Abstract
Traditional approaches to dental public health education across Europe remain dominated by lecture-based learning which often fail to cultivate critical reflection on inequities, privilege, and the broader social determinants of oral health. Social accountability has been recognized as core competency for dental graduates, requiring dental professionals to align professional practice with the health needs of communities. Community-engaged education is a promising pedagogical model that situates learning within real-world contexts, fosters empathy, cultural competence, and advocacy skills, and strengthens professional identity formation. This paper discusses the Peninsula Dental School’s innovative model, which integrates community engagement, reflective practice, and interprofessional education within a spiral curriculum. Through the Interprofessional Engagement (IPE) module, students collaborate with local community organisations to co-design health improvement projects, critically reflect on their experiences, and gain deeper insight into oral health inequities. Embedding community engagement and social accountability across European dental curricula is both timely and necessary to equip future practitioners to address oral health inequities, meet evolving societal needs, and contribute to a more just healthcare system.
Traditional dental public health teaching
Dental public health is a recognised specialty in the UK. At undergraduate level dental public health competencies form part of UK dental graduate registration requirements (General Dental Council., 2024). Across Europe dental public health is an essential component of undergraduate dental education though its structure and emphasis vary widely between institutions (Rizvi et al., 2020). A survey of European dental schools indicated inconsistent integration of dental public health within curricula, with variation in topics, teaching methods, and assessment approaches (Rizvi et al., 2020). Key curricular elements typically include health promotion, disease prevention, healthcare systems and workforce planning (Rizvi et al., 2020). The above survey found most European dental schools use traditional teaching methods, primarily lectures, supplemented by seminars, project work, outreach visits, tutorials, and workshops (Rizvi et al., 2020). Traditional lecture-based learning in dental public health, community health, and social determinants of health, however, has been criticised for its failure to examine issues such as power and privilege or promote critical thinking about justice and inequity (Kontaxis and Esfandiari, 2023; Noushi et al., 2020; Sharma et al., 2018). Learning about social determinants of health is not consistently embedded and integrated into undergraduate teaching and clinical training, resulting in graduates who may have strong technical knowledge but little appreciation of the broader socioeconomic and political factors shaping oral health inequities (Leadbeatter and Holden, 2021; Noushi et al., 2020).
Dental care professionals play a vital role in delivering high-quality care that not only meets the clinical needs of patients but also upholds their ethical and professional duty to address inequities in oral health, particularly among vulnerable and underserved populations (Watt, 2012; Watt et al., 2016). Achieving patient-centered care requires moving beyond a narrow biomedical perspective and instead embracing a biopsychosocial approach that considers the wider social, psychological, and cultural factors influencing health (Bedos et al., 2018; Scambler et al., 2016). To support this shift, there is a pressing need for dental education to evolve, with schools moving away from traditional, biomedical models and adopting socially accountable approaches that prepare future practitioners to respond effectively to diverse community needs (Clithero et al., 2017).
Social accountability
Efforts to address health inequities are increasingly centered on the role of health professional schools and their graduates, with the objective of aligning educational outcomes more closely with the health needs of communities (Freeman et al., 2025). This notion stems from the concept of social accountability which was introduced by the World Health Organisation (WHO) in 1995 (Boelen et al., 1995). Social accountability is defined as “the obligation to direct [health professional] education, research, and service activities towards addressing the priority health concerns of the community, the region, and the nations [health professional schools] have a mandate to serve” (Boelen et al., 1995). In response, European initiatives, such as the Association for Dental Education in Europe (ADEE) have advocated for embedding ‘Dentists in Society’ as a domain of dental public health education and the European Association for Dental Public Health (EADPH) has an education special interest group to promote innovation in dental public health education (Gallagher and Field, 2017). In particular, a graduating European dentist is expected to take account of the wider context within which they practice, integrate effectively with society, and advocate for general and oral health, and system change (Gallagher and Field, 2017). In the UK, the General Dental Council (GDC) has similarly embedded social accountability within the Safe Practitioner Framework, which sets out the required behaviours and learning outcomes in dental professional education, making it a required competency for graduates under the professionalism domain (General Dental Council, 2024).
Social accountability has also been used as a benchmark of excellence in accreditation of healthcare education institutions. The Association of Medical Education in Europe (AMEE) launched the ASPIRE to Excellence initiative in 2012, with social accountability being an integral indicator for excellence (Hunt et al., 2018). Dentistry has been incorporated into the ASPIRE panels and board since 2014 (Hunt et al., 2018). Initiatives such as the THEnet Social Accountability Framework have been developed to help healthcare institutions align their education, research, and service activities with the priority health needs of the communities they serve (Larkins et al., 2013). By providing clear guidelines and measurable indicators, THEnet enables institutions to assess how effectively they address societal health challenges, engage stakeholders, and contribute to equitable health outcomes. education and service delivery (Larkins et al., 2013).
Community engaged education
Community-based dental education emerged in North America in the 1960s, and adapted in the UK in the 1970s, in response to concerns that the insular environment of dental schools limited students’ social awareness and sensitivity to the realities of healthcare delivery (Elsheli et al., 2024). US government funds were used to incentivise dental schools to develop rotations for their students outside the university in order to broaden dental students’ education and serve the community (Elsheli et al., 2024). However, even when dental schools incorporate community-based or outreach rotations in their clinical curricula, these experiences primarily focus on delivery of patient care without associated educational activities that would engage students in their understanding of the community served by the clinic (Elsheli et al., 2024; Plessas et al., 2024).
Community engagement, on the other hand, is a type of community-based education, which has been advocated as a promising pedagogical approach to produce socially accountable graduates (Plessas et al., 2024; Reeve et al., 2017). It is conceptualised as a form of experiential education which utilises community exposure educational programmes or activities (i.e., students are exposed to the population/community of interest usually in a non-clinical setting) aiming to highlight and address community needs (Magzoub and Schmidt, 2000). It draws on the learning theory of experiential learning and involves learning activities that take place in and with the community to educate the learner and at the same time serve the community (Hood, 2009). The primary aim of incorporating community engagement into dental curricula is to situate learning within real-world contexts and provide students with exposure to diverse populations and social circumstances (Hood, 2009). This approach helps students to develop a deeper understanding of the social dimensions of patient care, moving beyond the acquisition of purely clinical skills typically developed within dental school clinics. Furthermore, such educational activities expose students to the intersectional and multilayered aspects of social determinants of health, barriers to access care, and the lived experiences of underserved populations (Elsheli et al., 2024; Hood, 2009). Evidence suggests that these experiences foster empathy, cultural competence and sensitivity, communication skills, and an orientation towards advocacy and social responsibility (Plessas et al., 2024). They also help students critically examine their own privilege, humanise community members and overcome misconceptions and bias towards different populations (Plessas et al., 2024).
The Peninsula Dental School model
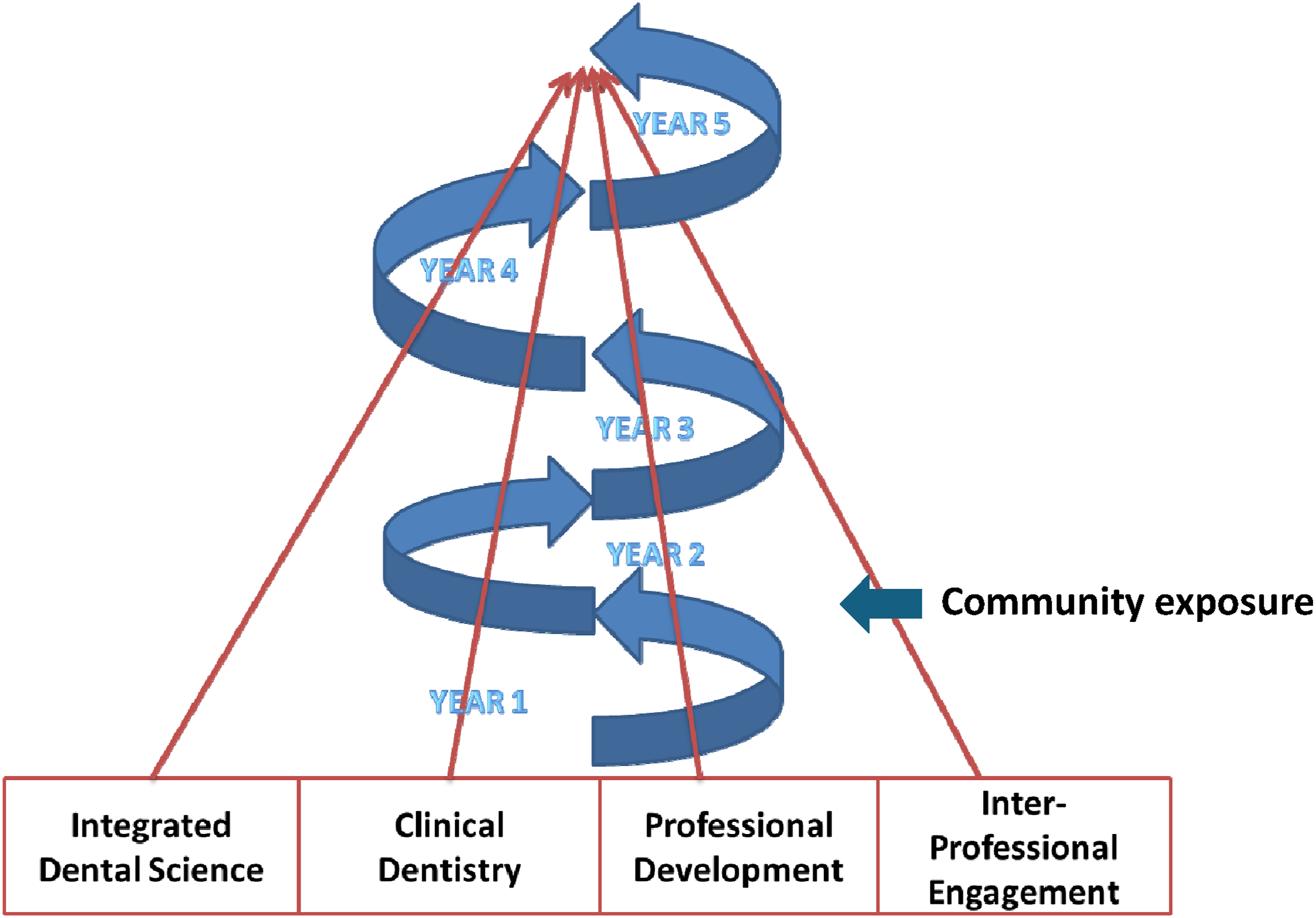
Peninsula Dental School, established in 2006 offers a unique community-oriented model of dental education in the UK that is aligned with social accountability values. Its vision is built on three pillars: professionalism, dental skills, and societal awareness and responsibility (McHarg and Kay, 2009; Tredwin et al., 2022). The curriculum has four main teaching blocks: integrated dental science; clinical dentistry; professional development; and inter-professional engagement. Each of these themes spiral up through the programme recognising that a learner’s growth is a gradual continuous process (Figure 1). Clinical patient exposure starts early in the curriculum, in the first year of study. Clinical skills are gained in primary care dental clinics situated in areas of high dental need, in an attempt to serve the local communities and address the poor access to NHS dental care; whilst community engagement and interprofessional education occurs continuously through the spiral curriculum (McHarg and Kay, 2009; Tredwin et al., 2022).
Illustrative examples of community projects delivered as part of the dental public health curriculum.
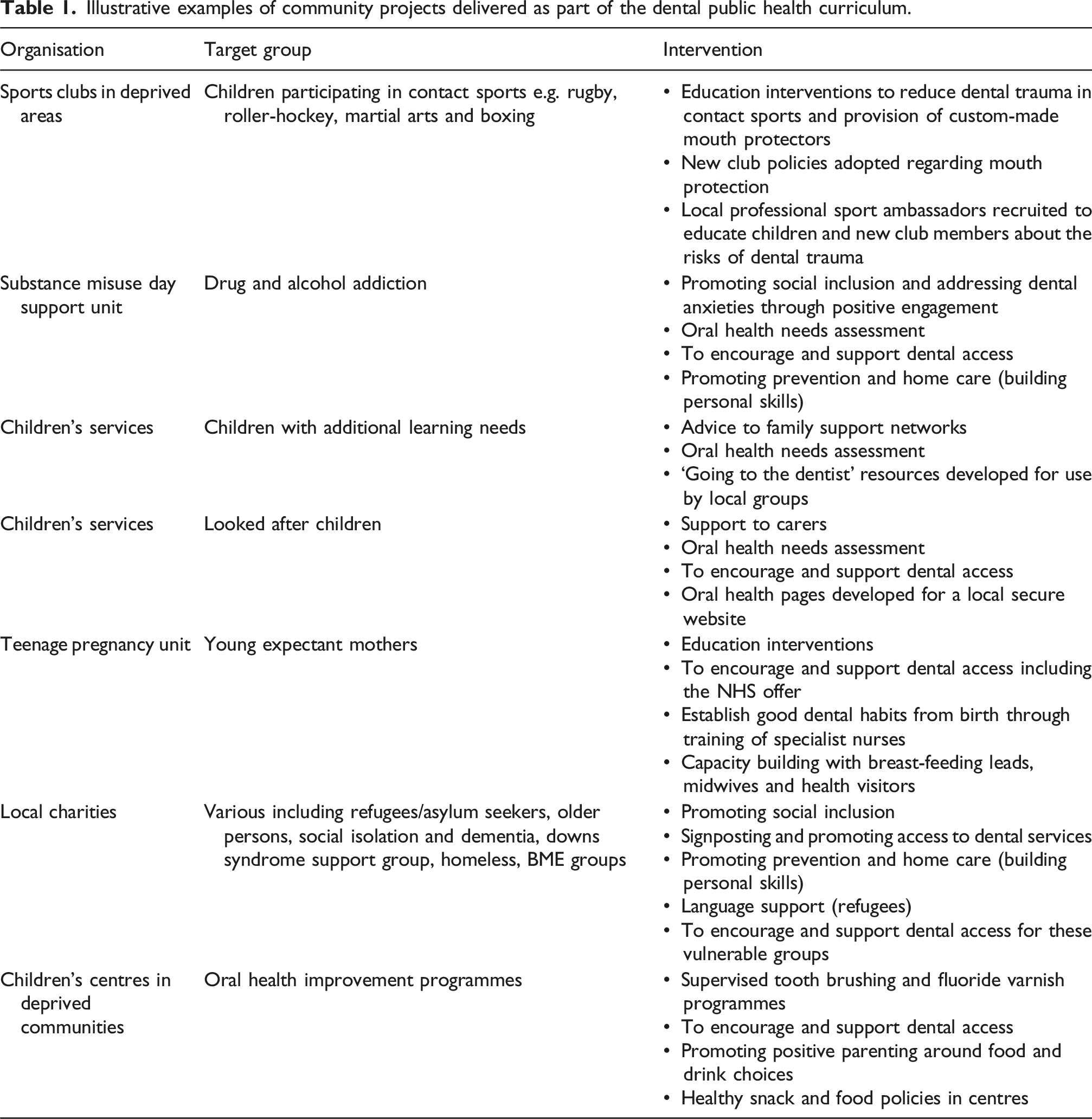
Through this engagement, students co-design small intervention projects with community partners, supported by academic tutors with an interest in public and community dental health. This fosters deeper insight into oral health inequities and the complexity of social determinants of health (Witton and Paisi, 2022). The IPE module integrates enquiry-based learning with reflective practice. Students participate in facilitated sessions to critically reflect on their experiences, connect these to professional development, and present their learning through posters, reflective writing, and an end-of-year symposium. Reflection is thus not only formative but also a formal part of assessment (Witton and Paisi, 2022). Research on the IPE module at Peninsula Dental School has shown that these community experiences enhance students’ communication skills, teamwork, empathy, and self-awareness (Hanks et al., 2016; Neve et al., 2020). Neve et al. found that students described profound emotional responses when faced with social realities of vulnerable individuals, which in turn deepened their understanding of their professional responsibilities (Neve et al., 2020). In the third year of studies, Peninsula dental students engage in interprofessional learning with other health and social care profession students, further reinforcing the idea of interprofessional collaboration and preparing them for delivering holistic care (Tredwin et al., 2022). Such experiences promote mutual respect, and the skills required for integrated healthcare delivery, crucial in tackling complex public health challenges such as oral health inequity (Jha Kukreja and Kukreja, 2025).
Strengths, challenges and opportunities
Community engagement gives students practical experience of community work to help them build their knowledge and skills in dental public health and bridges the gap between theory and practice. Students work with and alongside community organisations to understand what they do, what community assets are, what challenges their beneficiaries experience, understand the impact of health inequalities, and the complexities of oral health in vulnerable groups. The IPE module brings to life issues communities face such as inequalities, power and privilege, the struggles people face in accessing services and discrimination (Witton and Paisi, 2022). This can be a daunting and challenging experience for some of our students talking to a person they may never have come across before and in the persons own environment, which is a highly effective way to reverse the power dynamic compared to when they are in the clinical environment.
An important strength of the Peninsula model lies in its sustained and authentic partnerships with local organisations. Nevertheless, developing and maintaining these partnerships, can be a challenge if the institution’s mission, ethos and priorities as well as organisational culture do not align with social accountability and community health values. The pivotal role of a dedicated community engagement team who support the organisation and delivery of the community-based curriculum cannot be emphasised enough. In order to create the learning opportunities, there is a requirement for reciprocal community-academic partnerships with a range of community-based organisations. One of the strengths of having a dedicated community engagement outreach team work is that they work with community organisations all year round, delivering health promotion projects addressing priority needs, ensuring a two-way relationship and ensuring that the community organisations do not perceive the student’s involvement as an opportunistic experience which would only benefit the school.
Reflection is a key aspect of community engagement, which separates this educational model from outreach clinical rotations. Without it, important learning opportunities can be missed. Students should be encouraged to reflect on their learning experiences in the community and how these may shape their personal and professional views and attitudes and their understanding of the role of socio-economic and political factors on oral health behaviours, outcomes and care delivery (Leadbeatter and Holden, 2021). Journaling, guided reflection, and critical incident reflection have been described as methods of reflection used in community engagement. Reflective journaling involves writing about insights gained over a period of time. Guided reflection is a structured form of reflection which occurs between facilitators and students and typically involves a series of prompt questions. Critical incident reflection is a type of guided reflection where a learner is prompted to reflect about a practice-based experience or incident that carried a particular significance (Leadbeatter and Holden, 2021). During the IPE module students are given multiple opportunities to reflect on their learning. The students attend a scheduled dedicated guided reflection session with their tutor after the project delivery, whilst they may also discuss a particular incident of interest and share insights during the milestones of the module, and finally they are expected to provide a reflective log as part of their module assessment.
Running the IPE module can present challenges as it is resource intensive and requires constant dedication to maintain the academic-community partnerships alive. According to the literature, funding constraints and resource allocation can limit the sustainability of community-based programmes, whilst limited curriculum time and competing demands between acquisition of technical skills versus what are termed soft skills may restrict the time allocation for community engagement (Elsheli et al., 2024; Freeman et al., 2025; Jha Kukreja and Kukreja, 2025). Hidden curricula within dental schools may implicitly devalue social responsibility compared to technical skills. This is why training faculty and clinical staff/supervisors in areas such as social determinants of health, cultural competence, health equity and social accountability is paramount, so the values of social responsibility and empathy are not eroded as the students progress through their clinical training (Jha Kukreja and Kukreja, 2025; Kontaxis and Esfandiari, 2023; Leadbeatter and Holden, 2021). The integration of the concept of social accountability across the curriculum and particularly in terms of clinical care and treatment planning will ensure that these values are embedded in the professional identity of the students and hence will be more likely to be sustained in their professional lives (Jha Kukreja and Kukreja, 2025; Kontaxis and Esfandiari, 2023; Leadbeatter and Holden, 2021). However, dentistry’s strong business model risks undermining social accountability values upon graduation. Students may experience tension between commercial imperatives and professional ideals of health equity and justice (Freeman et al., 2025). A dental school invested in delivering socially accountable education should therefore demonstrate a commitment towards influencing the working environment through research and policy to increase the likelihood of graduates being able to implement the ideals the school has shaped (Freeman et al., 2025; Kontaxis and Esfandiari, 2023).
Conclusion
Traditional approaches in dental public health teaching, while effective in imparting knowledge, remain insufficient to prepare graduates for the complex socioeconomic and policy challenges shaping oral health. The Peninsula Dental School model demonstrates how a spiral curriculum, community engagement, reflective learning, and interprofessional education can be operationalised to produce socially accountable graduates. It highlights the importance of community partnerships, and reflective assessment to deepen student learning and professional identity formation. As regulatory bodies such as the GDC in the UK, begin to mandate social accountability as a graduate competency and European bodies are advocating in the same direction, all dental schools have both the opportunity and the responsibility to align their curricula with this vision. By doing so, they will not only enhance the professional formation of dental graduates but also contribute meaningfully to reducing oral health inequity across society. However, a European-wide framework on public health teaching is warranted in guiding curricula towards a shared vision of socially accountable dental education. Peninsula dental school spiral curriculum model.