
Abstract
The objective of the study is to assess the relationship between functional limitation and use of dental services among older American adults; and whether this relationship is independent from socioeconomic factors. We used data pertaining to older American adults aged 60 years and over from the 2022 Behavioral Risk Factor Surveillance System (BRFSS). Functional limitation was indicated by difficulties in hearing, seeing, concentrating or remembering, walking or climbing stairs, dressing or bathing, and doing errands alone. Use of dental service was indicated by one or more dental visit within the past year. Logistic regression was conducted to assess the association between any limitation and use of dental service adjusting for income, education, health insurance, smoking, tooth extraction, age, sex and ethnicity. The analysis included 142,095 participants. Dental visit within past year, and functional limitations were reported by 67.4% and 39.7% of the participants, respectively. Functional limitation was negatively associated with dental visit in the previous year with Odds Ratios 0.69 (95% Confidence Intervals: 0.65, 0.74) in the fully adjusted model. Functional limitation could be a potential and additional barrier to use of dental services among older Americans. Public health strategies should consider alternative care models for those with functional limitations.
Introduction
With the ageing population oral diseases of older adults and use of dental services are becoming global public health issues. In 2019, oral diseases resulted in over 8 million years of healthy life lost among the global population aged 50-74 (Patel et al., 2021). Nutrition, communication, and general health in later life are all significantly associated with oral health. Despite the recognized importance of oral health, the utilisation of dental services among older adults remains inadequate (Chavis and Macek, 2022). As society progresses, a larger population of older adults are in an increased need of complicated dental treatment due to the rise in tooth retention at old age (Peres et al., 2019). However, public funding constraints, age-related mobility issues and transportation difficulties have further exacerbated access to oral healthcare. This resulted in low utilisation rates of dental services among older adult, accumulation of untreated dental diseases or diseases diagnosed at an advanced stage, ultimately leading to a poor prognosis (Peres et al., 2019).
Functional limitations measured using impairments in Activities of Daily Living and Instrumental Activities of Daily Living (ADLs/IADLs) are increasingly becoming an obstacle to healthcare access in ageing societies (Conant et al., 2014; Katz, 1983; Shiraishi et al., 2019). Furthermore, given their effects on older individuals, hearing and vision impairments may also be significant elements of functional restrictions (Bright et al., 2023; Lin et al., 2019; Rahmati et al., 2025). Therefore, it is reasonable to include them as additional markers of functional limitations.
While earlier studies demonstrated an association between disability and low dental visit rates, but they mainly focused on specific health conditions, younger age groups, or failed to distinguish functional limitations from other types of disability (Binmogren et al., 2024; Chavis and Macek, 2022). Another study demonstrated an association between number of extracted teeth and functional limitations among older Americans, but they did not include dental visits (Chalittikul et al., 2020). Evidence remains limited on whether functional limitation is independently associated with dental visits among older adults, particularly in countries with no universal coverage of oral healthcare such as United States. In this context, this study utilises a nationally representative cross-sectional survey of Americans adults to assess this relationship. The objective is to examine the relationship between functional limitations and use of dental services among older American adults, and whether the relationship, if existed, is independent from socioeconomic factors.
Methods
The study utilised data from the 2022 Behavioural Risk Factor Surveillance System (BRFSS), an annual cross-sectional telephone survey of American adults. The sample was restricted to 142,095 participants aged ≥60 years, who had complete data on exposure, outcome and confounders. The BRFSS is a state-based telephone survey conducted using standardised protocols. Additional details of BRFSS could be found elsewhere (Alzahrani et al., 2024; Chalittikul et al., 2020).
Data were collected via telephone interviewing of United States (US) residents in 50 states, the District of Columbia, Guam, Puerto Rico, and the US Virgin Islands. Interviews were conducted in English or Spanish. The survey included questions on functional limitations, dental visits, tooth loss, health insurance and sociodemographic factors.
Main exposure
The survey included six questions which indicated functional limitations. Participants who reported difficulties in concentrating, remembering, walking, climbing stairs, dressing, bathing, and independently running errands alone are widely recognized as components of ADLs or IADLs. According to recent research, hearing and vision impairments should be regarded as significant elements of functional limitations since they affect people’s ability to live independently and seek healthcare (Bright et al., 2023; Lin et al., 2019; Rahmati et al., 2025). In this study, functional limitation was indicated by difficulties in hearing, seeing, concentrating or remembering, walking or climbing stairs, dressing or bathing, and doing errands alone. A variable for functional limitation was created where participants who indicated having any of these 6 limitations were categorized as having functional limitations. We also used the sum of the 6 limitations in the descriptive analysis. These 6 variables were originally reported as binary (yes/no) responses to whether the respondent has serious difficulty in each domain.
Outcome variable
Dental service utilisation was assessed by asking respondents how long it had been since they last visited a dentist or dental clinic. The response included: within the past year, 1 to <2 years ago, 2 to <5 years ago, 5 or more years ago, and never. For this study, responses were recoded into a binary variable: dental visit past year versus more than 1 year or never.
Covariates
These included demographic variables: age (in years), sex, race/ethnicity (White, Black, Hispanic, Others). Socioeconomic factors included education (high school or less, some college, college graduate), and income which was categorised into quartile. Availability of any health insurance (covering medical services), smoking (current, former and never smoked) and tooth extraction (one or more tooth removed vs none) were also included in the analysis.
Statistical analysis
Overall characteristics of the sample was assessed. Distribution of each variable by dental visit in the past 12 months and by functional limitation were also assessed. Furthermore, the mean number of limitations among participants who reported and did not report dental visits was also assessed. Two multivariable logistic regression models examined the association between functional limitation (any limitation) and dental visit within the past 12 months. Model 1 was adjusted for age, sex and race/ethnicity. Model 2 was additionally adjusted for education, income, health insurance, tooth extractions, and smoking. Stata version 17 survey commands were used throughout the analysis using the final weight for landline and cellular phone interview.
Results
Characteristics of the participants and associations with dental visits in the Past 12 Months - older American adults (BRFSS, 2022; N = 142,095).
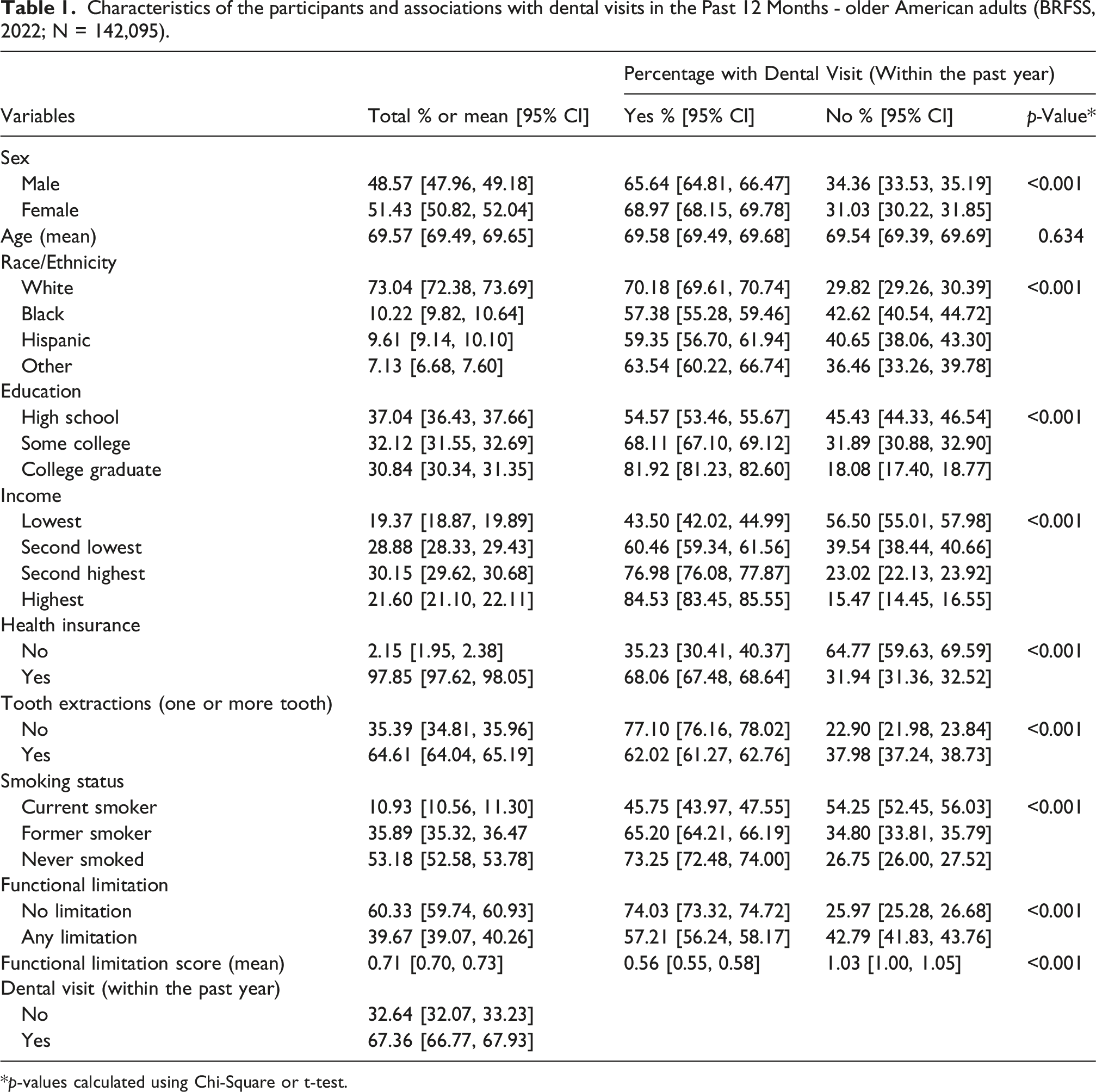
*p-values calculated using Chi-Square or t-test.
Association between sociodemographic, behavioural factors and functional limitation among older American adults (BRFSS, 2022; N = 142,095).
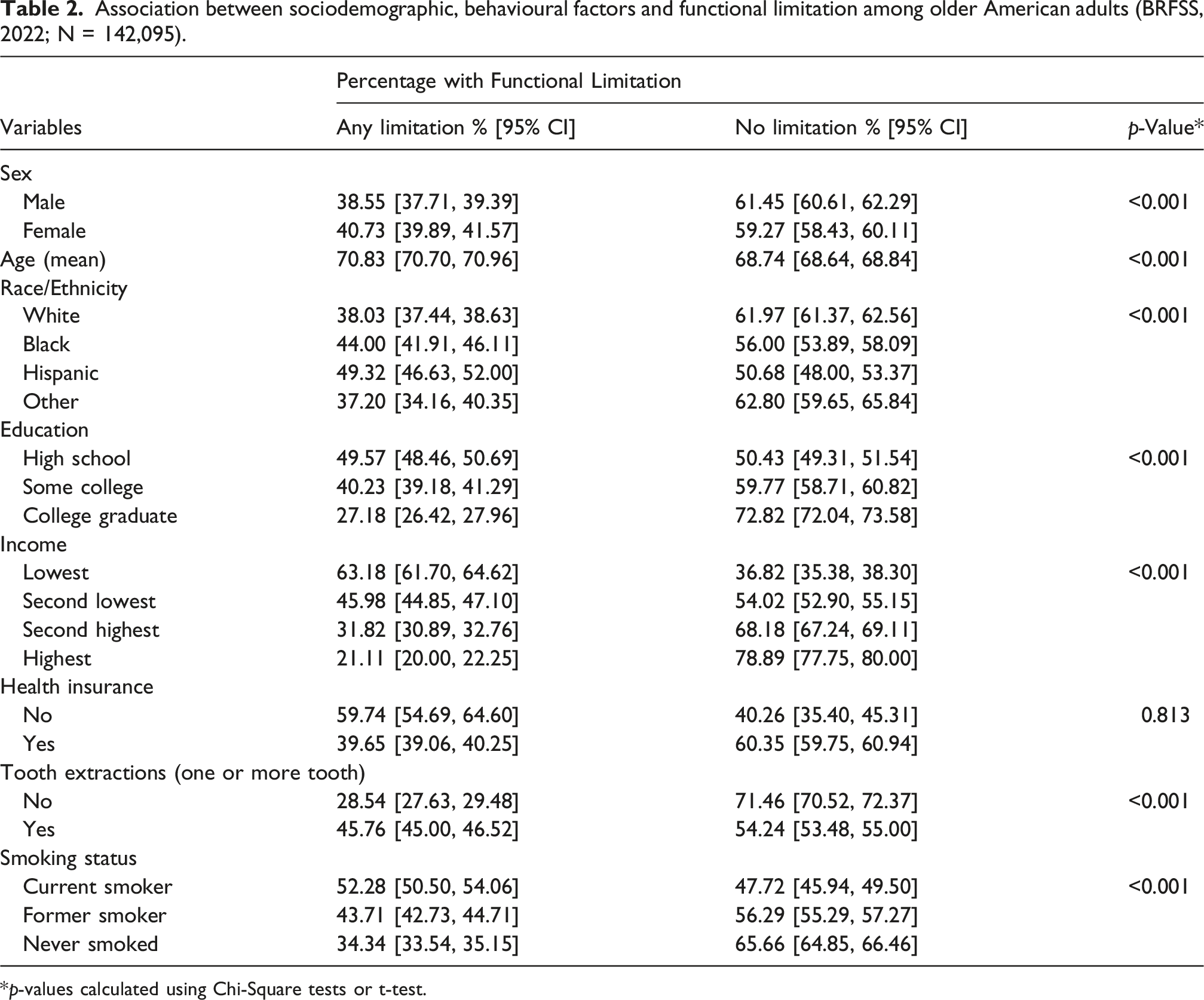
*p-values calculated using Chi-Square tests or t-test.
Logistic regression showing the association between functional limitation and dental visit among older American adults (BRFSS, 2022; N = 142,095).
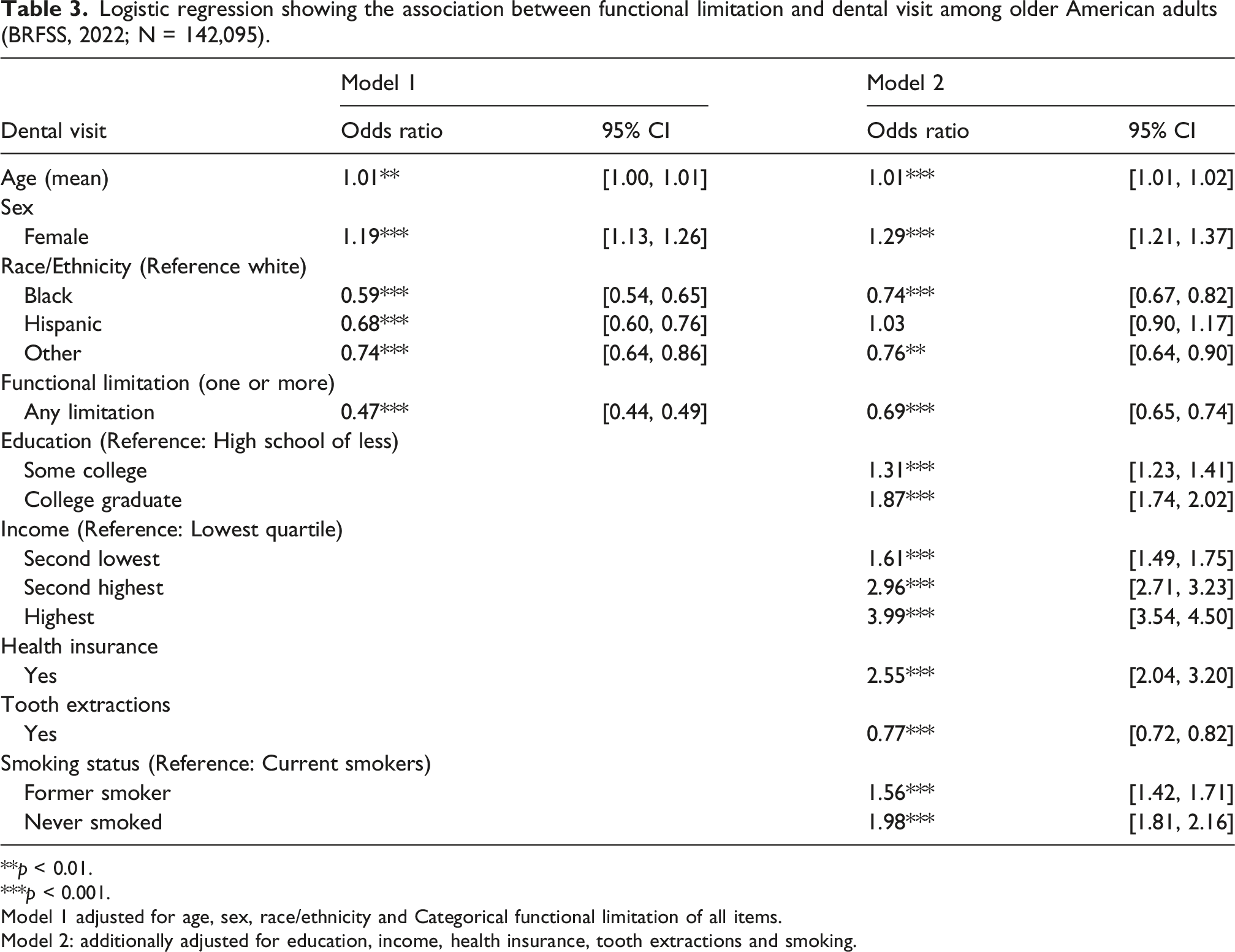
**p < 0.01.
***p < 0.001.
Model 1 adjusted for age, sex, race/ethnicity and Categorical functional limitation of all items.
Model 2: additionally adjusted for education, income, health insurance, tooth extractions and smoking.
Discussion
This study examined the relationship between having functional limitation and use of dental services in the previous year among older Americans. The findings of this analysis demonstrated that having any functional limitation was significantly and negatively associated dental visits. Interestingly, after accounting for socioeconomic factors and health insurance the negative relationship persisted, although slightly attenuated, highlighting that this association is independent from socioeconomic factors. This indicates that functional limitation could be a distinct and possibly independent obstacle to this population’s use of dental services.
Previous research has established a link between disability and reduced use of dental care, but most studies have failed to isolate functional limitation as an independent factor, particularly among older adults (Binmogren et al., 2024; Chavis and Macek, 2022). For example, one study used BRFSS 2020 data to show that adults with disability had significantly lower dental care utilisation, but their analysis included adults aged 18 and above, and functional limitation was not distinguished from other disability types (Binmogren et al., 2024). Another study using BRFSS 2014, found that there was a significant association between the number of extracted teeth and function limitation among US older adults aged 65 and more, yet their outcomes did not include dental attendance (Chalittikul et al., 2020).
Studies from outside the US have also assessed the association between functional limitations and dental visits. A study based on a Japanese cohort demonstrated how physical decline affected the continuation of dental care (Tanaka et al., 2025). On the other hand, the current analysis benefits from using a nationally representative sample, using a current policy-relevant outcome (recent dental attendance), and providing timely insight into post-pandemic inequalities in access to care. Another prospective study from Japan demonstrated a reversed relationship, arguing that regular dental visits may prevent severe functional disability (Tomioka et al., 2020).
Functional limitation is likely to influence utilisation of dental services through several pathways: First, physical access and transportation. Mobility limitation, vision impairment or hearing problems make travelling to a clinic and tolerating procedures more difficult (Chavis and Macek, 2022; Lin et al., 2019; Rahmati et al., 2025). Second, cognitive limitation, such as difficulties with concentrating or planning may hinder appointment scheduling (Gold, 2012). Third, reduced perceived need. Persons with advanced limitations often prioritise other health problems and may consider dental care less essential. Last, self-care difficulty and independent living difficulty. Older adults with functional limitations could have increased reliance on caregivers (Granados-Santiago et al., 2023).
The attenuation of the association between functional limitations and use of services after accounting for education and income highlights the importance of socioeconomic factors in dental utilisation (Soares et al., 2025). This is particularly important in countries with no universal/free dental coverage. Although the analysis showed a positive association between having any health insurance and dental visits, this does not necessarily reduce inequalities in access particularly among those with functional limitation. In the US, having insurance does not guarantee coverage for dental care, especially for older adults on Medicare, where dental services are not included or minimally covered (Simon et al., 2023). Smoking was another predictor of dental visits which was consistent with earlier studies that showed that health risk behaviours, such as smoking are usually associated with other negative behaviours such as lack of dental visit (Alzahrani et al., 2024). While Black Americans had lower odds for visiting a dentist than Whites, Hispanic older adults did not differ significantly from Whites after accounting for socioeconomic factors. These results may suggest that racial or ethnic identity alone does not drive inequalities in dental attendance as suggested in earlier research, socioeconomic position and access to resources may account for the observed gaps, particularly among Hispanic older adults (Wu et al., 2022).
This study has the advantage of using a large nationally representative sample and accounting for several confounders. To the best of our knowledge, no known study using a nationally representative post-pandemic data examined the association between functional limitation and the utilisation of dental service among older American adults. However, there are few limitations worth mentioning. First, the cross-sectional design does not allow for conclusion on temporality. Second, exposure, outcome and confounders were self-reported, which may have introduced recall bias. Third, BRFSS lacks detail on dental care type (urgent care, routine check-ups or continuation of treatment), clinic accessibility, dental insurance, caregiver support and psychological obstacles such as dental anxiety. The survey did not include participants with advanced cognitive impairment or those institutionalised which could lead to underestimation of the association between functional limitation and reduced dental service utilisation.
The findings highlight the need for revising Medicare policies to expand dental coverage, particularly for people with mobility, cognitive, or hearing and visual impairments, which could significantly improve coverage and accessibility of services.
Among older American adults, functional limitation appeared to be an additional and independent obstacle to using dental services. This relationship persisted even after accounting for education, income, insurance, tooth loss and smoking status. To improve equality in access, public health strategies should prioritize alternative care models for those with functional limitations.
Footnotes
Ethical considerations
Ethical approval was not required for this analysis.
Author contributions
CQ: conception of research, data analysis, writing; WS: conception of research, data analysis, editing and writing; RM: editing and writing final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.