
Abstract
Oral squamous cell carcinoma (OSCC) and its precursor, oral epithelial dysplasia (OED) comprises significant disease burdens in southeast Asia. In Sri Lanka, OSCC is the commonest cancer in males. Oral health-related quality of life (OHQoL) assesses the impact of oral health on the overall well-being of an individual. This study aimed to investigate OHQoL using Oral Health Impact Profile (OHIP-14), to identify the most affected domains in the study groups and potential associations with sociodemographic variables. A cross-sectional study with 129 participants including OSCC, OED and control groups was conducted using a translated version of OHIP-14. Data analysis was conducted using SPSS and Graph Pad Prism software. The total OHIP-14 scores were compared between study groups. Descriptive statistics on OHQoL domains and correlation with monthly income and OHIP-14 score were conducted. The mean OHIP-14 scores were 25 ± 13, 14 ± 8.1, and 2.4 ± 3.3 for the OSCC, OED, and control groups respectively with a statistically significant difference (p value <0.0001). Domains with highest mean scores indicating a poorer OHQoL in OSCC and OED groups were physical pain and psychological disability. Worse OHQoL correlated with low monthly income in patients. This study identified most affected domains in the OHQoL in study groups and revealed a correlation between income and OHQoL in patients. The findings have important implications for clinicians to take OHQoL into consideration during treatment design and inform policy changes to improve outcomes for OSCC and OED patients.
Keywords
Introduction
Head and neck cancers (HNC) are malignancies arising in the oral cavity, salivary glands, larynx, pharynx, nasal cavity, and paranasal sinuses with the highest incidence reported in the lip and oral cavity (Johnson et al., 2020). In Sri Lanka, oral squamous cell carcinoma (OSCC) is the histological presentation of more than 70% of malignancies arising in the oral cavity (Wijesingha et al., 2023). Clinical conditions that carry an increased risk of developing into OSCC are identified as oral potentially malignant disorders (OPMD). Oral epithelial dysplasia (OED) is the histological entity that precedes many OSCC (Tilakaratne et al., 2019). More than two-thirds of the total global OSCC incidence is reported in Asia (Sarode et al., 2020). OSCC is the commonest malignancy in the male population in Sri Lanka, with a crude incidence rate of 20.5 per 10,000 (Ministry of Health, 2021). The main risk factors for OSCC are smoking and smokeless tobacco, betel quid chewing, excess alcohol, and synergistic action of combinations of risk factors (Edirisinghe et al., 2022). Socioeconomic status (SES) is a significant factor associated with the incidence and mortality of HNC (Johnson et al., 2010). Late diagnosis and low survival due to OSCC were more prevalent in communities with low SES (Auluck et al., 2016).
Health-related quality of life is a concept that captures the interactions between biological, environmental, and psychological aspects on the well-being of an individual (Karimi and Brazier, 2016). Oral health-related quality of life (OHQoL) is defined as “the impact of oral disease and disorders on aspects of everyday life that a patient or person values, that are of sufficient magnitude, in terms of frequency, severity or duration, to affect their experience and perception of their overall health” (Locker and Allen, 2007). The Oral Health Impact Profile (OHIP-14) is a fourteen-item questionnaire tool widely used to measure OHQoL with cross-cultural adaptability, successfully translated and validated to multiple languages (Leoncini et al., 2014; Rimal and Shrestha, 2015; Vinita Mary et al., 2017). The OHIP-14 has been previously validated in older adults in Sri Lanka (Ekanayake and Perera, 2003). OSCC and OPMD can predispose to compromised OHQoL in patients at the time of diagnosis, due to disease associated factors, personal and socioeconomic factors. A study on OHQoL in OSCC patients in Sri Lanka undergoing radiotherapy revealed that patients were suffering from eating problems and speech problems before commencing treatment (Kosgallana et al., 2023).
Most published research focuses on the variation of OHQoL with different treatment modalities and treatment outcomes in HNC (Yuwanati et al., 2021). It is important to gather evidence on the OHQoL at the time of diagnosis, which can promote evidence-based delivery of optimum care and support systems for patients. Further, OHQoL can have associations with sociodemographic indices, which are population specific. This study was conducted with the aim of evaluating OHQoL using the OHIP-14 tool in patients with OSCC and OED at the time of diagnosis, compared to a disease-free control group in Sri Lanka. The specific objectives were to identify the most affected OHQoL domains in the study groups and potential associations with sociodemographic factors.
Methodology
Ethical approval
The study protocol was reviewed, and ethical approval was obtained from the Ethics Review Committee, Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka (Ref: 21/19); and approval from the Education, Training and Research division, Ministry of Health, Sri Lanka (Ref: ETR/AC/2019/11).
Study design and participant recruitment
This study employed a cross-sectional design with three groups: patients with OSCC, OED, and disease-free controls. Three hospitals (National Cancer Hospital, Maharagama, Colombo South Teaching Hospital and Teaching Hospital University of Sri Jayawardenapura) within proximity in the Colombo district, Western province in Sri Lanka, which received patients from urban and semi-urban communities, were selected for participant recruitment. Regarding the lifestyle risk factors of this population, 72.3% of OSCC patients and 47.1% of disease-free controls were smokers, while 78.0% of the OSCC patients were betel quid chewers as reported in a previous study (Edirisinghe et al., 2022). OSCC and OED patients were recruited from the National Cancer Hospital, Maharagama and the Colombo South Teaching Hospital, and the disease-free controls were recruited from the outpatient department of the Teaching Hospital, University of Sri Jayawardenapura. Inclusion criteria for patients were adults over the age of 18 years and histopathologically confirmed diagnosis of OSCC or OED. Exclusion criteria for patients included previous history of any type of malignancy and pregnant and lactating mothers. Inclusion criteria for disease-free controls were adults over the age of 18 years. Exclusion criteria were a history of any type of malignancy, and individuals with clinically suspicious lesions to be either OSCC or OED. Informed written consent was obtained from all participants prior to recruitment. Detailed information regarding the sampling and salivary biomarker analyses conducted in the same study participants was previously published (Piyarathne et al., 2023).
Questionnaire design and pretest
Medical history, histopathological diagnosis, past treatment, and co-morbidities were gathered from hospital records. The sociodemographic data collected from the questionnaire were sex (assigned at birth), ethnicity (assigned at birth), income (independent income status and value of monthly income in Sri Lankan Rupees), and education level (primary or none, secondary or above).
OHIP-14 is a tool that assesses seven domains related to OHQoL (Slade, 1997); each domain is assessed using two questions. Participants were asked to rate the frequency of the experience of each item in the past 1 month using a five-point Likert scale. The translated version of the tool used by Ekanayake and Perera (2003) was more than 10 years back. Upon assessing the translation, we found that parts of the vocabulary (words refereeing to teeth, mouth, or dentures) did not align with contemporary vocabulary. Therefore, the research team used a newly translated version of the tool, following pre-testing. The English version of the questionnaire was forward and backward translated to Sinhala language and pre-tested using n = 10 participants. Higher score in OHIP-14 tool indicated worse OHQoL. All data were recorded by one interviewer to minimize variation.
Data analysis
Data was entered and analyzed using SPSS (version 20), Graph Pad Prism (version 20). Cronbach’s alpha was computed to assess the internal consistency of the questionnaire tool. A score for each question of the tool was assigned in the five-point Likert scale as 0: never, 1: hardly ever, 2: occasionally, 3: often, 4: very often. A total individual score for OHQoL was calculated by the sum of the scores for the 14 questions in the OHIP-14 tool. For each question the maximum score was 4, with an overall maximum score of 56 for the whole questionnaire. The OHIP-14 scores of the three study groups were assessed using the Shapiro-Wilk normality test. Since the datasets deviated from the normal distribution, comparisons between groups were conducted using the Kruskal Wallis and Dunn’s tests, under non-parametric assumptions. The scores for each study group were presented as Box and Whisker plots, where the box indicated the interquartile range, and the whiskers indicate the minimum and maximum values. Domain scores were calculated by the sum of the scores for the two questions for each, and mean domain scores in study groups were presented as a stacked bar chart. Correlation between monthly income and OHIP scores were assessed using Spearman’s correlation coefficient. Participants’ total OHIP-14 score was categorized as high and low using the mean value as the cut-off point. Accordingly, the cut-off value for the OSCC group was 24, and for the OED group it was 14. Associations between high and low OHQoL categories within OSCC and OED groups and socioeconomic variables were assessed using the Chi Square test and results of this analysis are presented in Supplement Data, For all interpretations p < 0.05 was considered as statistically significant difference.
Results
Characteristics of study groups
Characteristics and mean OHIP-14 scores of the study groups.
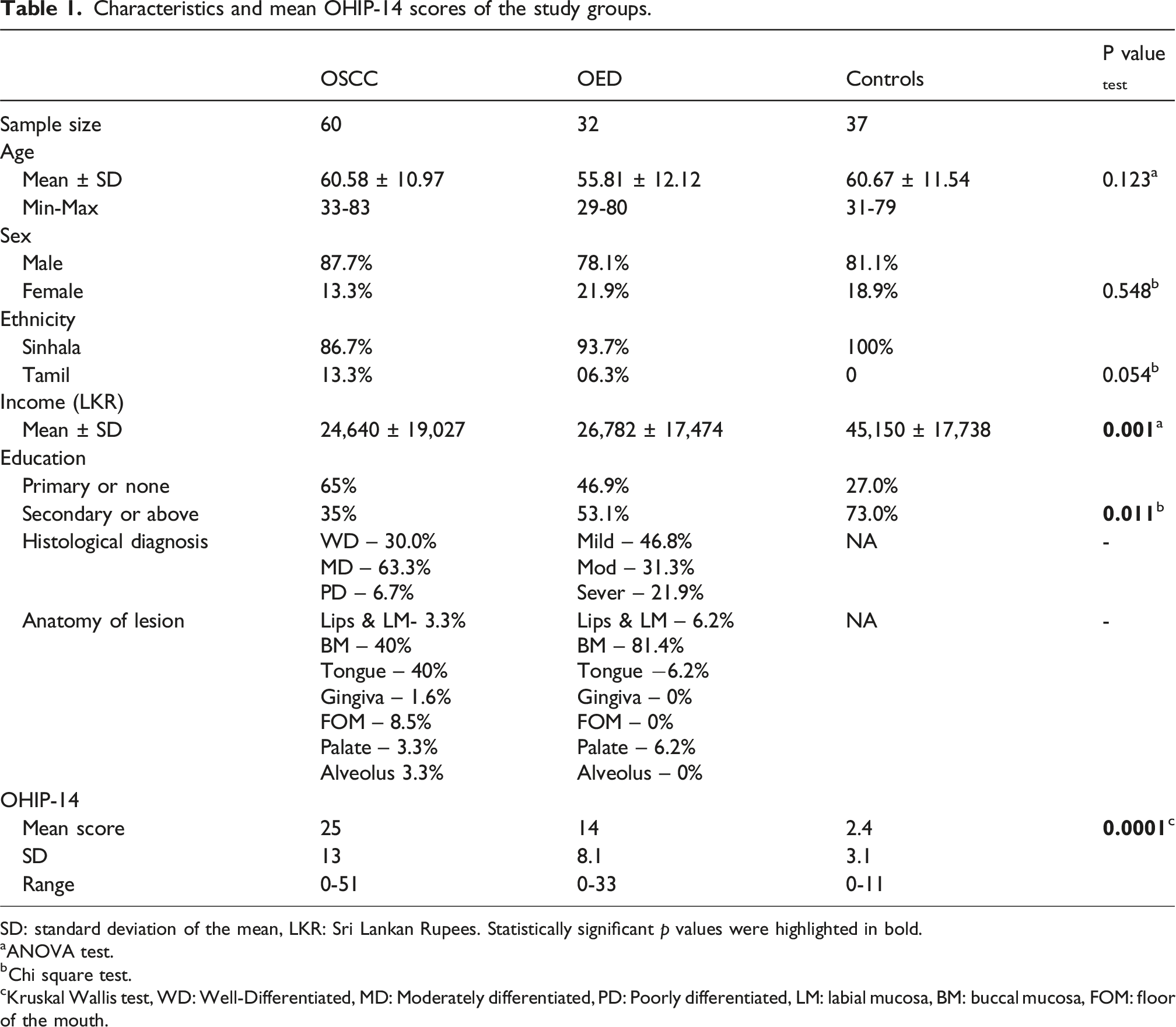
SD: standard deviation of the mean, LKR: Sri Lankan Rupees. Statistically significant p values were highlighted in bold.
aANOVA test.
bChi square test.
cKruskal Wallis test, WD: Well-Differentiated, MD: Moderately differentiated, PD: Poorly differentiated, LM: labial mucosa, BM: buccal mucosa, FOM: floor of the mouth.
OHQoL scores using OHIP-14 tool
The internal consistency of the translated OHIP-14 questionnaire used in this study was excellent (Cronbach’s α = 0.908). For OSCC, OED and controls, the total OHIP-14 mean ± SD scores were 25 ± 13, 14 ± 8.1, and 2.4 ± 3.3 respectively (Figure 1). As expected, worse OHQoL was observed for OSCC followed by OED, and the lowest scores indicating a better OHQoL were observed in the disease-free control group (Figure 1). Comparison of the total mean OHIP-14 scores in the three study groups. Kruskal Wallis test, p value <0.0001. Multiple comparisons between groups were performed using Dunns tests by comparing the mean rank. ****p value <0.0001, **p value = 0.008.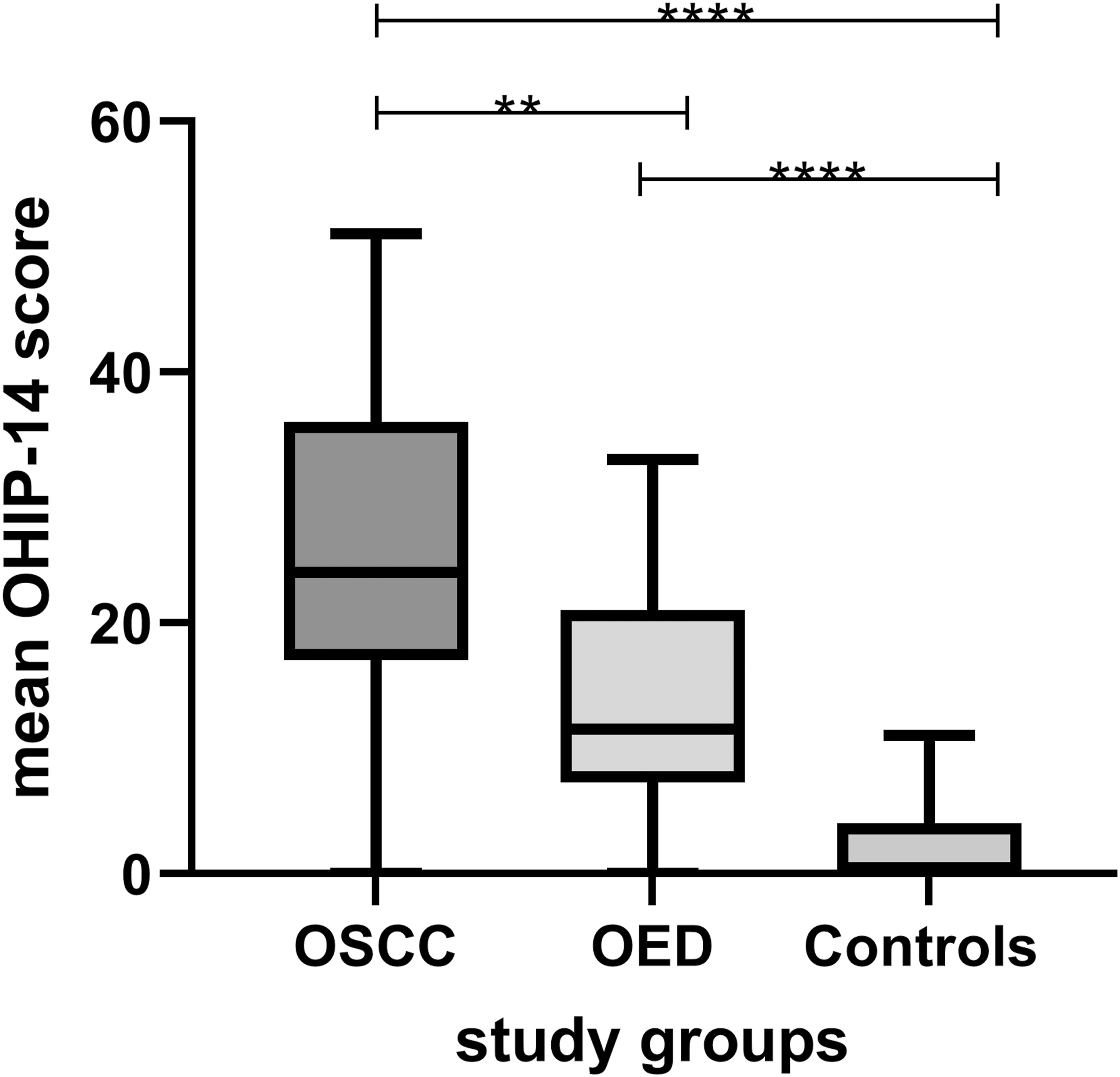
The mean scores for each domain in the three study groups are presented in Figure 2. The domains that reported the highest mean scores in OSCC and OED groups were physical pain (D2) and psychological disability (D4). Functional limitations (D1), physical pain (D2), and physical disability (D4) were the domains that reported highest scores in the disease-free controls. Unsurprisingly, all the domains had higher mean scores in the OSCC group, followed by the OED group indicating a poorer OHQoL with disease progression. Mean OHIP-14 domain scores of the study groups. D1: functional limitations, D2: physical pain, D3: psychological discomfort, D4: physical disability, D5: psychological disability, D6: social disability, D7: handicap.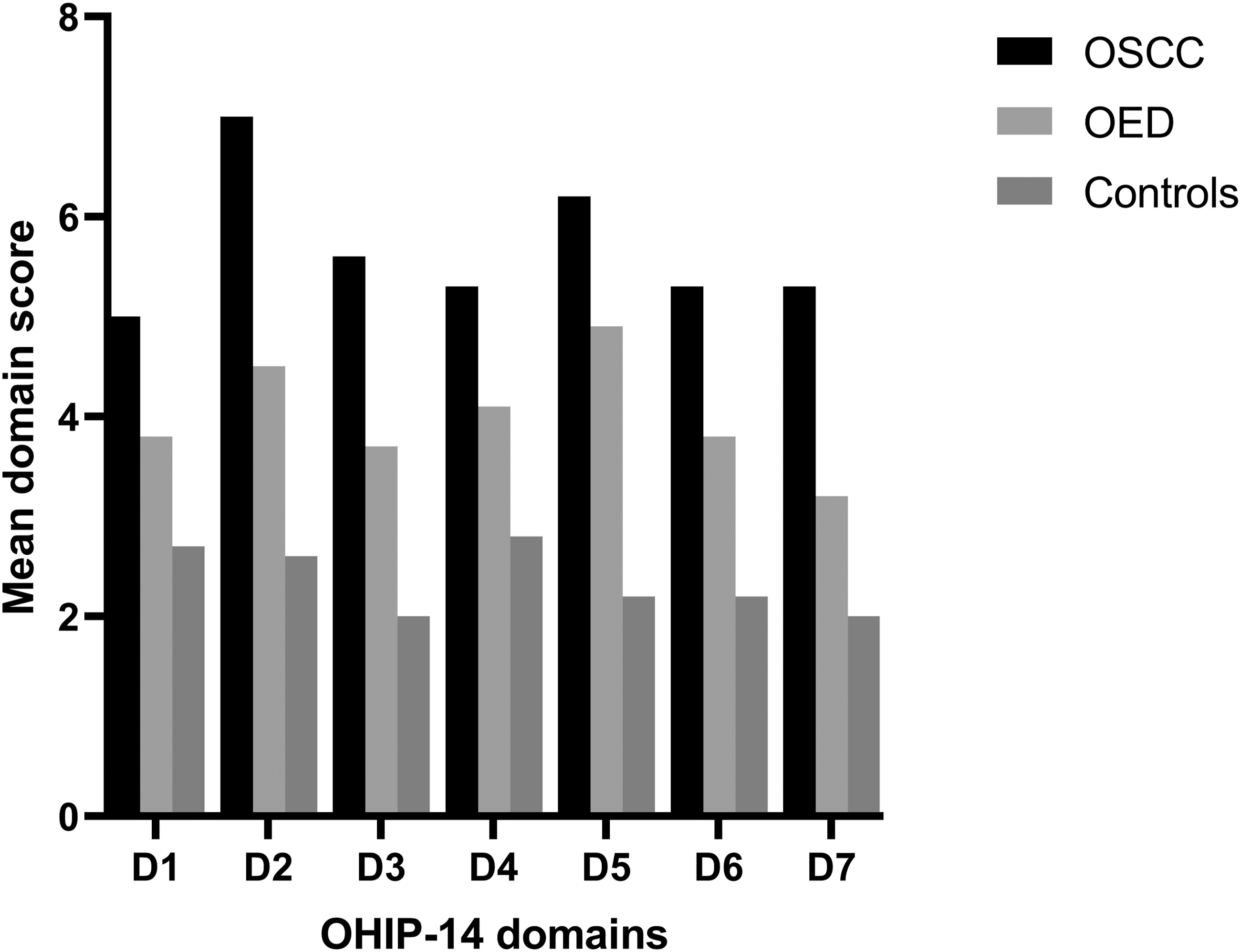
Associations between OHQoL and income
Correlation between individual income and OHIP-14 scores was assessed in patients. A negative correlation was reported in both the OSCC and OED groups; a statistically significant (p = 0.0119) negative correlation (Spearman’s rho = −0.495) was observed in the OSCC group. Figure 3 shows the correlation between total OHIP-14 score and monthly income in Sri Lankan Rupees (LKR) in study participants with fixed monthly income in the OSCC (n = 25) and OED (n = 23) groups. Results demonstrate a tendency towards worse OHQoL with reduction in monthly income. Correlation between total OHIP-14 score and monthly income in patients. This graph includes data from participants who had independent monthly income among the OSCC and OED groups (the rest of the cohort were dependent in terms of their income). As a higher OHIP score indicates worse OHQoL, this result indicates that worse OHQoL was associated with low monthly income.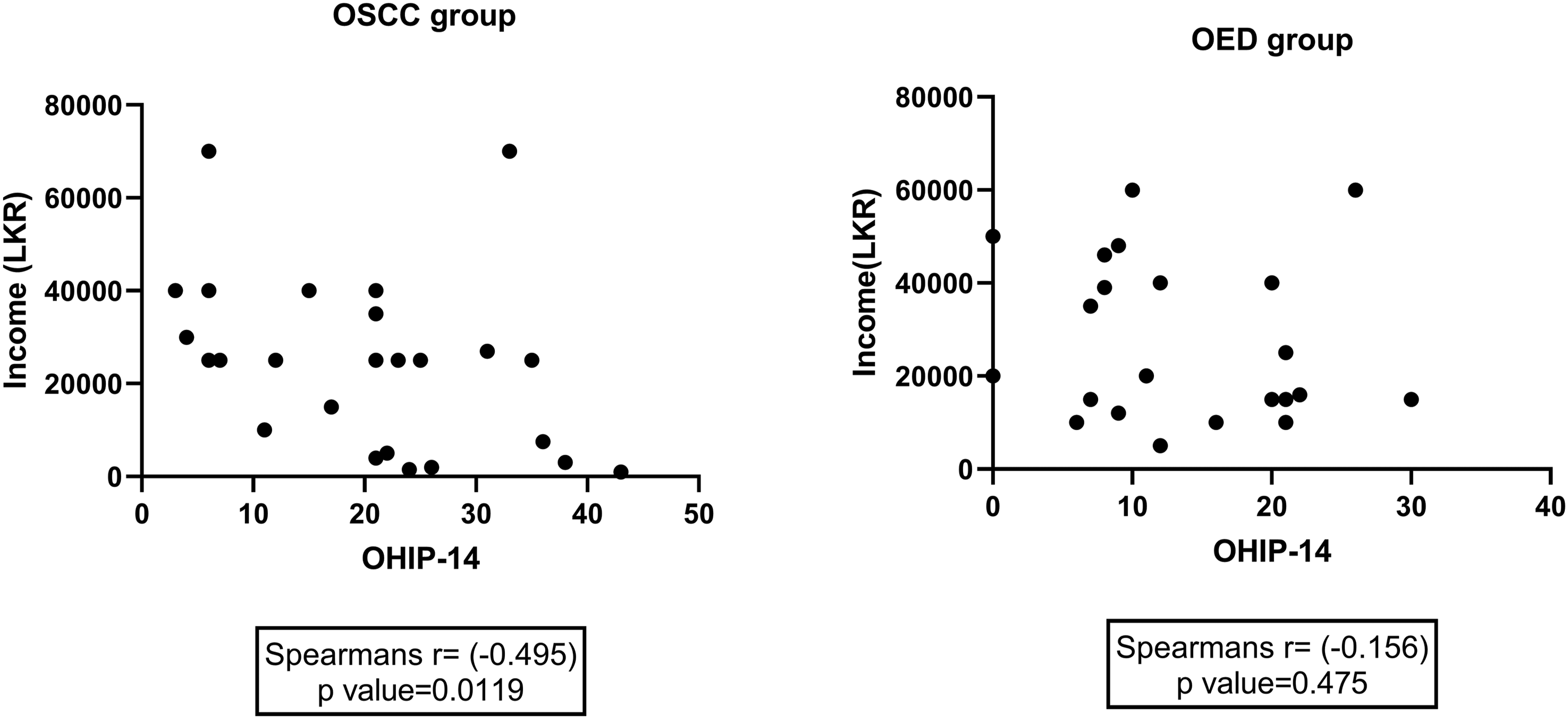
Discussion
OSCC and OED are significant public health problems in Sri Lanka, demonstrating an increasing trend in the male population (Perera et al., 2021). Betel quid (chewing smokeless tobacco and Arecanut), smoking, and alcohol drinking are the main risk factors for OSCC. Sociodemographic variables were shown to be correlated to oral health, and OSCC is commonly identified in the low socioeconomic strata of the population (Edirisinghe et al., 2022). OHQoL is defined as ‘a multidimensional construct that includes a subjective evaluation of the individual’s oral health, functional well-being, emotional well-being, expectations and satisfaction with care, and sense of self’ (Sischo and Broder, 2011). Biological, socio-economic, and health system related determinants can influence OHQoL in disease-free adults (Gupta, 2014). The current study aimed to investigate the OHQoL in OSCC and OED patients at the time of diagnosis using the OHIP-14 tool. The specific objectives were to identify OHQoL domains that were more affected in the study groups and potential associations between OHQoL and sociodemographic variables. The main findings of the study included OHIP-14 scores in study groups, domain level comparison of OHQoL within study groups and associations between income status and OHQoL in patients.
In agreement with published studies, our results indicated worse OHQoL in OSCC patients, followed by OED and the disease-free group. In the current study, the mean overall OHIP-14 score for OSCC patients was 25. Similar findings were reported in OSCC patients undergoing treatment in Brazil, where the mean OHIP-14 was reported as 22 (De Melo et al., 2019). A much lower mean score (8.8) was reported in OSCC patients from Germany (Karbach and Al-nawas, 2014). Lower mean scores indicate better OHQoL in patients from Germany, compared to patients from Brazil and Sri Lanka, indicating that population-specific factors can be associated with OHQoL in patients with the same disease. The mean OHIP-14 score for the OED group was 14 in the current dataset, slightly higher than another study (mean = 11.5) conducted in UK (Alsoghier et al., 2021). This variation in OHIP-14 scores in different populations could be related to differences in the health care system in addition to sociodemographic factors. Therefore, population-specific characteristics and associated sociodemographic factors should be investigated to provide optimised management strategies to maximise OHQoL during treatment.
One objective of the present study was to identify the most affected OHQoL domains in study groups. Interestingly, in both OSCC and OED patients, physical pain (D2) and psychological disability (D4) were the domains that reported the highest scores, indicating that they were main contributing factors for compromised OHQoL in patients. Psychological disability refers to limitations in mental or emotional functioning as a result of a disease or diagnosis. Results of this study can also suggest that absence of pain and lack of oncological awareness may predispose to ignorance of initial lesions and facilitate delayed presentation in OSCC patients. Similar to the current finding, physical pain and psychological discomfort were the significant domains in patients with oral lichen planus, leukoplakia, and OED (Alsoghier et al., 2021; Karbach and Al-nawas, 2014). On the other hand, the OHQoL domains that reported high scores in the control group were functional limitations (D1), physical pain (D2), and physical disability (D4).
A recent study in Sri Lanka identified that, in oral cancer patients following radiotherapy, there were variable effects on different OHQoL domains; however, this study assessed OHQoL using the EORTC QLQ-OH15 tool, and the domains assessed in this tool were eating problems, gum and speech problems, soreness and teeth (Kosgallana et al., 2023), mainly focusing on the functional aspects of OHQoL. Their study reported associations between post-treatment OHQoL scores with baseline OHQoL at the time of diagnosis, marital status and the site of metastasis (Kosgallana et al., 2023). In a study conducted in India, Gondivkar and colleagues (2021) conducted a domain-level analysis of OHQoL using the OHIP-14 tool in oral cancer patients following treatment and reported that functional limitations, physical pain and physical disability were the domains significantly associated with OHQoL (Gondivkar et al., 2021). These findings hold translational significance for clinicians, highlighting the various domains of OHQoL that should be assessed and addressed at the time of diagnosis to optimise post-treatment outcomes.
Psychological disability may arise in patients when they become aware of the diagnosis of cancer or a lesion that may develop into it, due to the associated stigma of the word “cancer.” Studies have revealed that compromised OHQoL is associated with conditions like depression, anxiety, malnutrition, and overall low quality of life in patients with OSCC (Barrios et al., 2015; Hassel et al., 2012; Kamatchinathan et al., 2016; Weeratunga EB et al., 2021). Quality of life affects biological pathways such as inflammation, neurotransmission, pain perception, catecholamine release and hormone secretion (Hassel et al., 2012; Kamatchinathan et al., 2016; Weeratunga EB et al., 2021). Therefore, low OHQoL at the time of diagnosis may be a significant factor that compromises the recovery and survival of these patients in the background of an inadequate support system. The need for psychological support at the time of diagnosis for OSCC and OED patients has been previously reported (Alsoghier et al., 2021; Kamatchinathan et al., 2016). In Sri Lanka, 6% of patients with OSCC were identified with severe depressive symptoms (Weeratunga EB et al., 2021); this can be a long-term consequence of compromised OHQoL. In a cohort study assessing OHQoL in recurrence-free patients treated for OSCC, the OHQoL predicted the psychological outcomes such as depression and anxiety (Hassel et al., 2012). Facial disfigurement and social support were factors associated with psychological adjustment in OSCC patients (Wang et al., 2018). For the present study, patients were recruited from two tertiary care hospitals in Colombo, Sri Lanka; from these, only one centre (National Cancer Hospital, Maharagama) had a unit dedicated to delivering counselling and psychological support to cancer patients. Even in this centre, psychological support for patients with OED was an overlooked treatment need. Incorporating tailored counselling into care pathways for all patients diagnosed with OSCC and OED may improve oncological awareness and mental well-being, improve OHQoL and help achieve successful treatment outcomes.
The results of the current study identified that monthly income was positively correlated with OHQoL in study participants, indicating that low income was associated with worse OHQoL. This finding suggests that apart from biological factors like oral disease, other socioeconomic factors are significant predictors of OHQoL. A systematic review including 40 studies on oral cancer patients concluded that, compared to the high socioeconomic stratum, low-income category had a pooled odd ratio of 2.4 in developing oral cancer (Conway et al., 2008). Further, the same review revealed that low socioeconomic status was associated with oral cancer consistently across both sexes, despite global regions, and the countries’ economic development status. A meta-analysis on healthy populations concluded that individuals with low SES had poorer OHQoL, regardless of their country’s economic classification, socio-economic indicators, and age group (Knorst et al., 2021). Researchers have highlighted the prevalence of high risk behaviours such as smoking and smokeless tobacco abuse, alcohol and betel quid consumption in explaining the association between low SES and oral cancer (Auluck et al., 2016; Azimi et al., 2020). In a study conducted in Europe and South America, high stress levels and low socioeconomic status were contributing factors for HNC (Conway et al., 2021).
In Sri Lanka, basic screening and dental treatments are provided by the state hospitals free of end-user charges. However, there are a limited number of centres that have facilities to diagnose and treat OSCC, and most of them are located in urban areas. Loss of daily wages, long travelling distance and high travelling costs are factors that delay the presentation of patients in low SES to treatment centres. High prevalence of risk habits, malnourishment, unsafe sexual practices, unawareness of the signs and symptoms of early oral cancer lesions, high work-related stress, job insecurity, unemployment, crime-related anxiety, debt, lack of social capital, and a lack of community cohesion were identified as contributing factors for high prevalence and delayed presentation of OSCC patients in the low-income and middle-income strata in Sri Lanka (Senevirathna et al., 2023). Community screening, especially in high-risk groups, and outreach programs along with early assessment of OHQoL, would be an effective approach for early detection of OSCC and OED in the low socioeconomic group. Limited and unbalanced sample size in study groups, absence of comprehensive assessment of oral health status and lack of follow-up were limitations of the current study.
Conclusions and recommendations
This study assessed OHQoL using the OHIP-14 tool in a group of OSCC and OED patients in Sri Lanka. Main findings reveal that physical pain and psychological disability were the most compromised domains of OHQoL in patients. Further, an association between low income and poor OHQoL was reported in the OSCC group. Existing care and support systems for OSCC and OED patients in Sri Lanka may be strengthened by regular OHQoL assessment, increasing awareness of different domains affecting OHQoL, effective pain management, integration of tailored counselling into treatment pathways, and expanded outreach programs for low socioeconomic groups.
Supplemental Material
Supplemental Material - Oral health-related quality of life in patients with oral squamous cell carcinoma and oral epithelial dysplasia – A cross sectional study in Sri Lanka
Supplemental Material for Oral health-related quality of life in patients with oral squamous cell carcinoma and oral epithelial dysplasia – A cross sectional study in Sri Lanka by Nadisha Sewwandi Piyarathne, Kalupe Ranasinghege Dhanushka, W. J. Wijesingha, Jap Jayasinghe, Rasha Abu-Eid, Ekta Gupta in Community Dental Health.
Footnotes
Acknowledgements
Authors would like to thank the valuable contributions from all study participants. For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission.
Author contributions
NSP: data collection, data analysis, writing the original draft. KRD & WJW: patient screening and recruitment, data validation. EG, RAE & JJ: conceptualization, study design, supervision, editing and reviewing the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.