
Abstract
Keywords
Introduction
The higher burden of dental caries of the primary dentition and lower access to preventive dental services among children from more disadvantaged backgrounds is well described in the literature (Kassebaum et al., 2017; Peres et al., 2019; Public Health England, 2020; Watt et al., 2018) and these inequalities are considered a global public health challenge (World Health Organisation, 2022). These socioeconomic inequalities in poor oral health have also been shown to intersect with and be compounded by disability for children with additional support needs (ASN) – including children with intellectual disabilities, autism, and other educational ASN manifesting in the preschool and early years of school (Authors, 2023).
Less is known about the oral health and access to dental services among older children with ASN as they transition from primary to secondary education; from deciduous to permanent dentition; and from child to adult healthcare services. Several reviews in this area have called for larger, greater quality, better designed studies to understand the oral health and oral healthcare needs of this population (Barbosa et al., 2022; da Silva et al., 2017; Erwin et al., 2022; Lam et al., 2020; Ningrum et al., 2021; Robertson et al., 2019; Ummer-Christian et al., 2018; Zhou et al., 2017). Only one recent national population health insurance database study was identified, from South Korea, of all children under 19-years-old which reported fewer dental visits, and more severe and costly dental treatments among children with autism compared to those without autism (Baek et al., 2024).
The aim of the study is to investigate rates of tooth extractions under general anaesthesia in hospital and access to primary care dental services among young people with educational ASNs attending secondary school compared to those with no recorded ASN.
Methods
Study design
Young people in the five secondary school year cohorts in Scotland: 2011/12, 2012/13, 2013/14, 2014/15 and 2015/16 were followed from their 12th birthday (S1-typical age of entry into secondary school) until their 16th birthday (S4-is the final year of mandatory secondary schooling) linking three national administrative, health and education datasets at the individual-child level.
Databases
(1) Pupil Census: the Scottish Government (Scottish Government, 2021) is Data Controller and collects data annually on all pupils attending local authority (state) schools (including special schools) - and records data on whether a pupil has any educational additional support needs. (2) Scottish Morbidity Records 01 (SMR01): Public Health Scotland (Public Health Scotland, 2020b) is the Data Controller and collect hospital admissions data on every patient attending NHS hospitals, including those admitted for a tooth extraction under general anaesthetic. (3) Management Information and Dental Accounting System (MIDAS): Public Health Scotland (Public Health Scotland, 2020a) is the Data Controller and is the system whereby General Dental Practitioners are paid for delivery of NHS services. This records NHS services provided by general dental practitioners (high street dentists) and the Public Dental Service (PDS).
Data linkage
Data linkage of the three databases above was facilitated by the electronic Data Research and Innovation Service (eDRIS) hosted within Public Health Scotland and has been described in detail elsewhere (Authors, 2023). Stringent data disclosure procedures were in place, and all analyses were conducted within the National Safe Haven.
Additional support needs status
The World Health Organization (WHO) defines intellectual disabilities as “impairments in adaptive functioning, social functioning, and intellectual functioning (IQ < 70), requiring a need for daily support, with the onset in the developmental phase (<18 years)” (International Association for the Scientific Study of Intellectual and Developmental Disabilities, 2025). Autism Spectrum Disorders (henceforth autism) is defined as “a diverse group of conditions that are characterised by some degree of difficulty with social interaction and communication and atypical patterns of activities and behaviours, such as difficulty from one transition to another” (World Health Organisation, 2025).
ASN categories were classified according to a previous study (Authors, 2023): (i) Intellectual Disability; (ii) Autistic Spectrum Disorder (autism); (iii) ASN associated with social issues:- “Social ASN” which included pupils flagged with at least one of the following: Interrupted learning, English as an additional language, Looked after, More able pupil, Communication support needs, Young carer, Bereavement, Substance misuse, Family issues, Risk of exclusion, Not disclosed/declared, Other. and (iv) “Other ASN” which included pupils flagged with at least one of the following: Dyslexia, Other specific learning difficulty, Other moderate learning difficulty, Visual impairment, Hearing impairment, Deafblind, Physical or motor impairment, Language or speech disorder, Social, emotional & behavioural difficulty, Physical health problem, Mental health problem. A young person was defined to have an ASN if any ASN was recorded between the age of 12 and 16 years by the Pupil Census. The comparator group comprised the children with no recorded ASN on the Pupil Census between 12 and 16 years of age.
Primary outcome
(i) Tooth extraction (due to decay) under general anaesthetic (from 12 to 16 years). (Obtained from SMR01). (a) Dental General Anaesthetic (DGA): yes/no
Secondary outcomes
(i) Attendance at NHS primary dental care. (Obtained from the MIDAS dataset) which included General Dental Service (GDS) and Public Dental Service (PDS). (a) Ever/Never attended between 12 and 16 years of age (b) Regular attendance (attended at least once every school year between 12 and 16 years)
Census year, sex (Male/Female), area-based socioeconomic circumstances (derived from the Scottish Index of Multiple Deprivation SIMD (2012) using fifths of the data zone distribution from SIMD1-20% most deprived areas to SIMD5- 20% least deprived areas) (NHS National Services Scotland, 2017) and type of school provision (secondary, special school) were considered putative confounders.
Statistical methods
For all three outcomes, Modified Poisson regression models with a log link function and robust standard errors were used and unadjusted and adjusted risk ratios and 95% confidence intervals were calculated for each of the four ASN categories (Intellectual disability, Autism, Social, Other) using the “no ASN” category as reference. All models were adjusted for the possible confounders above. Results were presented by pooling the cohorts for all outcomes, as sensitivity analyses showed little difference across cohorts. Sample weights were not used in these analyses. All linked data were analysed using R (R Core Team v1.2.1335, 2019) within the National Safe Haven.
Results
Characteristics of the full cohort of children in Scotland aged 12-16 years (between 2011/12 to 2015/16) according to ASN classification.
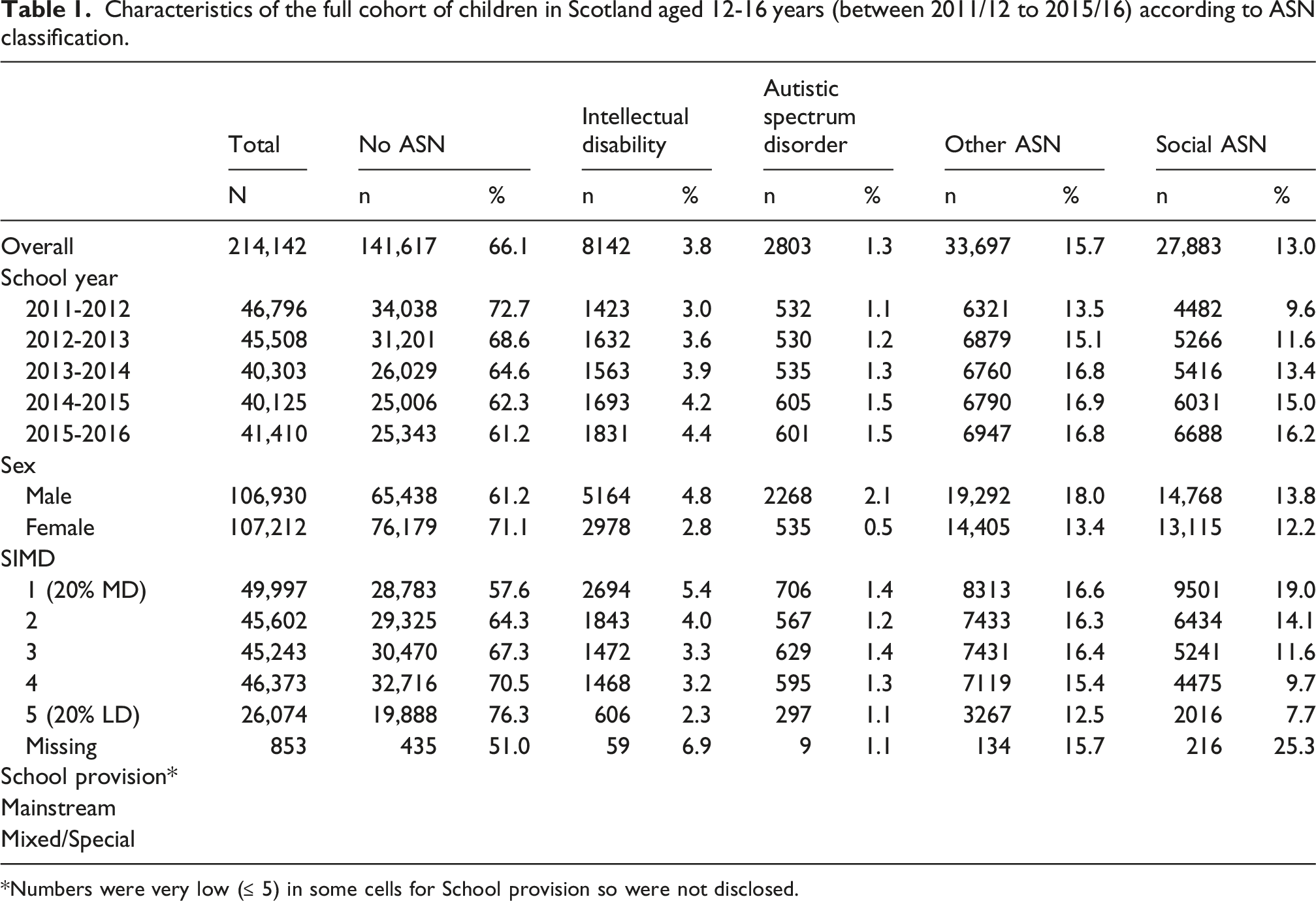
*Numbers were very low (≤ 5) in some cells for School provision so were not disclosed.
Dental general anaesthetics (DGA)
Hospital admission for tooth extractions under general anaesthetic among children aged 12 to 16 years in Scotland between 2011/12 to 2015/16 according to ASN status. Unadjusted and adjusted risk ratios and 95% confidence intervals.
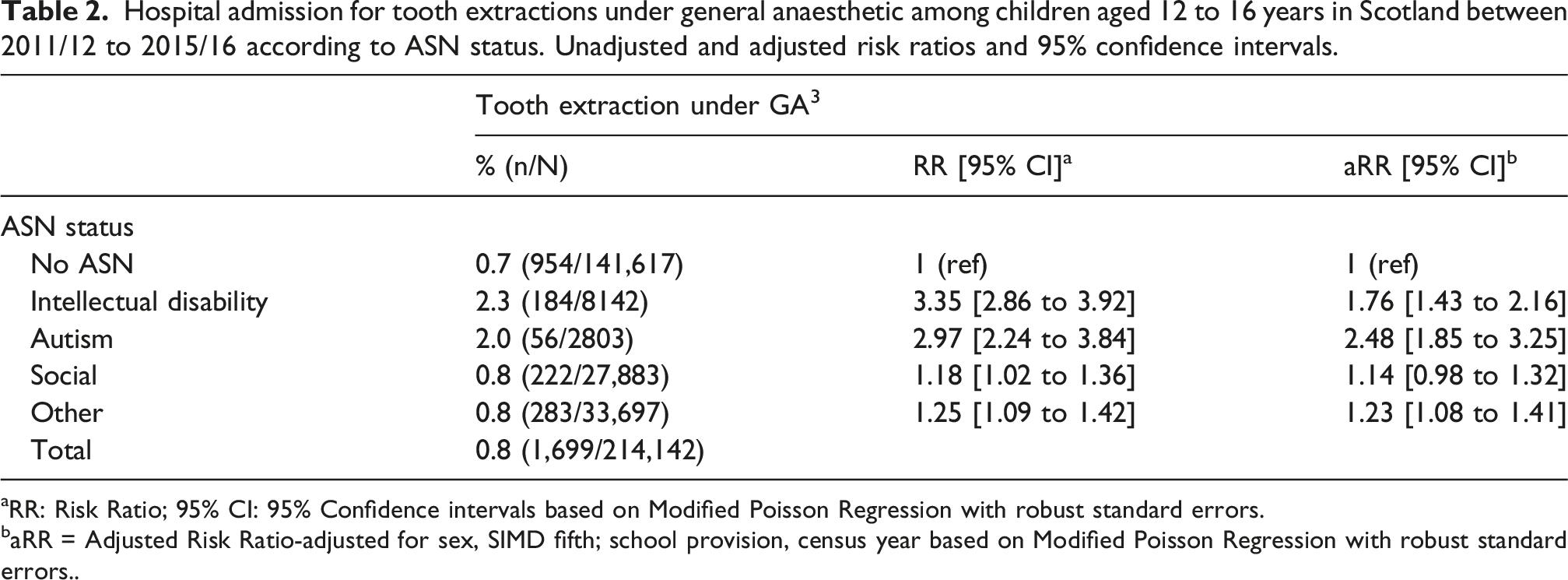
aRR: Risk Ratio; 95% CI: 95% Confidence intervals based on Modified Poisson Regression with robust standard errors.
baRR = Adjusted Risk Ratio-adjusted for sex, SIMD fifth; school provision, census year based on Modified Poisson Regression with robust standard errors..
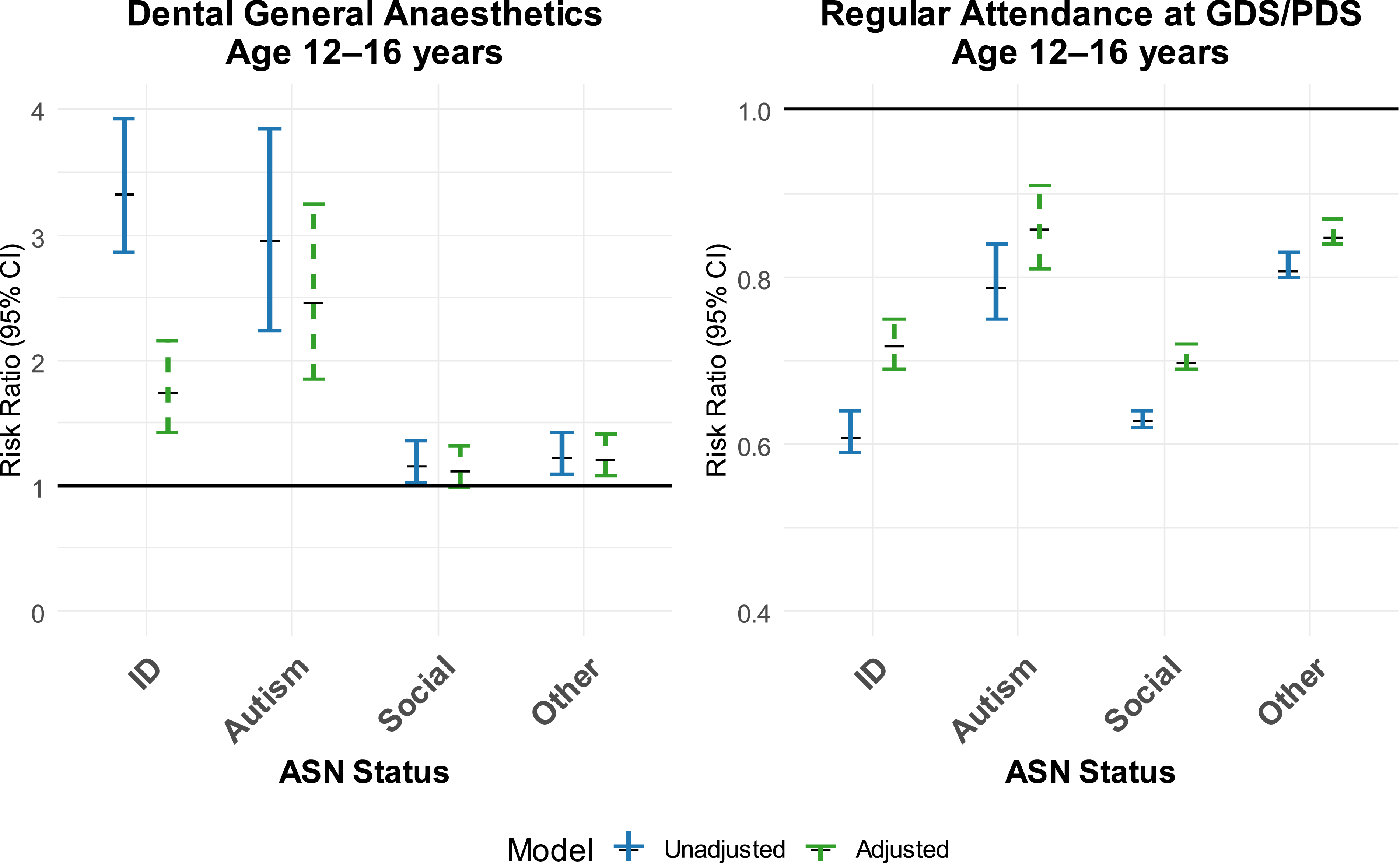
Regular attendance at NHS dental primary care and hospital admission for tooth extractions under general anaesthetic among children aged 12 to 16 years in Scotland between 2011/12 to 2015/16 according to ASN status. Unadjusted and adjusted risk ratios and 95% confidence intervals.
Attendance at NHS primary dental care
Secondary outcomes: Ever attended and Regular attendance at NHS dental primary care among children aged 12 to 16 years in Scotland between 2011/12 to 2015/16 according to ASN status. Unadjusted and adjusted risk ratios and 95% confidence intervals.
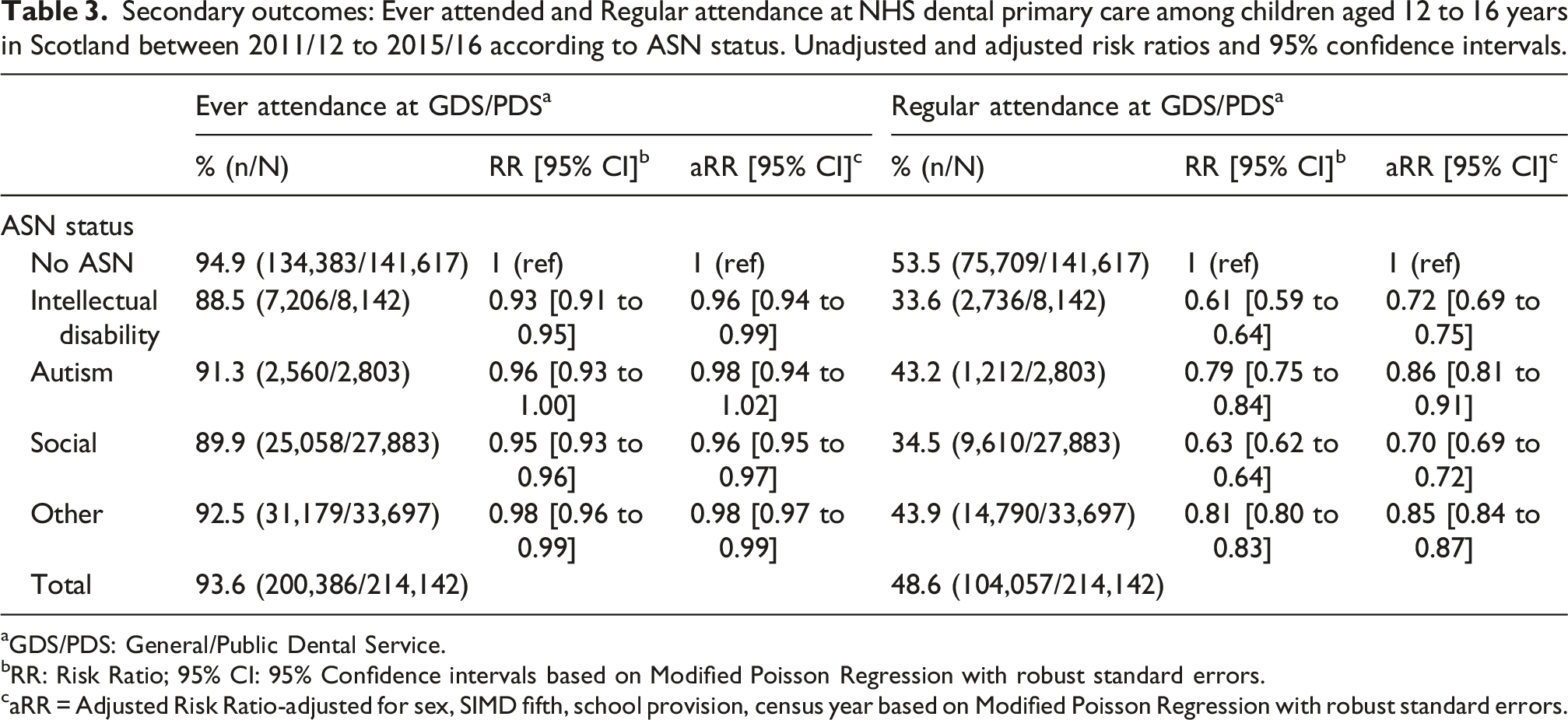
aGDS/PDS: General/Public Dental Service.
bRR: Risk Ratio; 95% CI: 95% Confidence intervals based on Modified Poisson Regression with robust standard errors.
caRR = Adjusted Risk Ratio-adjusted for sex, SIMD fifth, school provision, census year based on Modified Poisson Regression with robust standard errors.
Almost 54% of young people with no ASN regularly attended a primary care dentist during S1 to S4 in secondary school, whereas only 33.6% of those young people with intellectual disabilities or social ASN (34.5%) attended regularly and 43.2% of those young people with autism or an “Other” ASN (43.9%) attended regularly. After adjustment young people with intellectual disability were still less likely to regularly attend primary dental care (aRR = 0.72; 95% CI = 0.69 to 0.75) as were those young people classified as having a “Social” ASN (aRR = 0.70; 95% CI = 0.69 to 0.72). Young people who were autistic (aRR = 0.86; 95% CI = 0.81 to 0.91) and those young people with an “Other” ASN (aRR = 0.85; 95% CI = 0.84 to 0.87) were also less likely to regularly attend primary dental care, but to a lesser extent.
Discussion
This is the first and largest population-wide cohort study investigating hospital admissions for tooth decay and primary dental care access among young people with educational ASNs in secondary school (aged ≥12 years). It follows on from an earlier study on younger children (aged 5 years) from the same population using a similar methodology (Authors, 2023). The risk of DGA was more than twice as high among autistic young people and 1.8 times higher among young people with intellectual disabilities in comparison to those with no ASN after adjustment for area-based socio-economic deprivation - despite concerns of complications associated with general anaesthesia (Choi and Doh, 2021) and the lifelong consequences of losing permanent teeth. It should however be acknowledged that in certain circumstances, DGAs may be the least traumatic treatment option for the patient. Although we cannot rule out the possibility that reduced access to preventive services may be one reason for higher risk of DGAs, the causes are likely to be multifactorial and more complex. Rates of DGA among young people (≥12 years) with a “Social” or “Other” ASN were similar to those with no ASN. This contrasts with findings in a previous study (Authors, 2023) that rates of DGA among children (aged 5 years) with “social” or “other” ASN were higher than those with no ASN, possibly suggesting a change in the management of these patients as they transition from deciduous to permanent dentition.
Regular attendance at primary dental care was slightly higher in the older age groups for all ASN categories and those with no ASN, when compared to 5 year old children from the same population (Authors, 2023), however young people (12 + years) with any ASN were still less likely to attend primary dental care regularly compared to those with no ASN, suggesting potentially similar barriers in access to services among children with ASN across childhood and adolescence.
A number of complex and multidimensional barriers have been identified in the literature that can explain the finding of reduced access to regular primary dental care among children and young people with ASN (da Rosa et al., 2020) - these included: difficulties in physical access; lack of knowledge about disability issues; and dental practitioners having limited experience and skills in looking after children with intellectual and developmental disabilities (Ummer-Christian et al., 2018). These same barriers were also specifically highlighted in relation to the delivery of dental care for autistic children and adolescents – compounded by reported negative attitudes of dental health professionals towards children and young autistic people and their parents/carers (Erwin et al., 2022). The latter finding is also observed in a review on barriers to the utilisation of dental care services among children with special needs (Krishnan et al., 2020), which also reported that in all the studies reviewed there was a general reluctance by dentists to treat children with special needs (e.g. ASN), but also that fear of dentists among children with special needs was a considerable barrier (Krishnan et al., 2020). It is also clear from the lack of literature that far more work is required on the facilitators of delivering regular preventive dental care services to this group of children and young people. The Scottish Government’s recent reform of the NHS primary care dental payment system providing enhanced capitation payments to cover the additional time involved in providing dental care to children and adults with additional support needs may help to address this in Scotland (NHS Scotland, 2023).
Strengths and limitations
Although this study is a population wide study using high quality routine administrative databases, there are some known limitations in the Pupil Census database. Only children from state schools are represented, and those children from public (fee paying) schools or who are home schooled are excluded. Combined, this is estimated to be around 5% of the population (Fleming et al., 2021) and is unlikely to have skewed the results significantly. The recording of ASN status is high quality, however nothing is known about the diagnosis or severity of the conditions recorded. This heterogeneity may dilute our findings for some groups of young people. The MIDAS data is high quality and highly complete as this is the source through which dentists are paid for NHS service provision, however it is limited in the detail it provides on the treatments recorded.
There could be under-reporting of primary care dental contacts among young people with additional support needs who attend NHS primary care dental care services in Scotland. During the timeframe of this study, the Public Dental Service PDS was established in NHS Scotland in 2014. This change merged health board delivered Community Dental Services which had a specific remit for care for those with additional support needs and the Salaried General Dental Services which had a role in addressing areas where access to dentistry was problematic. Before this change only the salaried GDS data were in the primary care dental data available, following this change - in theory - both Salaried GDS and former CDS data would be captured in the primary care dataset. However, we did not observe a shift in contacts as a result of this change and similarly there was no step change in the national statistics on dental registration and participation (contacts) as a result of the merger. This possibly indicates under-reporting of data related to those with additional support needs both prior and post 2014.
The hospital admissions database (SMR01) is highly reliable but is restricted to NHS hospitals and does not cover private treatment, however for young people still at school, private medical provision is rare. Additionally, SMR01 does not record the reason for a procedure/operation and particularly for tooth extraction does not record the number of teeth extracted. Again, for young people this is possibly less of a limitation than for adults where tooth extraction may be for reasons beyond that of simple decay.
Conclusions
Young people with ASN in secondary schools in Scotland have a higher level of dental general anaesthetics and lower access to regular primary dental care than their contemporaries with no recorded ASN. This is particularly observed among autistic young people and those with intellectual disabilities. Improving access to primary dental care including provision of preventive or earlier interventions is important and recent NHS dental service payment reforms in Scotland are welcome and could be important in this regard. In relation to primary prevention, additional school-based oral health improvement interventions particularly focused on daily supervised toothbrushing in both mainstream primary schools (ensuring they are inclusive for children with additional support needs) and in Additional Support for Learning (“special”) schools including secondary schools should be considered. Further efforts are needed to develop and improve preventive care pathways and integrate oral health to wider healthcare systems for these vulnerable children and young people – both before and through the transition to adult services.
Footnotes
Acknowledgements
The authors acknowledge the support of the electronic Data Research and Innovation Services in Public Health Scotland and the Indexing Team in National Records Scotland along with the data providers in Dental Team in PHS.
Ethical consideration
Ethical approval was obtained from the University of Glasgow Ethics Committee (Project number MVLS200150076). This study received approval from the NHS National Services Scotland Privacy Advisory Committee and Public Benefit and Privacy Panel - Approval no.1617-0302 Amendment Approval 2019 09 04.
Author Contributions
DIC, AS conceived the idea of this study. DIC, AS, DC, AH designed the study. DIC prepared data requests and study approvals and data sharing agreements. RS, KD and RY undertook data management. RS, KD, RY, LD with AS performed analysis and prepared figures and tables. WW and LD undertook literature review. AS, WW prepared first draft of the manuscript. All authors critically reviewed and approved final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Baily Thomas Charitable Fund (No. 4998-7964). The study funder had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
We applied for approval to access, link, and analyse the study data within the NHS national safe haven environment and undertook information governance training. The data generated, linked, and analysed during the study are not publicly available. The data controller for all health data is Public Health Scotland, and researchers can apply to access [via email: