
Abstract
Keywords
Background
Communication and language are fundamental features in a child's development and strongly correlate with health, learning, and well-being (McCormack et al., 2018; McLeod, 2018). Language disorders are regarded as a public health problem as they fulfil the criteria of placing a large burden on society, are distributed unfairly, and preventive strategies are available to reduce the burden (Law and Levickis, 2018). The prevalence of these disorders ranges between one and 50%, depending on problem severity, study population, and the measurement used (Locke et al., 2002; Norbury et al., 2016; Reilly et al., 2010). Several factors impact the development of language disorders, wherein some of them are associated with low-income status, low parental education, and mental health problems (McKean et al., 2017). Disadvantaged children are unfairly affected by language disorders as the prevalence is very high in children reared in poverty (Locke et al., 2002).
Research on language interventions is often carried out on children identified through diagnostic procedures, i.e. indicated interventions or treatment. Few studies have been conducted on selective interventions targeting children at risk for language disorders, usually socio-economically disadvantaged children (Law and Pagnamenta, 2017). Studies on universal preventive or promoting strategies targeting parents are sparse (Smith and Gibbard, 2011; Goldfeld et al., 2012; Smith et al., 2017). However, the studies often target literacy skills through book reading interventions, even though research has questioned the strength of the evidence of such interventions for enhancing language and literacy development (Needlman and Silverstein, 2004). Book reading interventions have shown to be less effective on children at risk for language or literacy disorders than children not at risk (Mol et al., 2008).
Furthermore, parents often report difficulties implementing book reading with their children, and parents with reading difficulties commonly drop out of reading interventions (Justice et al., 2015). There are also indications that universal interventions may have a larger positive effect on socio-economically advantaged children than on those who are less socio-economically advantaged (Heywood et al., 2009). Contrary to parent-directed interventions, universal preschool or school interventions have a significant impact on children's language, such as vocabulary. These interventions focus on interactive book reading, adult-child interaction, play-based teaching, and conversation-facilitating approaches (Dobinson and Dockrell, 2021).
Sweden has a child health service (CHS) that reaches almost 99% of children 0–5 years old (Wallby and Hjern, 2011). Through a general programme, comprising 16 visits to the CHS centre (hereinafter centre), the CHS aims to enhance and monitor child health and development through regular growth and developmental assessments, vaccinations, and parental support. The programme is structured in a three-tiered system, with a first tier consisting of universal interventions targeting the whole population. The second tier comprises selective preventive interventions targeting individual children or groups with an increased need or risk of poor health or developmental outcomes. The third tier includes children and families with greater needs, who should be offered an intervention from, for example, speech and language pathologists, psychologists, or the social welfare system (Tell, 2019). During the child's first year, the visits are intensive with a visit every month. Thereafter, they are fewer, including one visit at 18 months, two-and-a-half, three, four, and five years of age.
The allocation of resources to the primary healthcare service is based on the administrative tool Care need index (CNI). The CNI is based on information in official registers about individuals and includes seven demographic factors: low educational level, unemployment, age ≥65 years and living alone, children aged five and younger living in the household, single parents, cultural needs, and having moved to the area during the past year. A higher CNI for a specific area leads to more resources being devoted to the centre (Malmström et al., 1998).
The Kodknäckarna (in English- the Codebreakers) is a non-profit association aiming to reduce the impact of literacy disorders in the Swedish society. They aim to inform about language development and literacy disorders and produce material to be used by parents and teachers. The Codebreakers developed a video guide presenting age-specific examples of language and literacy enhancing activities. The video guide aimed at increasing parents’ awareness of the importance of early language stimulation and enhance the children's opportunities to be engaged in language and literacy enhancing activities. It was available through a website and a digital video disc (DVD), a format chosen purposefully to reach parents with low literacy. Moreover, the video guide and written material were available in six languages. Specifically, the video guide encompassed an introduction for all ages, followed by three chapters for different language development levels. The first chapter was named “From birth to first words”. It included activities labelled as (a) Sing for your child, (b) Giving things names, and (c) Everyday games, recommending the parent to use the everyday activities to stimulate the child's language. Chapter 2 was named “From single words to many”. It included activities such as (a) Nursery rhymes, (b) Playing fetch by naming objects, and (c) What did you do today, where the parent was encouraged to talk about their day as a model for the child. Finally, chapter 3, named “Whole sentences and reasoning”, involved (a) Rhyme games, (b) The child's name a springboard to writing, and (c) Long or short words, which a focus on meta-language. All chapters included information regarding book reading. Additional information was provided on the website, such as a pamphlet with 27 language-enhancing activities listed. The video guide was produced in cooperation with literacy researchers and the central unit of CHS in Uppsala County, Sweden. To reach all parents of children in the target age (0–5 years), the video guide was delivered through the CHS.
No study has previously explored the characteristics of families who received the video guide or any potential differences in the distribution of the video guide between different centres.
Aims
The study aimed to explore which specific socio-demographic characteristics of the family and centre were associated with parents who reported receiving the video guide through the CHS in Uppsala Municipality, Sweden. We also aimed to explore the proportion of parents who had watched the video guide and tried any of the activities presented in the guide.
The following research questions were addressed:
Which socio-demographic characteristics of the family and the centre were associated with parents who reported receiving the video guide?
To what extent did parents report having watched the video guide and trying any of the activities presented?
Methods
Intervention delivery procedure
Three services were involved in implementing and delivering the video guide: The Codebreakers, the CHS's central unit, and the CHS nurses. The Codebreakers produced the video guide and provided the guide through a website and a DVD. Thereafter, the DVD was delivered in an envelope with brief information and a link to the video guide website to accommodate those without a DVD player. Moreover, the Codebreakers hosted a one-time volunteer group meeting and were interviewed in a newspaper article published in the major local newspaper in May 2014 (Sandow, 2014). In August 2014, the Codebreakers delivered the video guide on a DVD to all centres in Uppsala Municipality.
The CHS's central unit informed the CHS nurses about the video guide during one visit to the centre, repeated e-mails, and through written information on a monthly basis. The CHS nurses were instructed to give the video guide to every family whose child, three months to five years of age, visited the centre. Nurses were also encouraged to show the video guide in parent groups during the child´s first year and, when there was an indication of an increased need for parental support, during individual visits. After feedback from the CHS nurses, indicating that few parents owned a DVD player and therefore declined the offer, the Codebreakers also produced an information card with the link to the video guide website. This information card was to be given to parents who declined the DVD.
Data collection procedure
To answer the research questions, we used a sub-sample of self-reported cross-sectional data from the Children and Parents in Focus study (Salari et al., 2013). Our sub-sample consisted of questionnaires from parents of three-year-olds collected from autumn of 2014 and onwards. The rationales for choosing this sub-sample were that the target group for the intervention primarily was children up to three years of age and that the video guide was offered during autumn 2014 and onwards.
Data were collected at 21 child health centres. CHS nurses consecutively recruited parents before their child's annual health check-up. The CHS nurses included the questionnaire, together with the invitation letter, which was routinely sent home to each child about three weeks before their annual visit. Questions related to the parents’ socio-demographic background and whether they received the video guide, watched the video guide, or tried any of the presented activities (appendix). Both parents of each child were requested to fill in one questionnaire and bring them to the visit.
Written consent was collected from both parents. The regional ethical review board had granted ethical approval of the study.
Participants
Of all three-year-olds in the Children and Parents in Focus study, recruited between 2013 and 2017, (n = 3590) (Dahlberg et al., 2020), our sub-sample consisted of parents of 2873 children recruited from autumn of 2014 and onwards (2466 mothers and 2209 fathers). Data were missing in 735 questionnaires; hence, these were excluded, leaving families of 2512 children in the analysis.
Measures and variables
In the Children and Parents in Focus study questionnaires, information about socio-demographic background was collected from both parents, including country of birth (Sweden or other), marital status (married/cohabiting, single, living apart, or other), and level of education. Additionally, the child's age when the video guide was initially offered within the CHS as well as the child's birth order were calculated.
The level of parental education was dichotomised into university education (college/university less than or more than three years) versus lower education (all other). The child's birth order was dichotomised into two variables: (1) the child being the youngest among siblings versus the child having younger siblings/being the only child, or having both younger and older siblings and (2) if the child was the oldest among siblings versus the child having older siblings, was the only child, or had both younger and older siblings.
The main dependent variable of interest was whether the mother or father reported receiving the video guide (yes/no). Whether the parents watched the video guide was dichotomised into yes (yes, at the CHC; yes, at the municipalities open playgroup activities; and yes, at home) and no. Responses regarding if the parents had tried any of the activities presented in the video guide (yes/no) and if the parents had watched the video guide were presented descriptively.
Data pertaining to the centre were collected from the central unit for CHS and were analysed regarding size (total number of enlisted children, range 143–1717) and CNI (range 0.70–1.77) as continuous variables.
Statistical analyses
The analyses were conducted using IBM SPSS for Statistics (Version 26. IBM Corp., NY, USA). Descriptive statistics, including means, standard deviations, ranges, frequencies, and proportions, were used for descriptive purposes.
The relation between family and centre characteristics and if the parents had received the video guide was analysed using multi-level Binomial Generalised Linear Mixed Models (GLMM), with mothers and fathers analysed separately. In these models, the parental socio-demographic variables, child's age when the video guide was initially offered within the CHS, birth order, size of centre, and CNI of the centre were entered as independent variables. Furthermore, a dichotomous yes or no variable for reporting having received the video guide was entered as a dependent variable. A cluster design was used based on the centre variables, and the variable for parental education was analysed with a random effect on the centre. The centre intercept term was used to account for the dependence between children at the same centre. Finally, a logistic regression model was computed to explore the relation between parents’ characteristics and having watched the video guide. P-values, along with Odds Ratios (OR) and 95% Confidence Intervals (CI), were reported from the models. P-values of ≤ 0.05 were used to define statistical significance.
Results
Of the total sample (n = 2512), most parents lived in a two-parent household, were born in Sweden, and had a university education (Table 1).
Descriptive statistics of parents and centres.
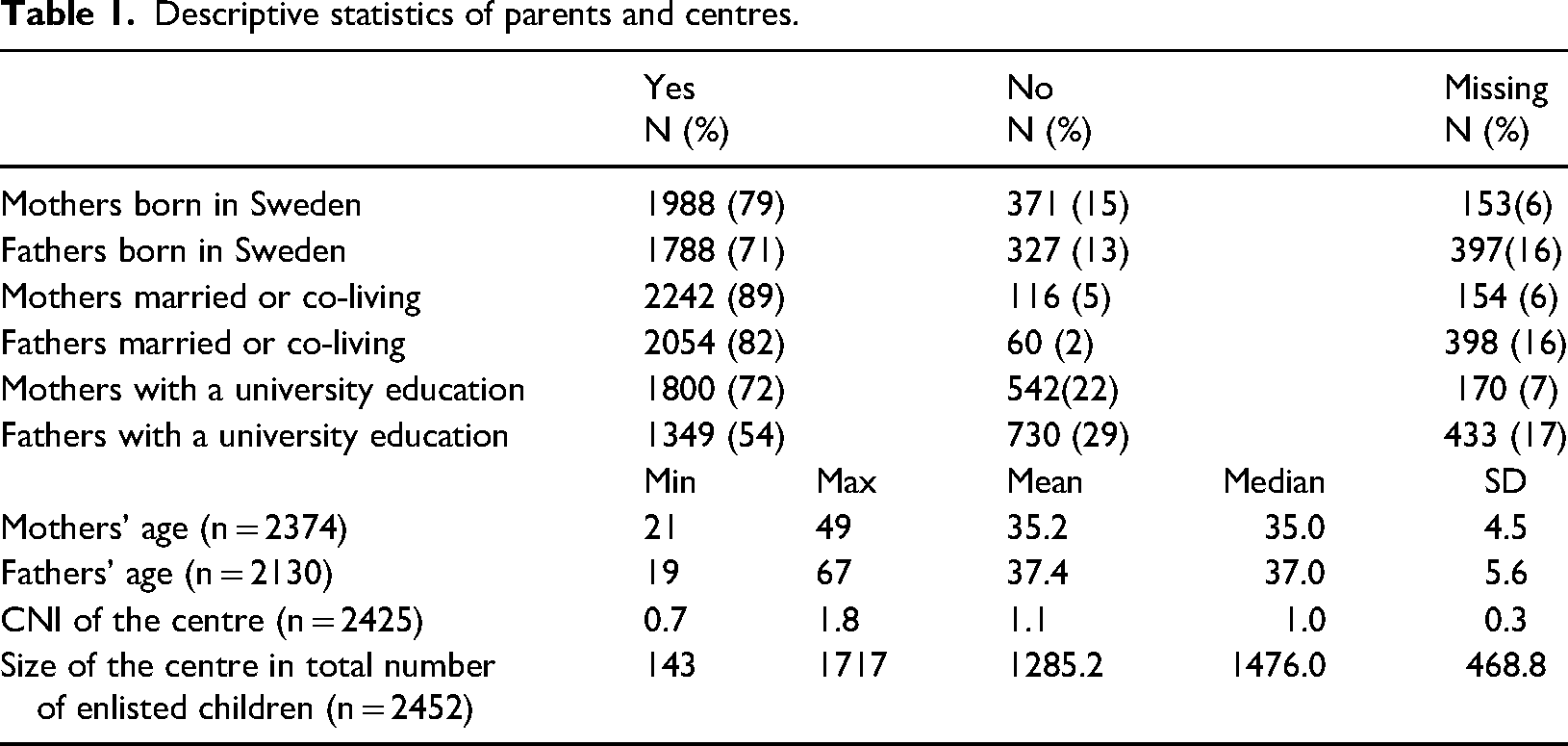
Descriptive statistics of parents and centres.
In families of 1518 children (60%), none of the parents reported having received the video guide (Table 2). Both parents reported having received the video guide in 525 families (21%). In 2099 families (84%), none of the parents reported having watched the video guide. Both parents reported having watched the video guide in 121 families (5%). A few parents reported having watched the video guide without receiving it (4 both parents, 21 mothers and three fathers). When excluding parents who did not receive the video guide, 61% families reported that none of the parents watched the video guide. In 2178 families (87%), none of the parents reported having tried any of the activities from the video guide. Out of the families who reported having watched the video guide, a total of 71% reported that one or both parents had tried an activity or activities presented in the video guide
Number and proportions of parents who received the video guide, watched the video guide, and tried any activity.
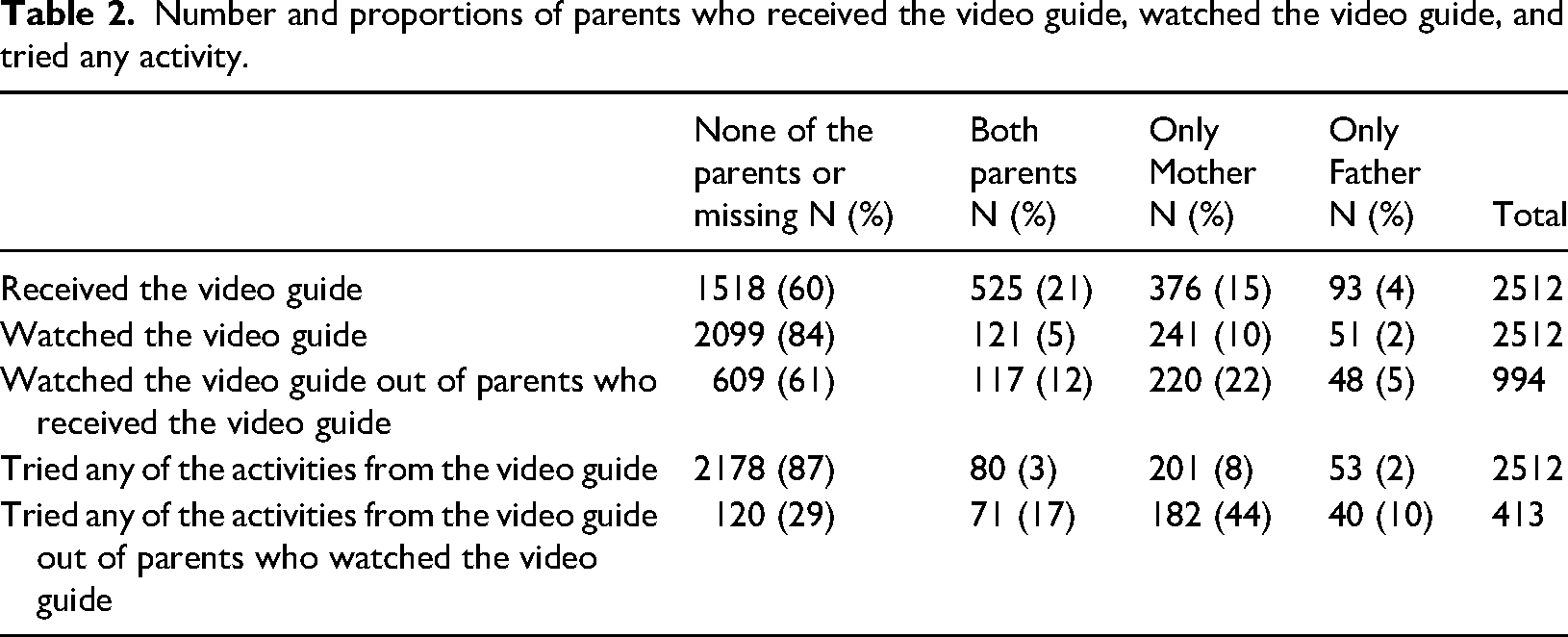
Number and proportions of parents who received the video guide, watched the video guide, and tried any activity.
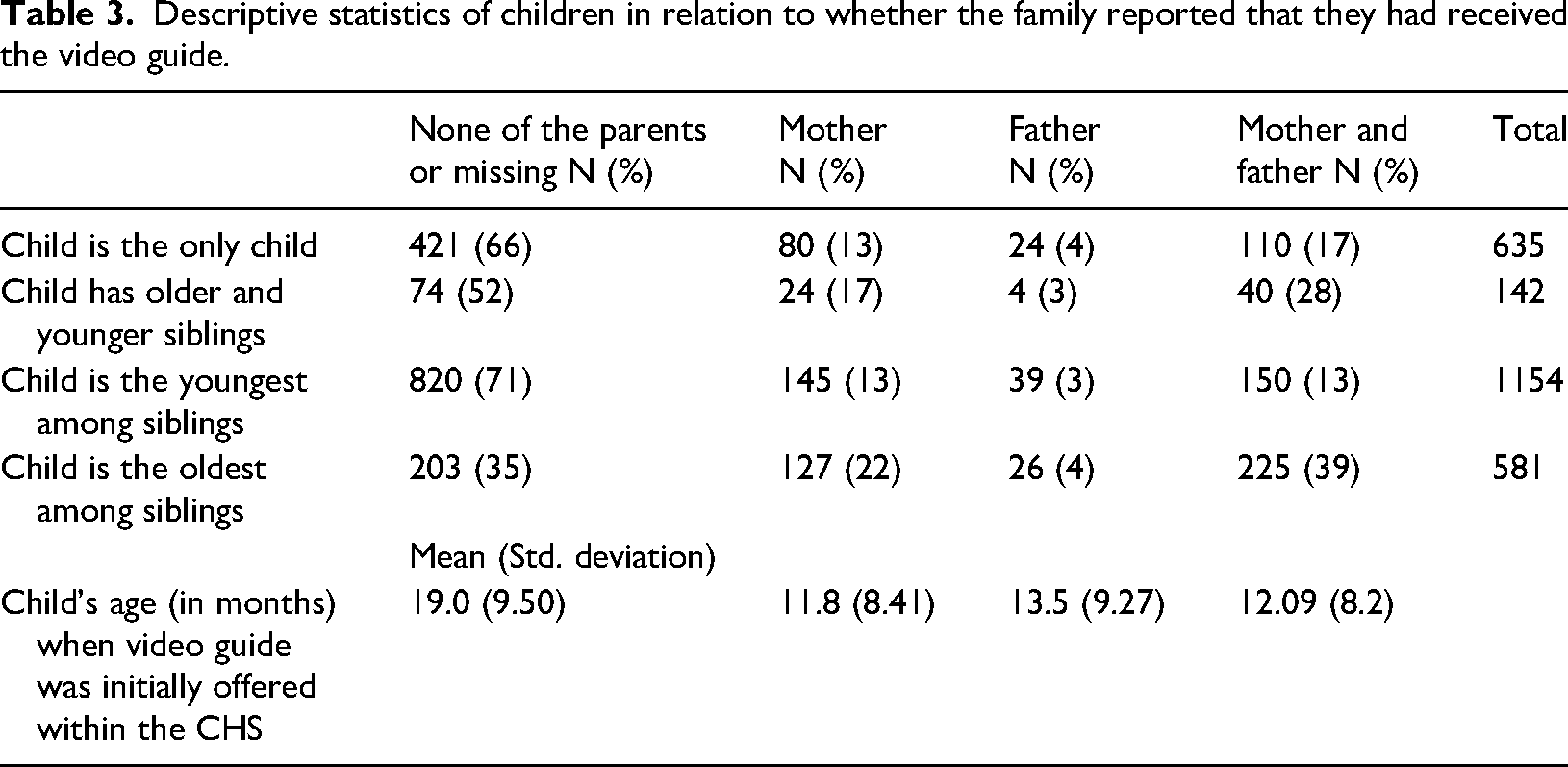
When the video was initially offered within the CHS, the children's age ranged between one and 36 months. Most children were the youngest among siblings, followed by children who were the only child in the family (Table 3).
Descriptive statistics of children in relation to whether the family reported that they had received the video guide.
The odds of parents who reported having received the video guide were not associated with the size or CNI of the centre (Table 4). The centre was not affected by the covariance with the parent's education level.
Results of the generalised linear mixed model (GLMM) analyses of family and child health centre characteristics associated with parents who reported having received the video guide.
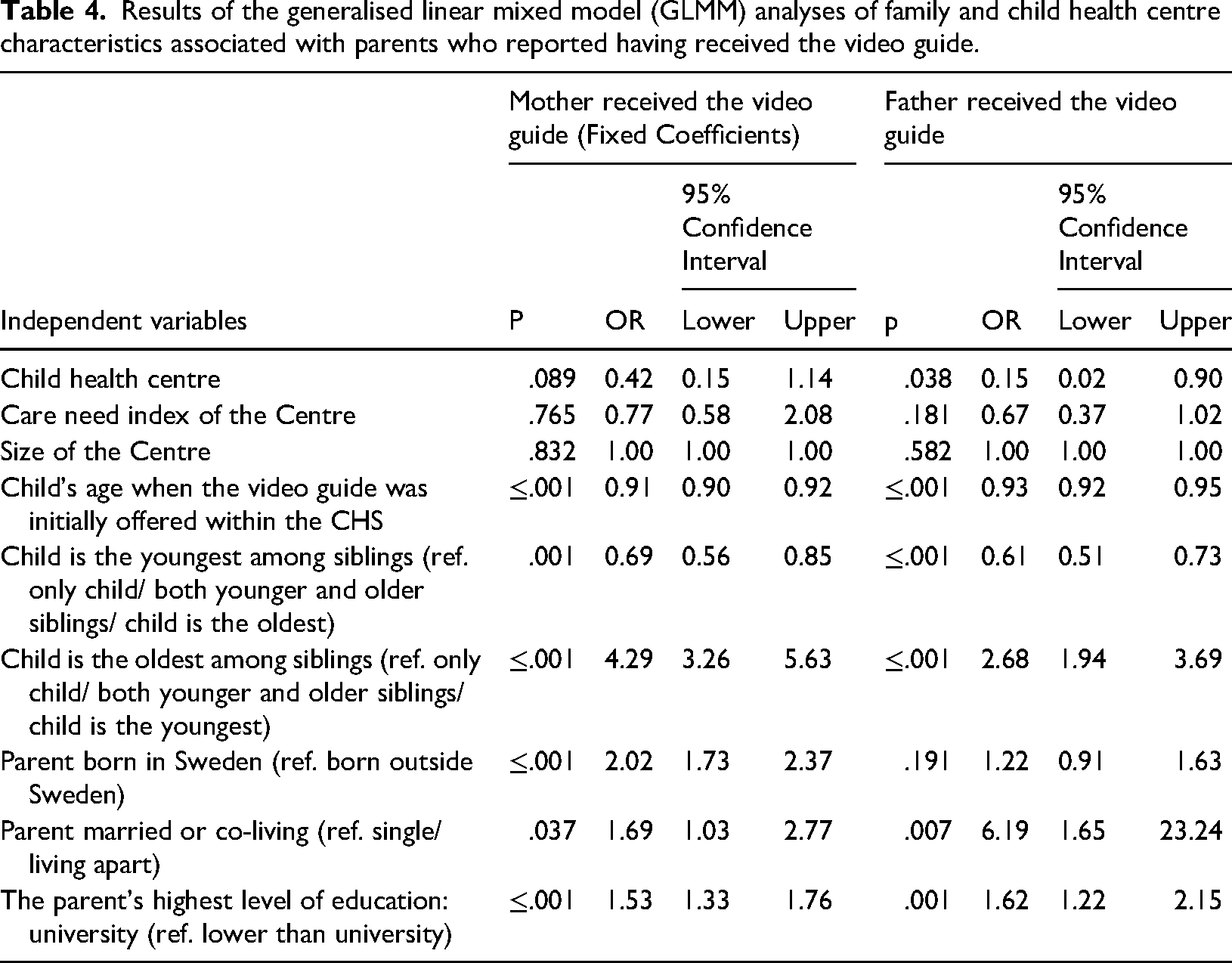
Results of the generalised linear mixed model (GLMM) analyses of family and child health centre characteristics associated with parents who reported having received the video guide.
Receiving the video guide was associated with younger age of the child when the video guide was initially offered within the CHS, the child's birth order, married and co-living marital status, parents having attended university, mothers born in Sweden, and the centre for the fathers. The GLMMs showed an overall explained variance of 73% for the model, including data on mothers and 74% for the model, including data on fathers, respectively.
A descriptive analysis of parents’ characteristics in those reporting they received the video guide showed that 112 (13%) of the mothers and 82 (13%) of the fathers were not born in Sweden. Very few parents were single: 26 (3%) of the mothers and 5 (1%) fathers. Few parents had an education level lower than university: 280 (20%) of the mothers and 167 (28%) of the fathers. When exploring the relation between the same characteristics and having watched the video guide, no significant differences were found regarding the parent's education level or if the parent was born in Sweden. Marital status was excluded because a few of the parents were single.
This study aimed to explore specific family and centre characteristics in relation to parents who reported having received a universal language and literacy promoting intervention in the format of a video guide delivered through the Swedish CHS.
Regarding the family characteristics, age of the child when the video guide was initially offered within the CHS and birth order were associated with having received the video guide. More specifically, families in which the child was the oldest were over four times more likely to have received the video guide as reported by mothers than families where the child was youngest, had no siblings, or had both younger and older siblings. Additionally, the odds of receiving the video guide were significantly lower in families where the child was the youngest. One possible explanation for this is that in families where the child was the oldest, it was likely that the family visited the CHS with the younger sibling/s. The video guide could have been repeatedly presented to the families during these visits, which potentially increased the exposure to the video guide. In contrast, families where the child only had older siblings could mean that there were fewer visits to the CHS, resulting in fewer possible presentations of the video guide. Furthermore, the positive association between the child's young age when the video guide was initially offered through the CHS and receiving the video guide could also be explained as resulting from exposure. The child could have had more visits to the CHS during the time period when the video guide was offered; thereby, the video guide could have been presented to the child on several occasions. Our results suggest that the number of possible times the video guide was presented, i.e. exposure, influences the impact of the video guide, as shown in previous research (Boles et al., 2014).
Another explanation for the age association could be that the CHS did not initially, i.e. during autumn of 2014, provide the video guide to the parents. Implementing new methods in health care settings is a time-consuming process, which might result in a delay in delivery. This delay could have been even more substantial, as no specific implementation strategy was used when the video guide was delivered. When implementing interventions, it is crucial to investigate the nature of the evidence of the method implemented, the context in which the change is proposed, and the mechanism for facilitation (Kitson and Harvey, 2016). None of these aspects had been investigated beforehand. The only facilitation strategy used was delivery of the DVDs to the CHCs and information delivered in one group meeting, at one visit to the CHC, and through written material on a monthly basis. The lack of implementation strategies and usage of only a few facilitation strategies could have prolonged and hindered the implementation of the video guide.
Despite the aim to include a diverse population, the participating parents were predominately born in Sweden, cohabiting, and highly educated (Fält et al., 2018). In previous studies, CHS nurses report difficulties interacting with foreign-born parents due to language barriers and lack of cultural competence (Berlin et al., 2006). Also, foreign-born parents do not receive the same interventions as Swedish born parents even when the material is translated into several languages (Carlsson et al., 2013). The video guide was translated into several languages in the current study. Still, it was not received by foreign-born parents to the same extent as Swedish-born parents. This is also reflected in the analysis of our sub-sample, where mothers born in Sweden had higher odds of receiving the video guide than mothers born outside Sweden.
Moreover, co-living or married and university education were factors associated with receiving the video guide. No significant differences were found between parents with high and low education or between native-born and foreign-born parents regarding watching the video. One explanation for this is that few parents born outside of Sweden or without a university education reported that they received the video guide. These results may be interpreted as the video guide reached children of more socio-economically advantaged families, which aligns with findings on universal intervention programmes targeting language disorder (Mol et al., 2008). Few studies in this research field include individuals from low socio-economic backgrounds (Heinrichs et al., 2005; Justice et al., 2015). Therefore, evidence-based advice may be less appropriate for parents with lower socio-economic backgrounds (Lingwood et al., 2020). This lack of research-based recommendations targeting low socio-economics parents needs to be considered when designing future interventions and studies. From the results, it can be interpreted that there are flaws in the three-tiered system in the CHS (Tell, 2019), as not all parents received the video guide, which was planned to be offered universally.
Overall, the exposure to the video guide seems to be limited, as few mothers and fathers in this specific sample reported that they had received the video guide. Out of these, only 37% of the mothers and 26% of the fathers had watched the video guide. Using a DVD format as the primary delivery method could explain the poor reach of the video guide. Specifically, it may have been too demanding for parents to access and use a DVD player to watch the video; a DVD could have been viewed as outdated. Other digital solutions, such as Quick Response (QR) codes or links, could increase the chances of parents watching a video guide, as the practical requirements would be more straightforward. The fact that a larger proportion of parents who watched the video guide tried an activity shows that the content of the video guide can be deemed appropriate for the target group.
The study was based on cross-sectional data. Thus, any conclusions about causality cannot be drawn from this study. Furthermore, the data were collected through recalled self-reports by the parents, which might have led to biased responses. For several of the questions, there were missing data. Parents reported receiving, watching the video guide, or trying any of the activities presented; the missing data were more extensive for the two last questions. Parents who had not received the video guide most likely chose not to respond to whether they had seen it or tried any of its activities. The missing data could, therefore, be treated as non-responses to these two questions.
It appears that the implementation of the video guide could be improved to reach a more significant number of parents overall, particularly parents with a low socio-economic status. A wider outreach of the video guide could lead to higher quality and quantity of language input for young children, which, in turn, could reduce language and literacy disorders in this population.
Conclusions
A low proportion of parents of three-year-old children reported being exposed to a universal promotion of language and literacy development. Only a few parents reported that they received the video guide, and even fewer watched the video guide or tried any of the presented activities. The results indicate that the video guide reached socio-economically advantaged children to a higher extent.
Supplemental Material
sj-docx-1-clt-10.1177_02656590221119923 - Supplemental material for Family and child health centre characteristics associated with exposure to universal language and literacy promotion
Supplemental material, sj-docx-1-clt-10.1177_02656590221119923 for Family and child health centre characteristics associated with exposure to universal language and literacy promotion by AE Fäldt, N Durbeej and HM Fabian in Child Language Teaching and Therapy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.