times they did speech practice, how long they did speech practice and with whom they did speech practice.
Children's drawings of DTTC intervention: focal points, identifying features, and occurrence (n = 30).
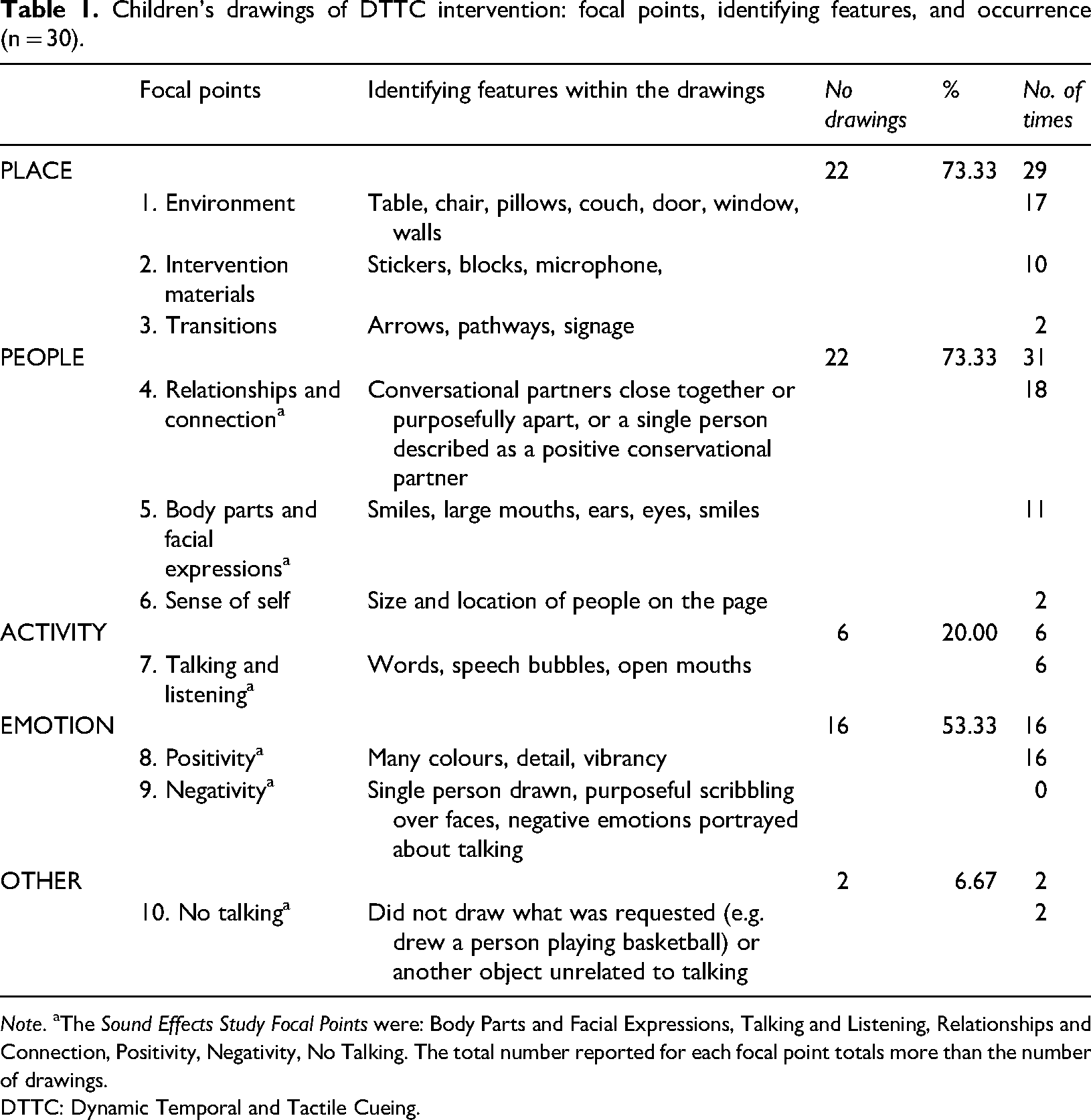
Note. aThe Sound Effects Study Focal Points were: Body Parts and Facial Expressions, Talking and Listening, Relationships and Connection, Positivity, Negativity, No Talking. The total number reported for each focal point totals more than the number of drawings.
DTTC: Dynamic Temporal and Tactile Cueing.
VIII Results
Thirty children's drawings and interviews were analysed. In the sections below, pseudonyms are used in place of children's names. The children selected their preferred pseudonym.
1 Children's drawings of Dynamic Temporal and Tactile Cueing intervention
Children were able to draw themselves undertaking DTTC intervention and explained their drawings to the researcher. Five main focal points were identified during the analysis of the children's drawings and descriptions relating to: Place (n = 22, 73.33%), People (n = 22, 73.33%), Activity (n = 6, 20.00%), Emotion (n = 16, 53.33%), and Not Talking (n = 2, 6.67%) (Table 1).
a Place
Place was illustrated in three ways: environment, intervention materials, and transitions.

Mr M’s (5;8) drawing of Dynamic Temporal and Tactile Cueing intervention illustrating the environment (table) and body parts (ears). Reprinted with permission from Anna Cronin, Jane McCormack and Sharynne McLeod.
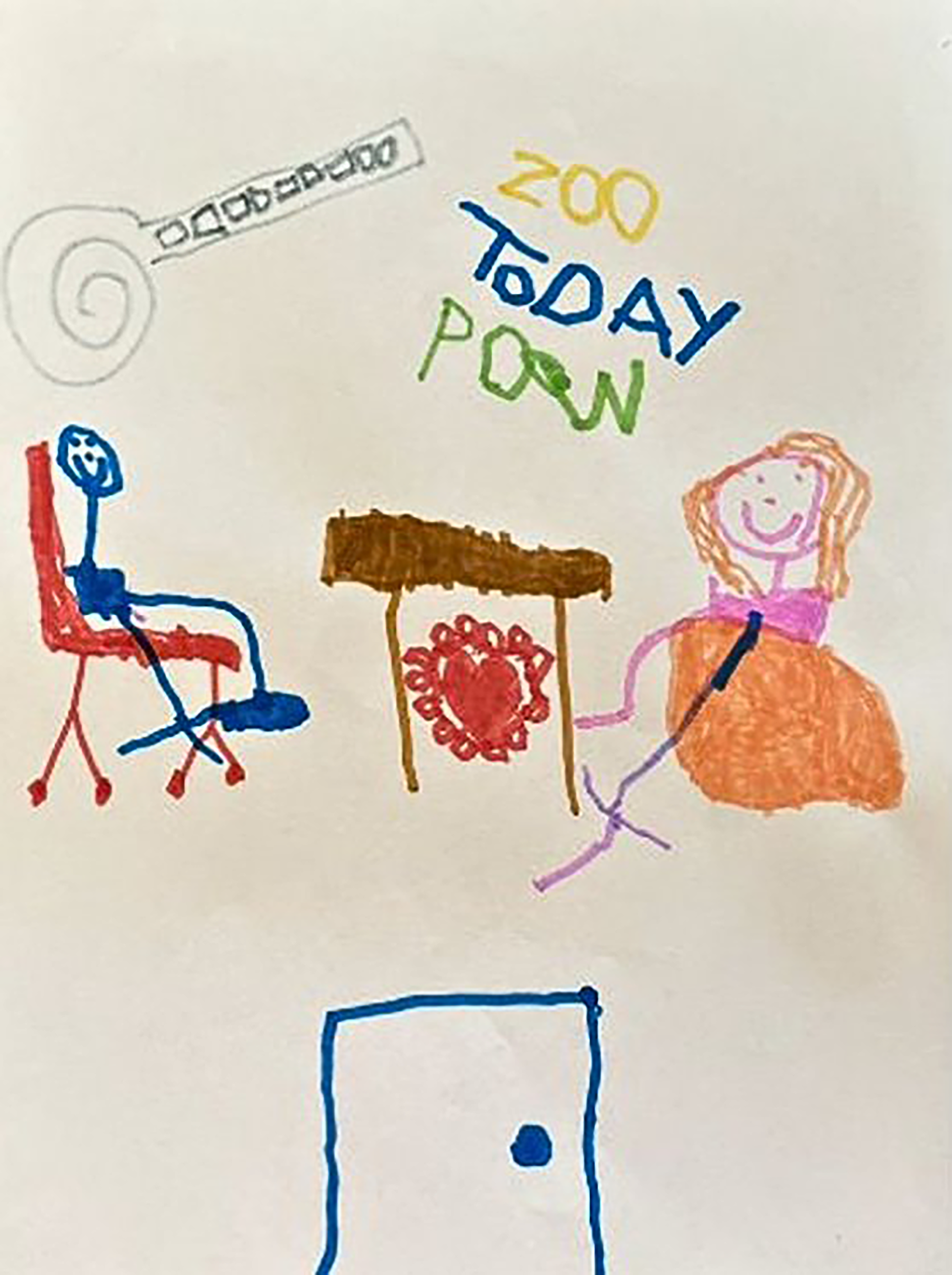
Captain America's (5;8) drawing of Dynamic Temporal and Tactile Cueing intervention illustrating the environment (door, table, chairs, cushion), intervention materials (roll of stickers), and activity (‘words we practiced’), and positivity (heart). Reprinted with permission from Anna Cronin, Jane McCormack and Sharynne McLeod.
b People
The participants illustrated people in three ways emphasising: body parts and facial expressions, relationships and connection, and sense of self.
c Activity
The participants illustrated activity by drawing words, talking, and listening. Captain America (5;8) wrote words from his intervention tasks ‘zoo, today, pow’ above the figures in his drawing. Similarly, Mr Bob (4;2) drew a picture of himself sitting opposite his SLT with the word ‘stop’ between them. He indicated the drawing was of him and his SLT ‘practicing the word “stop”’. Luigi (6;5) wrote words at the top of his drawing and explained that he was asking his SLT to ‘help me’.
d Emotion
The participants illustrated positive emotion and none illustrated negative emotion.
e Not talking
A few participants chose not to draw talking. Godzilla (6;1) drew a picture of ‘Godzilla’ and Cool Dude (5;10) drew himself playing football in the sun, rather than speech practice, indicating that football was something he really enjoyed: ‘you know, look at this smile and you, and you understand’.
2 Children's emoji responses about Dynamic Temporal and Tactile Cueing intervention
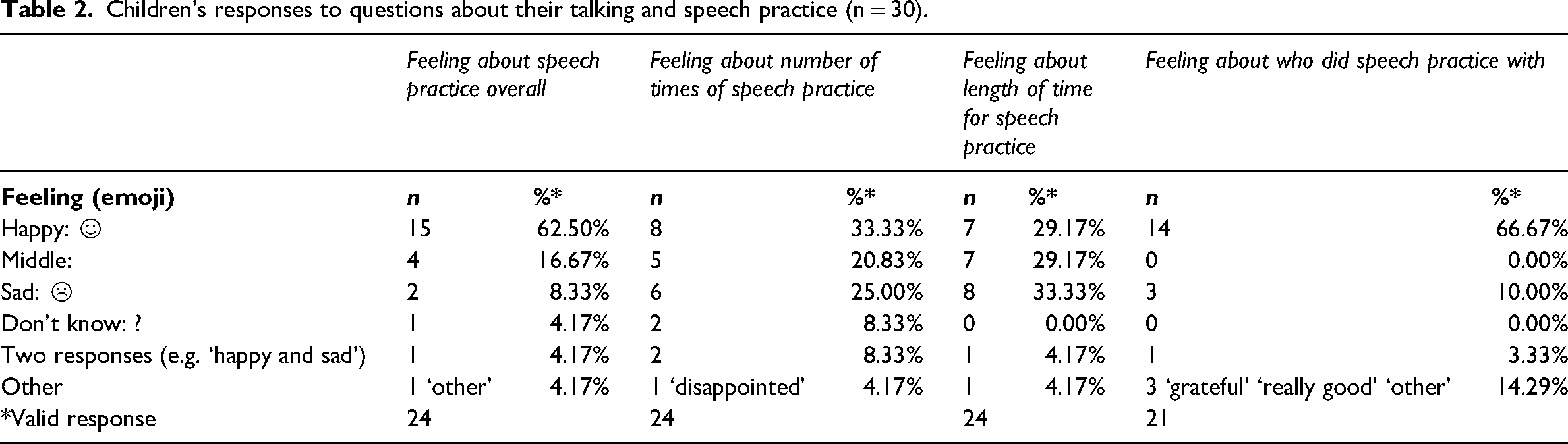
During the interviews, the participants were asked to indicate how they felt about different aspects of intervention by selecting between emojis (Table 2). Not all participants answered each question. Generally, participants indicated that they felt happy ☺ about speech practice (☺ n = 15, 62.50%), and who they did speech practice with (☺ n = 15, 62.50%) and another two said ‘grateful’ and ‘really good’. Participants were divided in how they felt about the number of times they did speech practice (☺ n = 8, 33.3%) and how long they did speech practice (☺ n = 7, 29.17%).
Children's responses to questions about their talking and speech practice (n = 30).
It was not possible to compare children's responses across conditions due to the small number of participants and some missing data related to allocated condition in the parent-supported intervention study and the massed/distributed intervention study. However, children's responses could be explored in the low-/high-dose randomised controlled trial study (see Table 3). The sample size was still too small for statistical analysis; however, the trend indicates that regardless of condition, the majority of children reported feeling happy ☺ about speech practice and about who they did speech practice with. They were divided in their responses regarding the number of times they did speech practice and how long they did speech practice.
Children's responses to questions according to condition in the RCT (low/high dose) study (n = 15).
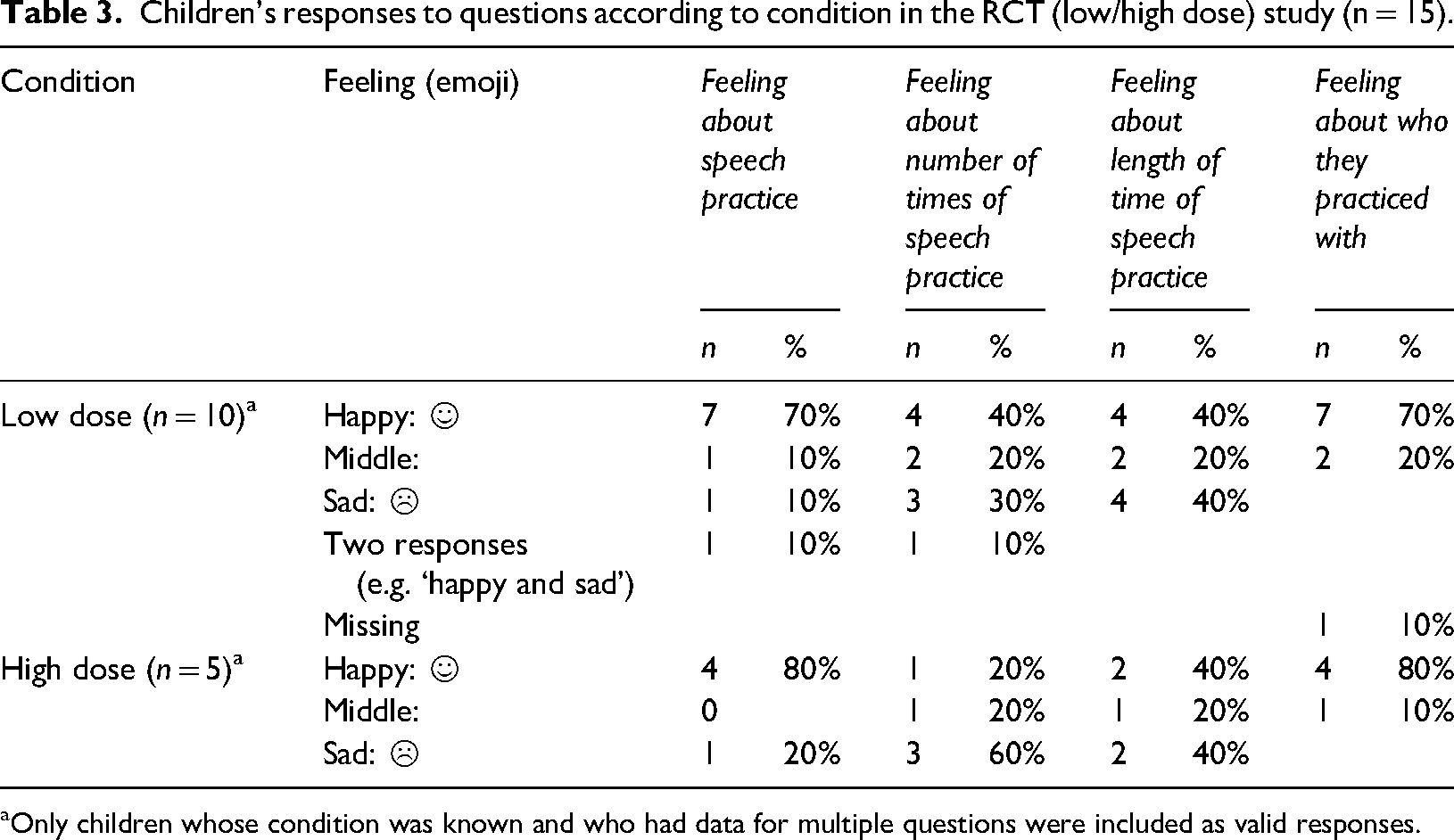
aOnly children whose condition was known and who had data for multiple questions were included as valid responses.
IX Discussion
This study used evidence-based research methods for collecting children's perspectives about SLT intervention. The research team recognised the value in using different data collection methods to provide children with a voice and audience to share their perspectives inspired by the work of researchers from across the world (e.g. Mahony et al., 2024; Roulstone & McLeod, 2011). The use of drawings was selected as they provide a natural language for children, enabling them to project and reflect their inner worlds and feelings. Subsequent checking with the children via asking them carefully designed questions enabled understanding and interpretation of their drawing to be confirmed.
The drawings and responses to questions provide evidence of children's ability to represent and/or describe their intervention experiences, as the children often detailed elements of intervention that are a focus of SLT intervention (e.g. cards, stickers, blocks). These are discussed in the following section. Additionally, the children's drawings provide points for clinician and researcher reflection, particularly the focal points or features of intervention children emphasised in their pictures. In the section that follows, the focal points are discussed and compared to the taxonomy of phonological intervention proposed by Baker and colleagues (2018). While we take care not to over-analyse the relative importance of the focal points, we believe a description of children's experiences and a comparison of their perspectives of intervention experiences with empirical/objective descriptions of intervention approaches, can provide an important contribution to thinking about intervention design and delivery. Furthermore, we believe that only through such reflections do we allow children's voices to have the opportunity for meaningful influence (Lundy, 2007).
1 Focal point analysis
Within the current study, five main focal points were identified during the analysis of the children's drawings and descriptions. These related to: (a) place, (b) people, (c) activity, (d) emotion, and (e) no talking. While the Sound Effects Study Drawing Protocol was used, the focal points in the current study were slightly different from those reported by McCormack et al. (2022): (a) body parts and facial expressions, (b) talking and listening, (c) relationships and connection, (d) positivity, (e) negativity, and (f) no talking. The key difference between the two studies was in the identification of Place as a focal point in the current study, which was not noted in McCormack et al. (2022). This difference may reflect the difference in instructions provided to the children in each; that is, in the original study, children were asked to draw themselves ‘talking to someone’ and in this study, they were asked to draw themselves ‘doing speech practice’. However, it might also highlight the importance of the setting/environment/context as a key element of intervention. Other differences between the two sets of focal points predominantly reflect differences in categorisation of the features within each study. That is, People included ‘relationships and connection’ and ‘body parts and facial expression’; Activity included ‘talking and listening’; Emotion included ‘positivity’ and ‘negativity’ (although only positivity was noted).
2 Place
Within the current study, Place was reflected in three ways by the children: the environment, the intervention materials, and transitions. In the phonological taxonomy (Baker et al., 2022), the domain of Context included both ‘venue’ and ‘resources’, which align with the first two elements illustrated by children. Thus, empirical research and children seem to recognise intervention occurs in a particular setting and with particular materials that are specific to speech and language therapy intervention. While Strand (2020) doesn’t highlight venue/place as a key element of DTTC intervention, she does describe the use of reinforcers. Strand recognises the challenge of balancing the use of treatment time with maintaining children's attention and engagement and so recommends using ‘very quick reinforcers that keep the child engaged and looking at the clinician's face’ or using tokens that can be exchanged for a prize after a number of trials (Strand, 2020: 44). In the current study, children illustrated stickers and blocks (quick reinforcers) in their pictures and referred to toys ‘in the cabinet’ (Bowser, 4;9), presumably for play at the end of the treatment session. They also commented on natural reinforcement, such as praise, provided by their SLT as the session progressed.
One feature of children's drawings that is not discussed by Strand (2020) or apparent in the phonology taxonomy (Baker et al., 2018) is that of ‘transitions’. Indeed, it may not be a feature we typically reflect on in our research or practice with children, but perhaps we should. It was clear for some children intervention was perceived as separate to, and a distance from, other familiar settings and people – this was represented through doors (Captain America 5;8 – Figure 2), the map Ash (8;7) drew to get to the therapy room, and the representation of parents ‘outside’ the therapy room and looking in the window (Luigi, 6;5 and Rider, 4;5). For some intervention approaches and in some service delivery models, this separation might be preferred/necessary, but it might be important for us to consider how we prepare and support children for this to ensure readiness and willingness to engage. For another child (Mr Cheetah, 6;4), transitions within the intervention were identified – through arrows drawn from the therapy table to where the rest breaks were taken. Again, considering the length of sessions, the number of activities, and how we provide children with autonomy to identify when rest breaks or activity changes are needed might be something to consider. Self-determination theory would suggest this autonomy-supportive approach might lead to more motivated clients and more positive outcomes (Haerens et al., 2021).
3 People
In the current study, People were represented through body parts, facial expressions and relationships, as well as sense of self. Again, some of these elements are reflected in the phonological taxonomy proposed by Baker et al. (2018). For instance, the domain of Context includes ‘agent’ and the domain of Teaching Moment reflects the ‘antecedent-behaviour-consequent’ event that may be reflected in children's representations of body parts and facial expressions. Thus, both objective descriptions of the intervention and the children involved in this study recognise the agent of intervention and their role in delivery. The role of the agent is a feature of DTTC (Strand, 2020). As a type of integral stimulation, DTTC is based on a procedure of having the child imitate a target produced by the clinician, who then provides feedback.
The emphasis on body parts and facial expressions in the children's drawings is particularly interesting, given the alignment with DTTC. As Strand (2020) states, a feature of this intervention is that ‘The clinician frequently reminds the child to “watch my face” or “look at me” so that the child has repeated opportunities to observe the visual model while hearing the auditory model’ (p. 44). Children like Mr M recognised they had to ‘hear what Miss SLT was saying’ during the intervention sessions.
A feature of children's drawings not represented in the taxonomy, or discussed in Strand's (2020) description of the intervention, is children's ‘sense of self’. It is perhaps not something we typically consider in our clinical/research activities. Again, perhaps we could. In Dude's (5;7) picture, he represented himself and the SLT as small images in a big room. This could reflect his (limited) sense of autonomy and influence in the bigger context of intervention completion. Considering how we might involve children in intervention – through helping select targets, stimuli, activities, or reinforcement – may be beneficial in helping build autonomy and self-determination.
The children's responses to the feelings/emoji questions are also interesting to reflect on here. Given the lack of difference observed in children's feelings (emoji responses), regardless of intervention condition, it may be that how they feel is less related to the frequency or duration of sessions and more related to the person delivering the intervention, again highlighting the importance of people and relationship.
4 Activity, emotion, and no talking
Activity was represented in the current study by illustrations of words, talking and listening. This might align with the Goal domain in the Baker et al. (2018) taxonomy, in particular, the ‘area of focus’, as children could typically describe the words they were working on. This was really the only element of the Goal domain represented in the children's drawings. However, it aligns with the recommendation of Strand (2020) that, ‘For children who have few words, parents (and, at times, the child) should also play a part in choosing stimuli so that the utterances are useful, meaningful, and motivating’ (p. 40).
Finally, some children represented positivity in their drawings, which was captured by the taxonomy as ‘Social/emotional valence – challenging, fun’ (Baker et al., 2018: 915). Most also reflected they were happy when asked questions about their experiences of intervention with the emojis. This corresponds with other research exploring older children's experiences of intervention, many of whom report positive attitudes towards therapy, particularly the activities, games, and rewards (Owen et al., 2004; Van Poucke et al., 2025).
Conversely, Godzilla and Cool Dude did not draw talking/intervention at all, with Cool Dude indicating he drew himself playing football, as it reflected something he really enjoyed. It is interesting to reflect on the extent to which children's enjoyment influences (or could influence) our intervention decision-making. Some parents reported in comments post-interview that SLTs aimed to make intervention fun and engaging for their children, and this was perceived positively by them and their children. Remembering the value of play, as a context for learning and development, and the value of warm and supportive relationships as a driver of good outcomes, we could consider positivity as an element of intervention alongside the necessary processes and procedures.
5 Clinical implications
This study included young children with CAS and a range of methods were used to ensure their voice could be shared (e.g. drawings, recordings, interviews, and emojis). The results showed these methods enabled children to share their experiences of intervention and reinforced the suggestion that using innovative methods can enable us to ‘listen to and understand the perspectives of children and young people with SLCN’ (Lyons et al., 2022: 547). In undertaking this research, we wanted to ensure that the perspectives shared by children were not just heard but were given due weight. In considering the children's drawings and their responses to questions, there are a number of implications for practice. Firstly, there is a reminder that children, even those who are young or experience difficulty with verbal communication, can contribute to our understanding of intervention experiences and clinical practice. Secondly, their frequent inclusion of place and recognition of transitions (to and from intervention and within intervention sessions) might encourage us to reflect on where we undertake intervention and how we prepare and engage children in intervention planning and implementation. Thirdly, their emphasis on people and relationships and possibly limited sense of self might encourage us to think about the therapeutic relationship, and consider how frameworks such as self-determination theory could support our current practices to enable greater intrinsic motivation and autonomy.
6 Limitations
While this study provides valuable insights into children's experiences of intervention, the intervention was being delivered as part of a series of DTTC research studies that required adherence to research protocols for therapeutic intervention. Exploration of the perspectives of SLTs and parents who were engaging in one of these research studies indicated that their experiences of this DTTC intervention was different from their other experiences of intervention, including other experiences of DTTC (Thomas et al., 2025). In particular, their experience of this DTTC intervention was perceived as prioritising adherence to the treatment protocol while other intervention experiences had prioritised flexibility. Thus, it is important not to generalise findings of this study beyond the context in which it was undertaken. Notwithstanding this, the children's drawings of their intervention remain valid representations of their experiences. In contrast to parents and SLTs, for many children, participation in the research was perhaps secondary to participation in the intervention sessions, and so their drawings likely reflected ‘intervention’ not ‘research’.
Children in the current study had undertaken intervention in different settings (private practices, home, clinics, school). Given the focal point of ‘Place’ that was identified in children's drawings, it may be interesting to undertake future research that explored the influence of setting in more detail. Exploring the experiences of children undertaking different types of intervention would also be interesting to see if the focal points illustrated in this study reflected the nature of the DTTC intervention or children's experiences more broadly.
Children completed the initial drawing with their parent at home. While parents were invited to video record their child undertaking the drawing task and responding to questions about the drawing, it is possible that the presence of their parent influenced their responses. Similarly, when they met with the interviewer for phase 2, their responses may have been influenced by the lack of familiarity with her and/or their parent's presence. The interviewer was a highly experienced SLT and engaged in rapport building before asking interview questions; however, children's experience and comfort level talking about their intervention and their feelings about talking may have impacted their ability and motivation to respond.
X Conclusion
Evidence-based practice includes the perspective of the client. Children can reflect on their emotions, thoughts, and feelings – including about speech and language therapy. This study provides further evidence of children's ability to reflect and talk about their emotions as they relate to intervention. Their insights align with the active ingredients of intervention identified in taxonomies of intervention. Most children found intervention to be a positive experience and enjoyed interacting with the therapists – but some provided insights about the transitions to and within intervention, the environment and the time for intervention. This research shows the importance of involving children as an active participant and incorporating their voice in matters concerning their wellbeing, including in speech and language intervention.
Footnotes
Acknowledgments
The research team acknowledges the support of the Once Upon a Time Foundation (OUAT) in the United States who provided funding for this research, as well as the other research teams funded by the OUAT Foundation who provided support for this project in the recruitment of participants. The team acknowledges especially the children and families who participated in this research project and generously shared their time and perspectives.
Author contributions
AC, JM, and SM were chief investigators on the project, co-designed the project, and supported implementation. JM undertook data analysis of the drawings and led the writing of this manuscript. AC and SM undertook analysis and writing for this paper. AC led the implementation of the study, including ethics approval, and some data collection. MI undertook the majority of the data collection with support from CT, who also de-identified and input data into storage systems and provided input into the analysis. C(A)W provided consultation throughout the project and advice in the data analysis.
Data availability statement
The participants in this research did not provide consent for their data to be shared more broadly and so the data is not available for researchers beyond the research team.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sharynne McLeod is a contributing author of this paper and guest editor of the special issue for which it has been submitted.
Ethical approval and informed consent statements
The Human Research Ethics Committee at Australian Catholic University approved this research (approval: 2023-3256H). Parents provided signed written consent for their children to participate and consent was confirmed with them verbally at the commencement of the interview with their child. Children provided assent to participate.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Once Upon a Time Foundation.