
Abstract
Introduction
People are living longer than ever before, which can enhance quality of life and well-being (World Health Organization [WHO], 2021). However, it also poses challenges, as increased life expectancy leads to a higher prevalence of age-related diseases like stroke, dementia and cancer. Consequently, a significant portion of the population will require care, support and preventive measures to maintain a good quality of life. Currently, half of Sweden’s population over the age of 65 has two or more chronic diseases, and this proportion increases to 80% among those aged 85 or older (National Board of Health and Welfare, 2020).
Oral health is a vital part of general health and encompasses basic functions like speaking, chewing, smiling and swallowing without pain (Glick et al., 2017). It is influenced by societal and cultural norms, as well as by individual perceptions. Improved living conditions and healthier habits have led to better oral health among the Swedish population, with more older adults retaining their teeth into old age (Norderyd et al., 2015). However, in the event of the onset of frailty, oral health is at risk of being neglected. Motor and cognitive impairment can make daily oral self-care more difficult, for example by not being able to perform it physically or simply forgetting to do so (Grönbeck Lindén et al., 2017). An additional factor that can make it difficult to maintain good oral health is medication, which can cause dry mouth, which in turn increases the risk of tooth decay (Barbe, 2018). Frail individuals may struggle to visit dental clinics due to energy constraints, frequent medical appointments and financial barriers (Derblom et al., 2017; Grönbeck-Linden et al., 2016). These challenges can lead to lost dental care contact and rapid deterioration in oral health, impacting their overall health and quality of life. Declining oral health is not necessarily limited to pain and discomfort from the mouth but can also have significant consequences for general health and, not least, quality of life.
Studies have shown that loss of regular dental care contact among older adults is associated with poorer oral health outcomes, including untreated caries, periodontal disease, and tooth loss (Petersen and Yamamoto, 2005; Holm-Pedersen et al., 2005). In Sweden in 2019, those aged 70–74 years were the age group that visited dental care most frequently (Dental and Pharmaceutical Benefits Agency, 2024). From the age of 75 and upwards, however, dental visits gradually began to decrease with age. Likewise, in a study in which more than 4000 patients in old age with regular dental care contact were studied over time, a clear risk of losing dental care contact with increasing age was shown (Grönbeck-Linden et al., 2016). There are several different reasons why frail older adults may lose their contact with dental care. In addition to, for example, lack of energy and aspects regarding mobility, research has shown that dementia diagnoses are a risk factor for missing dental care (Fereshtehnejad et al., 2018). Older adults diagnosed with dementia reduce their contact with dental care from shortly before until shortly after their diagnosis.
Introduction to current practice
In the west of Sweden (Region Västra Götaland), there were 440,000 inhabitants above the age of 60 in 2021, and they constituted about 40% of the population (SCB. Population statistics 2025). The majority of the older adults in the west of Sweden was listed at a private dental clinic. However, about 30% of them were listed as patients in the Public Dental Services. At the time this study was conducted, older people, like the rest of the Swedish grown up population, paid a patient fee for dental care. The cost was partly covered by state support, with higher subsidies for more extensive treatments.
To reduce the risk of older people losing regular dental care contact, a new routine was implemented at 105 Public Dental Service clinics in the west of Sweden in 2017. The goal was to maintain contact with patients who are at risk of losing their dental care contact due to increased age, disease, impairment or lack of energy. The routine aims to enable contact with relatives and/cognitive or care staff, including individualized revision intervals, and offers oral health information (by phone and/or mail) as well as extended fluoride protection by prescription when the patient is unable to visit the dental care clinic. The routine entails that it is noted when patients repeatedly do not show up, cancel their planned dental care appointments or state in a vague way that they will return when they feel better. In their medical record, the patient is enrolled in the routine and regularly followed up by contact via mail and/or telephone to encourage them to visit the dental clinic and inform them about the importance of maintaining good oral health. A conversation guide was provided to facilitate this contact with the patient. The routine also entails that one member of the dental staff at each dental clinic should be appointed as a representative, with the overall responsibility for the routine functioning and being maintained. The representative could be a dental nurse, dental hygienist, dentist, clinic coordinator, administrator or manager. In the Swedish national guidelines for dental care, it is emphasized that dental care clinics should support older adults with frailty in maintaining their regular dental care contact (National Board of Health and Welfare, 2022). However, there is a gap in research about how this should be done, and how to do so in an effective way. Therefore, the aim of the study was to evaluate a routine for maintaining dental care contact for frail older adults – how the routine is used and how it is experienced by dental professionals in Public Dental Service in the west of Sweden.
Material and methods
Study design
The study was conducted in three parts, using a mixed-methods design (Nicolau et al., 2023). The first two parts were of quantitative design consisting of a register study and a questionnaire study, and the third part was a qualitative study using interviews. The register study was intended to find out to what extent the routine was used at each Public Dental Service clinic in the west of Sweden in 2018–2023. Based on the results of the register study, the questionnaire aimed to investigate how the dental care staff used and experienced the routine and whether there were suggestions for improvement. The purpose of the third part, the qualitative study, was to gain a more in-depth understanding of the dental professionals’ experiences of the routine.
Part I: Collection of register data including all clinics within the Public Dental Service in Region Västra Götaland regarding the number of frail patients who had been registered to the routine between 2018 and 2023.
Part II: A questionnaire was sent to one representative at each Public Dental Service clinic, preferably the clinic’s representative for the routine, in March 2021.
Part III: In-depth interviews with staff from 11 clinics in Public Dental Service in June 2021.
Procedure and sample
Part I – Register data
Register data regarding the number of total number of patients (children and adults) and patients aged 60+ were obtained from the Public Dental Service in Region Västra Götaland. This region (population: about 1,800,000) consists of 49 municipalities both urban and rural (population in 2023: min. 4606; max. 608,993). The Public Dental Services in the west of Sweden are the largest dental care service in Sweden, with dental clinics in all the region’s municipalities and a staff of 3200. Between 2018 and 2020, there were 105 public dental clinics in the region. In 2022, two clinics were merged with two nearby clinics, resulting in a total of 103 clinics during the period 2021–2023. Nevertheless, the patient population and clinical staff remained largely unchanged. In 2023 the total number of patients (children and adults) in the 103 clinics was close to 900,000 (mean: 8600, SD 4695, md = 7753, min/max:1840/21882). Register data regarding the number of frail patients aged 60+ was 118,927 in 2018 within the Public Dental Service in Region Västra Götaland. A steady increase was observed over time, with the number rising to 128,858 by 2023.
All Public Dental Service clinics within the region were included in the collection of register data. Data were collected for each year from 2018 to 2023. The data showed the number of patients per clinic registered to the routine and the total number of registrations of individuals within the region, collected in December each year (2018–2023). Data from 2017 were not included in the study since the routine was implemented that year and was only used in the second half (1 July – 31 Dec). The data obtained also included information about the gender and age of those enrolled in the routine.
Part II – Questionnaire
The authors (TF & MI) contacted the managers of all 105 clinics by telephone and/or mail and introduced them to the study and the upcoming questionnaire. One manager declined his clinic’s participation. The intention was that the questionnaire would be answered by each clinic’s appointed representative for the routine. At the clinics where there was no representative for the routine, the clinic manager could suggest another suitable employee to answer the questionnaire. The 104 questionnaires were distributed by email in March 2021. Six questionnaires were not returned. Four respondents were representatives of two neighbouring dental clinics each, and they chose to fill in one questionnaire for both of these clinics. Thus, the questionnaire was answered by 94 respondents, representing 98 different clinics out of 105 possible.
There was no suitable validated questionnaire available for the study, so the authors designed the questionnaire. The questionnaire consisted of 10 questions about how the respondent perceived that the routine was used and how it functioned at the clinic, and also asked whether they had any suggestions for improvement. Questions about the respondents’ profession and whether they were representatives for the routine at the clinic were also included. The questions differed depending on whether the respondent stated that the clinic used the routine or not. On some questions, there was also the opportunity to elaborate their answers in open comment fields. First, the questionnaire was tested by five dental hygienists working in a collaborative intervention with municipal care (Persson et al., 2022b; Persson Kylén et al., 2024b). They were asked to answer the questionnaire and give their views on whether anything was unclear or could be improved. The questionnaire was deemed to be good, and no revision was required after having received the dental hygienists’ responses. The questionnaire was designed in esMaker and distributed by email with attached research subject information. Consent was obtained by answering the questionnaire, which was pointed out in the information. The participants had 3 weeks to answer the questionnaire from the time it was sent out. After 2 weeks, a reminder was sent out to those who had not yet responded to the questionnaire.
Part III – Interviews
For the third part, the interviews, the overall focus was to explore barriers and facilitators for working with the routine. The selection of dental clinics to provide informants was based on the data obtained during Part I as well as on the size and geographical location of the clinics in order to obtain a more strategic selection. The dental clinics were selected based on the number of registrations to the routine in 2019: (1) a significant number of registrations (>100), (2) an average number of registrations (20–50) or (3) few/no existing registrations (<10). Four clinics from each group were asked to participate. Initially, the manager of the selected clinics was contacted by email to approve the invitation of a representative for the routine or another employee to participate. One manager declined the clinic’s participation. In total, interviews were conducted with 12 employees at 11 different clinics: four clinics from the group with “significantly many” registrations, three clinics from the “average” group and four clinics from the group with “few/no” registrations. All of the participants were women; six were dental assistants, three dental hygienists, one a clinic coordinator and one an administrator.
The intended informants were contacted by phone and asked whether they wanted to participate. If they agreed, an appointment was made for an interview. A link to the interview, which was to be carried out online, was then sent out by email along with research subject information and a consent form. The consent form was printed, signed and mailed to the office of a member of the research group (CH). All interviews were conducted digitally in June 2021 via Microsoft Teams. The interviews lasted 20–30 minutes and used a semi-structured interview guide, focusing on barriers and facilitators for the routine. The interviews were recorded with a Dictaphone and transcribed verbatim. One of the authors (TF) was appointed as the interviewer, while another author (MI) acted as the observer, noting non-verbal communication and ensuring that all questions in the interview guide were addressed. During the initial interviews, JPK participated for supervision.
Analysis
Parts I and II – Register data and questionnaire
The register data (Part I) and the data collected from the survey in esMaker (Part II) were transferred and processed in two Statistical Package for the Social Sciences files (SPSS version 21). The data were analysed and presented in the form of frequencies, percentage distributions, mean values (x̄), medians (Md), standard deviations (SD) and maximum (max) and minimum (min) in text, tables and figures. Due to skewed distributions, clinic-level correlates of registration volume were explored using Spearman rank correlations between number of registrations, clinic size, and municipality population size (proxy for urban/rural setting). In Part I sensitivity analyses were conducted to assess the influence of the year 2020 on the results, as registration volumes that year were markedly higher than in other years. All descriptive analyses were therefore repeated after exclusion of data from 2020. Temporal trends in the number and proportion of registered patients were assessed using the non-parametric Mann–Kendall trend test. This method was chosen due to the non-normal distribution of the data. The magnitude of the trend was estimated using Sen’s slope estimator, representing the median annual change over the study period. In Part II, due to highly skewed distributions with extreme kurtosis in the number of registrations for all years (skewness 2.77–5.22; kurtosis 7.80–30.31), and a small number of non-responding clinics, non-parametric Mann–Whitney U tests were used for the non-participation analysis.
Part III – Interviews
The transcribed texts were analysed through qualitative content analysis according to Graneheim and Lundman (Graneheim and Lundman, 2004). To gain a general understanding of the content, the transcriptions were read through individually by the authors. Meaning units that were considered to answer the research questions were identified. The authors then had regular meetings where they compared the meaning units, condensed the meaning units further and identified codes. Using codes and the condensed meaning units as a basis, subcategories were distinguished. These were put in relation to the purpose of the study. Special consideration was given to differences and similarities in the data and to making the informants’ voices heard. Then the subcategories were abstracted and divided into categories. The analysis process took place in an iterative way, based on dialogue between the authors.
Ethical approval
The Ethical Review Authority in Uppsala approved the study (No. 2021-00908). Oral and written research subject information was provided to the participants in Parts II and III of the study. The participants were informed about the design of the study, the possibility to discontinue participation before, after and during the course of the study, and that they would be anonymous in the published results.
Results
Part I
Number of patients (n) registered according to the routine per year and the proportion (%) of these who had more than one registration, as well as mean (x̄), standard deviation (SD), median (Md) and mean/max of number of registrations per clinic and year.
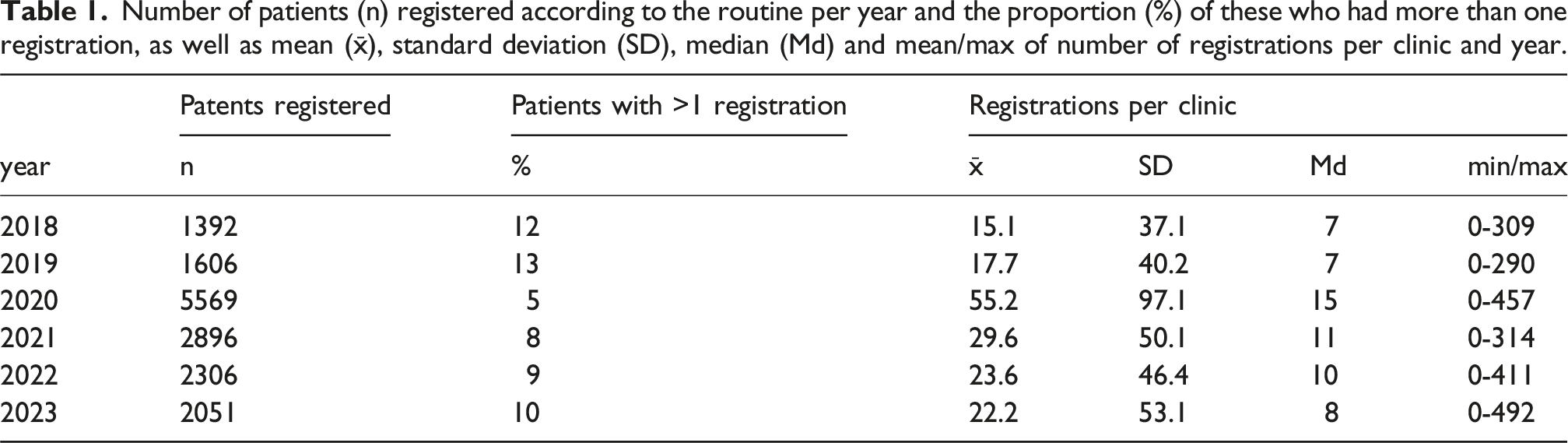
As shown in Table 1, registrations increased sharply in 2020, both in absolute numbers and as a proportion of patients aged ≥60 years, followed by a decline in subsequent years. Mean registrations per clinic peaked in 2020 and were accompanied by substantial between-clinic variation. In sensitivity analyses excluding 2020, registration levels remained relatively stable across the remaining years, with consistently low median values, indicating a right-skewed distribution with a small number of high-registering clinics (Table 1). Despite high mean values, the median number of registrations per clinic remained low throughout the study period.
Trend analyses excluding 2020 showed an increasing but non-significant trend in the annual number of registered patients over time (τ = 0.40, p = 0.21). Sen’s slope estimator indicated a median increase of approximately 214 registrations per year. Similarly, the proportion of registered patients among all patients aged ≥60 years demonstrated an increasing but non-significant trend (τ = 0.40, p = 0.21), corresponding to a median annual increase of approximately 0.1 percentage points.
During the study period, between 57% and 61% of those registered were women. Register data are presented in Figure 1 and show the distribution of the clinics by their number of registrations to the routine from 2018 to 2023. The distribution of the number of public dental clinics (n = 103–105) based on the number of registrations to the routine per year from its introduction in 2018 until 2023.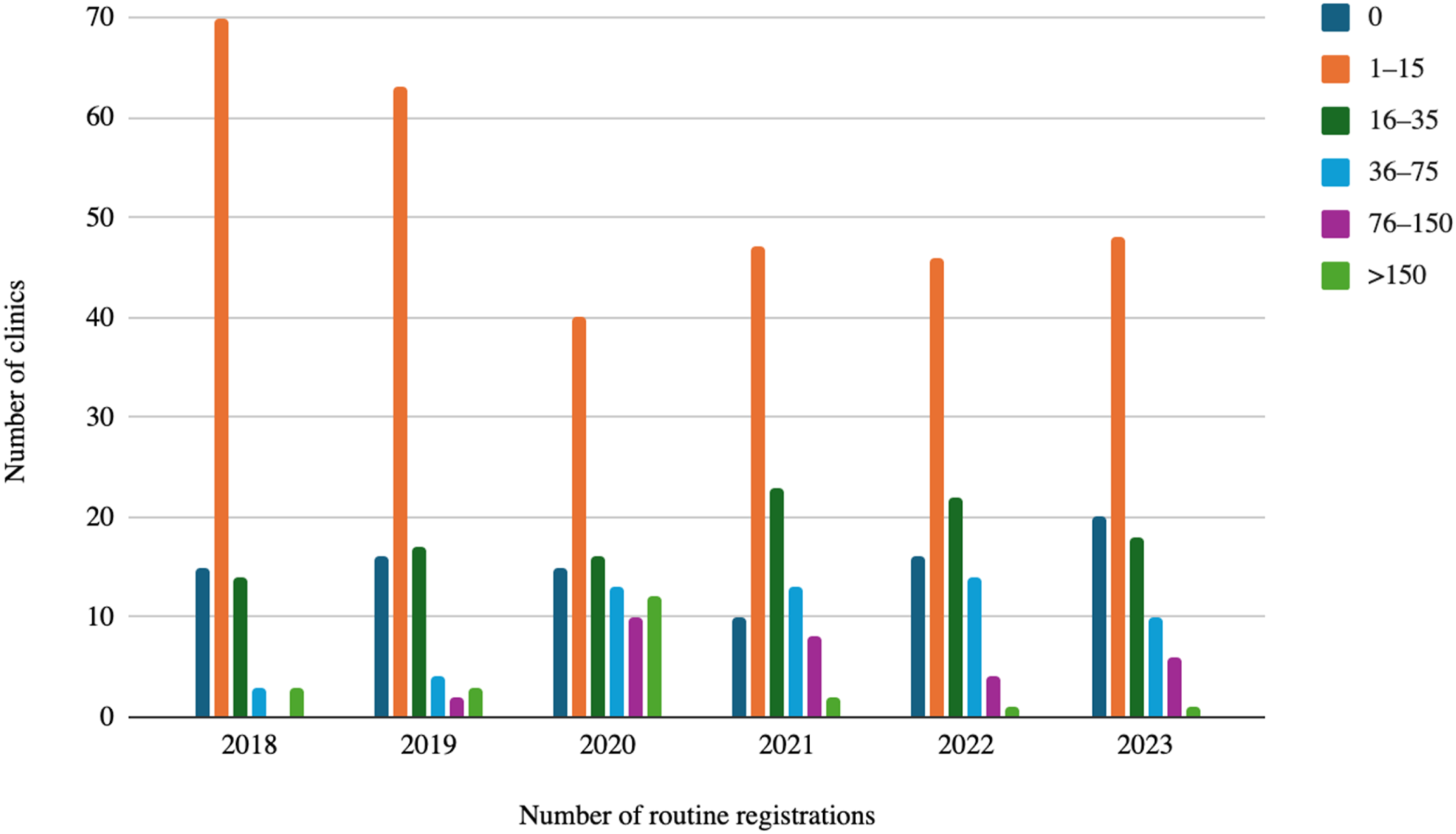
In 2018, there were 20 dental clinics (19%) with more than 15 patients enrolled in the routine and 15 (14%) that did not use the routine at all. In 2020, the number had increased to 50 clinics (48%) with more than 15 registrations, but there were still 15 clinics (14%) that did not use the routine at all. In 2023, there had been a decrease to 35 clinics (27%) with more than 15 registrations, and 20 clinics (19%) did not use the routine at all. Registration volume was weakly but significantly associated with clinic size (Spearman ρ = 0.24, p = 0.016), indicating that larger clinics tended to register more patients. No statistically significant association was observed between registration volume and municipality population size (p = 0.17, p = 0.080).
Figure 2 presents the distribution of the number of individuals enrolled in the routine by age group over the years from 2018 to 2023. The largest number of registrations was in the age group 80–89 years for all years except 2020, when the age group 70–79 years instead made up the largest number. Distribution of registrations to the routine for each year 2018–2023, broken down by age group.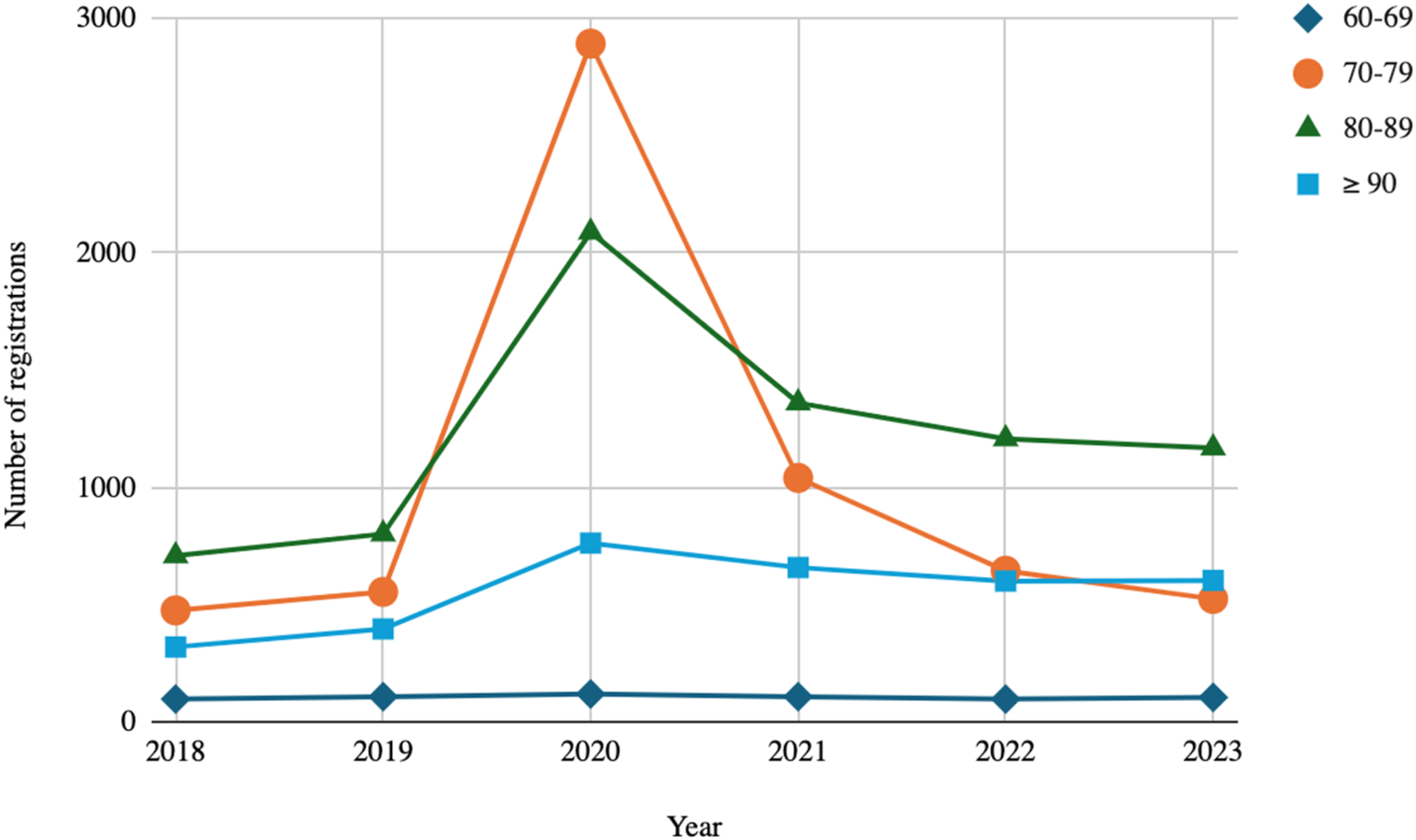
Part II. Questionnaire
The response rate to the questionnaire was 93%, with a total of 94 respondents. In a non-participation analysis, no statistically significant differences were found for the number of registrations to the routine for the years 2018–2020 for the clinics that responded to the questionnaire in March 2021 compared to those (n = 8) that did not or had refused to participate (2018: p = 0.995; 2019: p = 0.772; 2020: p = 0.375). Most of the respondents were dental assistants (n = 58), and dentists were the least common as respondents (n = 2). Additionally, administrators (n = 5), managers or clinic-coordinators (n = 15) and dental hygienists (n = 14) responded. In 82% of the clinics, it was stated that they had a representative for the routine. A majority (75 of the 94 respondents, 80%) stated that they used the routine, to different extents. Of those who stated that they used the routine in their clinic, 75% used it “to some extent”, while a smaller proportion (27%) used it “extensively”. In total, 20% of the respondents stated that they did not use the routine at all in their clinic. Of these, 10% had used it in the past.
The 19 respondents who answered that the routine was not used in their clinic were asked about the reason (response: n = 18). The stated reasons included that the routine was experienced as complicated (n = 1), that they did not know that it existed (n = 2), that they had forgotten all about it (n = 3), that it was not deemed necessary (n = 1), that it was not used due to staff shortages (n = 1), that they used a different method to call frail patients (n = 7) and that the routine had been discontinued in connection with the Covid-19 pandemic (n = 3).
A majority of the respondents at the 75 clinics that used the routine stated that they thought the instructions were clear (71%). The respondents could choose to add an open comment to this question. Of those who left comments (n = 22), seven respondents mentioned that the instructions should be repeated and that the staff should regularly be reminded of it and discuss it at the clinic. A number (n = 5) also responded that there is a need for clearer guidelines regarding which patients should be assessed as “frail”. One respondent wanted clearer and more developed conversation support. Two respondents felt that the instructions in general needed to be clearer.
When contacting patients as part of the routine, the majority (67%) of the 75 respondents stated that they used both mail and phone to reach the patient, while 16% stated that they only used invitation letters and 13% that they only called the patient by phone. Two respondents (3%) did not know which procedure for contact was used at the clinic. Among the respondents, 37% stated that they did not use the routine’s conversational guide at all, 41% that they used the guide on occasion and 12% did not know that it existed.
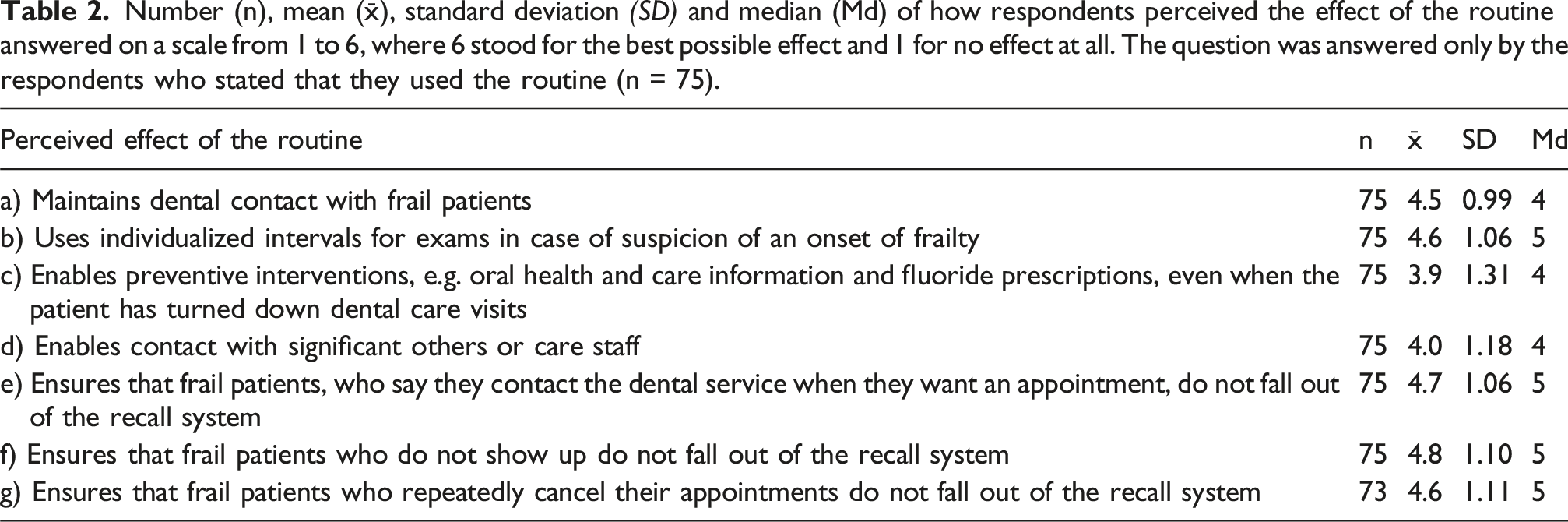
Number (n), mean (x̄), standard deviation (SD) and median (Md) of how respondents perceived the effect of the routine answered on a scale from 1 to 6, where 6 stood for the best possible effect and 1 for no effect at all. The question was answered only by the respondents who stated that they used the routine (n = 75).
A majority (93%) of the respondents at the clinics that used the routine thought that it was good, but 41% thought that it needed to be improved. On this question, the respondents could choose to comment in a free text box, which 29 respondents did. Of these, 15 comments described a need for training and information about the procedure and expressed a wish for it to be followed up regularly and that staff should be reminded of it, for example at work-place meetings, via the intranet or by the clinic management. Six respondents expressed difficulties regarding conversations with frail patients who no longer wished to visit dental care and wanted clearer guidelines on how these patients should be followed up. Three respondents pointed out shortcomings regarding whether or not patients should be called based on their age. A further three respondents believed that the procedure should be simplified and limited in time to reduce the administrative burden that the procedure entails. One comment called for better cooperation with municipal care.
Part III. Individual interviews
Identified categories and subcategories.

Lack of conformity
In the category “Lack of conformity”, three subcategories were identified: “Room for interpretation”, “Creation of own systems” and “Difficulty of identifying target group”.
Room for interpretation
While the participants knew about the routine, none of them stated that they followed it to the letter. Rather, the results indicate the opposite: it seemed to be used more as a foundation from which to make adjustments according to one’s own needs and preferences. I think I’m probably very bad at doing it the same way for all, it probably ends up very different for different ones, you can give them a brochure where you just highlight some sentence.
Several of the participants stated that different strategies from the routine were used based on what they thought was correct in regard to who the patient was, or was perceived to be. Many mentioned that it was important to be responsive in order to reach the patient. The interpretation of the routine and how it should be used varied between different professionals and between the professionals at different clinics. For example, professionals at one clinic had decided to systematically send out several letters per month to patients who were enrolled in the routine, while those at another clinic preferred to call all the patients included in the routine before sending letters by mail. In summary, it can be stated that the routine seemed to be interpreted and used in different ways at different clinics and by different professionals.
Creation of own systems
A number of participants stated that they had alternative methods of maintaining contact with patients perceived as “frail”. Usually, these methods had been in use before the routine was introduced, and it was experienced as difficult to stop using a method which they considered effective, just to implement a new routine. We’ve maybe had some difficulties in transitioning to the new routine there. Before, we always used to write “Health?” in the invitation, that this was someone who refers to their age, disease, disability and difficulty getting here, or who questions whether there is any point at all in still taking care of one’s teeth.
Examples of such alternative methods could be to have the patients with frailty placed on a list for frequent check-up calls, or to set them as a high priority in the call queue. One participant stated that the routine could be useful when one was late and behind in the call queue. Another participant mentioned that they used the same invitation method regardless of age and health status at their clinic; in case of cancellation or no-show, everyone was put up on a list for new invitations in 6 months. All in all, it can be stated that some clinics already used alternative methods to maintain contact with patients who were considered frail, which could make it difficult to implement a new routine.
Difficulty of identifying target group
Many participants experienced it as difficult to identify who should be classified as frail, as there were no clear guidelines within the routine for what it meant. Most participants still had their own thoughts about who falls within the group. Examples of criteria that were used as a starting point were age, diseases/medications, forgetfulness, unwillingness/lack of energy, whether there existed any social support and whether someone had previously had regular dental care but then suddenly stopped showing up. I think that’s difficult … to determine. Uhm. Because, there is no, no specific age, no specific diseases, no specific diagnoses.
One participant stated that the clinic had started to enrol all patients over the age of 80 in the routine, while another participant thought that they focused far too much on chronological age at the clinic when people can be 80 years old and very alert. Several participants mentioned that they used their gut feeling when identifying who was frail.
Dependence on conditions and needs
In the second category, four subcategories were identified: “Concerns someone else”, “Depends on the context”, “Not sufficiently informed” and “Administrative burden”.
Concerns someone else
Some participants mentioned that they did not need the routine as they already had a good overview of their patients with frailty. However, some of them believed that the routine was much needed at other clinics with a wider patient intake. This was mainly expressed by participants who worked at small clinics in smaller municipalities and with low staff turnover, but also by individual participants at more urban clinics. Many expressed that they knew their patients so well that they would notice if they stopped showing up. When you have worked in a place for a long time, you have a really good grasp of the frail patients, after all I meet them maybe every three or four months […] then you miss them when they don’t show up or when they cancel, so you have a close eye on them anyway.
In addition, some participants mentioned that it could happen that they met a relative to a patient with frailty and then could get an update about the patient. A further common denominator for those who felt that they had a good grasp of their patients and did not need the routine was that they perceived that they did not have very many patients with frailty.
Depends on the context
The participants were asked why they thought that the number of registrations to the routine varied that much between different clinics within the region. Many participants mentioned that it could depend on the size of the clinic, the management’s interest in implementing the routine, staff turnover and a lack of consistency between colleagues. Staff turnover was mentioned both in relation to difficulties in getting the routine to settle, and in relation to how it was necessary to have the routine when there was a high turnover of staff to ensure that patients with frailty were not lost. Lack of agreement between colleagues seemed to be common, as several of the participants stated that they handled the routine in a certain way, but that they did not know if their colleagues did the same. No but, partly it’s that the person who’s responsible quits, somebody else is to take over, that takes a while to get into and learn what you’re supposed to do, there’s a lot to read up on routines and things like that … And then I think that it [depends] maybe also a lot on the clinics’ management, how allowing they are that you can sit and work with this, it’s that sort of thing it depends on, too, I think, maybe at a lot of clinics.
Not sufficiently informed
Many of the participants concluded that for various reasons they had not been able to properly familiarize themselves with the routine. One commonly stated reason was that there was a lack of knowledge about the routine and how it should be used. Some participants mentioned that they lacked the time and motivation to fully familiarize themselves with the routine and that it had been pushed aside and forgotten; others said that staff turnover had caused the implementation of the routine to be de-prioritized. It would probably have a different effect if we learned how to handle this, and then it’s quite possible that we would see that it works better. But we don’t have the knowledge and we don’t have the routine as it is today. So if we get that, or learn about it, it’s quite possible.
Some participants felt that they had difficulty expressing their opinion about the routine because they felt that they were not sufficiently informed, and that the routine would probably work better in the clinic if all employees in a better way learned how to use it. Some participants pointed out that the routine seemed complicated, that there was a lot to read up on and that they therefore did not learn it fully. One of the participants said that the clinic manager himself did not know about the routine, and this participant believed that there was a need for a better implementation strategy for the management. One participant stated that it was difficult for her to use the routine because she was not trained in dentistry in the first place. For example, she experienced that it was hard for her to fully have a discussion, from an oral health perspective, with frail older adults about why it was important to maintain their dental care contact.
Administrative burden
Several participants reasoned that the lack of time and the routine being administratively demanding were reasons why the routine was not implemented at the clinic. It turned out that they did not really think the routine was particularly difficult to understand, but rather that it consisted of such a large amount of paperwork and information that they felt it was overwhelming to take on. Many also thought that the routine took up too much administrative time and that there was no room for it in their working day, and that there were too many steps to go through in daily practice. As it is today, it is really time-consuming. Alongside many, lots of patients. It takes a lot of time after all. I understand the idea behind it, getting this contact, but at the same time it is … the time […] I suppose that’s where the problem maybe lies a bit, with such a routine.
Ethical dilemmas
The two subcategories identified in the category “Ethical dilemmas” were “Considering autonomy” and “Considering integrity”.
Considering autonomy
Several participants found it challenging to align the routine with the patient’s right to self-determination. They struggled to determine how often they could contact these patients without appearing too assertive or aggressive. Although the routine recommends regular follow-ups to encourage patients to attend dental care, many informants expressed having difficulties with this approach, especially when patients already had indicated that they did not wish to be contacted further or that they did not want to visit the dental clinic. Several participants thought that in such cases, the patient’s decision, and the fact that the patients do not want to or do not have the opportunity to come, should be respected. I’ve experienced that many older people become angry and think it’s a bother. They have so many other things. Diseases and medical appointments, and they are so tired and don’t have the energy, and then we call as well.
Some participants pointed out that several of the patients were already heavily burdened with so much medical care and other health problems that the mouth was no longer prioritized, and that it felt as though the patients with frailty only were further burdened by the dental care contacting them regularly.
Considering integrity
Several participants expressed concerns about the potential privacy issues involved in obtaining the contact information of the relatives or healthcare professionals of patients with frailty. Some felt it was difficult to ask for this information unless there was a natural opportunity to do so, while others emphasized the challenge of reaching out to relatives or professionals without breaching the patient’s confidentiality. The routine was experienced as somewhat vague regarding support on this issue. … how are you supposed to make this happen, to ask, is there anyone who can help you, maybe one shouldn’t cross this integrity I’m thinking about a little, too. That one shouldn’t be doing this without their consent. These are difficult, kind of … ethical dilemmas I think. That you don’t want to just ride roughshod over a person who is a fully grown adult, who makes their own decisions.
However, some of the participants pointed out that they felt that several patients were grateful when asked if they could contact a relative to help them remember their booked appointment or to get help with transport. The majority of participants asked for closer contact with for example health and care staff to make the care process more integrated for each patient and easier for both the clinic and the patients themselves.
Discussion
This article aimed to evaluate a newly implemented routine for frail older patients maintaining dental care contact in Public Dental Service in the west of Sweden. This was done by exploring how the routine was used and how it was experienced by dental professionals in Public Dental Service. Given the broad aim, the methods used were quantitative and qualitative. Surprisingly, the results revealed a somewhat conflicting outcome, which is hereby discussed.
First, the results from the register data showed that the routine was used to very varying extents. This was visible in differences both between the different dental clinics in the Västra Götaland region during the years 2018–2023 and also within the individual clinics from year to year. Moreover, in line with the outcome of the register data (Part I), the questionnaire indicated that the majority of the staff at the participating clinics used the routine in different ways, and the majority experienced the routine as good. However, the qualitative part (Part III) contributed to nuancing these results. The results revealed that contextual factors seemed to affect the routine in daily practice, and that the use of the routine was associated with ethical dilemmas in relation to older adults with frailty. The main category “ethical dilemmas,” with subcategories “challenging autonomy” and “challenging integrity,” illustrates how staff often struggled with balancing professional obligations and patient rights. Many participants reflected on how difficult it was to respect a patient’s refusal of care in situations where the patient might not fully understand the consequences. Concerns were also raised about how to approach collecting contact information for next of kin or caregivers, without bypassing or disempowering the patient. These reflections point to a need for ethical guidance and support in handling complex situations where frailty, autonomy, and patient dignity intersect (Beauchamp and Childress, 2019).
The qualitative findings (Part III) indicated that staff at smaller clinics in smaller municipalities often described a strong familiarity with older patients with frailty and, in their own setting, perceived the routine as less necessary. This perception was attributed to continuity of care and the belief that deviations in attendance would be readily noticed. At the same time, these participants contrasted their situation with what they perceived to be conditions at larger clinics with broader and more fluctuating patient populations, where the routine was considered to be more needed. In contrast, the register-based findings (Part I) showed a modest association between clinic size and registration volume, suggesting that structural capacity may play a role in implementation, while the urban–rural context appeared less influential at an aggregate level. Even though many participants in the study agreed on the goal of the routine, it seemed to be used in so many different ways that it is difficult to say that there is a common routine for preventing older adults with frailty from losing their previously regular dental care contact. Now, from a perspective of implementation, there are several factors that could be discussed here, and we limit the factors to three overall considerations.
First, research suggests that the implementation of work models in health care settings can take a considerable amount of time, often spanning over a decade (Morris et al., 2011). This indicates that implementation is demanding, and research furthermore shows that new models that are being implemented need to be evaluated and followed over time, with caution (Graham et al., 2006).
Second, national guidelines for dental care in Sweden prioritize models where the dental care organization supports older adults with frailty in not losing their previous regular dental care contact (National Board of Health and Welfare, 2022). Nevertheless, there are, to our knowledge, no dental care organizations in Sweden that have a model that is considered to be “the answer” to this question; rather, it is a work in progress, where small models are tested and evaluated. This is in line with Niesten et al. (Niesten et al., 2021), who state that testing pilot models when developing models for oral health care for older adults is the way forward. Therefore, the Public Dental Service organization in the west of Sweden conducts pioneering work for a frail population. While further research and evaluation are needed, the potential for scaling up promising models like this routine ought to be part of future national strategy discussions. Moreover, both survey and interview data indicated that many dental professionals struggled to define who qualifies as “frail.” While some clinics relied on age, others argued that frailty is not age-dependent. The absence of clear criteria was seen as a barrier to consistent use of the routine. Use of a structured frailty assessment instrument, ideally integrated into existing electronic records, could improve the identification of at-risk patients and help standardize the use of the routine.
This leads us to the final and third point, namely the importance of further integrating dental care into general health care, in line with the global call published in the Lancet (Watt et al., 2019). Older adults with frailty have many caretakers from many care organisations. In the qualitative results, voices were raised, in line with this global call, for integrating the information about older adults entering frailty between healthcare organizations. This is certainly an ethical concern on many levels. While nursing staff in home health care might have access to information about many aspects of personal care, information about oral health care is often lacking (Persson et al., 2022a; Persson Kylén et al., 2024a). However, older adults want to be involved in decision-making about their oral health, and the sharing of information with their surroundings should be individually tailored and person-centred. Some want all information to be shared directly with their significant others and their home health care nurse, whilst others do not want to share any information at all. For future research on a new work model, this will be further developed and tested in a randomized controlled trial (Persson Kylén et al., 2025).
Methodological considerations
During the study period, the mean number of routine registrations per clinic was high, whereas the median was low
Another important limitation is that only aggregate data per year for the Public Dental Service regarding patients aged 60 and older were available. Data on the total number of individuals over 60 years of age per clinic were absent, which makes it difficult to calculate precise rates or coverage measures.
This heterogeneity undermines the comparability of registration data as a metric for how effectively the routine is being implemented. At one clinic, a registration might simply indicate a healthy patient aged 80+, whereas at another clinic it may signal a complex case of frailty in a 60–65-year-old. These divergent interpretations stem from variations in each clinic’s inclusion criteria. Nevertheless, this variability is also a strength, as it exposes the diverse usage patterns of the routine and underscores the importance of context when adjusting protocols for broader use.
The age-stratified data revealed that patients aged 80–89 dominated registrations in all years studied except 2020. This aligns with expectations given that the prevalence of chronic conditions and frailty increases with age (Statistics Sweden, 2022). The lower proportion of registrations in the 90+ group likely reflects the smaller size of that population cohort.
Sensitivity and trend analyses excluding the year 2020 showed stable registration levels across the remaining years, with no statistically significant temporal trends. Against this background, the marked peak observed in 2020 is best understood in relation to the COVID-19 pandemic. A sharp increase in numbers and patients aged 70–79 years accounting for almost half of all registrations. This change appears to be linked to regional pandemic-related regulations; in many regions, routine visits for patients aged ≥70 years were cancelled altogether, as was the case for the clinics surveyed in Western Sweden. Findings from the survey and qualitative interviews suggest that some clinics responded by registering all patients aged ≥70 years according to the routine, regardless of frailty, which may explain the extreme increases observed at some clinics. Conversely, other clinics appear to have stopped registering frail older patients entirely. As a result, data from 2020 are likely confounded by pandemic-related changes in clinical practice and should therefore be interpreted with caution. Data distributions nevertheless remained highly skewed, with substantial between-clinic variation, underscoring the importance of considering clinic-level decision-making when interpreting registry data.
Conclusion
This study shows that while the routine for maintaining dental care contact for frail older patients was generally valued by dental staff, its use varied significantly across clinics and over time, limiting its function as a standardized model. Ethical dilemmas related to autonomy and integrity further complicated its implementation in practice. These findings highlight the need for continued evaluation, ethical guidance, and clearer national strategies. A standardized, nationwide system could support more equitable and coordinated dental care for older adults with frailty.
Footnotes
Acknowledgements
The authors are grateful to all the contributing participants in the study.
Ethical considerations
The Ethical Review Authority in Uppsala approved the study (No. 2021-00908). Oral and written research subject information was provided to the participants in Parts II and III of the study. Informed consent was received from all participants prior to the start of the respective parts of the study.
Consent to participate
The participants were informed about the design of the study, the possibility to discontinue participation before, after and during the course of the study, and that they would be anonymous in the published results.
Author contributions
CH and JPK conceptualized the project. TF and MI conducted the data collection under guidance from CH and JPK. All authors analysed the data, wrote the article and agreed on the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data is available upon reasonable request.