
Abstract
This article summarizes the evidence as regards the effectiveness of therapy for grammar for school-aged children with language impairments. I first review studies focusing on specific areas of grammar (both expressive and receptive targets) and then studies aiming to improve language more generally, several of which focus more on the effectiveness of different methods of delivery. I conclude that while there is a growing body of evidence in this area, there are still many gaps. The most concerning gap is the small amount of evidence of effectiveness of intervention for children with receptive as well as expressive language impairments. The evidence to date seems to indicate that these children need specialist, intensive help in order to make progress with their language. Further research is also needed to consider the relative impact of different types of interventions (or their combination) on children of different ages and with different language profiles, including establishing the most effective and/or cost-effective methods of delivery of these interventions.
I Introduction
Children with language impairments often have difficulties in many areas of language, but grammar is particularly affected. These children often produce short, simple sentences containing grammatical errors and have difficulties understanding longer and more complex sentences. Language difficulties which are still present by school entry are likely to persist (Stothard et al., 1998), especially if children have receptive as well as expressive language difficulties (Clark et al., 2007). Such difficulties are likely to affect their ability to do well at school (Nippold, 2010) and hence their employment prospects (e.g. Law et al., 2009). Thus, there is a need to establish the best ways to help school-aged children with language impairments improve their language abilities and hence their educational and life prospects. Improving their use and understanding of grammar is likely to be one aspect of this.
This review concentrates on intervention studies that aim to improve understanding and use of grammar in school-aged children (over five years) with language impairments. Some studies investigate improvements in general language abilities (of which grammar is a major part) but do not specifically consider grammar. These may use a specific approach (e.g. Fast ForWord, Scientific Learning Corporation, 1998) or a therapy package containing many different elements. The outcome measures of these studies are usually quite general, although some measures more closely related to the intervention itself may also be included. I will consider these studies after examining those that use more specific intervention methods and outcome measures related to grammar.
The majority of published language intervention studies indicate that intervention is generally successful, regardless of the targets or methods used. However, a few important exceptions exist; these are often the studies with more rigorous designs. Many gaps in the evidence persist, where relatively little has been published; this is particularly the case for receptive language. Indeed, previous reviews of the effectiveness of therapy for children with language impairments have concluded that ‘the most substantial single gap in the literature … is the lack of good-quality literature about intervention for children with severe receptive language difficulties’ (Law et al., 2004) and that there is ‘an overall lack of evidence for approaches to effective treatment for children with RELI [receptive and expressive language impairment]’ (Boyle et al., 2010).
II Important variables in intervention studies
The ultimate goal of intervention research is to establish which method is the most effective, for which areas of language, for which children, using which method of delivery. The most important variables within the children are likely to be: age, severity and pervasiveness of language difficulties and any co-occurring difficulties. When considering different methods of delivery, the variables include: who or what delivers the therapy – e.g. speech and language therapist (SLT), SLT assistant, teaching assistant (TA), teacher, parent, computer – and whether the therapy is delivered 1:1 (one-to-one) or with other children. If the therapy is delivered with other children: how many others (e.g. in a pair, small group, large group) and who are the other children (in terms of age, diagnosis, etc)? The duration and distribution of therapy are also important variables as, of course, is the precise nature of the therapy itself.
When appraising a particular study, it is important first to consider the research design. Some designs are much more robust than others, and this depends on the degree of experimental control provided by the study and hence how many other possible factors can be ruled out. For further discussion of these factors see Ebbels (2008: 150–52).
Practitioners are aided in their appraisal of the evidence by searchable websites, which rate articles or interventions according to the strength of their research design and hence the reliability of their findings. The SpeechBITE website http://www.speechbite.com (accessed September 2013) has the facility to search for published articles on all areas of speech and language therapy. The resulting studies are listed in order of the strength of their design, although single case experimental designs have not yet been rated. The recently launched What Works website https://www.thecommunicationtrust.org.uk/whatworks (accessed September 2013), hosted by the Communication Trust complements the SpeechBITE website as it allows searches for particular intervention methods or packages. The evidence for each is reviewed and rated as strong, moderate or indicative.
Another factor to consider when evaluating intervention studies is how specific or general the outcome measures are and how closely related they are to the intervention. The effectiveness of an intervention is also indicated by whether positive effects are maintained after intervention ceases and whether they generalize to similar linguistic targets and to spontaneous use and comprehension of language in a range of settings.
In this review, I start by considering studies specifically focused on grammar and review the evidence for different methods of intervention. Tables 1–3 show the key features of all the studies discussed; I therefore leave out many of these details from my discussion as the information can be found in the tables. The studies are grouped into tables by target area and sorted within each table according to the level of experimental control. This is so that practitioners wishing to focus on a particular area of language can quickly find the evidence relating to that area. More confidence can be placed in studies higher up the tables due to their stronger designs. Table 1 includes studies focusing on specific expressive language targets, and Table 2 includes studies focusing on specific receptive language targets. The studies in Table 3 also focus on expressive language, but not on specific targets. The tables do not include studies teaching artificial rules or novel linguistic forms. Following this, I review studies with more general language outcome measures that would be influenced by changes in grammatical ability, but include other areas of language.
Studies targeting specific expressive language targets.

Notes. At number of participants, t = treated and c = control; 1:1 = one-to-one; ASD = autistic spectrum disorder; RAPT = Renfrew Action Picture Test (Renfrew, 2003); RCT = randomized controlled trial; RELI = Receptive and Expressive Language Impairment; SLI = specific language impairment; SLT = speech and language therapist; TA = teaching assistant.
Studies targeting specific receptive language targets.

Notes. See notes at Table 1.
Studies targeting improvements in expressive language (not target specific).

Notes. See notes at Table 1; CLI = contextualized, literature-based narrative intervention; DLI = decontextualized language intervention; MLU = mean length of utterance.
III Intervention approaches aimed specifically at grammar
Two main approaches to improving grammar in school-aged children with language impairments have been studied: grammar facilitation and meta-linguistic methods. Grammar facilitation approaches are predominantly implicit and meta-linguistic approaches predominantly explicit (and usually involve visual support). In practice, a mixture of explicit and implicit approaches may be used, and the balance between the two may change as the child moves through therapy. Some studies have examined the effectiveness of primarily implicit or explicit approaches, and some involve a combination. A few aim to compare the relative effectiveness of these two methods.
1 Implicit approaches
a Grammar facilitation methods
Grammar facilitation methods are the most widely investigated in intervention research studies. These aim to make target forms more frequent, which is hypothesized to help the child identify grammatical rules and give the child practice at producing forms they tend to omit. The studies are mostly with pre-school or early school-aged children, many of whom have expressive language difficulties only. Indeed, the focus of grammar facilitation methods is on improving expressive language; receptive language is rarely mentioned. The most common grammar facilitation approaches are: imitation, modelling or focused stimulation, and recasting.
(i) Imitation
Imitation approaches usually involve the adult providing a non-verbal stimulus (e.g. a picture) and a target form, which the child then imitates, receiving reinforcement for correct productions. The adult model and reinforcements are gradually reduced until the child produces the target in response to the non-verbal stimulus only. Two early randomized control trials (RCTs) showed that imitation approaches can be effective for improving production of syntax in general (Matheny and Panagos, 1978) and yes/no questions in particular (Mulac and Tomlinson, 1977). However, in the latter study, progress only generalized to other settings for those children who received additional sessions with the clinician and parent, where the target form was elicited in the context of conversation and stories.
(ii) Modelling / focused stimulation with or without evoked production
In modelling and focused stimulation approaches, the child is not required to respond, merely to listen to examples of the target structure. Modelling approaches direct the child’s attention to the stimuli but do not give explicit guidance on which particular features to attend to. Focused stimulation, in contrast, does not direct the child’s attention to the model in any way. Evoked production may follow the modelling or focused stimulation period. In this case, the child produces a novel utterance that uses the same rule as the model and then receives feedback. The degree of modelling is gradually reduced as the child begins to use the new rule productively.
One study showed that modelling without evoked production was effective in teaching auxiliary is and auxiliary inversion to three children with expressive language delays, but the addition of evoked production led to a more stable learning pattern (Ellis-Weismer and Murray-Branch, 1989). However, neither method was successful in teaching he to a fourth child with both expressive and receptive language difficulties.
Two studies found modelling with evoked production improved the ability of an experimental group to produce is and don’t (Leonard, 1975) and wh-questions accurately (Wilcox and Leonard, 1978). The delayed therapy groups made no progress until they too received therapy. The latter study showed generalization of is inversion to other wh-constructions requiring inversion.
Courtwright and Courtwright (1976) compared the effectiveness of modelling vs. imitation methods for teaching correct use of they in subject position (as opposed to them). The children in both groups improved on their initial performance, but those in the modelling group showed greater progress. They found a similar advantage for modelling when teaching children to produce an artificial grammatical rule (Courtwright and Courtwright, 1979). However, two studies (Connell, 1987; Connell and Stone, 1992) showed that modelling alone seemed to be less effective for teaching novel derivational morphemes to children with Specific Language Impairment (SLI) than just imitation or modelling plus imitation, particularly if they were required to produce the new form. The differing results of these studies may be due to the nature of the invented rules, which for the Connell studies involved derivational morphology, but for the Courtwright and Courtwright (1979) study involved a novel sentence structure.
(iii) Recasting
Recasting methods are designed to be non-intrusive conversational procedures. The adult does not initiate teaching directly, but manipulates play activities to increase the chances of the child using targeted grammatical forms. When the child fails to use the target form or makes an error, the adult immediately follows his or her utterance with a modified version that includes the target form (a ‘recast’). The theory behind this approach is that the child is more likely to be interested in what the adult is saying if it links semantically to the situation and the child’s own prior utterance. The immediate contrast between the two forms should also focus the child’s attention on the features of the utterances that differ. In addition, the child does not need to parse the adult’s meaning and thus should have more processing resources available for analysing the target form in the recast.
Three studies compared the effectiveness of recasting vs. imitation for increasing production of a range of morphosyntactic structures in children with SLI (Camarata and Nelson, 1992; Camarata et al., 1994; Nelson et al., 1996). These found targets treated with either type of intervention improved more than untreated targets, but Camarata et al. (1994) found target forms occurred spontaneously after fewer presentations using recasting than imitation. In contrast, imitation led to faster elicited production of the target. However, there is evidence of an interaction of target type, child and intervention method. Camarata and Nelson (1992) found that children acquired the passive construction faster with recasting, whereas they acquired the gerund faster with imitation. Individual variation was revealed in Camarata et al. (1994) when three of the 21 participants only acquired targets with imitation and three only with recasting.
More recent studies have begun to unpack the necessary features for recasting approaches to be effective. This includes: the density of recasts, the similarity of the recast to the original sentence, whether they serve a corrective function, and whether the child’s initial levels of use of the target matter. I discuss these studies below as they have clinical implications for recasting therapy, but they do not appear in the tables because they are either with pre-schoolers, or use novel linguistic forms or are not intervention studies.
The original studies demonstrating the efficacy of recasting by Camarata, Nelson and colleagues (discussed above) used recast rates of between 0.7 and 1.8 recasts per minute. Subsequent studies have shown that lower levels (0.47; Proctor-Williams and Fey, 2007) and conversation-like densities (Proctor-Williams et al., 2001) do not seem to benefit children with SLI (unlike typically developing children). Another study (Fey and Loeb, 2002) with recasting densities similar to the original studies (one per minute) found no effect of recasting on the ability of 3-year-old children with SLI to produce auxiliaries or modals. They suggested the children may not have been ready to benefit from recasts and that recasting may be best when the children are already using the target form to a certain extent rather than for encouraging use of a new form. Indeed, Saxton (2000) showed that typically developing children need to use a grammatical form above 50% of the times required before they can benefit from corrective recasts. It appears that recasts do not necessarily need to be corrective. Hassink and Leonard (2010) found that conversationally relevant recasts containing a new form were facilitative for pre-schoolers with SLI even when the recasts served no direct corrective function.
Thus, it seems that for recasting to be maximally effective, the recasts need to be of high density and the children need to already use the target to a certain extent. It does not seem to matter whether or not the recast corrects an error.
(iv) Combined grammar facilitation approaches
Some intervention studies have used a combination of the methods discussed above. In particular, modelling with evoked production together with recasting has been shown to be effective for generalization of newly learned grammatical rules to spontaneous discourse (Culatta and Horn, 1982) and for increasing grammatical accuracy and range (Fey et al., 1993; 1997; Gillam et al., 2012; Tyler et al., 2002). The studies by Fey and colleagues also investigated the role of parents in the delivery of intervention. These revealed a significant effect of intervention, whether delivered by parent or clinician, although the children in the clinician groups made more reliable progress.
A series of studies by Tyler and colleagues investigated the effectiveness of grammar facilitation (and phonological therapy) approaches with children with both language and phonological impairments. An early study (Tyler and Watterson, 1991) found no significant effect of grammar facilitation therapy on the mean length of utterance (MLU) of these children. However, two later studies (Tyler et al., 2002, 2003) showed that children receiving a block of grammar facilitation therapy focused on morphosyntax, improved their production of finite morphemes (and indeed their phonology) more than a control group who received no therapy. Tyler et al. (2002) additionally showed that the amount of progress in finite morphemes was the same regardless of whether the children received morphosyntactic therapy before or after phonological therapy. However, Tyler et al. (2003) showed that the largest gains were found in children receiving therapy that alternated weekly between a focus on phonology and morphosyntax. The children were assigned randomly to groups, thus there was no consideration of the extent to which each child’s morphological difficulties were due to phonological factors. This may have contributed to the highly variable responses to therapy in this study.
Indeed, a study including both implicit and explicit therapy (Smith-Lock et al., 2013a, discussed below) found that children whose articulation difficulties interfered with production of targeted grammatical constructions made no progress with grammatical therapy. A single case study (Seeff-Gabriel et al., 2012) considered the impact of phonology on the targeted morphosyntactic structures and varied the therapy accordingly. Phonology was not considered to affect his production of past tense and, indeed, grammatical therapy (mostly using grammar facilitation methods) improved his production of the regular past tense. However, phonology was considered to affect his production of plurals, as he could not accurately produce /s/ or /z/. In this case, phonological therapy led to increased marking of plurals.
A recent study (Gillam et al., 2012) found combined grammar facilitation approaches were more effective when embedded in a story context than when presented in a decontextualized way. However, a large scale RCT (Gillam et al., 2008; see Table 5 for details) compared grammar facilitation approaches with two other interventions: Fast ForWord (reviewed below) and computer-based language games and also with a control intervention: ‘academic enrichment’ (computer games focusing on Maths, Science and Geography). They found no significant advantage for any group. Indeed, the language intervention groups only showed greater progress than the ‘academic enrichment’ group on blending words. Thus, the grammar facilitation group fared no better on language measures than the other groups, including the ‘control’ academic enrichment group.
b Usage-based approach
Riches (2013) evaluated an alternative implicit approach (a usage-based approach; e.g. Tomasello, 2003), which takes into account the gradual development of grammatical structures in typically developing children. Riches evaluated this approach with reference to passives. The intervention gradually built up to a full event passive, starting with state passives (e.g. I like my sausages chopped) which could be interpreted as an adjective, via ambiguous passives (e.g. I want my sausages chopped) to event passives (e.g. the sausages were chopped by the cat). He found that two children with receptive and expressive SLI significantly improved their comprehension and production of passives, but not the control structure (relative clauses).
c Summary of implicit approaches
The effectiveness of implicit methods has been investigated in a range of studies including some RCTs. These generally indicate that these methods are effective for improving expressive morphology and syntax in pre-school and early school-aged children with expressive language delays and disorders when delivered 1:1 by an SLT or parent. However, the study by Gillam et al. (2008) indicates that this may be no more effective than ‘academic enrichment’. For children with co-occurring phonological impairments, the impact of these on specific grammatical targets should be considered, as should delivering an alternating phonological and grammatical approach.
2 Explicit approaches
Meta-linguistic approaches provide predominantly explicit teaching of language, often in the context of specific visual cues. Once the child has learned a new rule, some grammar facilitation methods (especially recasting) may be used alongside visual templates and explicit references to the child’s errors, and more context may begin to be added. These approaches are based on the hypotheses that children with primary language impairments have difficulties learning grammar implicitly and benefit from explicit teaching of the rules (for further discussion, see Ebbels et al., 2013).
a Colourful semantics
Colour coding is frequently used in meta-linguistic approaches. Colourful Semantics (Bryan, 1997) colour codes thematic roles in sentences in order to help children identify thematic roles and create a variety of argument structures. Several uncontrolled case studies have been carried out using this or similar methods (Bryan, 1997; Guendouzi, 2003; Spooner, 2002). Also, a group study (Bolderson et al., 2011) found improved expressive language after therapy, compared with no progress during a baseline period. Progress on receptive language was seen both during baseline and the therapy period and thus the changes could be due to maturation or practice at the tests.
b Shape coding
A related meta-linguistic approach (Shape Coding, Ebbels, 2007) uses a combination of shapes, colours and arrows to indicate phrases, parts of speech and morphology respectively. It was originally conceived as a combination of the ‘Colour Pattern Scheme’ (Lea, 1970) and ‘Colourful Semantics’ systems, but was further developed so that it can also show complex sentence structures and verb morphology. Each shape is linked to a question word and colour.
An RCT (Ebbels et al., 2007) investigated production of verb argument structure and compared therapy using Shape Coding with therapy focusing on verb semantic representations and a control therapy (focused on inferencing, which was not predicted to have any effect on verb argument structure). Both the Shape Coding and verb semantic methods were based on detailed hypotheses regarding the underlying reasons for the participants’ difficulties with verb argument structure and both groups made significant progress, particularly in linking arguments to the correct syntactic positions (i.e. reducing errors such as ‘she is filling the water into the glass’). Progress generalized to control verbs and was maintained three months after intervention ceased. The Shape Coding group also used more optional arguments after therapy. The control group showed no progress in verb argument structure.
A second RCT (Ebbels et al., 2013) focused on comprehension of coordinating conjunctions (but not, neither nor, not only but also). We found that those receiving Shape Coding therapy improved their comprehension of the targeted conjunctions significantly more than the waiting controls, who then also made progress when they too received therapy. Progress also led to increased scores on the Test of Reception of Grammar (TROG-2, Bishop, 2003). However, we found no generalization to comprehension of passives. Analyses of child-related factors showed no predictors of which children would improve the most with the therapy. The predictors considered including non-verbal and visual processing abilities, which while correlated with each other, were not correlated with any language measure or progress with therapy.
Ebbels and van der Lely (2001) investigated the efficacy of Shape Coding for improving expression and comprehension of passives and wh-questions. Three of the four participants showed significant progress in both their comprehension and production of passives. Two had difficulties comprehending wh-questions pre-therapy and both showed significant progress in this area. All four participants showed short-term progress with the production of wh-questions, but only one participant maintained this at a significant level by follow-up. The three participants who responded best participated in a follow-up study (Ebbels, 2007) targeting comprehension of the dative construction (e.g. the boy is giving the girl the rabbit) and wh-comparative questions (e.g. what is bigger than a cat? vs. what is a cat bigger than?). All three received intervention on datives, but only two received intervention for wh-comparatives due to a change of SLT. Two of the three participants showed significant progress in their comprehension of dative constructions. The third was hypothesized to have additional short-term memory difficulties that made progress on this area more difficult, due to the need to remember the order of three key nouns. However, this participant made significant progress in comprehension of wh-comparative questions, as did the other participant who was taught this structure.
The studies of Shape Coding discussed above all involved individual therapy sessions. However, an uncontrolled study on the use of the past tense in writing (Ebbels, 2007) involved group teaching. A class of nine pupils (aged 11–13 years) were taught using the Shape Coding system during English lessons. Six used the past tense more after the class sessions, but two more made progress only when they received additional intervention in a pair. Possible explanations are either that they merely needed more intervention time, or that they needed a more individualized approach which could be provided in a pair, but not in a group of nine.
Until recently, all the studies of Shape Coding have been with secondary-aged children. However, Kulkarni et al. (in press) investigated its effectiveness for improving oral use of the past tense by two younger children (8-year-olds) in both structured tasks and conversation. We also considered whether additional generalization therapy was required for participants to use target forms in their spontaneous speech. One participant improved markedly in sentence completion but required the generalization therapy before gaining in the conversational task. The other made more modest gains in both areas without recourse to the generalization therapy.
c Other explicit approaches
The effectiveness of an explicit meta-linguistic approach has also been investigated in Hebrew in a single uncontrolled case study (aged 12;2). Levy and Friedman (2009) investigated its effectiveness for improving the comprehension and production of structures involving syntactic ‘movement’ (relative clauses and topicalization) in Hebrew. Their method was similar to Colourful Semantics and Shape Coding in that they colour coded verbs and their arguments (as in Colourful Semantics) and they explicitly taught movement showing the link between the moved item and its trace (as in Shape Coding; see Ebbels and van der Lely, 2001). They found significant progress in most areas targeted and also generalization to areas not targeted, such as wh-questions.
d Summary of explicit approaches
Studies of metalinguistic approaches indicate that they can be effective for school-aged children with language impairments, including those of secondary age and those with receptive language difficulties. There is no evidence of whether these approaches are effective when delivered by anyone other than an SLT.
3 Comparison of explicit and implicit approaches
A few studies have compared the effectiveness of implicit vs. explicit therapy for improving expressive language. These have found conflicting results, which may be due to the age of the children, the target of therapy, or the design of the studies. One study (Swisher et al., 1995) found that younger children with SLI (age 4–6 years) learned to generalize novel bound morphemes trained in a story context to untrained vocabulary stems better with implicit than explicit training. In contrast, Finestack and Fey (2009) found that children with language impairment (aged 6–8 years) learned to use novel verb inflections better with explicit than implicit training. Motsch and Riehemann (2008) found German children with SLI (aged 8–10 years) learned the dative case better with explicit than implicit intervention, whereas both methods were equally effective for improving the accusative. However, there were several possible biases in this study; for example, the more willing and knowledgeable teachers carried out the explicit intervention. It is also unclear whether the two groups received equal amounts of intervention.
These three studies together appear to indicate that implicit approaches may be more effective for younger children (under 6 years) while explicit approaches may be more appropriate for older children. However, given the limited range of targets and the fact that all the targets involved expressive morphology, much more work needs to be done to draw any firm conclusions.
4 Combination of explicit and implicit approaches
In a study of the effectiveness of grammar therapy in a school setting, Smith-Lock et al. (2013a) showed a significant effect of direct explicit teaching combined with grammar facilitation techniques on the ability of 5-year-olds with SLI to produce subject pronouns, possessive s and past tense -ed. Their experimental group improved more than the control group, but only when they received intervention (in a group), not during baseline. The effects did not generalize to untreated grammatical targets. At a single-case level, most children showed a treatment effect. Six made no progress, but five of these had articulation difficulties. A follow-up study (Smith-Lock et al., 2013a) showed that this approach was only effective when provided in eight weekly sessions rather than eight daily sessions.
Some of the studies discussed above (e.g. Kulkarni et al., in press), while predominantly using explicit methods, also used some grammar facilitation methods. Indeed, in clinical practice, the two are often combined. Given that 50% usage of a targeted structure may be required before recasting can be effective, it may be that explicit methods could be used for initial teaching and then recasting could be used thereafter. However, further research is needed to establish whether a combination of approaches is more effective than purely implicit or explicit therapy and, if so, how and when the two methods should be combined.
Several studies have focused on both narrative and grammar abilities in parallel. These are shown in Table 4. These tend to have an explicit approach to narrative structure and an implicit approach to grammar. Specifically, the ‘narrative based language intervention’ (NBLI) used in Swanson et al. (2005) and Fey et al. (2010) explicitly taught narrative structure while using grammar facilitation approaches to teach grammar. Swanson et al. (2005) found their intervention improved the quality of the children’s narratives, but not their grammatical abilities. The authors suggest this could be due to limited processing resources, such that children with SLI only focus on explicit targets. Fey et al. (2010) also found NBLI did not yield significant improvements in the grammatical production of children with SLI, but did improve their narrative comprehension (as this study primarily focused on the effectiveness of Fast ForWord, it is shown in Table 5).
Studies targeting narrative and grammar together.
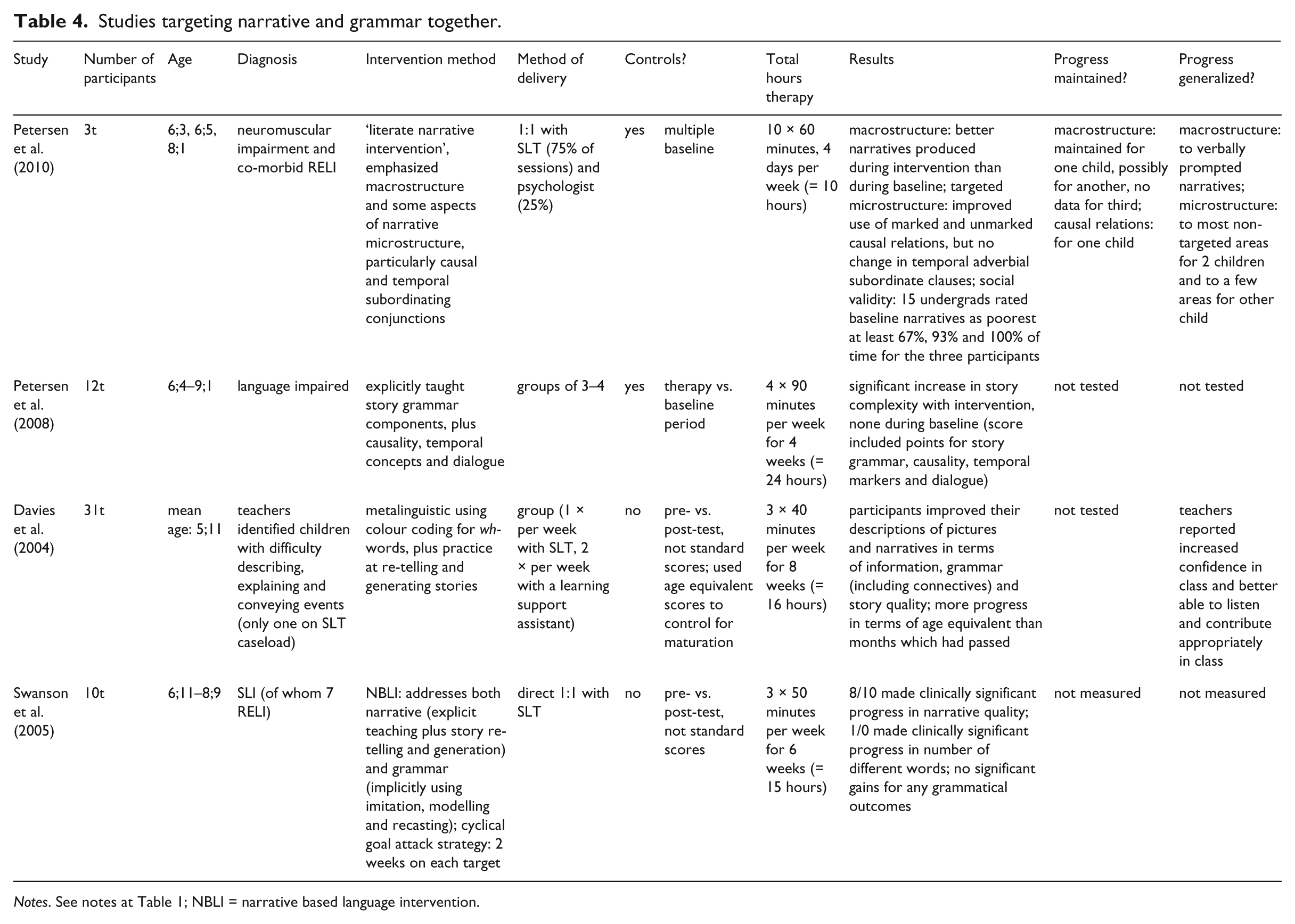
Notes. See notes at Table 1; NBLI = narrative based language intervention.
Studies targeting improvement in general receptive and/or expressive language (assessing effectiveness of Fast ForWord, FFW).

Notes. See notes at Table 1; AE = academic enrichment; CALI = computer assisted language intervention; CASL = Comprehensive Assessment of Spoken Language; CTOPP = Comprehensive Test of Phonological Processing (Wagner et al., 1999); FFW = Fast ForWord; ILI = individualized language intervention; NBLI = narrative based language intervention.
Some other studies (Davies et al., 2004; Petersen et al., 2008, 2010) used explicit therapy to focus mainly on narrative production, but also included some work on expressive grammar. These found progress on narrative ability and grammar. However, the scores for narrative and grammar were often conflated, so it is difficult to know whether the positive change was in both areas.
IV Language interventions not specific to grammar
1 Acoustically modified speech (including Fast ForWord, FFW; Scientific Learning Corporation, 1998)
Intervention studies using acoustically modified speech have focused mainly on receptive rather than expressive language and are shown in Table 5. They are based on the theory that children with SLI have difficulty processing rapid or brief stimuli (Tallal et al., 1985) and aim to improve this underlying deficit by training the auditory system using acoustically modified speech. The children’s general language abilities are hypothesized to improve as a direct consequence of their improved temporal processing abilities. An early study of FFW reported that children’s language comprehension improved significantly (Tallal et al., 1996). However, there were several problems with the design of this study.
Independent case study investigations of FFW (Friel-Patti et al., 2001; Gillam et al., 2001; Loeb et al., 2001) showed the majority of children made some progress with some areas of language, although the children with the most severe language impairments appeared to benefit the least. However, recent independent large-scale RCTs (Cohen et al., 2005; Fey et al., 2010; Gillam et al., 2008) found control groups showed equal progress to those receiving FFW (or similar acoustically modified speech; see Bishop et al., 2006; details shown in Table 2) and a recent meta-analysis, which is the strongest form of evidence (Strong et al., 2011) has concluded ‘there is no evidence … that FFW is effective as a treatment for children’s oral language or reading difficulties’ (p. 224).
2 Language intervention packages
Several recent studies have considered the effectiveness of intervention packages delivered in different ways and are shown in Table 6. These studies include a range of intervention approaches and targets with the aim of improving language generally, and their main focus is on establishing whether non-SLTs can effectively provide intervention.
Studies assessing different models of service delivery (targets and intervention method not the focus).

Notes. See notes at Table 1; CELF = Clinical Evaluation of Language Fundamentals; DEAP = Diagnostic Evaluation of Articulation and Phonology (Dodd et al., 2002); SLTA = speech and language therapy assistant.
Studies by Boyle and McCartney and colleagues of commonly used interventions delivered in mainstream schools found that children with ELI made more progress than controls in expressive language on the Clinical Evaluation of Language Fundamentals-3 (CELF-3, Semel et al., 2006) when they received intervention by an SLT or SLT assistant employed by the research project (Boyle et al., 2007, 2009). This contrasted with children with RELI who made no progress relative to controls with either receptive or expressive language. Indeed, on the Receptive Language Scale, children receiving therapy (whether or not they had receptive language difficulties) showed no greater progress than controls.
However, a follow-up study (McCartney et al., 2011), using the same intervention but delivered by school staff (teachers, deputy head teachers, language support teachers and classroom assistants), found no effect of intervention for either receptive or expressive language relative to the Boyle et al. (2009) historical controls. The most likely reason for this is probably the limited amount of intervention actually delivered. However, this model of working through education staff is one followed by many SLT services.
The major difference between the Boyle et al. (2007; 2009) and McCartney et al. (2011) studies was in the background and employment those delivering the intervention. In Boyle et al. (2007; 2009), they were employed by the researchers running the study and were psychology graduates. In the McCartney et al. (2011) study, they were school staff, with many other demands on their time. Indeed, 54% of the teachers who had implemented the intervention in this study agreed or strongly agreed that ‘this method of working expects too much of the teacher’ (McCartney et al., 2010: 362). Even after modification of the language therapy support model and revision of the manual (now called the Strathclyde Language Intervention Programme, SLIP) following feedback from some of the teachers, potential users (teachers who had not been involved in earlier studies) were unsure whether implementing the model and delivering the language-learning activities would be realistic (McCartney et al., 2010). These studies are extremely worrying as they indicate that a very common model of therapy in the UK may be unrealistic and ineffective.
Nevertheless, an ‘enhanced consultative model’, using SLT assistants employed by the SLT service (Mecrow et al., 2010), was effective. Progress on targets (both speech and language, receptive and expressive) was significantly greater than progress on control areas. They also found significant change on the CELF-Preschool receptive and expressive language scales. However, they did not split the analyses to see if the effectiveness of therapy varied between target areas or between different groups of children.
It is not the case that school staff cannot effectively deliver intervention if they are well enough trained, supported and monitored. A small-scale study (Hutchinson and Clegg, 2011) indicates that language groups delivered by well-trained and supported education professionals can improve expressive language. In this study, a teacher from a collaborative team of specialist teachers and SLTs who initially delivered a whole-school training package was in the school for two days a week during the project. Thus, the education professionals delivering the intervention were well-supported and their provision was closely monitored.
Several studies from the education literature (e.g. Bowyer-Crane et al., 2008) have also shown that, if well-supported and closely monitored, TAs can successfully deliver intervention that improves expressive language, taught vocabulary and literacy in children with literacy difficulties. Follow-up analyses (Bowyer-Crane et al., 2011) of only the children from the Bowyer-Crane et al. (2008) study who had language impairments showed that intensive intervention from a highly trained and well supported TA can improve understanding of taught vocabulary and expressive grammar (although not comprehension) in children with language impairments, regardless of their non-verbal IQ level.
V Variables in intervention
1 Targets of intervention
Implicit, grammar facilitation methods have focused on production of a wide range of morphological and syntactic targets; however, language comprehension has been largely ignored as a focus of intervention (with the exception of the usage-based approach by Riches, 2013). Studies using acoustically modified speech have focused on general language abilities, not specific morphological or syntactic targets (with the exception of Bishop et al., 2006). Studies of explicit methods have mainly focused on specific areas of grammar (both comprehension and production). The few studies that have considered maintenance of progress generally show that progress is maintained but does not usually continue after intervention has ceased.
2 Child factors
The majority of studies of implicit grammar facilitation methods reported here either do not mention the receptive language status of their participants (seven studies), or state that the majority of their participants have age appropriate comprehension (four studies). Eight of the studies reviewed included children with RELI, but of those, three showed no greater progress than controls. The other five did not investigate whether those with vs. without receptive language difficulties differed in the amount of progress they made, but analysed them as a whole group which may mask any differences between them. However, a case series (Ellis-Weismer and Murray-Branch, 1989) found that the three children with expressive difficulties only made progress, but the one with RELI did not.
The participants in studies of explicit meta-linguistic methods have usually had both receptive and expressive language difficulties (regardless of whether the targets of intervention were receptive or expressive). However, these different participant profiles could be a function of age, as those children whose language difficulties persist are often those who have more pervasive difficulties (Bishop and Edmundson, 1987). The majority of grammar facilitation studies have been carried out with children under the age of seven, often with pre-schoolers, although a few studies using these methods include children up to 10 years of age. In contrast, studies of explicit approaches have involved a wider age range, but have tended to focus on older children.
Direct comparisons of explicit and implicit methods indicate that explicit methods may be better for older children and implicit for younger, but differing responses by age have not been measured in a single study. Also, the relationship between age, severity and response to different intervention approaches remains to be considered. Ebbels et al. (2013), did look for correlations between progress and age (and indeed non-verbal abilities) and found no correlations, but all participants were over 11 years. Direct comparisons of the two main approaches (explicit vs. implicit) with different age groups and different levels of severity (especially as regards expressive language) are therefore now required.
3 Methods of delivery
The overwhelming majority of studies aiming to directly improve children’s grammatical abilities involve 1:1 delivery of intervention by an SLT or (for the modified speech studies) by a computer. However, several recent studies have focused on the effectiveness of education staff delivering intervention. These have found that well-trained and supported assistants employed directly by the SLT service, or research teams, or very closely monitored, can improve the expressive language of children with expressive language difficulties only, whether the intervention is delivered 1:1 or in groups. However, a ‘consultative model’, where a programme is left for school staff to carry out with little support and monitoring, does not seem to be effective.
Disappointingly, standard therapy packages (whether delivered by an SLT or assistant, 1:1 or in groups) do not seem to improve the receptive or expressive language abilities of children with RELI. However, several studies indicate that explicit therapy methods, either alone, or in combination with more implicit methods, delivered by an SLT can be effective for improving both receptive and expressive language in this group. Implicit therapy methods alone may be effective for this group, but we cannot evaluate this until analyses of progress of children with RELI have been carried out separately from those with purely expressive difficulties.
VI Implications
1 Future research
Many areas of grammar have been targeted in intervention studies but many gaps remain. In particular, grammar facilitation methods have focused only on expressive language, primarily with younger children, many of whom do not have receptive language difficulties. In contrast, metalinguistic methods have focused on both comprehension and production skills, but mostly with older children. Thus, both these methods should be investigated further with different age groups and receptive language status, for both comprehension and production of language.
The relative benefits of the two main approaches, and indeed their combination, also needs to be investigated with different age groups and with those with and without receptive language difficulties. Such studies will require large numbers of participants. Even if age and receptive language skills are held constant, the effect size of a difference between two interventions is likely to be much smaller than between an intervention and control (where significant effects can be found in quite small studies). Varying age and receptive language status will require even larger numbers of participants in order to find significant effects within different groups.
Children with receptive language difficulties appear to be the least likely to progress with therapy, but also are those the most in need. Therefore studies are urgently needed with this group to establish which aspects of intervention are crucial in enabling these children to make progress.
2 Clinical implications
The intervention research base needs further development before clinicians can make reliable judgements regarding the appropriateness of different intervention approaches and methods of delivery for individual children for particular grammatical targets. However, it is important for clinicians to make informed decisions using the evidence available. I would suggest that clinicians who wish to target the grammatical difficulties of a school-aged child, should first establish which areas of grammar are causing difficulties. Then, they should decide which areas they wish to treat and in which order. These decisions should be based on factors such as functional importance (e.g. the impact on access to the curriculum and friendships), typical developmental order of acquisition and a plan of how to proceed from one target to another, as one target may require prior learning of another.
Having decided on the targets, they should then consider whether any particular method of intervention has been shown to be effective (preferably in a study including experimental control) for that target, for children of a similar age, diagnosis and level of severity to the child they wish to treat. The tables in this paper are grouped by language target and sorted by level of experimental control to aid clinicians in this process.
The final step is to choose the method of delivery. The research evidence is primarily based on 1:1 delivery of therapy by an SLT. For a variety of reasons, clinicians may not be able or wish to offer this method of delivery, but they should be aware that a change in the method of delivery may affect the effectiveness of the intervention. It seems that delivering therapy via assistants and/or in groups can be effective for improving expressive language in children with ELI, but only if the assistants are well trained, supported and closely monitored to ensure that they do actually carry out the intervention. Indeed, McCartney et al. (2011) recommend that ‘SLT and school services adopting a consultancy model require a careful activity audit to be undertaken’ (p. 80).
However, for children with RELI, the limited evidence to date of effective intervention indicates that progress may only be made when intervention is delivered by an SLT, as in the studies of explicit therapy methods which mostly involve such children (even when focusing on expressive targets). However, if a clinician decides to use other methods of delivery for children with RELI, they should evaluate closely what they have done and share their findings with the rest of the SLT community.
VII Conclusions
In recent years, the quality and quantity of studies investigating the effectiveness of intervention for grammar in school-aged children has greatly improved. We can have reasonable confidence in the effectiveness of some interventions for particular types of children, but we have yet to compare directly the effectiveness of these different approaches with different types of children in order to establish which method is the most effective for which children using which method of delivery.
A parallel challenge is using this evidence wisely in clinical practice. Clinicians and services are under pressure to deliver effective interventions at the lowest possible cost, and at times effectiveness and cost may indicate different intervention or methods of delivery. A balance has to be struck. However, clinicians should ensure they do not waste everyone’s time and money providing intervention which has been shown to be ineffective, even if it is the cheapest option. Providing ineffective intervention benefits nobody.
We also need to be very clear about the difference between:
evidence that an intervention is ineffective; and
no evidence that an intervention is effective.
In the former case, we should not provide the intervention, even if we / the children / their parents / schools / commissioners like it. In the latter case, the intervention may be effective or ineffective: we just do not know. If there is evidence that another intervention is effective, then that should be used. But if there is no evidence, we should use a best-fit approach combined with clinical experience and then evaluate its effectiveness for the particular combination of target and child factors with which we are faced.
All clinical work has the potential to be a research project with the addition of experimental control. This can be achieved, for example, by use of waiting lists as waiting controls, using school holidays as baseline periods, or having control areas for each targeted area (for discussion of the value of case studies, see Vance and Clegg, 2013). Small group studies and even small-scale RCTs can also be carried out within clinical services, involving children with a profile relevant to that particular service and targeting priority areas. If the effect sizes are large enough (and hence clinically important), these can be significant even with relatively small numbers of participants. Indeed, the small-scale clinically-based RCTs that I have led have had only 14 (Ebbels et al., 2013), 15 (Ebbels et al., 2012) and 27 participants (Ebbels et al., 2007). All showed significant differences between intervention and controls (although not between interventions), because the effect sizes were large. Thus, RCTs need not require huge amounts of money to run (unless small effects are expected, such as comparisons of interventions) and should be possible for SLT services to carry out with appropriate support. If research becomes more embedded in our clinical practice, we have the potential to improve our evidence base dramatically, which will benefit both the SLT profession and the children we serve.
Footnotes
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.