
Abstract
Immigrants in high-income countries experience disproportionately high rates of oral diseases compared to the general population. Existing research largely focuses on biomedical models, individual behaviours or cultural factors providing limited insights into how everyday practices shape oral health outcomes. This study explored how oral health social practices were performed, sustained and/or modified within Indian immigrant families with young children in Australia. A qualitative study was conducted using semi-structured interviews with 17 participants (12 mothers, 5 service providers), using focused ethnography and a social practice theory lens (based on Shove et al.), beginning with inductive coding followed by deductive coding to identify practices and their elements. Social practices such as teeth cleaning/brushing, mouth rinsing, flossing, tongue cleaning and mouth wiping, along with feeding/eating and health advice seeking, along with their elements (meanings, materials and competences) were identified as shaped by intergenerational knowledge of hygiene and care, children wanting to fit in, acculturation and protecting cultural identity. By exploring social practices, and their elements this research offers a new way to engage families into focusing on their everyday routines to understand what supports or undermines performances of oral health related practices rather than solely focusing on persuading individuals to follow recommended behaviours.
Introduction
Oral health in children is fundamental to long-term well-being (The Lancet Child Adolescent and Health, 2019). Research demonstrates that poor oral health in childhood can lead to various health concerns, including developmental and psychosocial issues (Peres et al., 2019). Immigrants from low- and middle-income countries who move to high-income countries, particularly those from South Asia (US Census Bureau, 2024) , experience poorer oral health compared to their host country counterparts (Lauritano et al., 2021). Poor oral health in immigrant children is often discussed in relation to various factors such as acculturation, access to care and oral health knowledge (Nicol et al., 2014) or in relation to socio-cultural norms and behavioural attributes of individuals (Godson and Williams, 1996; Kannan et al., 2004; Williams and Hargreaves, 1990). Previous literature on immigrant communities and oral health have reported that cultural norms (Goossens et al., 2025), such as prioritization of household responsibilities and childcare led to less occurrence of oral hygiene behaviours (Farokhi et al., 2025) and different cultural beliefs such as dental fear, beliefs about primary teeth, and influence of elder family members can have an impact on young children’s access to preventive dental care (Hilton et al., 2007). However, focusing on these factors in isolation, provides limited insights into how oral health is produced through everyday practices.
Despite growing interest in children’s oral health, current research has rarely examined everyday family practices through which oral health is produced within families. This is particularly important in the context of Indian immigrant families, where practices are tied to cultural identity, care, and intergenerational knowledge. Research involving Indian immigrant communities have tended to focus on barriers or influences such as mistrust in dentists, cost of care, limited cultural awareness of healthcare providers about participants’ diets (Newton et al., 2001), language barriers, and cultural differences in oral health perceptions and unfamiliarity with local healthcare systems (Pabbla et al., 2024b). One study that highlighted role of religious practices shaping oral health practices such as mouth rinsing (Kay et al., 1990), however, it did not examine oral health related social practices as interconnected practices involving various aspects of practices. Taken together, existing literature provides valuable insights into contextual challenges faced by Indian immigrants but offer a limited understanding of oral health as a set of everyday social practices enacted and sustained within families particularly in migration contexts.
Current approaches to children’s oral health are largely grounded in biomedical or behavioural models, with subsequent interventions often targeting individuals’ behaviours, access to care and oral health literacy (Dahlgren and Whitehead, 1993; McNeil, 2023). While these approaches have contributed important insights, they offer limited insights into how cultural meanings such as traditional beliefs, dietary customs and intergenerational caregiving roles and shared understandings are enacted in practice. This gap is particularly evident in Indian families, where cultural meanings are often described as beliefs, or barriers rather than examined as part of the everyday routine and materials conditions through which oral health is managed in daily life.
Within an Australian context, Indian immigrants are an important group of South Asian immigrants, numbering over 900,000 nationally and exceeding 70,000 in Western Australia (WA) according to the 2021 census (Australian Bureau of Statistics, 2024). This large-scale migration create conditions in which every day oral health practices may be disrupted, adapted or modified as families navigate new environments, healthcare systems and social expectations negatively impacting oral health (Pabbla et al., 2025; Riggs et al., 2015). Families with Indian backgrounds, with their distinct cultural practices and social norms, provide a rich context for understanding oral health (Arora et al., 2016; Pabbla et al., 2024a). The diverse experiences of Indian families combined with the challenges of resettlement provides a valuable context in understanding how oral health in young children is managed. These limitations suggest the need for an approach that shifts from focusing on individuals and their behaviours to exploring how oral health is managed through everyday caregiving practices.
Social practice theory (SPT) is particularly suited to inform this type of exploration as it focuses on understanding the patterns of daily lives and its implication for health as outcomes of organisation of multiple social practices occurring across space and time (Blue et al., 2016). SPT highlights how collective routines, shared meanings and social norms shape practices (Shove et al., 2012) including health-related practices. SPT has been widely used to inform empirical research focusing on health-related issues. One study on smoking highlights how smoking should be understood as a social practice, not an individual habit and how it is made up of different elements. This study notes that smoking declined when the elements of this practice were modified and not by persuading people not to smoke (Blue et al., 2016). One study on obesity argues that people cannot easily choose ‘healthy habits’ even though they know what is good or even if they feel motivated. Obesity results from normal eating practices which are shaped by work schedules, convenient foods, time pressure and family routines (Blue et al., 2021). Two studies highlight that oral health needs to be understood not as individual behaviours, or parental knowledge but as a part of everyday practices. These studies suggest that children’s oral health care is not a single isolated decision of parents, but they are embedded within routines and shared understandings of routine life. Hence it is important to understand these interconnected practices and see where leverage can be applied to have improved oral health (Durey et al., 2021, 2024).
There are various interpretations of SPT but all revolve around the central idea that social life is made up of different interconnected social practices and not individual actions (Bourdieu, 1977). This study utilised Shove et al.’s interpretation of SPT-proffering that a social practice is made up of a combination of materials, meanings, and competences (Shove et al., 2012). Materials refer to physical objects and physical infrastructure; competences refer to the knowledge and skills required to perform the practice, and meanings refer to the purpose and symbolic significance of doing the practice (Shove et al., 2012). Meanings were a crucial component for this study as it shapes how people perceive a practice, why people engage in a practice and the value they derive from it (Frost et al., 2020; Haslanger, 2018). SPT suggests practices are not stationary but evolve across time (temporal) and space (spatial). The temporal aspect of the practice refers to the different aspects of time, that is, duration, and frequency, while spatial refers to the physical location and geographic context of the practice (Shove et al., 2012). Like meanings, the temporal and spatial aspects of the practices were also crucial for this study as they reveal how practices are situated, reproduced and transformed across different contexts and through time (Shove et al., 2012).
Moving from the limitations of biomedical, behavioural and culture focused approaches, this study aimed to explore how oral health related practices are performed, sustained and/or changed within Indian immigrant families in Australia through Shove et al.’s SPT framework. By focusing on social practices and their elements, rather than solely on individual behaviours or cultural beliefs this research offers new insights into how oral health is produced and maintained in young children. The findings offer an understanding so as to inform culturally appropriate oral health interventions for this population group that aligns with families’ existing practices rather than relying solely on behaviour change focused strategies.
Methods
This qualitative study employed focused ethnography (Knoblauch, 2005; Rashid et al., 2019). Focused ethnography enables the exploration of a defined issue—in this case, oral health-related practices—within a particular community context over a relatively short fieldwork period (Trundle and Phillips, 2023). Semi-structured interviews included questions informed by Shove et al.’s interpretation of SPT to ensure a comprehensive understanding of social practices and their associated elements, including what meanings were ascribed to the practices, how practices were performed and what was used to perform them (Creswell and Poth, 2017). Ethics approval for this study was obtained from The University of Western Australia Human Research Ethics Committee (2021/ET000223)].
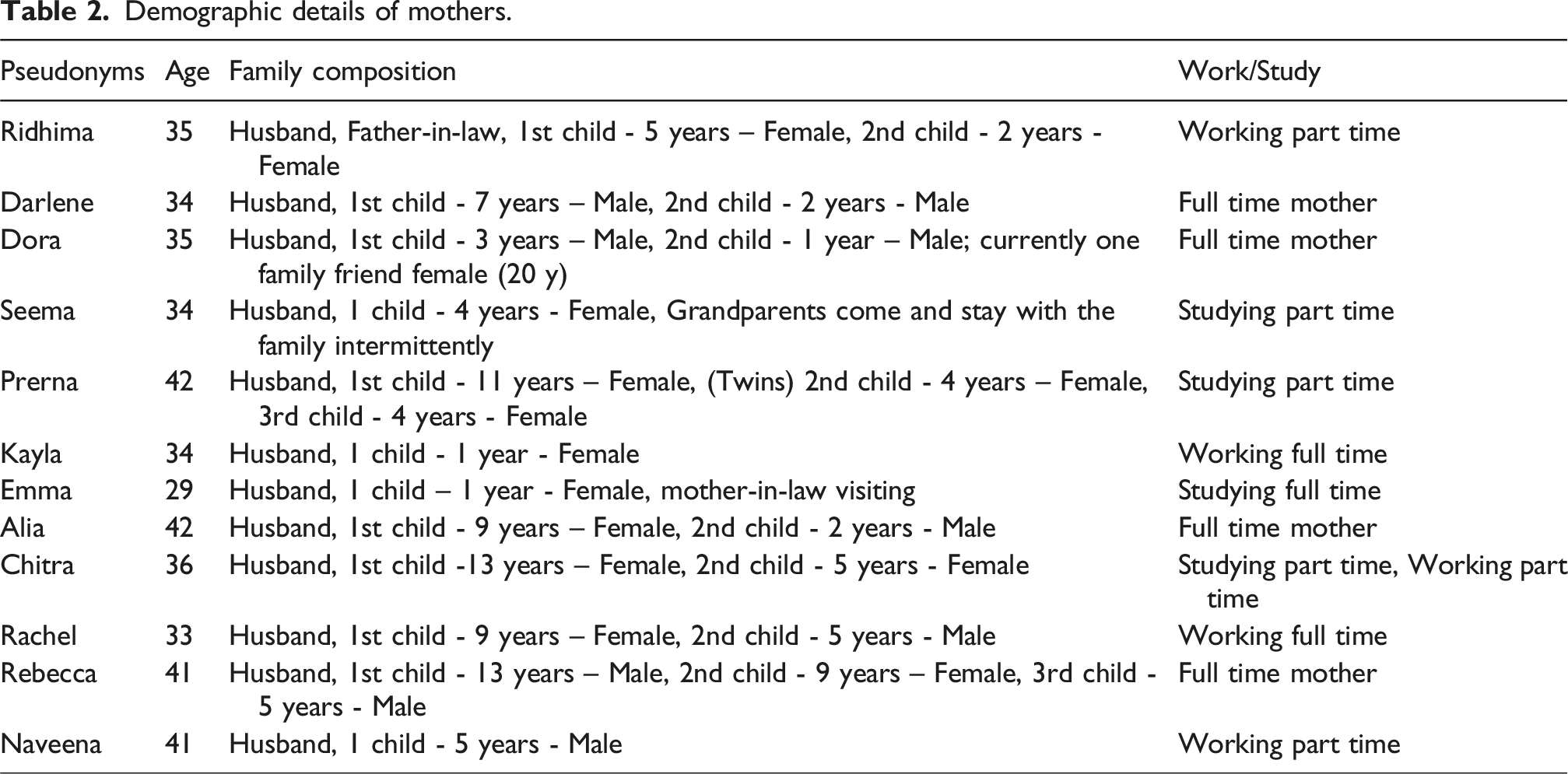
A total of 17 participants were included in the study (12 mothers with Indian backgrounds and five service providers experienced in providing general and oral health services to children from Indian backgrounds). Both groups of participants were purposively recruited through Indian community networks and snowball sampling. Mothers were recruited based on their Indian background, having at least one child aged 0–5 years, living in Perth for at least 5 years, residing in areas of low Socio-Economic Indexes for Areas (SEIFA) (Australian Bureau of Statistics, 2016) and English speaking. A total of 15 mothers were approached for this study. One did not respond to communication, while the other two declined because of the time commitment. After the twelfth interview, no additional significant insights were gleaned, and data saturation - the point where the issue under investigation was fully understood - was achieved. Service providers were recruited based on their experience in working with children from various culturally and linguistically diverse (CALD) backgrounds around oral and general health. The contact details of the service providers were gathered via a professional referral from a known service provider, and after establishing eligibility, they were invited to participate. Signed written informed consent was obtained from participants prior to participation.
Data were collected between November 2023 and August 2024. Following consent, data were collected through semi-structured interviews and observations with mothers and semi-structured interviews with service providers. An interview guide was used. The interview with mothers focused on the everyday routine of families. They were asked about their morning/after-school/night and weekend routines, what children do when they wake up in the morning, what foods children eat at breakfast/lunch/dinner, who cooks using what materials, food shopping routines, and information on dental visits, if any. Observations of the materials in the homes, including contents of the pantry, fridge, kitchen, and oral hygiene essentials in the bathroom, were made; and photographs were taken. This enhanced understanding of interview data and allowed triangulation. Acculturation was considered during data collection where probing questions and examples were asked to clarify what practices were sustained, or modified an/or newly adopted after migrating to Australia.
After interviews with mothers, semi-structured interviews were undertaken with service providers. The main purpose of including service providers in this study was to establish if they provided any information around providing families with information about oral hygiene, feeding, overall health, and ascertain if they introduced new practices, materials or skills to families that may impact children’s oral health. We also sought to understand if the families asked questions about maintaining good oral hygiene, including what to feed, how to brush, floss, or looking after milk teeth thereby again helping to understand their practices and their elements.
A total of 12 interviews conducted with mothers, ten were conducted in their homes, and two were conducted via online video call. During home-based interviews, observations were also conducted to capture materials (e.g., physical infrastructure, food materials, kitchen appliances) and contextual insights. Service provider interviews were conducted at their workplaces (2) and via telephone (3). Interviews were audio-recorded with consent and transcribed verbatim. Notes were taken where audio-recording consent was not provided (four mothers). Interviews with service providers lasted between 20 and 40 min, and interviews with mothers lasted between 60 and 120 min.
An example of coding process.
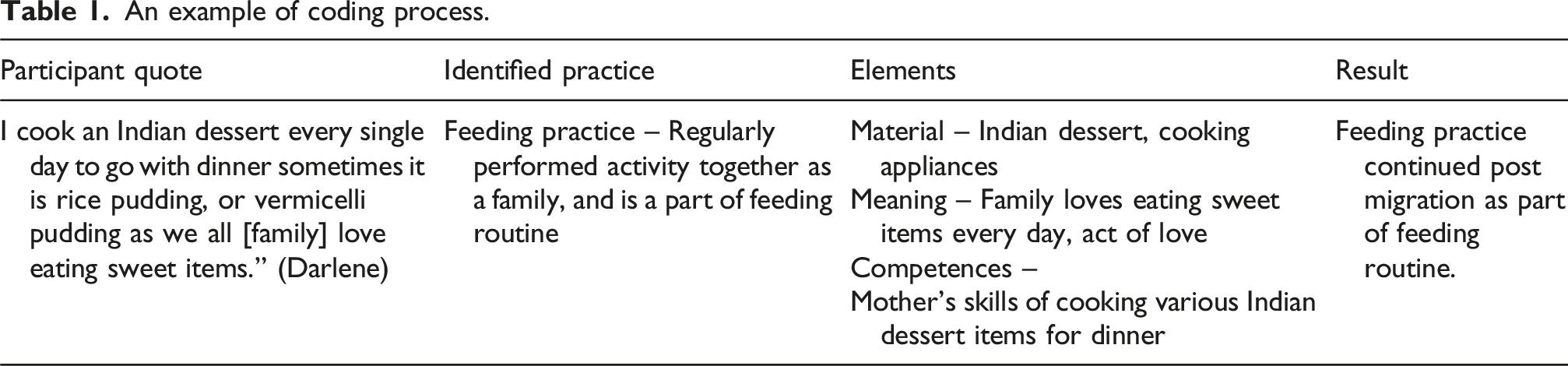
Where mothers discussed how they performed a certain practice, those responses were coded as ‘competences’. The explanations and rationales mothers provided as to why they engaged in a particular practice, the significance of performing a practice were coded as ‘meanings’. The spatial (mentions of locations and contexts) and temporal (mentions of duration, and frequency of the practice) components of each practice were also captured and were coded under ‘spatial aspects’ and ‘temporal aspects’. The data from service providers were analysed following analysis of data from mothers to add depth and were coded to existing codes. The content of the codes ‘meanings’ ‘spatial aspects’ and ‘temporal aspects’ were inductively analysed whereby like-concepts were clustered together, abstracted and reported in this manuscript.
The research team comprised researchers from the fields of dentistry, public health and sociology which shaped the analytic approach informed by Shove et al.’s SPT. Members of the team had varying degrees of cultural proximity to participants including experience working with Indian communities, one author shared the same Indian origin backgrounds as the mothers’ which facilitated rapport development during interviews. Simultaneously, the team was mindful about researcher bias arising from shared cultural experiences. To address this, the first author maintained reflexive notes, following interviews to document assumptions, and emerging interpretations. To support a rigorous analysis, developing findings were discussed regularly among authors, and codes and interpretations reviewed and agreed.
Results
Demographic details of mothers.
Continuity of social practices post migration
Initially, some of the oral health related practices appeared to be ‘retained’ but were, in fact, actively ‘maintained’ as a way of reinforcing cultural identity (meaning) in the diaspora. Many households described a range of oral health related practices and their elements. The practices demonstrated a conscious effort to sustain cultural identity.
We have detailed various practices identified relating to oral hygiene, highlighting the elements identified in each practice. Through verbatim quotes from participants, we provide a nuanced understanding of these practices offering a comprehensive view of how oral health is approached among these mothers and their families.
Teeth brushing/cleaning practice
When discussing morning routine, teeth brushing/cleaning was the first activity/practice mentioned by the mothers in relation to oral health. The quotes below illustrate how, why and using what this practice was performed.
To ensure brushing practice as an everyday routine, one mother used ‘fear of losing teeth’ (meaning) as a strong motivator, along ‘with raising voice with children’ suggesting they are ‘Indian mum kind of things.’ “If you [to her children] are not taking care of teeth, then [teeth] are gone. How can you [children] eat and everything? I take five to ten minutes efforts every day, I tell him, and then my voice is getting up.” (Rachel)
Other strategies were also used including withholding breakfast until the child had brushed his teeth. This could be seen as reinforcing social regulation (meaning) as it is quite common in India to immediately brush in the morning before eating. The meanings behind the practice remained the same as they were before migration to Australia.
Some practices were maintained through intergenerational knowledge (competences) as the crucial element in the way the practices are performed. The excerpts below reflect the influence of older generations on continuing practices and, hence, shaping and contributing their children’s oral health.
Some mothers reported the use of certain Indian objects (materials) for brushing, including Ayurvedic materials (teeth cleaning paste). This practice was passed down from older generations (children’s grandparents, great grandparents). Although mothers did not specify the brand or formulation, the Ayurvedic paste is typically made up of herbal ingredients such as clove, turmeric, neem, or rock salt, all of which are beneficial for oral health. These materials continued to hold cultural significance in the post migration context. One mother, for example, used Ayurvedic paste as it was suggested to her by her father-in-law (meaning) to clean her teeth. “My father-in-law – he’s an Ayurveda person. He gave us [her family] the paste this Indian paste that won’t damage your enamel. So, we always try to brush with that paste, but sometimes kids don’t like the smell, so we use only a little bit of normal toothpaste [brand name], and wash after that. So, I gain a little bit more knowledge from my father-in-law.” (Rachel)
Another mother reported cleaning her teeth with a combination of Indian tooth powder and mango leaves (material) which she learned from her own grandfather growing up (meaning). “Growing up in Kerala, my grandparents used to brush their teeth with “mango leaves paste” and “Umikari” it’s this black powder stuff like charcoal but it isn’t charcoal, I used to blacken all my teeth with that powder and then smile silly with all my cousins and siblings.” (Emma)
Mothers reported watching and following Indian health professionals (an indicator of trust) on social media to learn about children’s health, including how to brush their children’s teeth, showing adaptation of specific competences. “Recently I came across a [social media app] reel, which showed that an Indian dentist was holding his daughter between his legs that helped him have more control and he could brush her teeth. So, I decided to use that technique with her [daughter].” (Emma)
Another mother reported reading content posted by Indian health professionals on social media platforms reflecting her continued trust (meaning) in them and in culturally shared approaches and health beliefs to regulate her child’s health related practices (adapting competences). “I follow some doctors based in Bangalore or Mumbai or whatever in India. So, a lot of them are really good, their education is really good, and they have their [social media app] pages. I just follow them and read their content about children’s health.” (Naveena)
Tongue cleaning and mouth rinsing practices
During the interviews, there were mentions of other practices such as tongue cleaning, and mouth rinsing. Tongue cleaning and mouth rinsing were identified as culturally relevant practices that mothers performed in their home country and continued to practice post-migration. “Like in morning, even if we [parents] do brush his teeth, He [her son] does that [brushing] but you know, like we [family] Indian, like, like to clean our tongue with the tongue cleaner.” (Alia) “Even if they [children] brush before having breakfast, I want to make sure that they rinse their mouth after breakfast, but then sometimes in a hurry, like to rush to schools, like they don’t get a chance to do that [rinsing mouth].” (Prerna)
Carrying practices (mouth rinsing, tongue cleaning) from their home country to the host country is indicative of the spatial aspect of those practices.
Mouth wiping practice
There were only two mothers in the study that mentioned cleaning baby’s mouth with a wet cloth after feeding. The first quote below indicates how the mouth wiping practice was passed down from one generation to the other. We have put mouth wiping as a practice because it involves the material (wet cloth), the skill (knowing to wiping the mouth and the inside) and the meaning (must clean after breastfeeding) and was routinely performed. It also has a temporal aspect; this practice lies dormant for years and is performed when the baby is of certain age and then gets replaced by tooth brushing. It may become active again once another baby is born.
Shaped by culturally informed meanings of hygiene and care, these mothers described engaging in the practice of wiping their baby’s mouth after breastfeeding to maintain oral cleanliness (meaning) depicting intergenerational influences along with the retention of the age-old practice. “My mother had taught her to use a wet cloth to wipe the child’s mouth and the inside of mouth after breast feeding.” (Rebecca) “I wiped her [baby] gums with a really soft cloth made from cotton which I brought from India.” (Kayla)
Using materials in relation to teething
The findings of this study suggest that social practices can be modified in how they are performed and the materials used, following re-immersion in the birth country culture. For example, following a return trip to India, one mother mentioned using a homeopathic medicine along with allopathic medicines for her child’s teething. Using Indian homeopathic remedies reflects cultural continuity in oral health related practices. “I have started giving her this like a German medicine and it helps with the baby teething which I found out about back in India, in an Indian [social media app] group. It’s not medicine, it’s not allopathic, it's homeopathic, so you can take it without prescription, I think.” (Kayla)
Feeding practice
In this study feeding was encountered as a major activity situated in everyday routine during various times of the day, morning breakfast, lunch at school/ECEC and dinner at night. Feeding was typically performed by mothers, consistent with cultural norms around caregiving. Despite some fathers preparing meals if mothers were unavailable, the meals were generally described as ‘easy to prepare’. This suggests traditional gender-based division of household labour was maintained despite acculturation minimally modifying competences through the redistribution of cooking/feeding practices “Mainly what I do is I cook. My role is to cook. When both of us [husband] are at home, like I’m cooking It’s just natural. If I’m on night shift, I know there’s lamb chunks in the fridge, and then I’ll just message my husband, he is a good cook, but he just knows basic cooking.” (Chitra) “I'm always in the kitchen, making dinner while children doing homework.” (Alia) “I'm dealing with them [children] on daily basis, so I know how my child is and what I need to provide for him.” (Rebecca)
Despite pressures to adapt to Australian culture, dinner continued as a protected practice where emotional and cultural meanings, including traditions and rituals such as eating together as a family, nurturing through diversity, and cooking a variety of Indian dishes were preserved and enacted. “We do have a heavy dinner because my husband is always home for dinner and it is always Gujarati style like roti [Indian bread] sabji [vegetable curry], dal and rice.” (Alia)
For some families, traditions that were transported to Australia from India. For instance, a sweet item every night continued as a part of the everyday routine of families and something they liked to share as a family. “The dinner is always typical Indian: Chapati [Indian bread], rice, dal, one vegetable curry and one sweet dish. I cook an Indian dessert every single day to go with dinner sometimes it is rice pudding, or vermicelli pudding as we all [family] love eating sweet items.” (Darlene)
Respecting older family members is a deeply ingrained cultural norm in India prioritising family harmony (meaning) even if it means compromising children’s eating patterns. For example, when mothers were discussing providing milk to children, one mother reported frustration over her mother in law’s insistence on providing sugars/sugar substitutes to the baby to finish her meals despite her own reluctance. “My mother-in-law tells me to give my baby “panikal kandam” it’s a sugar substitute that she claims does not have harmful sugars in it, she tells me to put it on the baby’s tongue so she [baby] can finish her meals.” (Emma)
Mothers also felt pressure from the older generation’s insistence on what to feed children, even if doing so impacted their child’s health. “In our Punjabi culture, dairy is a big thing especially in my house, so when we visited India, my baby was six months, and I strictly said no dairy for her [baby]. But I noted that they [grandparents] will try to give her dairy, so that was my little problem because that's why she had the rashes, she couldn't tolerate it, she had diarrhoea.” (Kayla)
To maintain cultural identity (meaning) through the inclusion of Indian foods in everyday life, all mothers reported consistently visiting Indian stores and two local Australian retail supermarkets for groceries. “My daughters go swimming and martial arts on Thursday. There is an Indian shop and there is a [brand name] grocery store as well, so we have one hour between classes to shop.” (Chitra)
Another example of intergenerational influence (meaning) was the introduction of discretionary foods (materials) to children by grandparents when it came to feeding. One mother explained how her daughter was first introduced to sodas by her grandparents, whereas the child’s parents had decided not to give soda to the child as they considered it bad for health. “My daughter tasted Soda [brand name] through her grandparents especially her grandfather, my father.” (Seema)
Visiting a dentist as a practice
Mothers were asked if the children ever visited a dentist and responses below describe how certain meanings; competences influenced this practice of visiting a dentist. There were few mothers who were reluctant to visit a dentist here in Australia because of perceived mistrust of oral health care services (meaning) offered in Australia. “When I went to India once, and I had teeth cleaning done, whatever it was, but that wasn’t like it is done here… Someone [friend] here told me, like, “Oh, the thickness of the teeth just reduces by a few inches when you do this [demonstrating scratching teeth with hands] or whatever and so I didn’t do it here.” (Chitra) “We [family] went to a paediatric dentist here [Australia]… he said she [daughter] goes under anaesthesia and then take pull out all the teeth. But then we were not ready for that because she was very small and then getting like general anaesthesia. We didn’t want to go through that. So, when we went to India, we went to an Indian dentist who took out only a few teeth… So, we managed it in India, which is better, because I don't think it was absolutely necessary to pull out most of her teeth.” (Prerna)
Visiting a general practitioner as a practice
During the interviews the mothers were also asked if they ever visited general practitioners (GP) for their children’s oral health problems or feeding issues to which some mothers responded that they did visit GPs regarding their children’s health. The issue of trust and the importance of shared health beliefs (meanings) was apparent in mothers visiting an Indian general practitioner (GP) in Australia, reflecting continued trust in GPs of Indian origin. For one mother, an Indian family in her social media app group suggested an Indian GP “I don’t know about how reliable the doctors [here] are, but mostly Indian families, they’ll go to a South-Asian GP. A few of my friends go to Dr [name] who is Pakistani, or I don’t know where his clinic is, but they say, “Oh, he’s a very good doctor.” (Chitra) “The health nurse would always say that she [child] is underweight, she is malnourished. But when I asked my [Indian] GP, he is like if she drinks enough fluids and running around then she is normal. All he did tell me that you can give chocolate that’s okay, but not lollies and sucking sweets.” (Seema)
Social practices changed or adopted through acculturation
The section below examines practices that were newly adopted or older practices modified in response to acculturation. From the interviews it is evident that practices were not modified for the children alone but for the mothers too in terms of oral hygiene and feeding because of moving to Australia and adapting to the Australian context.
Tooth brushing/cleaning practice
Although toothbrushing practice has been described above as largely remaining unchanged, in some cases, some of its elements like competences changed. Mothers initially took full responsibility and gradually shifted from co-brushing to supervising to child-led brushing, all the while teaching their children how to brush. Here the competences and meanings behind toothbrushing modified. “I used to help her [daughter] [for brushing] before, but from last one week, she started doing it by herself.” (Ridhima) “We [parents] just keep an eye that he [son] is [brushing] right or wrong because then we have to tell him this is wrong thing [of brushing].” (Naveena)
Flossing practice
One mother mentioned performing flossing practice which she started after visiting a dentist here which suggests how service providers (dentist) influenced adopting a practice that is beneficial to oral health. Learning to use floss was a competence that was developed following migration to Australia. This suggests a strong cultural influence on establishing certain practices. “I never did floss in my 25 years. But here we [herself] do floss…. I went [dentist] here for…. and she said, oh, start doing flossing every day so it [food] won’t get stuck. So now I’m doing [flossing].” (Alia)
Mouth rinsing practice
Even though the practice of mouth rinsing spatially travelled to Australia, the practice had changed over the period participants had been in Australia. This was particularly pronounced for children. In India, where hands were used for eating, hand washing, and mouth rinsing followed. With the adoption of cutlery use since moving to Australia, hand washing was not required, and concomitantly, mouth rinsing no longer occurred, as per one of the mothers. This reflects how a modified way of eating modified practice. “In India, mostly we eat with our hands so, like after finishing our food, when we wash our hands, we make sure that we rinse our mouth as well. So, I think that’s a very good way of practicing but here [Australia], especially for my daughter and children, they eat with spoon, and then they don't have to wash their hands. So, then they don’t rinse their mouths too.” (Prerna)
Feeding practice
Feeding is one practice that is included in both continued post migration and modified post migration. Feeding practice differs in the way it is performed during different times of the day highlighting how the meaning behind the practices changes with the change in environment. When discussing feeding practices, many mothers described serving traditional Indian foods depending on the time they had available in the morning and children’s preferences: Indian breakfast options (e.g., flattened rice savoury breakfast with carrots) were served if time permitted, otherwise convenient ready to eat food options (cereals, toasts) were served. This shift from traditional Indian to modern Australian food was not for practical reasons alone but reconfigured the meaning of breakfast as a culturally embedded act of care and nourishment. Temporal constraints and material availability (ready-to-eat foods) eroded the embodied competences and symbolic significance attached to traditional Indian meals.
Tension also arose between cultural identity and social norms as evidenced by the inclusion of foods in children’s lunchboxes. Mothers described how children rejected traditional Indian lunches such as roti (whole wheat Indian bread), sabji (vegetable curry), dal and rice, which are typical Indian lunches and requested modern Australian foods (Figure 1) to avoid being embarrassed and standing out at school. This shift in materials reconfigured the meaning of food from an expression of ethnic identity to one of social belonging. The school lunch became a site where the practice of traditional eating destabilised: meanings shifted, and competences were modified under the pressure of their children’s desire to fit in. “My daughter just likes to eat whatever her friends are eating in school.” (Ridhima) “My daughter goes, mom, I don’t want to eat like Indian food every day, can I have something else in school?” (Alia) Inclusion of retentive and sugary foods in lunchboxes.
Interestingly, certain foods/drinks are used as a reward for children and to instil the importance of good behaviour in the future. “Bubble tea is like a cheat for us [daughter and mother]. She likes the bubble tea.” (Seema)
When discussing the practice of shopping for food, some mothers reported buying foods according to the child’s preference for discretionary foods, reflecting their adoption of Australian culture. “We [mother & sons] go to local grocery stores and Indian stores. I buy my children whatever foods they want.” (Darlene)
Despite many mothers in the study preferring to seek health advice from Indian or South Asian health professionals, some mothers had begun trusting Australian health professionals. This was particularly the case when the mother was anxious. One mother reported following Indian traditions but also following advice from Australian nurses at her health practice. “I very much follow the Indian traditions, but I listen to Australian nurse as well, some of the texts, some of the things [from nurses]. It was very helpful.” (Rachel)
Discussion
The current study highlights that Indian mothers’ oral health related social practices following migration are characterised by selective continuity and adaptation rather than linear change. Viewed through SPT lens, these patterns can be understood as the outcome of changing meanings, availability of materials and competences of everyday practices. Informed by Shove et al.’s interpretation, identified social practices were understood as temporally situated, shaped by spatial dynamics and shifting cultural norms (Shove et al., 2012).
As mentioned earlier, certain oral health related practices continued from before migration. The persistence of these practices can be understood through their strong anchorage in cultural and traditional meanings, materials and embodied competences that remained largely intact following migration. For example, the practice of feeding, cooking an Indian dessert for dinner in particular, demonstrates that this practice sustained because of its meaning – dessert was symbol of love, it was a tradition. Similar to our study, previous literature also demonstrates how cooking a meal is a representation of love and care (Bugge and Almås, 2006; Moisio et al., 2004). Another sustained practice was mouth rinsing that was identified as a culturally relevant practice that had travelled from the families’ home country to Australia. The meaning behind mouth rinsing was identified as an efficient way of removing food debris retained in the mouth after eating that kept it anchored in the everyday lives of families. Similar findings were reported in a study conducted in the UK, which also reported the practice as a religious custom (Kay et al., 1990) however the meaning for performance differed from our study. Findings from Singh et al. (2017) reported mouth rinsing as a cost-effective preventive measure to prevent dental decay. Mouth wiping after breastfeeding to maintain oral hygiene was another practice that is worth discussing because of its elements, it is the learned competency from older generations that led for that practice to continue following migration. Similar to our study, one study citing The American Academy of Paediatric Dentistry also recommends cleaning a baby’s mouth after breastfeeding to prevent tooth decay (Salone et al., 2013).
Among the continued practices, using ayurvedic/homeopathic materials for teeth cleaning demonstrates how this practice is deeply anchored in age old rituals and traditions. Unpacking this practice revealed how it was the learned competences from older generations and informal support network that reflects the routinised integration of social practices. Mothers reported bringing these materials from India every time they visited their home country which suggest unavailability of resources but the mothers persistence on continuing the practice. This is echoed in the literature. For example, Nicol et al. (2014) reported how participants used traditional materials for teeth cleaning (using charcoal, miswak) and dental pain relief (rubbing gums with clove oil) the use of which was passed down from grandparents. Although not specific to oral health (Kisecik et al., 2023) reported how mothers emphasised intergenerational transfer of traditional practices and knowledge from mothers and grandmothers to support their children’s general health.
Among the practices that were newly adopted or were modified following migration, there are a few worth discussing such as feeding practice in relation to school. Previous literature suggests that school can be a powerful site of social adaptation for immigrant children and their families (Blanchet et al., 2018; Seko et al., 2024). In this study, what children ate for lunch (materials) at school was found to be a constant tension between cultural identity and social norms for the mothers. The meaning behind the content of school lunchboxes was children wanting to fit in school, which changed the materials from traditional Indian foods to modern Australian foods. Similar to our study, one study described immigrant children experiencing feelings of exclusion and a perceived need to ‘fit in’ by bringing a so called ‘normal’ lunch - implicitly white, mainstream foods. Even though parents believed food packed from home is healthier, their children’s reluctance to accept cultural foods drove them to provide Western food items for lunch (Seko et al., 2024). The practice of providing sugary snacks and drinks as rewards for their children’s good behaviour was another practice reported by some mothers. Mothers wanted to treat their children with sugary drinks/foods because of the meaning associated with it, that of indulgence. Previous literature suggests using sugar containing drinks, such as bubble tea or kombuchas, can unintentionally promote unhealthy consumption patterns, affecting children’s wellbeing, as well as have potential implications for overall health, including oral health concerns (Jansen et al., 2020; Lind et al., 2023; Yang et al., 2021).
Despite their own preference for withholding sugar, for cultural reasons, mothers had to prioritise their mother-in-law’s suggestion of including sugar items in children’s diet. Conflict arising between mothers and their mothers-in-law regarding children’s diets and oral health have also been reported in other studies. For example, Burgette et al. (2023) found that more than 50% of mothers in their study reported conflicts with their children’s grandparents, leading to frustration in mothers centred around providing a low-cariogenic (low-sugar, fermented carbohydrates) diet for children and maintaining a regular oral hygiene routine.
The practice of visiting a dentist was differently practiced among mothers. Some mothers had a strong preference for visiting Indian background health professionals for their children’s health, while some mothers waited until their next trip to India for a dental visit. There were some mothers who made sure their child attended the school dental office whenever suggested by the letter sent to them. But largely, their mistrust of Australian dentists, healthcare providers and the treatments they offered was highlighted. Similar findings are evident in the literature, with a lack of trust in dentists and an inadequate understanding of oral health procedures (Batra et al., 2019) and mistrust of dentists and cultural misunderstandings around participants’ diets were reported (Newton et al., 2001).
This study is not without limitations. First, the participation was limited to English speaking Indian mothers which may shape who was able to participate, the findings also may be less transferable to Indian mothers with limited English proficiency or mothers from other backgrounds. Even though the mothers were proficient in English, subtle nuances of meaning may not have been fully conveyed, which could have influenced the depth of the mothers’ responses. Mothers were recruited from low-SEIFA index suburbs where social, and material contexts may likely influence everyday practices. Third, network-based recruitment may have favoured mothers with existing social networks, potentially underrepresenting more socially isolated mothers whose practices may differ. The study was conducted with mothers without participation from fathers or extended family which limits the exploration of their impact on everyday routines. SPT is an abstract theory and hence leaves room for subjective interpretation which may differ from individual to individual (Strengers, 2010).
Conclusion
The findings of this study highlight how children’s oral health related practices are driven by culturally meanings, materials and old/new learned competences. By applying Shove et al.’s SPT this study extends existing literature that is largely focused on preventive and behavioural based approaches demonstrating cultural adaptation as a constant tension between everyday occurring practices. For health care providers, the findings underscore the importance of engaging mothers in conversations about everyday caregiving routines, family roles and constraints related to migration rather solely focusing on their compliance with recommended practices. This research offers a new way to understand what factors (barriers/facilitators) support or undermine oral health related practices, in this case migration, family and social environment. Future research could extend this practice-based approach to other diverse communities to explore how their oral health related practices evolve across space and time.
Footnotes
Acknowledgments
The research team acknowledges the chief investigators of this Australian Research Council Discovery project, who contributed to the conceptual design of the overall project. Open access publishing is facilitated by the University of Western Australia as part of the Taylor & Francis—The University of Western Australia agreement via the Council of Australian University Librarians.
Ethical consideration
Ethics approval for this study was obtained from The University of Western Australia Human Research Ethics Committee. (2021/ET000223)]
Consent to participate
Written informed consent was obtained from all the participants.
Author contributions
RJ was responsible for conceptualisation, methodology, data collection, data curation, data analysis, drafting and editing the original manuscript. PW was responsible for conceptualisation, methodology, funding acquisition, project administration, verifying analysis, and reviewing and editing the manuscript. CF was responsible for conceptualisation, methodology, verifying analysis, reviewing and editing the manuscript. HC was responsible for conceptualisation, project administration, funding acquisition, verifying analysis, reviewing and editing the manuscript. LSS was responsible for conceptualisation, methodology, funding acquisition, project administration, verifying analysis, reviewing and editing the manuscript. All authors read, reviewed, edited, and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Australian Government through the Australian Research Council’s Discovery Projects funding scheme (Project DP210101166).
Disclaimer
The views expressed herein are those of the authors and are not necessarily those of the Australian Government or Australian Research Council.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Given ethics requirements, data collected is not available to be shared.