
Abstract
This study aims to examine the associations of ethnicity and socioeconomic factors with obvious dental caries and assess longitudinal changes between 5 and 11-years of age. A retrospective longitudinal design was employed, linking individual-level health and education records for children aged 5 and 11-years living in Scotland between 2004 and 2018 (n = 155,737). At age five, Polish and Gypsy/Traveller children had around four times higher odds for developing obvious caries compared to White Scottish peers (OR = 4.37, 95% CI: 3.87–4.94) and (OR = 3.47, 95% CI: 2.52–4.79) respectively. By age 11, African, Chinese, Indian, and White British children showed lower odds of developing obvious caries, while Gypsy/Traveller (OR = 2.70, 95% CI: 1.98–3.70), and Polish (OR = 1.34, 95% CI: 1.18–1.52) children remained at elevated risk compared to White Scottish children. Longitudinal analysis revealed limited overall ethnic differences in new obvious caries development, though African (OR = 0.51, 95% CI: 0.39–0.67) and Chinese (OR = 0.58, 95% CI: 0.38–0.90) children were less likely to develop new obvious caries compared to White Scottish children. Several minority groups, including Polish, Gypsy/Traveller, Pakistani, and Arab children, demonstrated improvements in caries status between ages five and 11 compared to White Scottish children. Obvious caries presence at age five is strongly associated with caries at age 11 (OR = 3.24, 95% CI: 3.16–3.33). Ethnic disparities in obvious dental caries were evident at age 5 and independent of socioeconomic status. By age 11, these inequalities diminished for most groups, with socioeconomic factors emerging as the primary drivers of oral health inequalities, except among Gypsy/Traveller and Polish children.
Introduction
Dental caries is considered to be amongst the most prevalent conditions worldwide (Peres et al., 2019), affecting almost half of the world’s population and approximately 600 million children (Bernabe et al., 2025; Watt et al., 2018). In the UK, tooth extractions for dental caries remains the leading cause for elective hospital admissions for children between the age of five to nine years old (Public Health England, 2019; Public Health Scotland, 2025a). For context, in the financial year ending 2025 in England, there were over 7,000 more five to nine-year-old children hospitalised for dental extractions due to caries under general anaesthetic than for tonsilitis, the second most common reason for hospitalisation in this age group (NHS England, 2025).
The impact of socioeconomic inequalities on oral health is well explored, with several studies showing a strong correlation with up to four times higher rates of dental caries in children living in the most socioeconomically deprived compared to the least socioeconomically deprived communities (Public Health England, 2021; Ross et al., 2023). However, inequalities related to ethnicity in children’s oral health, are less well explored. One systematic review indicated that ethnic inequalities in dental caries among children are present in the UK, although the patterns are complex and not uniform, these differences are frequently driven by socioeconomic and cultural factors (Peres and Heilmann, 2015). A recent report by Public Health England (2021) reviewed multiple studies examining the inequalities that are related to ethnicity in child oral health, finding some evidence of higher caries rates among certain broad ethnic minority groupings children compared with rates in White children. The authors concluded that the findings were inconsistent and frequently confounded by levels of area-based socioeconomic deprivation.
Ethnicity and national identity are complex social and political constructs. They are linked to structural disadvantage and health inequalities independently of socioeconomic status (Ingleby, 2012). Throughout history, especially in countries with a colonial past, these constructs have been intertwined with power: the ability of certain groups to accumulate resources and opportunities at the expense of others. While socioeconomic status has long been an important driver of health inequalities, ignoring the complex dynamics between ethnicity, nationality, and power might miss an important element of this picture. Migration adds a further layer of complexity as the process itself, the journey, the vulnerability from a legal standpoint, language barriers, uprooting of social networks, and limited access to services can have significant consequences on health outcomes (Davies et al., 2009). At a time when societies experience increasing polarisation around immigration, ethnic minorities are becoming more vulnerable to the drivers of these inequalities. Oral health is no exception from this, as data suggests that people from Black, Asian and minority ethnic groups are often less likely to be able to access dental care (Public Health England, 2021).
One longitudinal study by Hall-Scullin et al. (2017) tracked a cohort of children from childhood through adolescence to examine the progression of dental caries. The findings showed that children who presented with caries in their primary dentition were significantly more likely to develop caries in their permanent teeth, particularly when influenced by socioeconomic disadvantage, a sugary diet, and poor oral hygiene – with children from Asian ethnic backgrounds having higher decay levels but no longitudinal changes were observed. In addition, migrant and native-born Irish children showed no substantial differences in oral health. Rouxel and Chandola (2018), in a cross-sectional study of school children in England, Wales, and Northern Ireland, found that ethnic and socioeconomic inequalities in oral health more were pronounced among younger children (aged five) compared to adolescents (aged 15), with residential deprivation reported as a consistent and significant determinant of poor oral health across both age groups. In a survey study from Ireland, migrant children consistently exhibited poorer oral health outcomes compared to their Irish-born counterparts, even after adjusting for socioeconomic variations – although differences by ethnicity were not considered (HagOmer and Hannigan, 2025).
One of the main challenges highlighted in the literature is the absence of consistent, disaggregated ethnicity data within national databases. This may result in an underestimation of the true magnitude of ethnicity driven inequalities. In addition, there is a recognised need for more intersectional oral health research including ethnicity (Elaine Muirhead et al., 2020), and more specifically on the explicit inter-relationship between ethnicity and socioeconomic factors, which was highlighted as a major public health issue during the COVID-19 pandemic (Amele et al., 2025).
Since 2003, in Scotland children’s oral health at age five and 11 years has been assessed annually through the National Dental Inspection Programme (NDIP), which collects clinical data at the individual child level (Merrett et al., 2005; Scottish Dental Epidemiological Co-ordinating Committee, 2003), however ethnicity data are not routinely recorded. In order to address this gap, there is a unique opportunity to examine inequalities in oral health among children by ethnic group via individual record linkage of health and education datasets. The latter accurately records child ethnicity (Scottish Government, 2018) which can be linked using secure NHS Scotland data linkage infrastructure (Clark et al., 2017; Pavis and D Morris, 2015). The aim of this study was to explore the associations between ethnicity, socioeconomic factors, and child dental health, and to investigate the longitudinal changes in obvious caries experience from age five to 11.
Methods
Study design and participants
Data
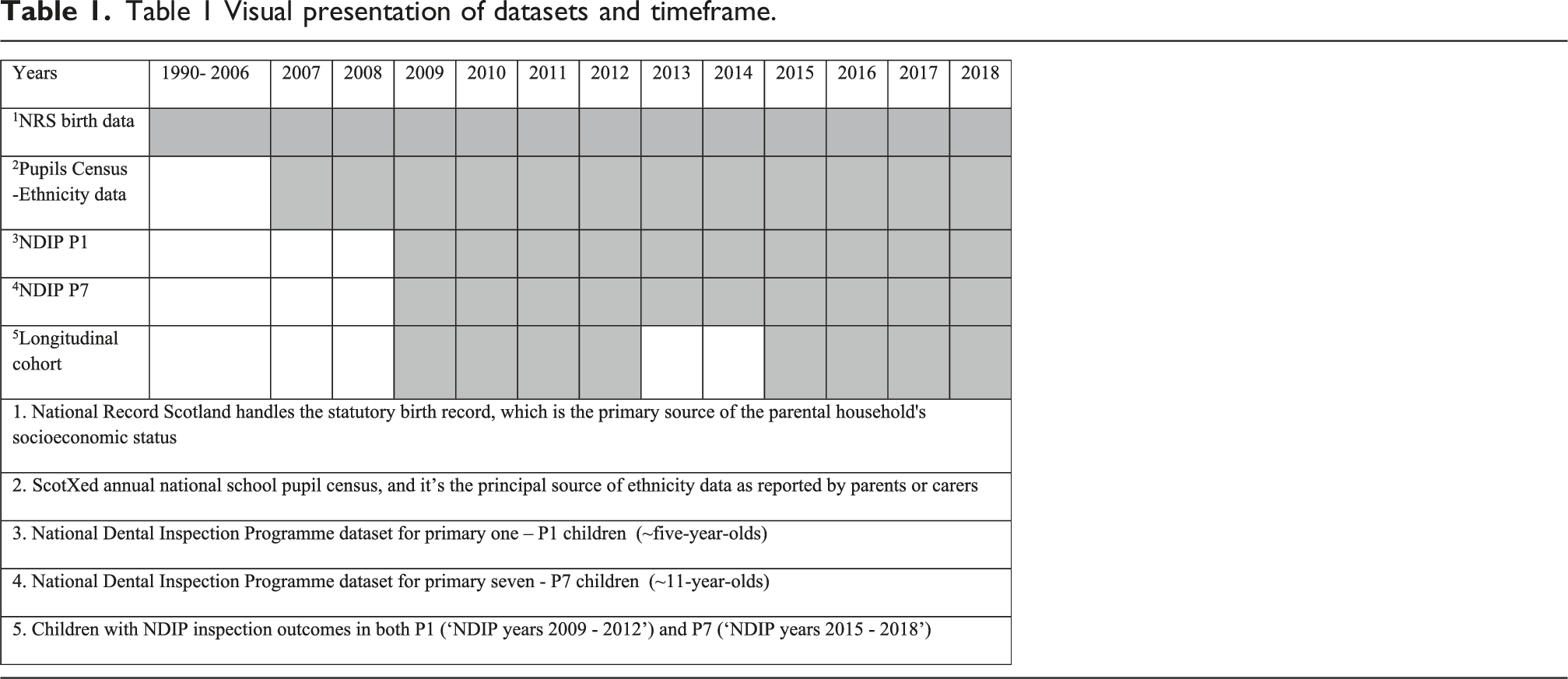
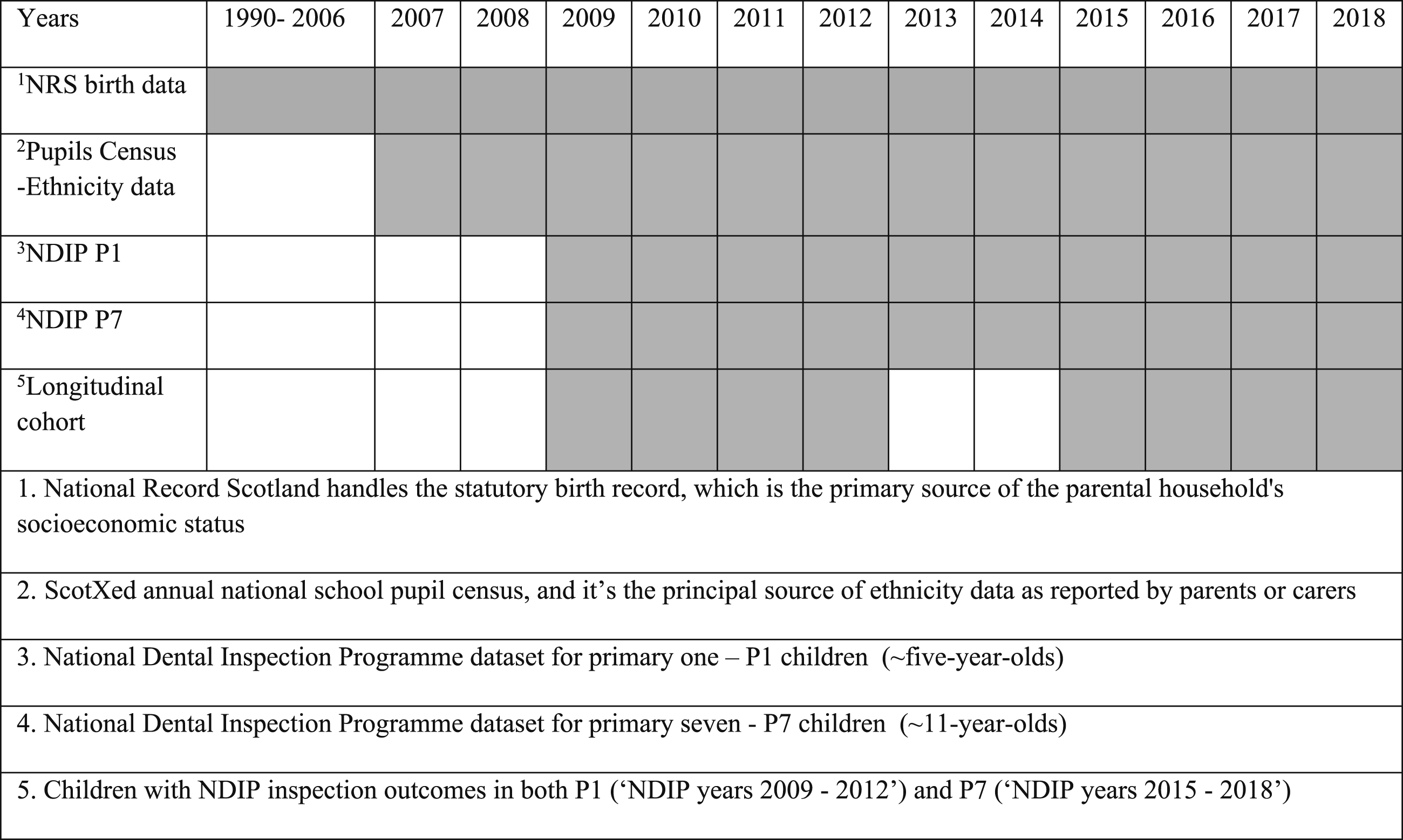
Children’s dental inspection records were sourced from the NDIP for the academic years from 2008/09 to 2017/18 (shortened to 2009 and 2018 for the rest of the manuscript) for both Primary 1 (P1 ∼ five-year-olds) and Primary 7 (P7 ∼ 11-year-olds). The annual basic NDIP inspection of publicly funded primary schools, conducted from November to May, involves a basic dental examination of pupils using a nationally standardised protocol (Macpherson et al., 2017). The Basic NDIP assessment involves a simple clinical examination of the child’s mouth using a light, mirror, and ball ended probe. Obvious caries experience is recorded by identifying the presence or absence of obvious decay, defined as caries into dentine, or by noting teeth that are missing, extracted due to decay, or filled. The oral health outcomes of NDIP fall into three categories: category ‘A’ shows severe decay or abscess, category ‘B’ shows history of tooth decay, and category ‘C’ shows no obvious decay experience. A new binary outcome was defined to denote obvious caries experience for children who were assigned A or B categories, and all category C children to represent no obvious caries experience (Macpherson et al., 2017; Sherriff et al., 2023).
Ethnicity data for study participants was sourced from the ScotXed annual national school pupil census. The census uses predefined ethnicity groupings used in Scotland’s census 2011 ethnicity classifications: White (Scottish, Other British, Irish, Gypsy, Polish, Other), Asian (Indian, Pakistani, Bangladeshi, Chinese, Other), African, Caribbean or Black, Arab, Other, Mixed - multiple ethnic group and ‘Not known/Not disclosed’ (Scottish Government, 2018). The Scottish Index of Multiple Deprivation (SIMD) fifths of the child’s home residence (postcode) was used as a measure of socioeconomic circumstances. The SIMD quantifies socioeconomic deprivation based on data zones - a geographical unit that is comparable to a postcode area. A total of 6976 data zones are ranked using combined and weighted data from seven domains (employment, income, crime, housing, health, education, and geographical access to services). Data zones are then ranked most to least socioeconomically deprived and can be converted to fifths, with SIMD-1 assigned to the 20% most deprived areas and SIMD-5 to the 20% least deprived areas (Ian et al., 2023). Parental occupational social class was also used as an individual (household) socioeconomic status (SES) measure – sourced from the Office of National Statistics Socio-Economic classification (NS-SEC) categories, which are recorded as part of the Scottish Statutory Birth Record (National Records of Scotland, 2025). For the purposes of this study, seven-class NS-SEC categories were used with an additional category added to classify children born outside Scotland.
Using individual-level data, the one-pass probabilistic method matched personal identifiers (date of birth, sex, and postcode from the pupil census, plus first and second names from NDIP datasets) was used to assign the Community Health Index number (CHI) to each record from the pupil census and NDIP datasets. A pseudonymised study identifier and a linkage identifier were assigned to each CHI (Wood et al., 2013). The relevant teams within Public Health Scotland (PHS) and Scottish Government Education Directorates extracted the data and passed it to the PHS Electronic Data Research and Innovation Service (eDRIS). The eDRIS analysts removed CHI numbers and uploaded all datasets into the National Safe Haven. A linkage agent replaced the study identifier with a pseudonymised anonymous study identifier, which uniquely linked each child’s records from all four databases (Sherriff et al., 2023) to ensure that none of the individual child-level data were identifiable.
The longitudinal cohort was compiled to include children with NDIP inspection outcomes in both P1 (‘NDIP years 2009 to 2012’) and P7 (‘NDIP years 2015 to 2018’). Following this, datasets from different NDIP years were combined to create an individual-level analytical cohort with ethnicity data, SMID fifths, and SES measures.
Analyses
All statistical analyses of outcome measures used data from the longitudinal cohort, which paired data from eight NDIP school years. Each child in the cohort belongs to one of four P1/P7 paired obvious caries experience groups (obvious caries in P1 and P7 = yes/yes, no obvious caries in P1 and caries in P7 = no/yes, obvious caries in P1 and no obvious caries in P7 = yes/no, and no obvious caries in P1 nor in P7 = no/no). Children with no obvious caries in P1 and no obvious caries in P7 served as the reference group. To evaluate the longitudinal transition in obvious caries experience between P1 and P7, McNemar’s test was used with the NDIP outcomes for the children in yes/no and no/yes groups. In addition, McNemar’s test was conducted for each ethnicity group separately to test that the proportion of change in P1 and P7 obvious caries experience is the same in all ethnic groups (Adedokun and Burgess, 2012). Multinomial logistic regression models with generalised logit link function were built with the four-level categorical obvious caries transition outcome as the dependent variable. The models were adjusted for sex, age, school year, SIMD, SES and ethnicity. Unadjusted logistic regression models were created to assess the association between obvious dental caries and all potential covariates for P1 and P7 children separately. An adjusted logistic regression model was created to test if early obvious caries in P1 were associated with obvious caries in P7. Additionally, interaction analyses were conducted to assess potential effect modification of the association between exposures and obvious caries outcomes. Attributable risks were calculated by estimating the percentage change in odds ratios (OR) using the formula
Statistical analyses were performed using SPSS version 29 and SAS version 9.4 within the Public Health Scotland National Safe Haven.
Results
Unadjusted ORs and 95% CIs for P1 and P7 obvious caries experience in relation to all covariates.
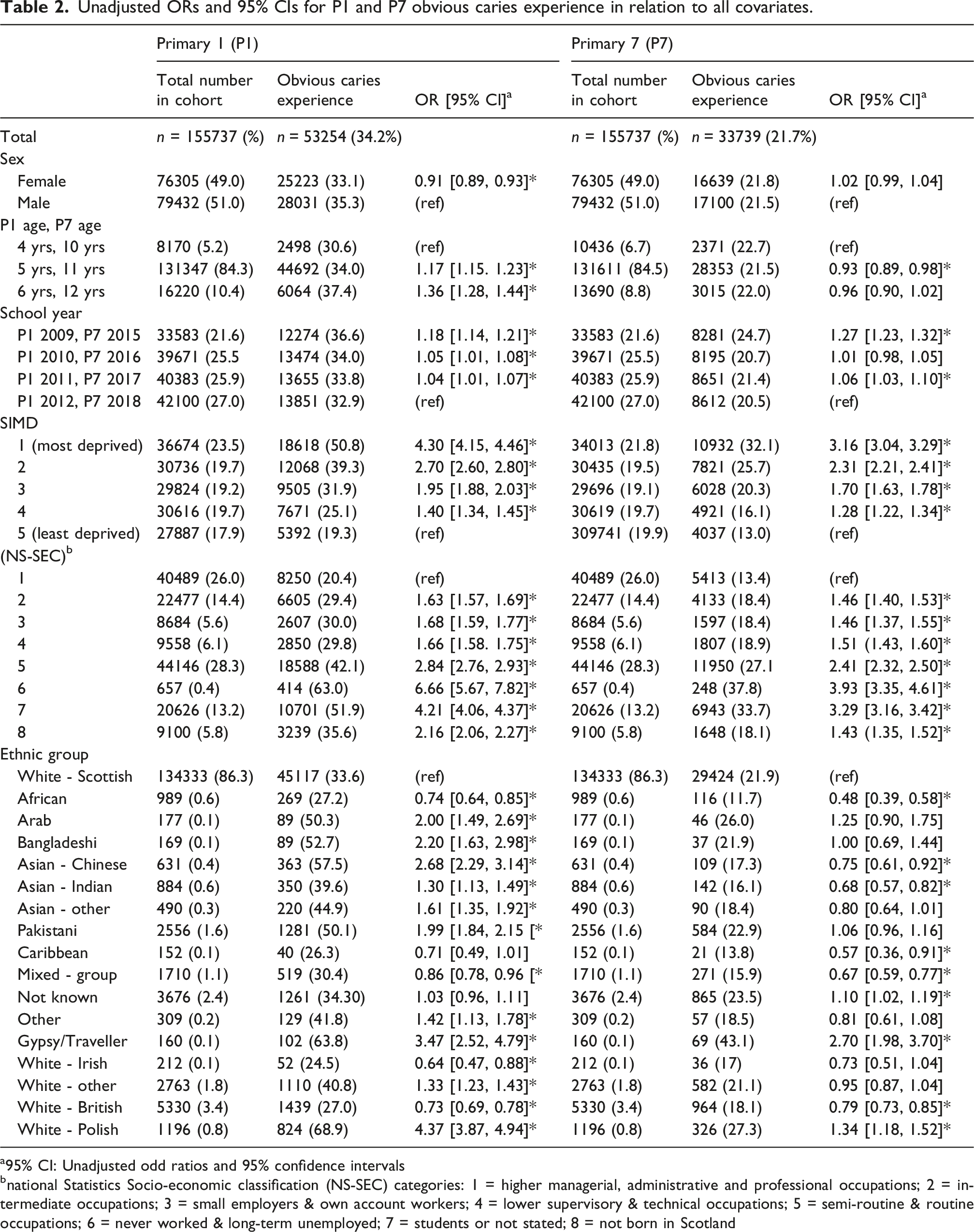
a95% CI: Unadjusted odd ratios and 95% confidence intervals
bnational Statistics Socio-economic classification (NS-SEC) categories: 1 = higher managerial, administrative and professional occupations; 2 = intermediate occupations; 3 = small employers & own account workers; 4 = lower supervisory & technical occupations; 5 = semi-routine & routine occupations; 6 = never worked & long-term unemployed; 7 = students or not stated; 8 = not born in Scotland
P1 oral health outcomes
The unadjusted univariate analysis of P1 (Table 2) on obvious caries experience showed that the prevalence of obvious caries was slightly lower in females (n = 25,223, 33.1%) than in males (n = 28,031, 35.3%). In addition, the data suggests that the risk of obvious caries increases with age in both groups. Children from the most socioeconomically deprived areas had over four times the odds of developing obvious caries compared to children from the least socioeconomically deprived areas (Risk Difference (RD): 31.5%; OR = 4.30, 95% CI: 4.15–4.46). Similarly, children whose parents had routine or manual occupations presented almost three times higher odds of developing obvious caries than children whose parents had professional or managerial occupations (RD: 21.7%; OR = 2.84, 95% CI: 2.76–2.93). Children from African, Mixed, Irish and White British backgrounds had lower odds of developing obvious caries compared to White Scottish children ((RD: 6.4%; OR = 0.74, 95% Cl: 0.64–0.85), (RD: 3.2%; OR = 0.86, 95% Cl: 0.78–0.96), (RD: 9.1%; OR = 0.64, 95% Cl: 0.47–0.88), and (RD: 6.6%; OR = 0.73, 95% Cl: 0.69–0.78) respectively). Children from Polish and Gypsy/Traveller backgrounds had around four times higher odds for developing obvious caries (RD: 35.3%; OR = 4.37, 95% Cl: 3.87–4.94) and (RD: 30.2%; OR = 3.47, Cl: 2.52–4.79) respectively compared to their White Scottish peers (Table 2).
P7 oral health outcomes
The unadjusted P7 caries analysis showed no significant differences in obvious caries prevalence between genders or age groups (Table 2). Socioeconomic inequalities continued to persist with children from the most socioeconomically deprived areas having over three times the odds of developing obvious caries compared to children from the least socioeconomically deprived areas (RD: 19.1%; OR = 3.16, 95% Cl: 3.04–3.29). Similarly, children with parents in routine and manual occupations had more than twice the odds of developing obvious caries than those with parents from managerial and professional occupations (RD: 13.7%; OR = 2.41, 95% CI: 2.32–2.50). Children from African, Chinese, Indian and White British backgrounds had lower odds of developing obvious caries compared to White Scottish children (RD: 10.2%; OR = 0.48, 95% Cl: 0.39–0.58), (RD: 4.6%; OR = 0.75, 95% Cl: 0.61–0.92), (RD: 5.8%; OR = 0.68, 95% Cl: 0.57–0.82), and (RD: 3.8%; OR = 0.79, Cl: 0.73–0.85) respectively). Children from Gypsy/Traveller backgrounds had more than twice the odds of developing obvious caries (RD: 22.2%; OR = 2.70, 95% CI: 1.98–3.70), and children from Polish backgrounds also had higher odds (RD: 5%; OR = 1.34, 95% CI: 1.18–1.52) compared with their White Scottish peers. (Table 2).
The transition of obvious dental caries between P1 and P7
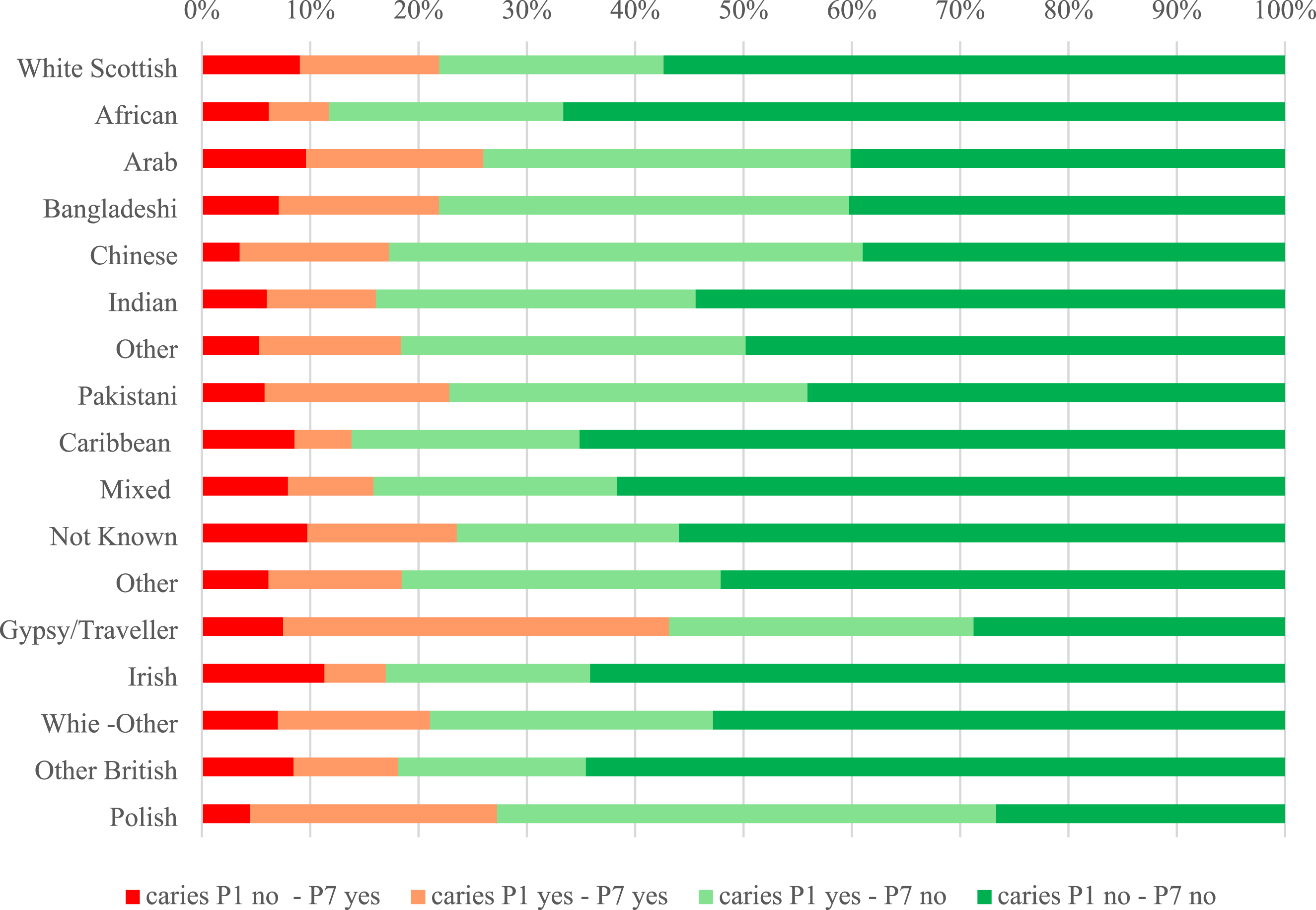
The longitudinal cohort enabled the pairing children’s dental inspection data across four matched NDIP survey periods: 2009/2015, 2010/2016, 2011/2017 and 2012/2018 (Table 1). Data on obvious caries transitions from P1 to P7 categorised into four groups (Table 3, Figure 1) were: (1) Yes obvious caries in P1 and Yes obvious caries in P7 (n = 19,988/12.8%). (2) No obvious caries in P1 and Yes obvious caries in P7 (13,751/8.8%). (3) Yes obvious caries in P1 and No obvious caries in P7 (33,266/21.4%). (4) No obvious caries in P1 and No obvious caries in P7 (88,732/57%) The transition (status) of obvious dental caries between P1 and P7. Children with no caries in Primary 1 and no caries in Primary 7 served as the reference group. aaOR 95% CI: Adjusted odd ratios and 95% confidence intervals, model adjusted by sex, school year, SIMD, SES and ethnicity. b‘*’ Denotes P-value significant level <0.05. The transition of obvious dental caries from P1 to P7 among different ethnic groups.
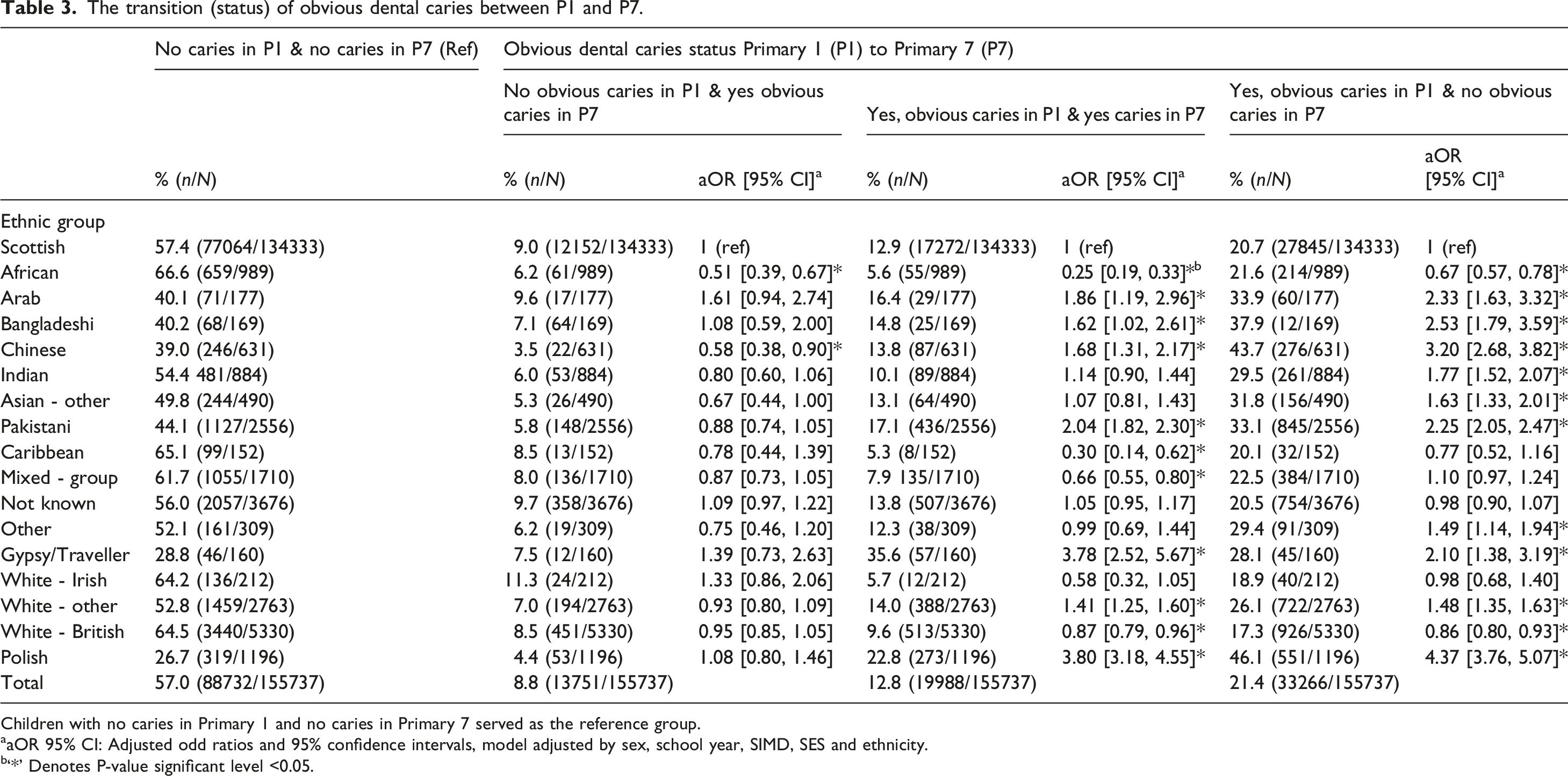
The McNemar test showed that the overall proportion change in obvious caries transition between P1 and P7 was statistically significant (P < 0.05). Separate McNemar tests were conducted for each ethnic group.
The adjusted analysis of changes in obvious caries status from P1 (no obvious caries) to P7 (presence of obvious caries) showed that overall there were no notable differences between White Scottish children and those from other ethnic backgrounds. However, children from African and Chinese backgrounds, were less likely to develop new obvious caries between P1 and P7 ((RD: 2.5%; OR = 0.51, 95% Cl: 0.39–0.67) and (RD: 5.5%; OR = 0.58, 95% Cl: 0.38–0.90) respectively). We observed differences in the improvement of obvious caries status from P1 to P7 among children from Polish, Gypsy/Traveller, Pakistani, and Arab backgrounds. Almost all children from ethnic groups other than White Scottish had improved obvious caries experience from “yes obvious caries in P1” to “no obvious caries in P7”. For instance, Polish and Chinese children had reduced obvious caries experience ((RD: 25.4%; OR = 4.37, 95% Cl = 3.76–5.07) and (RD: 23.0%; OR = 3.20, 95% Cl = 2.68–3.82) respectively) (Table 3).
Association between obvious caries experience in primary 1 and obvious caries in primary 7
Obvious caries experience in P1 was modelled as associated with obvious caries in P7. In the unadjusted model children with obvious caries in P1 had over three times higher odds of developing obvious caries in P7 (OR = 3.88, 95% CI: 3.79–3.98). After adjusting for sex, school year, SIMD, SES, and ethnicity, obvious caries experience in P1 remained associated with obvious caries in P7 (OR = 3.24, 95% CI: 3.16–3.33).
Attributable risk of socioeconomic factors
The proportion of risk attributable to area-level and individual-level socioeconomic factors show limited attenuation of the ethnicity obvious dental caries associations in P1 and P7 (Supplemental Tables S1 and S2) – suggesting ethnicity particularly in the early years (P1) is a strong independent factor associated with obvious dental caries.
Discussion
This study analysed a large and unique longitudinal cohort, incorporating data on ethnicity, area-based and individual-level socioeconomic status, alongside obvious dental caries outcomes at ages five and 11. The findings for area based socioeconomic deprivation suggest that five-year-old children from the most socioeconomically deprived areas had more than four times higher odds of developing obvious dental caries compared to those from the least socioeconomically deprived areas. These findings were consistent with the findings that were observed in other studies (Peres and Heilmann, 2015; Ross et al., 2023).
When examining individual-level based deprivation indices, five-year-old children whose parents had never worked or were long-term unemployed had over six times the odds of developing obvious dental caries compared to children whose parents held higher managerial, administrative, or professional occupations.
After adjusting for both area-based and individual-level deprivation, five-year-old children of Polish, Gypsy/Traveller, Chinese, Bangladeshi, Arab, and Pakistani backgrounds still had significantly higher odds of experiencing obvious dental caries compared to Scottish White children of the same age. These findings are consistent with earlier published research on the topic, (Conway et al., 2007; Public Health England, 2021; Rouxel and Chandola, 2018), supporting the association between ethnicity and dental caries (particularly in children up to 5 years olds) independently of area-based and individual-level socioeconomic measures.
Among the older children, aged 11 years, those residing in the most socioeconomically deprived areas had more than a threefold increase in obvious dental caries prevalence compared to those living in the least socioeconomically deprived areas. Eleven-year-old children whose parents had never worked or were long-term unemployed had around four times the odds of developing obvious dental caries compared to children whose parents held higher managerial, administrative, or professional occupations. At this age, ethnicity-related inequalities in obvious dental caries were no longer statistically significant, with the exception of children from Gypsy/Traveller and Polish backgrounds. Overall, for children in P7, area-based and individual-level measures of deprivation were more strongly associated with obvious dental caries than ethnicity. Comparable findings have been reported by Rouxel and Chandola (2018) who observed similar patterns in their study. Children’s oral health in Scotland has shown sustained year-on-year improvement, a trend widely attributed to the introduction of the national oral-health improvement programme Childsmile. This programme delivers a suite of universal, evidence-based interventions, including supervised daily toothbrushing and fluoride varnish applications in nurseries and schools, community-based support from dental health workers, and routine preventive care within NHS primary care dental practices. Collectively, these components have demonstrated a substantial impact in reducing obvious dental caries among children across Scotland (Kidd et al., 2020). Improvements in dental obvious caries among some ethnic groups may reflect the early benefits of the Childsmile programme and its role in reducing oral health inequalities. In addition to this, another factor might be acculturation, as families who have been settled in Scotland for longer may gradually adopt the host country’s dietary patterns and health-seeking behaviours including greater engagement with dental care services.
Analysis of changes in obvious caries status from P1 (no obvious caries) to P7 (presence of obvious caries) revealed no significant differences between White Scottish children and those from other ethnic backgrounds, except for children from African and Chinese backgrounds, who were less likely to develop obvious caries over time. Significant differences were observed in the persistence of obvious caries from P1 (obvious caries present) to P7 (obvious caries present) among children from Polish, Gypsy/Traveller, Pakistani, Arab, Bangladeshi, Chinese, and White - Other backgrounds. These findings were similar to those reported by (Hall-Scullin et al., 2017). A notable positive (improving) transition from obvious caries in P1 to obvious caries-free status in P7 was observed across nearly all ethnic minority groups when compared to their White Scottish peers. Consistent with previous studies (Hall-Scullin et al., 2017; Lam et al., 2022), the presence of obvious caries in deciduous teeth in P1 at is strongly associated with obvious caries in the permanent dentition in P7, with affected children being over three times more likely to experience this obvious caries progression.
A key strength of this study lies in its use of large, routinely collected national administrative datasets, enabling robust record linkage within a population-based cohort. The study benefits from the inclusion of both area-level and individual-level socioeconomic deprivation measures, as well as ethnicity data reported by parents or carers through the annual national school census. However, there are a number of limitations to consider. Individual-level socioeconomic data were not available for children born outside of Scotland, as parental occupation was recorded only at the time of birth registration. Ethnicity data were reported annually based on parental input. In around 0.2% of the cases, parents changed the reported ethnicity over time; therefore, we used the most recent entry (Public Health Scotland, 2025c). Some ethnic groups had small sample sizes, resulting in wider confidence intervals. To preserve the uniqueness of each group, we avoided aggregating heterogeneous ethnic groups (Public Health Scotland, 2025c). To address missing data on ethnicity, we excluded the small proportion of children (approximately 1%) for whom ethnicity was not recorded, rather than creating a separate “unknown” category. This decision was made to avoid potential misclassification and because the number of missing cases was too small to support meaningful interpretation. Obvious dental caries data were derived from the robust basic NDIP assessment, which uses a binary variable of obvious caries prevalence (presence or absence of obvious caries) rather than a measure of severity (eg DMFT) from a comprehensive dental examination (Macpherson et al., 2017). It is important to acknowledge that we took a pragmatic approach of using a binary outcome of obvious caries/no obvious caries for the purposes of this analysis. The transitions from obvious caries in P1 to no obvious caries in P7 do not represent reversal of disease but reflect the exfoliation of primary teeth affected by obvious caries and their replacement by obvious caries-free permanent teeth.
There was limited attenuation of the relationship between ethnicity and caries experience observed in this study. This could be a limitation of the area-based socioeconomic measure and the parental occupational socioeconomic status at birth. There could be residual confounding in the relationship and socioeconomic factors such as household income/wealth, social security payments, and parental employment/education could still be important explanatory factors.
These findings may support policy makers in further strengthening prevention interventions that are targeted to address determinants of oral health inequalities beyond socioeconomic class and consider interventions that are culturally competent for all ethnic groups. Further research may provide more in-depth exploration on the reasons for these inequalities and consider barriers and facilitators for accessing oral health improvement as well as nutrition and diet programmes and access to dental care services.
Conclusion
At age five, the prevalence of obvious dental caries was significantly higher in most minority ethnic groups than among White Scottish children, independently of socioeconomic factors. By Age 11, ethnicity-related inequalities were less pronounced, with the exception of children from Gypsy/Traveller and Polish backgrounds, and socioeconomic factors were the main drivers of oral health inequalities in this older child age group.
Supplemental material
Supplemental material - Associations between ethnicity, socioeconomic status and dental caries in children: A population-based record linkage longitudinal cohort study
Supplemental material for Associations between ethnicity, socioeconomic status and dental caries in children: A population-based record linkage longitudinal cohort study by Ahmed Mahmoud, Stefan Serban, Alex D. McMahon, David I. Conway in Community Dental Health
Footnotes
Acknowledgments
The authors gratefully acknowledge the support provided by the Electronic Data Research and Innovation Services (eDRIS) at Public Health Scotland, the Indexing Team at National Records of Scotland, and the data contributors from the Dental Team at Public Health Scotland.
Ethical considerations
The study received ethical approval from the West of Scotland Research Ethics Service (WoS ASD 980).
Author contributions
DIC, AM, and ADM conceptualised the study and developed its design. AM coordinated data requests, secured study approvals, and established data sharing agreements. AM carried out the data management, while AM and ADM conducted the analysis and generated the figures and tables. The initial manuscript draft was prepared by AM and SS. All authors contributed to the critical review and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scottish Government through funding for the evaluation of the Childsmile programme (Scottish Government Health Directorate – Evaluation of National Oral Health Improvement Programmes, 2013–2016, 2016–2019). It also forms part of a part-time PhD studentship sponsored by Public Health and Intelligence, initially funded by National Services Scotland.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Study permissions
The study was granted ethical approval from the West of Scotland Research Ethics Service (WoS ASD 980). In addition, the study received approval from NHS Scotland Public Benefit and Privacy Panel for Health and Social Care approval no. 1516-0368 and amendment approval no. 1819-0227.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.