
Abstract
Children’s dental health is closely linked to the knowledge and practices of parents and caregivers, especially regarding caries prevention. This study aims to assess their knowledge and attitudes toward fluoride treatments and dental sealants for children aged 6 to 12 in the Eastern Province of Saudi Arabia. A cross-sectional study was conducted using convenience sampling to recruit parents and caregivers from the Eastern Province. Participants were invited to complete an online questionnaire shared via social media platforms such as Twitter, Facebook, and Snapchat. A total of 336 parents and caregivers from the Eastern Province participated. Most parents demonstrated good knowledge of caries prevention, especially regarding regular toothpaste use (97%), brushing (96.4%), and filling decayed teeth (85.4%). Awareness of fluoride mouthwash, fluoridated water, flossing, and professional fluoride application was lower (<70%). Regular dental visits (69.6%) and brushing children’s teeth (88.4%) were common, while daily flossing (53.3%), professional fluoride application (59.2%), fluoride mouthwash use (51.8%), and consumption of fluoridated water (49.1%) were less frequent. Sealant application was reported by 61.3% of participants. While parents show strong engagement with basic dental care, gaps remain in understanding and utilizing additional preventive measures. Targeted educational efforts are recommended to raise awareness about fluoride applications, promote daily flossing, and encourage the establishment of a dental home by age one.
Keywords
Introduction
Childhood Caries remains a significant public health challenge (Garg et al., 2025). The ramifications of untreated ECC extend beyond localized tooth decay, contributing to systemic infections, nutritional deficiencies, and impaired cognitive development due to chronic pain and sleep disturbances (Neves et al., 2019). Furthermore, the economic and emotional burdens of managing advanced caries—often requiring invasive treatments under general anesthesia—highlight the urgency of preventive strategies (Nair and Singh, 2016).
The global prevalence of cavitated dentine carious lesions in children varies widely across age groups, geographic regions, and socioeconomic levels. In 5- and 6-year-olds, the median prevalence ranges from 49% to 83.4%. In 12-year-olds, the median prevalence ranges from as low as 42.2% up to 69.4% (Frencken et al., 2017). In Saudi Arabia, the prevalence of dental caries among children is alarmingly high, with recent statistics indicating that 93.7% of 12-year-olds and 96% of 6-year-olds are affected (Ministry of Health, 2024). These rates exceed global averages and underscore systemic gaps in preventive care and health education, highlighting the urgent need for preventive measures, oral health education, and improved access to dental care in Saudi Arabia (Aqeeli et al., 2021).
Risk factors for ECC are multifaceted, encompassing prolonged breastfeeding or bottle-feeding practices, frequent consumption of sugary snacks, and inadequate oral hygiene routines (Tahani et al., 2017). Cultural practices, such as the delayed introduction of toothbrushing and reliance on traditional remedies, further exacerbate susceptibility to caries (Alshunaiber et al., 2019).
Topical fluoride applications and pit-and-fissure sealants are evidence-based interventions endorsed by the American Academy of Pediatric Dentistry for reducing caries incidence by up to 80% (American Academy of Pediatric Dentistry, 2024). Despite their efficacy, utilization rates remain suboptimal (Al Mutairi, 2020; Deep et al., 2020).
Parents and caregivers serve as primary influencers of children’s oral health behaviours, yet studies consistently reveal critical gaps in their knowledge, both in Western countries (Calcagnile et al., 2019; Mariotti et al., 2025; Vozza et al., 2017) as well as in studies from Saudi Arabia (Nassar et al., 2022; Saheb et al., 2023). These knowledge deficits are compounded by cultural attitudes that prioritize reactive over preventive care, as many families seek dental treatment only in response to pain or visible pathology (Walker et al., 2017). Therefore, implementing oral health promotion programs targeting parents, starting at school, is essential to reduce children’s oral health risks (Calcagnile et al., 2019; Mariotti et al., 2025; Vozza et al., 2017).
While existing studies have highlighted general trends in parental knowledge regarding children’s oral health, significant regional disparities within Saudi Arabia have yet to be thoroughly investigated. Most research has concentrated on urban cities like Riyadh and Jeddah, leaving a gap in knowledge regarding the Eastern Province, where socioeconomic and cultural factors may differ considerably (Alyousef et al., 2021; Kadi, 2024). Additionally, the relationship between parental attitudes, preventive practices, and broader health policies—including school-based sealant programs—has not been systematically assessed within the Saudi context. This lack of comprehensive understanding hinders the development of targeted interventions that can effectively align with local cultural values and practical realities.
Parental knowledge and practices strongly influence children’s oral health throughout childhood. Studying parents of school-aged children (6–12 years) provides insights into oral health practices that often originate earlier and affect younger siblings. Thus, findings on this population can inform strategies to promote oral health starting in preschool and continuing through later childhood. By addressing the gaps in knowledge and understanding of parental attitudes towards caries prevention methods, this study aims to inform more effective strategies for improving oral health outcomes in the Eastern Province of Saudi Arabia. This research seeks to determine what extent the parents and caregivers in the Eastern Province of Saudi Arabia perceive the importance of children’s caries prevention methods and what prevention methods are being used.
Methods
Research design
This cross-sectional study examines the knowledge and practices of parents and caregivers of children aged 6 to 12 years towards the use of fluoride treatment and dental sealants in the Eastern Province of Saudi Arabia. The study obtained ethical approval by Prince Sultan Military College of Health Sciences Institutional Review Board (Approval number IRB-2024-DOH-009).
Participants
Using the convenience sampling method, parents and caregivers from the Eastern Province of Saudi Arabia served as the research sample in this study. The target sample for this study consisted of parents and caregivers of children aged 6 to 12 years. This age group is critical for dental health interventions, as children are transitioning from primary to permanent teeth and are particularly susceptible to dental caries. The study focused on the Eastern Province due to its unique sociocultural characteristics. Selecting this region allows for targeted insights into the population’s specific oral health behaviors and challenges. Additionally, logistical considerations such as accessibility, resource availability, and existing collaborations facilitated focused data collection in this area. Findings from the Eastern Province may provide a valuable reference point for similar regions and inform region-specific interventions.
The sample size calculation was based using the following formula:
We have set the response rate to be 50% as this ensures the highest sample size when the actual proportion is unknown or cannot be reliably inferred from previous studies. Accordingly, the minimal calculated sample under these assumptions was 385 participants.
Data collection instrument
The researchers used a questionnaire as the data collection instrument for this study. The questions were prepared based on other studies (Alshunaiber et al., 2019; Alyousef et al., 2021; Kadi, 2024) and clinical guidelines published by the American Dental Association (ADA), the European Academy of Pediatric Dentistry (EAPD), and the American Academy of Pediatric Dentistry (AAPD) in the field of fluoride and fissure sealant therapy.
The questionnaire comprised three sections. The first section focused on the demographic data of the participants. The second section assessed the participants’ knowledge of caries prevention methods. The third section addressed the application of caries prevention methods. The items of the second and third sections were formulated as closed-ended questions. The response options for the second section included Important/Not important/Don’t know. The responses with “Important” were assigned one point, while those of “Not important” and “Don’t know” were assigned zero points. The responses for the third section’s questions incorporated the answers Applied/Not applied/Don’t know. The responses with “Applied” were assigned one point, and those of “Not applied” and “Don’t know” were assigned zero points. The points were summed up for each section to create total scores for knowledge and practice. Higher scores generally indicated better knowledge or more frequent application of preventive measures.
The researchers ensured the content validity of the questionnaire by submitting it to four experts in dental public health and two specialists in pediatric dentistry. Feedback from these experts was meticulously reviewed, and their comments and suggestions were incorporated to develop the final version of the questionnaire. The questionnaire, translated into Arabic, was administered through a link created via Google Forms. This link was disseminated on various social media platforms, including Twitter, Facebook, and Snapchat, inviting participants to engage with the questionnaire. All pertinent information regarding the questionnaire—its contents, the target demographic, and the method of response—was clearly communicated alongside the publication link. The participants were asked to provide consent at the start of the questionnaire.
Data analysis
All statistical analyses were conducted using R version 4.5.0 (R Core Team, 2025). Categorical variables were summarized as counts and percentages. Derived scores were assessed for normality of distribution using the Shapiro-Wilk test, skewness, kurtosis, and Q-Q plots; as they were not normally distributed, they were expressed as median and interquartile range (IQR: 25th–75th percentiles). Comparisons between two independent groups were performed using the Wilcoxon rank-sum test, with effect sizes reported as rank-biserial correlation (denoted as r). Comparisons across more than two groups were conducted using the Kruskal–Wallis test, with post-hoc pairwise comparisons adjusted for multiple testing and effect sizes reported as eta-squared (η2). Correlations between continuous variables were examined using Spearman’s rank correlation coefficient. A multivariable linear regression model was fitted to identify independent associations, with covariates selected based on relevance. Statistical significance was defined as a two-tailed p-value <0.05.
Results
A total of 411 responses were obtained. Three individuals declined to participate, and 72 had no child aged 6–12 years; thus, 336 responses were included in the analysis.
The internal consistency of the questionnaire was evaluated using Cronbach’s Alpha. The results of alpha coefficients were 0.761 (95% CI: 0.721 to 0.795) for knowledge, 0.853 (95% CI: 0.827 to 0.876) for practice, and 0.888 (95% CI: 0.870 to 0.904) for the total score, indicating good internal consistency of the questionnaire.
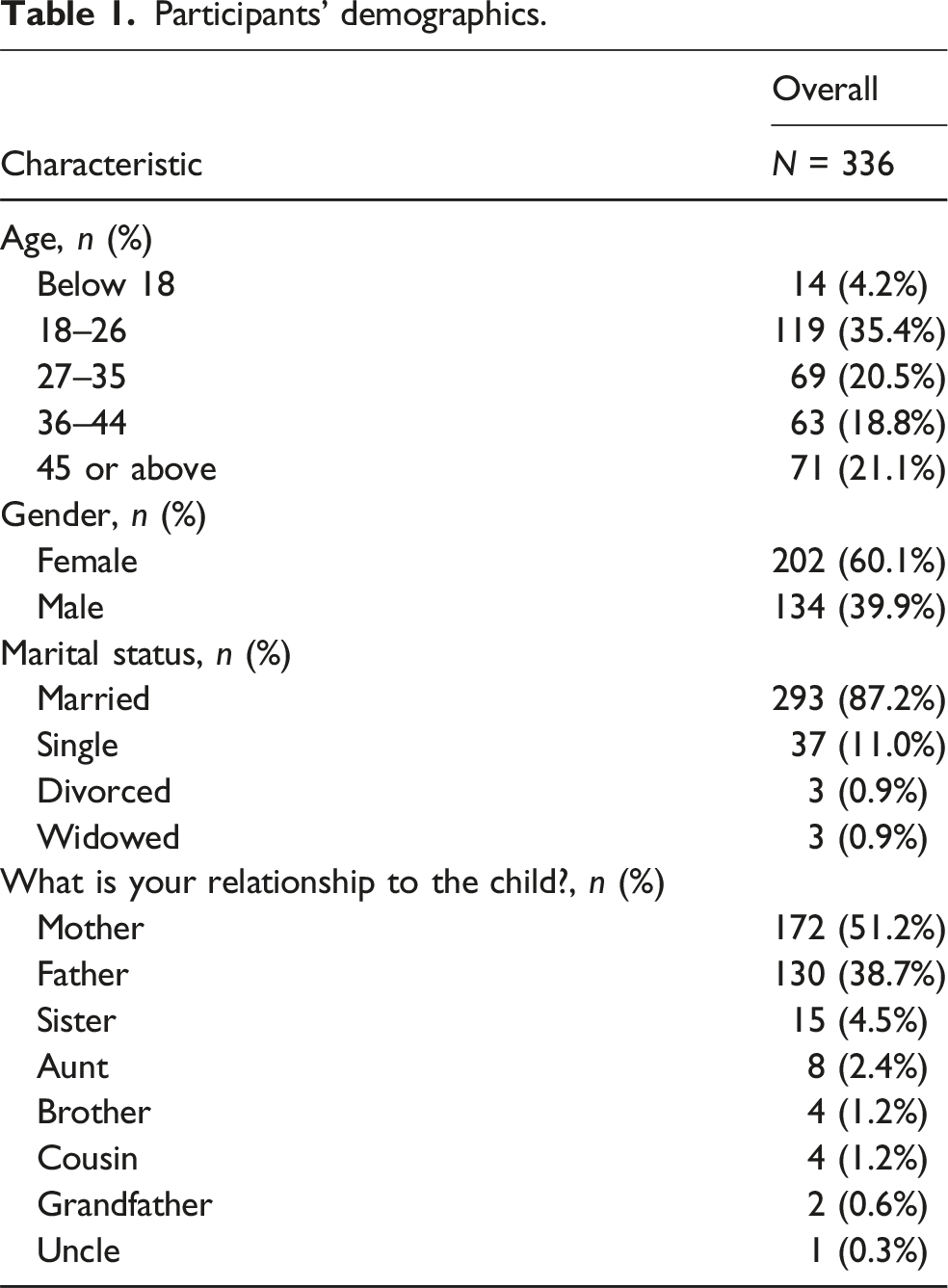
Participants’ demographics.
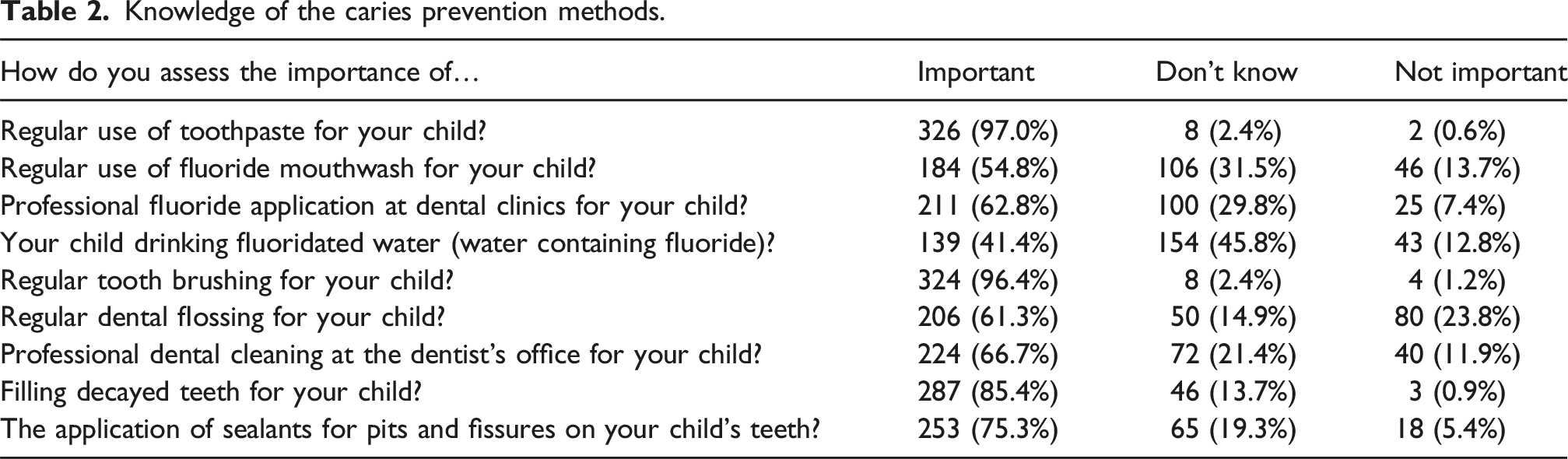
Knowledge of the caries prevention methods.
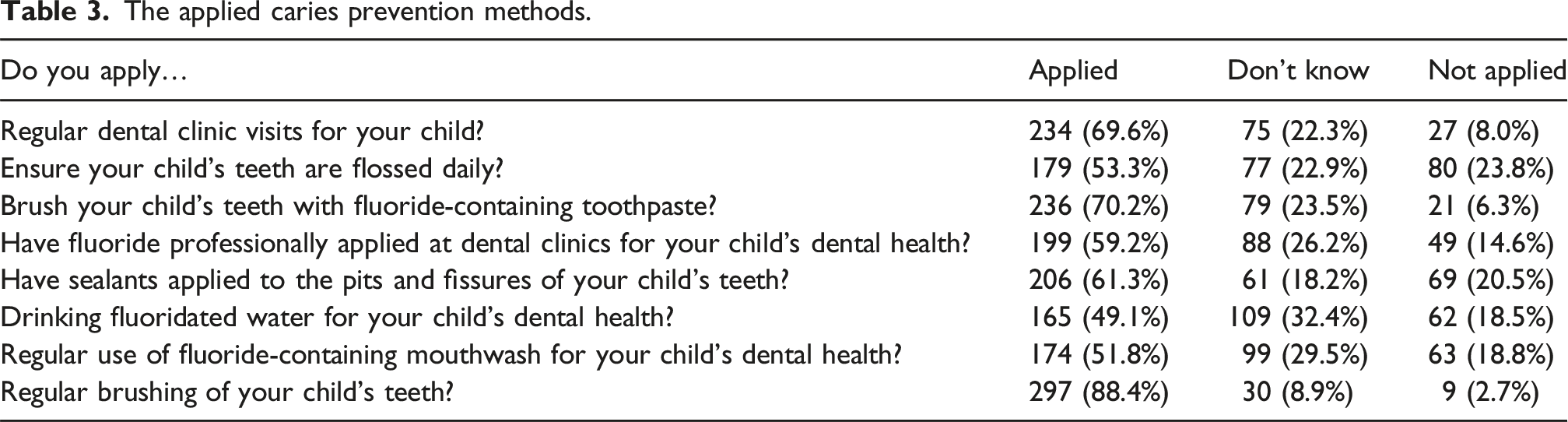
The applied caries prevention methods.
Differences in knowledge scores among the categories of demographic factors.
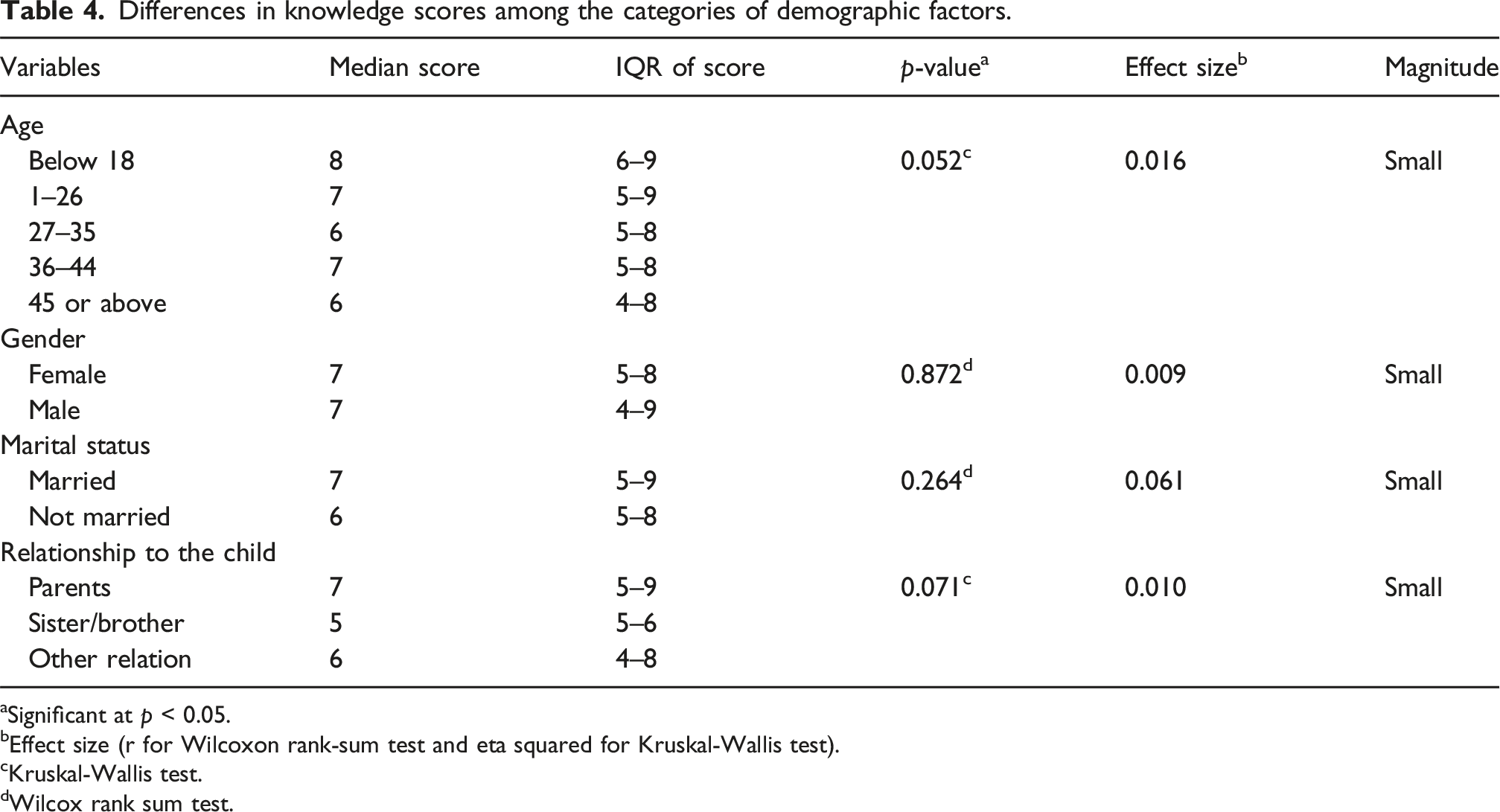
aSignificant at p < 0.05.
bEffect size (r for Wilcoxon rank-sum test and eta squared for Kruskal-Wallis test).
cKruskal-Wallis test.
dWilcox rank sum test.
Differences in practice scores among the categories of demographic factors.
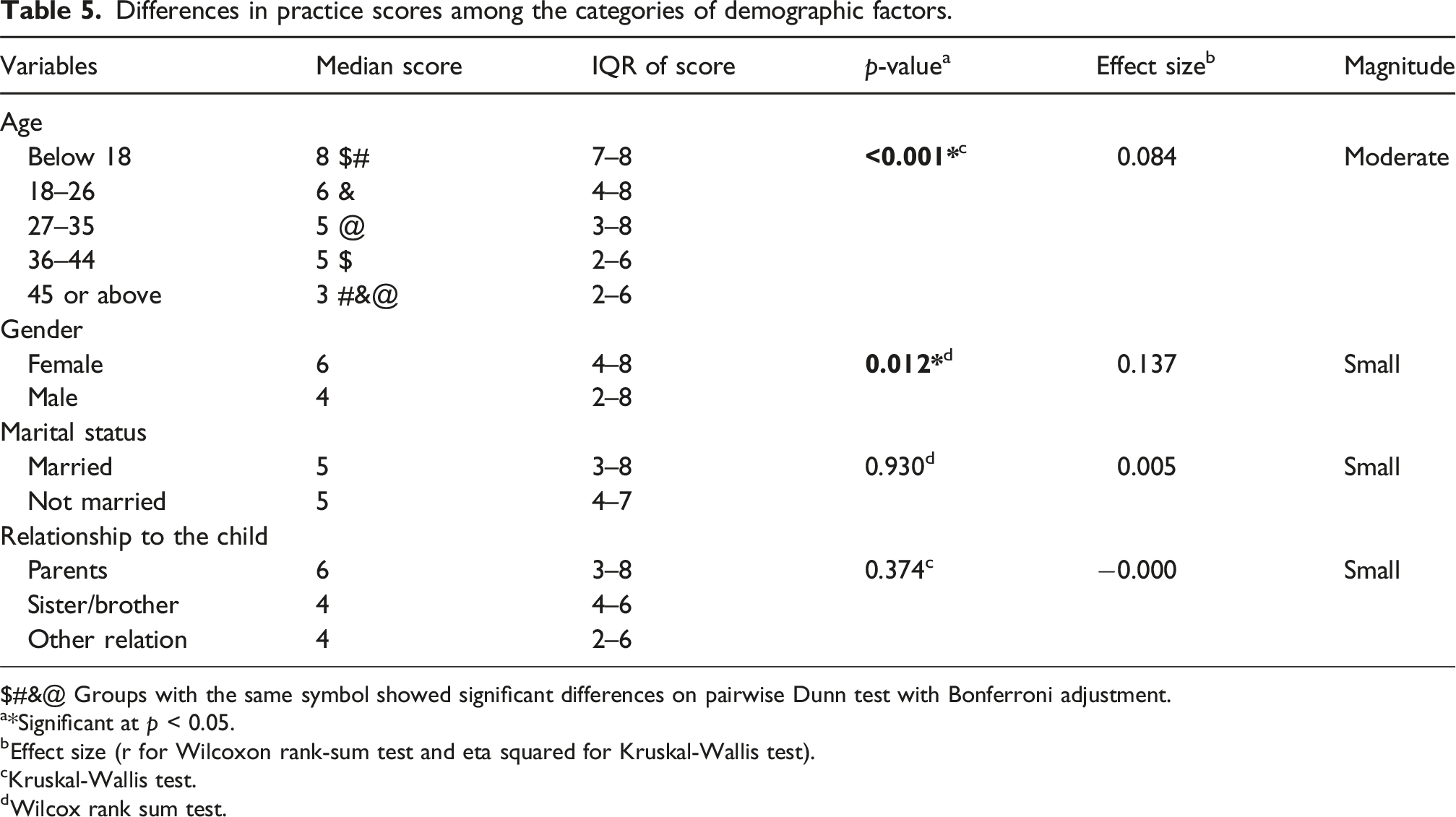
$#&@ Groups with the same symbol showed significant differences on pairwise Dunn test with Bonferroni adjustment.
a*Significant at p < 0.05.
bEffect size (r for Wilcoxon rank-sum test and eta squared for Kruskal-Wallis test).
cKruskal-Wallis test.
dWilcox rank sum test.
There was a significant, positive, strong correlation between the knowledge and practice scores (rho = 0.745, p < 0.001), indicating a tendency for an increase in practice scores with the increase in knowledge score (Figure 1). Correlation between knowledge and practice scores. r (rho): Coefficient of Spearman’s rank-order correlation, p: p-value.
Multivariable linear regression for potential factors affecting the practice score.
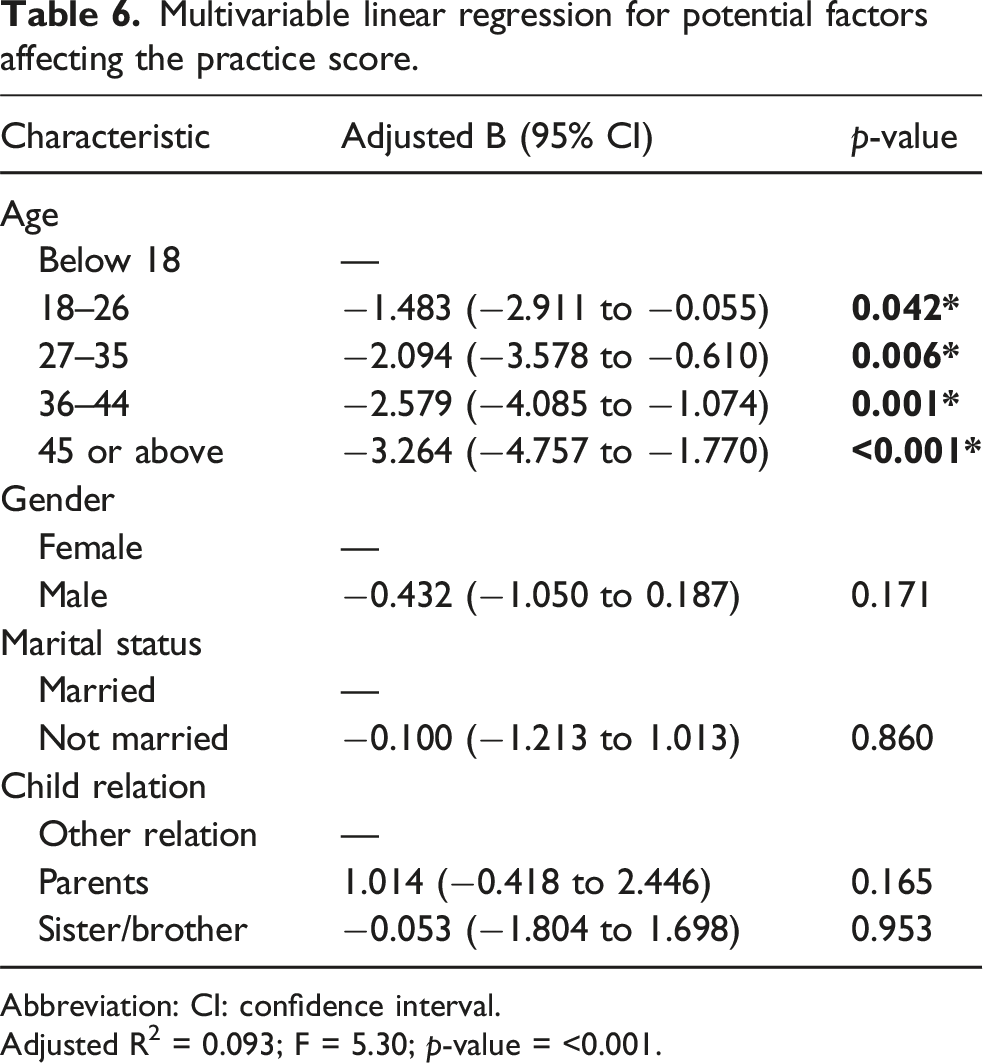
Abbreviation: CI: confidence interval.
Adjusted R2 = 0.093; F = 5.30; p-value = <0.001.
Discussion
The findings from the present study on parental knowledge regarding caries prevention methods reveal a good understanding of basic dental hygiene practices, particularly in the areas of regular toothpaste use, tooth brushing, and filling decayed teeth. Such findings suggest that effective public health messaging has successfully conveyed the significance of these fundamental practices in maintaining oral health.
However, the study also highlights notable gaps in knowledge regarding other preventive measures, particularly the awareness regarding fluoride mouthwash, drinking fluoridated water, dental flossing, and professional fluoride application. This indicates a critical area for educational intervention to increase awareness regarding the advantages of professional dental care, which has been shown to significantly reduce the incidence of dental caries in children. These practices are considered cost-effective public health measures that have been proven to reduce dental decay (Horst et al., 2018). Flossing maintains oral health by removing plaque and food particles from between teeth where toothbrushes cannot reach (Muralidharan et al., 2019).
Finally, regarding the application of sealants, 75.3% consider them important, yet 19.3% remained unsure. This highlights a relatively good understanding of sealants’ preventive role but also indicates a need for further education to bolster confidence in this preventive measure, as sealants have been shown to significantly reduce the risk of caries in children (Ng et al., 2023). Previous studies from Italy and Spain have reported that parents’ awareness regarding dental sealants is unsatisfactory (Calcagnile et al., 2019; Mariotti et al., 2025).
The findings also provided a comprehensive overview of the application of various caries prevention methods among parents and caregivers, highlighting both strengths and areas needing improvement. We found that 69.6% of the participants have reported making regular dental visits for their children, indicating a strong commitment to preventive dental care. Such commitment is crucial for maintaining good oral health from an early age, as emphasized by the American Academy of Pediatric Dentistry (2024), underscoring early dental visits’ significance in preventing future dental issues. However, there is considerable room for improvement in ensuring all children receive regular professional care. This observation aligns with previous studies in Saudi Arabia, which noted that early dental visits are often overlooked, particularly in certain demographics (Al Mejmaj et al., 2022; Alhareky and Nazir, 2021; AlHumaid et al., 2018; Murshid, 2016). The low adherence to regular dental check-ups is noteworthy, particularly given the high quality and accessibility of medical care facilities available to Saudi citizens.
The most frequently applied practices included regular brushing of children’s teeth (88.4%) and the use of fluoride-containing toothpaste (70.2%). These findings reflect a strong understanding of the significance of toothbrushing and fluoride in preventing caries. A recent systematic review has reported widely varying rates of using fluoride-containing toothpastes for children, which differed considerably even in the same country (range: 20.7% to 94.8%) (Aiuto et al., 2022).
In contrast, adherence to daily flossing (53.3%), having fluoride professionally applied at dental clinics (59.2%), regular use of fluoride-containing mouthwash (51.8%), and drinking fluoridated water (49.1%) were notably less practiced. These findings highlight a significant gap in compliance with some of the key components of oral hygiene. The results underscore the need for educational initiatives aimed at emphasizing the importance of daily flossing and fluoride, which are essential for preventing caries (Stangvaltaite-Mouhat et al., 2021). This need for enhanced knowledge is further supported by similar previous studies among the Saudi population (Alyousef et al., 2021; Kannan et al., 2020), which found that many parents lacked sufficient awareness regarding the importance of flossing in children’s oral hygiene routines. Also, Aqeeli et al. (2021) in Al-Madinah, Saudi Arabia, identified a lack of awareness regarding the benefits of professional dental interventions. Previous studies have also reported a lack of sufficient fluoride supplies for children. Mariotti et al. (2025) reported low rates of providing fluoride supplements to children among Spanish parents. In the Eastern Province of Saudi Arabia, Aljami et al. (2022) found that only 24.6% of the parents of 3–6-year-old children had applied fluoride varnish to their children before, and only 29% of them were satisfied with the experience. Another study from Jeddah, Saudi Arabia, reported that two-thirds of parents had not heard before about fluoride varnish and more than half of the parents were not sure about its safety (Almehmadi et al., 2022).
The application of sealants was admitted by 61.3% of participants, suggesting a reasonable level of awareness regarding sealants and their role in preventing decay, particularly in children who are at higher risk. However, it also points to the potential for enhanced education about their benefits, as research has demonstrated the effectiveness and safety of sealants for preventing or arresting the progression of non-cavitated carious lesions (Wright et al., 2016).
Among our sample, there were no significant differences in the knowledge score in relation to age, gender, marital status, or relation to the child. Similarly, Al Mejmaj et al. (2022) conducted a pilot study in Buraidah City, Saudi Arabia, among parents of 2–6-year-old children, and found a lack of significant difference in oral health knowledge between mothers and fathers. These results partially align with those of Lakshmanan and Gurunathan (2020) in India, who reported a significant difference only for age on bivariate analysis, while there was no significant difference between fathers and mothers.
As regards the participants’ factors potentially associated with practice scores, we found that younger age and female gender had higher scores. However, on adjusting for participants’ characteristics, only age was identified as significantly associated with differences in the practice scores. On the other hand, Lakshmanan and Gurunathan (2020) reported that age and sex were not associated with significant differences in practice scores.
The differences among the age groups may be explained by the observation that younger caregivers often have more current knowledge and greater motivation to implement preventive oral health measures. They may also have fewer competing responsibilities and more physical ability to supervise children’s oral hygiene. In contrast, older caregivers might face time constraints or rely on established habits, leading to reduced adherence to recommended practices as age increases. This aligns with evidence that parental involvement and supervision tend to decrease with child age (Wikle and Cullen, 2023), which potentially affects oral hygiene behaviors.
The present study has found a strong positive correlation between the knowledge and practice scores, underscoring the importance of elevating awareness levels and how that potentially improves oral hygiene practices. This finding disagrees with that of Lakshmanan and Gurunathan (2020), who reported a lack of significant correlation between knowledge and practice scores of parents.
The insights presented by the current study are potentially marred by some limitations. First, the cross-sectional design of the study prevents the establishment of causality between parents’ demographics and their knowledge/practices. Second, the employment of a self-administered questionnaire may introduce recall bias. Also, some participants may select some answers because they are more socially appealing. Third, the study focused on participants from the Eastern province, which may limit the generalizability of the results to other geographic regions. Fourth, the study used the convenience sampling technique, which is quick, cost-effective, and suitable for exploratory studies. However, convenience sampling may introduce bias through overrepresenting certain groups that are more motivated to participate in the survey and underrepresenting other, less motivated groups, which limits the generalizability of the results.
Conclusion
In conclusion, while parents and caregivers show strong knowledge and engagement with basic caries prevention, significant gaps persist in awareness and adherence to fluoride mouthwash, fluoridated water, daily flossing, and professional fluoride application. Regular dental visits and tooth brushing are common, but the use of additional preventive measures is inconsistent. Targeted education through community workshops, schools, and pediatric clinics is needed to increase awareness and promote comprehensive oral health behaviors, including establishing a dental home by age one.
In Saudi Arabia, where childhood dental caries prevalence remains high, integrating such educational programs into existing public health initiatives is crucial. Programs like the School Dental Prevention Program (SDPP), the supervised toothbrushing program (“TOPS”), and national campaigns under Vision 2030 are key platforms for enhancing parental engagement and preventive care. Leveraging schools, healthcare centers, and digital tools alongside the active involvement of dental professionals can effectively address these gaps, contributing to improved oral health outcomes for Saudi children.
Footnotes
Ethical considerations
The study obtained ethical approval by Prince Sultan Military College of Health Sciences Institutional Review board (Approval number IRB-2024-DOH-009).
Consent to participate
Consent to participate was the first question to be answered before being able to start the questionnaire.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.