
Abstract
Sexuality is central to well-being in many romantic relationships. Equity theory suggests that perceiving equal contributions within the relationship—presumably also within the sexual relationship—is associated with better outcomes, while a perceived imbalance may lead to distress or dissatisfaction. The current research examines whether equity of received and provided partner contributions to sexual self-esteem, as perceived by men and women, is associated with sexual satisfaction and sexual function for both partners. We conducted Dyadic Response Surface Analyses using data from 327 mixed-gender couples. Our results indicate that perceiving high, but not necessarily similar (i.e., equitable) levels of partner contributions to sexual self-esteem are associated with greater sexual satisfaction and function of both partners. When analyzing the subscales of partner contributions to sexual self-esteem, i.e. partner contributions to sexual self-worth and sexual self-efficacy, separately, we found a broad equity effect between received and provided sexual self-worth and sexual satisfaction for both partners. This means, that equality in received and provided sexual self-worth is associated with higher sexual satisfaction compared to when inequality is perceived. Additionally, perceived overbenefit in partner contributions to sexual self-efficacy in men was linked to lower sexual function in men. Our findings have implications for research and practice and suggest that gendered sexual scripts should be considered alongside equity theory when conducting research on sexual health in couples.
Introduction
In monogamous romantic relationships, partners typically rely on each other exclusively to fulfill their interpersonal sexual needs (Impett et al., 2020). Research shows that sexual health within couples is interdependent (Chew et al., 2021), making sexual interactions an important element for experiencing high sexual satisfaction and high sexual function within partnered sexual activities (Velten & Margraf, 2017). Additionally, engaging in sexually satisfying interactions benefits both individual well-being (Stephenson et al., 2024) and relationship satisfaction (Fallis et al., 2016), highlighting partner interactions as a key research interest.
One aspect of sexual interactions within romantic relationships is sexual self-esteem, since it is directly linked to sexual behaviors (Kohlberger et al., 2019; Satinsky & Jozkowski, 2015), motivations (Aspis & Gewirtz-Meydan, 2024), emotional reactions (Horne & Zimmer-Gembeck, 2006; Kotiuga et al., 2021), sexual satisfaction, and sexual function (Brassard et al., 2015; Peixoto et al., 2018). Recent research shows that sexual self-esteem is shaped through reciprocal interactions with a romantic partner, highlighting the role of partner contributions to one’s sexual self-esteem and their association with sexual health (Heinrichs et al., 2009; Hewitt-Stubbs et al., 2016; Kohlberger et al., 2019). However, the nature of how partner contributions to sexual self-esteem are associated with sexual health in a romantic couple remains unclear. Previously, equitable interactions with a romantic partner have been associated with better relationship function (Sprecher, 2018), with emerging work extending this concept to the sexual context (Hatfield et al., 1982; Johansen et al., 2023). In the current study, we draw on equity theory (Adams, 1965) as a theoretical framework to understand the unique role of how perceived contributions to one’s own and the partner’s sexual self-esteem relate to sexual satisfaction and sexual function. By doing so, this research aims to contribute to the understanding of how partner contributions to sexual self-esteem are associated with sexual health within romantic couples.
Sexual self-esteem
Sexual self-esteem is defined as one’s positive regard and confidence in the ability to have satisfying and enjoyable sexual experiences (Snell & Papini, 1989), and consists of sexual self-worth and sexual self-efficacy (Cast & Burke, 2002; Kong et al., 2023). Sexual self-esteem it is directly associated with sexual behaviors, motivations, and feelings (Aspis & Gewirtz-Meydan, 2024; Brotto et al., 2016; O’Sullivan et al., 2016), therefore being relevant for partnered sexual interactions. For instance, feeling sexually valued and confident in initiating and engaging in sexual activities is linked to increased likelihood of communicating one’s sexual needs and boundaries (Kohlberger et al., 2019; Satinsky & Jozkowski, 2015). Additionally, higher sexual self-esteem has been associated with higher sexual approach motivations (Aspis & Gewirtz-Meydan, 2024) and experiencing positive emotions during sexual activities (Horne & Zimmer-Gembeck, 2006; Kotiuga et al., 2021). Improving sexual self-esteem through cognitive-behavioral therapy was associated with higher levels of sexual function after the intervention in women with urinary incontinence (Moradinasab et al., 2023). Therefore, sexual self-esteem plays a key role in shaping individuals’ sexual experiences and contributes to greater sexual satisfaction (e.g., Bornefeld-Ettmann et al., 2018; Brassard et al., 2015; Peixoto et al., 2018) and improved sexual function (e.g., Anzani et al., 2021; Peixoto et al., 2018; Rodríguez-Domínguez et al., 2021). At the same time, self-esteem research suggests that high sexual satisfaction and sexual function reinforce higher sexual self-esteem (Peixoto et al., 2018; Weber et al., 2024), indicating a bidirectional process between sexual self-esteem and sexual health.
Given the interdependent nature of sexual health and the importance of sexual self-esteem to partnered sexual activities, sexual self-esteem should be understood in a dyadic framework. Indeed, both self-esteem theories (i.e., sociometer theory; Leary, 2005; Leary & Baumeister, 2000; and self-broadcasting theory; Srivastava & Beer, 2005) and research findings indicate that sexual self-esteem is shaped through reciprocal interactions within the couple, where both partners contribute to each other’s sexual self-esteem (Heinrichs et al., 2009; Hewitt-Stubbs et al., 2016; Kohlberger et al., 2019). Thus, attention should be directed toward how partner interactions shaping sexual self-esteem are associated with sexual satisfaction and sexual function rather than solely focusing on individual sexual self-esteem.
Received and provided partner contributions to sexual self-esteem
The process of how sexual self-esteem is shaped through reciprocal interactions within the couple is conceptualized in the Dyadic Sexual Self-Esteem Model (Wehrli et al., 2025). The model builds upon sociometer theory (Leary, 2005; Leary & Baumeister, 2000) and self-broadcasting theory (Srivastava & Beer, 2005) as well as dyadic interdependence theories (Bodenmann, 1997; Kelley & Thibaut, 1978), suggesting that sexual self-esteem is interdependent between partners and emphasizing the importance of each partner’s contribution to the other’s sexual self-esteem. For example, contributing to a partner’s sexual self-esteem entails making them feel sexually capable and valued—by showing that their sexual desires matter or encouraging open communication about those desires. In turn, receiving a contribution to one’s own sexual self-esteem involves feeling supported and valued by one’s partner in these same areas.
Partner contributions to sexual self-esteem can be further differentiated into two aspects, namely partner contributions to sexual self-worth and partner contributions to sexual self-efficacy. Partner contributions to sexual self-worth are defined as the degree to which partners make each other feel like being of sexual value and deserving of respect during sexual interactions. Partner contributions to sexual self-efficacy refer to the degree to which partners make each other feel sexually capable and efficacious. Existing studies show that a differentiation of sexual self-esteem into aspects of sexual self-worth and sexual self-efficacy might be clinically relevant (Kong et al., 2023, 2024). While both constructs contribute to sexual self-esteem, they are not considered overlapping constructs and operate differently (Cast & Burke, 2002; Kong et al., 2024). Higher sexual self-efficacy has been more strongly related to better sexual functioning (Bond et al., 2020), less sexual anxiety (Horne & Zimmer-Gembeck, 2006) as well as better sexual satisfaction and sexual communication (Kohlberger et al., 2019) compared to sexual self-worth-related aspects. However, studies that distinguish between these two aspects are limited, especially with regard to partner contributions, highlighting the need for further research (Kong et al., 2024).
The Dyadic Sexual Self-Esteem Model suggests that higher levels in received and provided sexual self-esteem are expected to benefit sexual health through adaptive affective, motivational, and behavioral processes within the couple. At the same time, higher sexual satisfaction and sexual function contribute to more favorable partner contributions to sexual self-esteem (Wehrli et al., 2025). Existing studies support this and suggest that being motivated to meet a partner’s sexual needs and expecting a partner to do the same is beneficial for sexual desire (Impett et al., 2020; Muise et al., 2013) and sexual satisfaction (Impett et al., 2019) for both members of a couple. Additionally, partners’ empathic responses and feeling special and valued as a partner were linked to sexual desire (Bergeron et al., 2024; Birnbaum et al., 2016) and sexual well-being (Bosisio et al., 2022). Furthermore, higher perceived partner responsiveness and support have been associated with better sexual satisfaction and greater sexual need fulfillment for both partners (Shoikhedbrod et al., 2023). For individuals facing sexual challenges, having a highly sexually responsive partner – and more importantly one that is perceived as such – can buffer the negative link of those challenges with both relationship and sexual outcomes of both partners (Balzarini et al., 2021; Day et al., 2015).
While most of these studies focus on general motivation, expectations, and responsiveness in partner interactions, the nature of how partner contributions to sexual self-esteem are associated with sexual health remains unclear. Given the relevance of sexual self-esteem for sexual motivations, feelings, and behaviors as well as the interdependent nature of sexual interactions, this should be investigated in more detail. One valuable framework to research this relationship is provided by equity theory.
The role of equity theory for partner contributions to sexual self-esteem
Equity theory suggests that people inherently strive for equitable contributions within social interactions (Adams, 1965). In the context of sexual interactions, this suggests that perceiving an equal balance in one’s own and the partner’s contributions to the sexual relationship can promote sexual satisfaction and function. For example, viewing a partner as equally responsive to one’s own sexual needs and desires, or being motivated to invest in the shared sexual relationship, is therefore considered beneficial for sexual health (Schoeb et al., 2013; Sprecher, 1998). When there is a perceived imbalance between the efforts provided and received by partners, equity theory proposes that individuals experience dissatisfaction and distress (Adams, 1965). Such imbalance can manifest as either an underbenefit, where one partner contributes more than they receive, or an overbenefit, where one receives more than they provide (Adams, 1965). Therefore, when contributions to the sexual relationship are not equal between partners, this may cause diminished sexual satisfaction or low sexual function (Schoeb et al., 2013; Sprecher, 1998). Research found support for negative correlates of both underbenefit and overbenefit in sexual interactions. For instance, individuals who perceived themselves as being in a sexually equitable or overbenefitting relationships had higher sexual satisfaction compared to those who perceived themselves as sexually underbenefitting (Schoeb et al., 2013). On the other hand, perceiving overbenefit might result in experiencing failure to acknowledge and meet the sexual needs of a partner, which could diminish sexual intimacy, increase conflict, and reduce relationship satisfaction (Vowels et al., 2022).
In the context of sexual self-esteem, this suggests that a perceived balance in contributions to sexual self-esteem within romantic relationships is associated with greater sexual satisfaction and function, whereas perceived imbalances can lead to distress or dissatisfaction (Adams, 1965; Sprecher, 1998). Overbenefit occurs when a partner feels that their partner puts in more effort to make them feel sexually capable and valued than they do in return. Underbenefit is the opposite, where one partner feels they are putting in more effort than they receive. While existing research highlights the links between partner interactions, sexual self-esteem and sexual health (Hewitt-Stubbs et al., 2016; Kohlberger et al., 2019), the role of equity in partner contributions to sexual self-esteem has not been investigated so far. Moreover, the distinct associations of sexual self-worth and sexual self-efficacy with sexual health outcomes have received limited attention (Aspis & Gewirtz-Meydan, 2024; Kong et al., 2023). Investigating this in more detail would contribute to the understanding of how interactions between partners are associated with couples’ sexual health.
The aim of this study
The aim of the present study is to explore the association between equity in partner contributions to sexual self-esteem and sexual satisfaction as well as sexual function as key sexual outcomes in monogamous romantic couples. Research shows gendered effects on sexual self-esteem (i.e., Kohlberger et al., 2019) and other sexuality variables (Busby et al., 2023; Velten et al., 2019), necessitating distinguishable dyads to avoid confounding results (Schönbrodt et al., 2018). Specifically, the study addresses three core research questions. In the first research question (RQ1), we investigate whether higher levels in equity of partner contributions to sexual self-esteem are associated with higher levels of sexual satisfaction and sexual function. Based on existing literature on relationship equity and sexual well-being, we hypothesize that higher levels of equity in partner contributions to sexual self-esteem will be positively associated with both sexual satisfaction (H1a) and sexual function (H1b).
In the second research question (RQ2), we examine the associations of inequity in partner contributions to sexual self-esteem with sexual satisfaction and sexual function. We hypothesize that inequity—whether overbenefitting or underbenefitting–will be associated with lower levels of sexual satisfaction (H2a) and sexual function (H2b). We expect a curvilinear association, where greater inequity in either direction corresponds to lower sexual satisfaction and function, while moving towards equity is associated with better outcomes.
Finally, given the limited empirical research on the relationship between sexual self-worth, sexual self-efficacy, and sexual outcomes, we aim to explore the differential relevance of equity in partner contributions to sexual self-worth versus partner contributions to sexual self-efficacy for sexual satisfaction and sexual function (RQ3). We hypothesize that there will be a difference in the association of equity in partner contributions to sexual self-worth compared to equity in partner contributions to sexual self-efficacy with both sexual satisfaction (H3a) and sexual function (H3b), though the direction of these associations is not predetermined due to the exploratory nature of this question.
Method
Participants
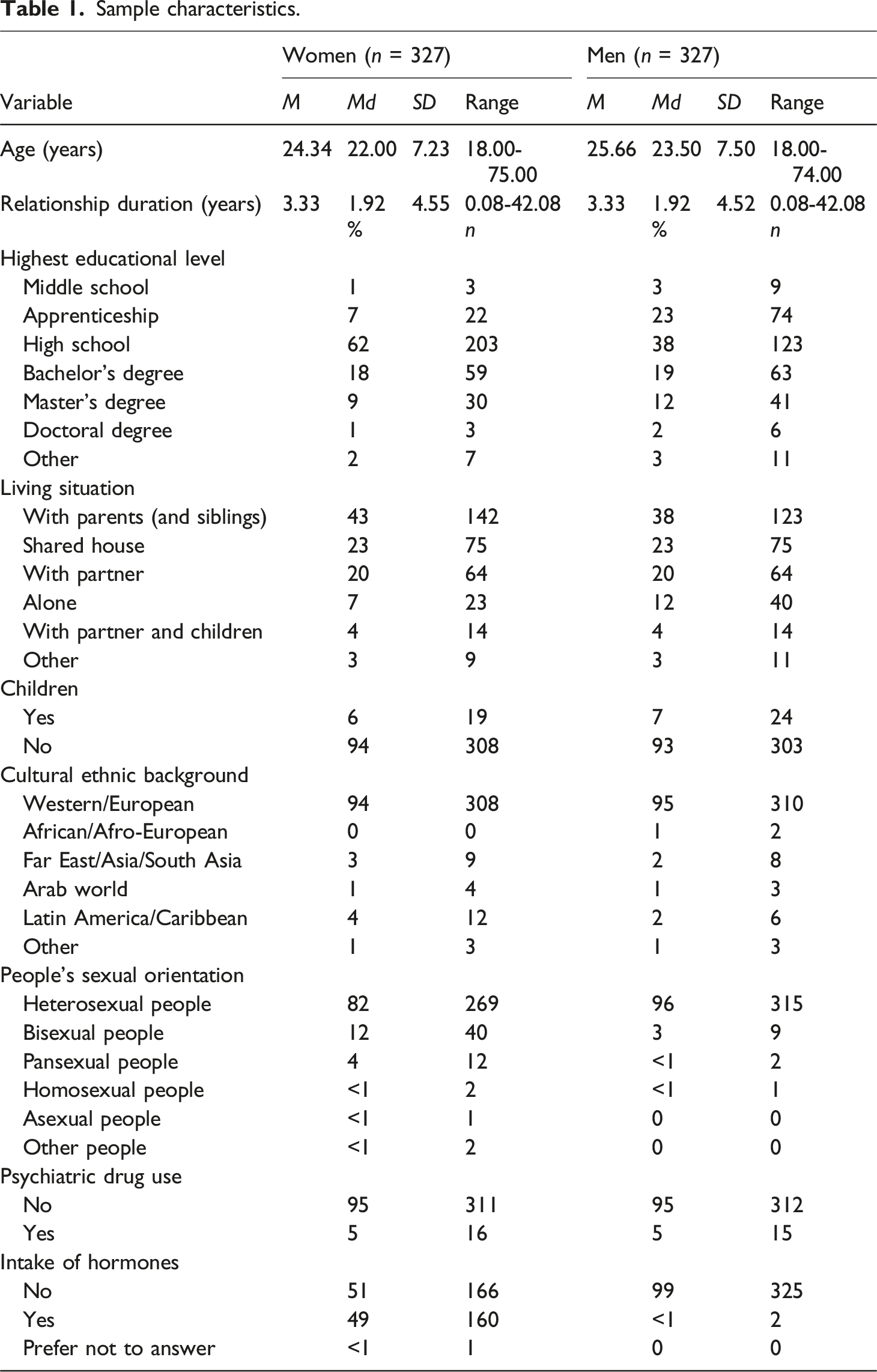
Sample characteristics.
Procedure
The study was preregistered on the Open Science Framework (OSF; https://doi.org/10.17605/OSF.IO/YTMK2) in accordance with open-science guidelines and was approved by the ethical review board of the University of Zurich on the 20th of February 2024 (ref. number: 22.12.17). Data was obtained through an anonymous online survey hosted by Unipark. The link to the survey was distributed via social media platforms (Instagram, Facebook), mailing lists of various organizations and universities, sexual health clinics, and via personal contacts. Paid advertisements on social media platforms were geo-restricted for adults living in German-speaking parts of Europe (e.g., Germany, Switzerland, Austria). Recruitment for the study started on the 25th of March 2024 and ended on the 24th of July 2024. To be eligible for participating in the study, participants were required to be in a committed romantic relationship, at least 18 years old, German speaking, and have a partner who was also interested in participating in the study. The couples were instructed to complete the survey alone and not discuss it with their partner. After individuals gave their written informed consent to participating in the study including to publishing the data on OSF, an individualized partner code was created before participants could continue with the survey. At the end of the survey, a link for their partner’s participation was automatically sent to them. The survey took around 30 minutes to complete and both partners individually received automated personalized feedback on their sexual and relational health at the end of the survey. After both partners completed the survey, the couple received information on how to improve and maintain partnered sexuality as well as the opportunity to gain university credits and to participate in a price draw.
Measures
All measures previously showed high reliability and validity. Higher scores in all questionnaires indicated higher levels in the respective construct.
Sociodemographic information
Participants were asked about their age, gender, sexual orientation, highest completed educational attainment, ethnic background, and living situation. Additionally, participants were asked about their relationship duration, number of children, psychiatric drug use (e.g., antidepressants), and intake of hormones (e.g., hormonal contraceptives).
Received and provided partner contributions to sexual self-esteem
Results of the correlation analyses of perceived provided and received partner contributions to sexual self-esteem with sexual satisfaction and sexual function.
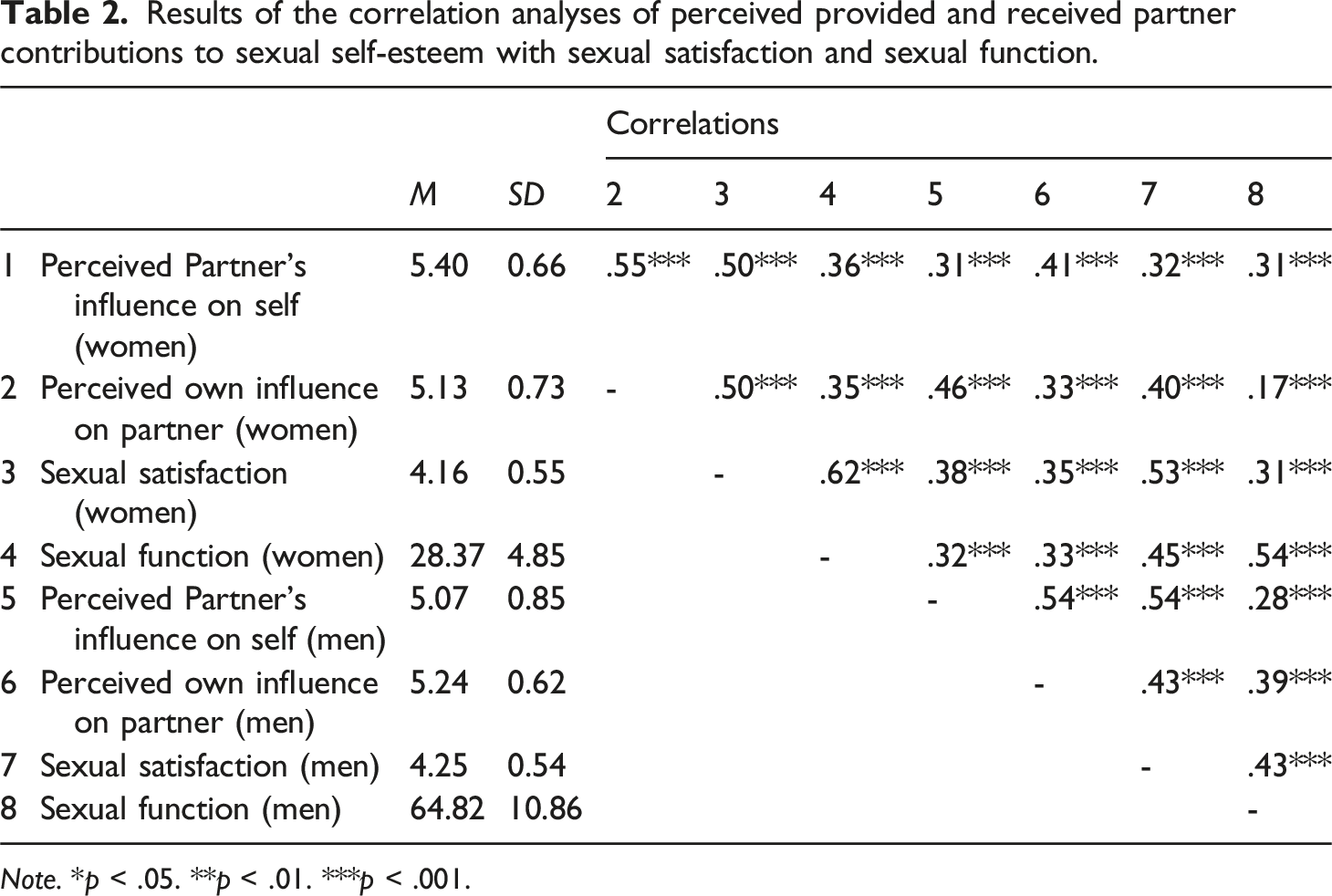
Note. *p < .05. **p < .01. ***p < .001.
Equity of partner contributions to sexual self-esteem
The equity index for the preliminary analysis was obtained by subtracting the values of the DSSEI scale Perceived Own Influence on Partner (DSSEpr) from the values of the DSSEI scale Perceived Partner’s Influence on Self (DSSEre; EQ = DSSEre − DSSEpr) as perceived by men and women separately (following prior research: Bar-Kalifa et al., 2018; Meier et al., 2021). If the respondent reported similar influence of the partner on one’s self-esteem (e.g., 4) as they had on their self-esteem (e.g., 4), the respondent’s equity of partner contributions to sexual self-esteem was zero (EQ = 4 − 4 = 0), the highest possible equity score. If the respondent reported an overbenefit of partner contributions to sexual self-esteem (DSSEre > DSSEpr), the equity score was positive. For example, if the respondent reported their partner as contributing a great amount to their own sexual self-esteem (6) while not contributing to the sexual self-esteem of the partner (1), the respondent’s score would be 5 (EQ = 6 − 1 = 5), which is the highest possible equity score in the direction of an overbenefit. Negative scores, on the other hand, describe an underbenefit of partner contributions to sexual self-esteem (DSSEre < DSSEpr) with −5 being the lowest possible equity score (EQ = 1 − 6 = −5) in the direction of underbenefit.
Sexual satisfaction
The Short form of the New Sexual Satisfaction Index (original English version by Štulhofer et al., 2010; German version by Hoy et al., 2019) includes 12 items, which are scored on a five-point Likert scale (1 = not at all satisfied to 5 = very satisfied; zero = does not apply to me). For up to three missing values or three instances of using the category “does not apply to me” the total score was calculated using mean imputation. Internal consistency of the instrument’s global score was good (α = .83 for women and α = .84 for men).
Sexual function
Sexual function for women was measured with the Female Sexual Function Index (Rosen et al., 2000; German version by Berner et al., 2004), which assesses six different sexual function domains (i.e., sexual desire, arousal, lubrication, orgasm, satisfaction, and pain). The 19 items are scored on a five- or six-point scale depending on the item (0/1 to 5 points). The internal consistency of the instrument’s global score was excellent (α = .91).
Sexual function for men was measured with the International Index of Erectile Function (Rosen et al., 1997; German version by; Wiltink et al., 2003), which evaluates five different sexual function domains (i.e., erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall sexual satisfaction). The 15 items are scored on a six-point or five-point scale (0/1 to 5 points). Internal consistency of the instrument’s global score was excellent (α = .91). Because sexual function was measured differently for men and women, we z-standardized the outcome to make comparisons between men and women.
Statistical analyses
Dyadic response surface analysis
For all our hypotheses, we used the Dyadic Response Surface Analysis (DRSA; Schönbrodt et al., 2018). The DRSA is a combination of an Actor-Partner-Interdependence Model (APIM; Kenny et al., 2006) and Response Surface Analysis (Edwards, 2003; Humberg et al., 2019). It builds on polynomial regression and provides three-dimensional graphs that illustrate the dyadic associations for each partner’s outcome. DRSA further allows us to capture how received (x-axis) and provided (y-axis) partner contributions to sexual self-esteem, as perceived by women and men, are associated with sexual satisfaction or function for each partner (z-axis). Existing studies recommend using individual perceptions of how participants rate themselves and their partner, as these are particularly predictive of sexual outcomes (Busby et al., 2023; Muise et al., 2016). Accordingly, we focus on within-person perceptions of received and provided partner contributions to sexual self-esteem for our analyses. Beyond what difference scores can offer, DRSA can give insight into how equity and inequity relate to the outcome variable and can detect curvilinear effects (Edwards & Parry, 1993; Shanock et al., 2010).
To ensure we had enough variance in the combination of received and provided partner contributions to sexual self-esteem, we examined equity and inequity of each partner’s partner contributions to sexual self-esteem. A cut off point of >.05 standard deviations was applied to consider a person as being discrepant (experiencing an overbenefit or an underbenefit), following the recommendations of Humberg et al. (2019) and Schönbrodt et al. (2018). Among women, 38% (n = 125) reported perceiving equitable partner contributions to sexual self-esteem, while 45% (n = 148) reported perceiving an overbenefit and 17% (n = 54) reported perceiving an underbenefit. Among men, 56% (n = 182) perceived equitable partner contributions to sexual self-esteem, while 28% (n = 91) perceived an overbenefit and 16% (n = 54) perceived an underbenefit. For valid results within DRSA, at least 10% of cases should be classified as discrepant, which is the case here.
The DRSA were computed using structural equation modeling. Robust ML estimator and bootstrap using 10,000 iterations to deal with nonnormality of the data and potential ceiling effects were employed (Pek et al., 2018). We compared the unconstrained models with actor and partner effects to a constrained version, where actor and partner effects were considered equal. Since the unconstrained version either fit the data significantly better or did not show any worse fit, we retained the unconstrained models for all analyses. Age was added to the models as a control variable since previous studies have shown associations of age with sexual self-esteem (e.g. Hewitt-Stubbs et al., 2016), sexual satisfaction (e.g. Miguel et al., 2024), and sexual function (e.g., Hayes & Dennerstein, 2005). Controlling for age did not change the results. For predictor and outcome variables, we dealt with outliers using best-practices recommendations (Aguinis et al., 2013). To ensure that influential cases do not heavily affect the DRSA results, we checked the difference in fit, Cook’s distance, and hat values (Pek & MacCallum, 2011). In case of having identified influential observations, we examined whether excluding them affected the DRSA results to determine the robustness of our findings and reported the results accordingly (Aguinis et al., 2013; Pek & MacCallum, 2011). To better understand the difference in results when influential cases were excluded, we looked at the characteristics of cases marked as influential (in total n = 25). ANOVAs revealed that cases marked as influential reported significantly higher age, longer relationship duration, as well as lower levels of perceived received and provided partner contributions to sexual self-esteem, sexual function, and sexual satisfaction compared to cases not marked as influential.
All analyses were performed using R version 4.4.2 (R Core Team, 2023). A significance level of p < .05 was employed. All code and results are available online from the OSF (https://osf.io/r2gmv/?view_only=05cd055fa9c54a7a920e41acd8f73a6e), and data is available upon request.
Overview of dyadic response surface analysis surface values
Our inferences in relation to the hypotheses are based on the response surface parameters a1 to a5 (see Bar-Kalifa et al., 2018; Kim et al., 2021; Landolt et al., 2024 for dyadic examples). To get an overall understanding of the association between equity of partner contributions to sexual self-esteem and the outcome variables, it is important that all response surface parameters are interpreted in relation to each other rather than in isolation (Humberg et al., 2019; Schönbrodt et al., 2018).
The surface parameter a1 represents linear associations and tests the line of equity (i.e., the line where perceptions of received and provided partner contributions to sexual self-esteem perfectly match at different levels). If only a1 is significant and positive, it indicates that matching at higher levels of perceived received and provided partner contributions to sexual self-esteem is associated with higher sexual satisfaction or function than matches at lower levels. The surface parameter a2 tests the curvature of the line of equity, indicating whether moderate levels of provided and received partner contributions to sexual self-esteem correspond to higher (or lower) sexual satisfaction or function. The a3 parameter assesses how sexual satisfaction and function are associated with overbenefit and underbenefit of partner contributions to sexual self-esteem (line of inequity). A significant and positive a3 indicates that sexual satisfaction or function are higher in case of overbenefit of partner contributions to sexual self-esteem, while a significant and negative a3 indicates that sexual satisfaction or function is higher in case of an underbenefit. The a4 parameter shows whether increasing inequity in either direction–underbenefit to the left and overbenefit to the right–is associated with better or worse sexual satisfaction or function (curvature of the line of inequity) compared to equity. A significant negative a4 indicates a decrease in sexual satisfaction and function when moving from the center of the line of inequity (where it intersects with the line of equity) in both directions of inequity. The a5 response surface parameter is mainly there to validate a possible (in)equity effect, since it tests whether the ridge line (first principal axis) is positioned at the line of equity. If all response surface parameters (a1–a4) indicated an (in-)equity effect, a nonsignificant a5 would be required to confirm this.
Evidence of equity effects within dyadic response surface analysis
To determine whether equity in perceived provided and received partner contributions to sexual self-esteem is better than inequity, we follow the guidelines of Humberg et al. (2019). Using the surface parameters above, requirements of a broad equity effect include a significant, negative a4 value, while a3 and a5 values are not significant. We expect a significant and positive a1 value next to the significant and negative a4 value. This would indicate that equity in partner contributions to sexual self-esteem is better than inequity but allows for the influence of the level of perceived received and provided partner contributions to sexual self-esteem.
Power analysis for dyadic response surface analysis
To date, there is no known method to directly determine the sample size required for adequate power in DRSA. According to the APIM-calculator (Ackermann et al., 2016), a sample size of 159 couples is necessary to achieve 80% power for detecting small actor and partner effects (r = .15) with an alpha of 5%. Current guidelines suggest that DRSA requires a sample size that is two to three times larger (Humberg et al., 2019; Nestler et al., 2015). Therefore, we aimed to recruit at least 318 mixed-gender couples for our DRSA. Additionally, previous studies have utilized similar sample sizes to study sexuality in couples using DRSA (Kim et al., 2021; Landolt et al., 2024; Tavares et al., 2022).
Results
Preliminary analyses
Table 2 presents the means, standard deviations, and correlations of partner contributions to sexual self-esteem, sexual satisfaction, and sexual function. Difference analyses of the equity index of received and provided partner contributions to sexual self-esteem showed that women, on average, report significantly more overbenefit (M = .27, SD = .66, range = −1.83–2.5), while men report more underbenefit (M = -.17, SD = .74, range = −3.33 to 2; t(326) = 7.18, p < .001, Hedges’ g = 0.63). Furthermore, large correlations (women: r = .55, p < .001; men: r = .54, p < .001) were observed between the perceived partner’s influence on one’s sexual self-esteem and the perceived own influence on the partner’s sexual self-esteem. Likewise, sexual satisfaction (r = .53, p < .001) and sexual function (r = .54, p < .001) between partners showed a large correlation.
Are there equity effects in the association between partner contributions to sexual self-esteem and sexual satisfaction and sexual function?
Equity in partner contributions to sexual self-esteem and sexual satisfaction
For sexual satisfaction, there was no support for a broad equity effect in the association between partner contributions to sexual self-esteem and sexual satisfaction (significant positive a1, nonsignificant a4). In men and women with higher levels of received and provided partner contributions to sexual self-esteem, both members of the couple reported higher sexual satisfaction (significant positive a1). Women’s perception of partner contributions to sexual self-esteem explained 34% of the variance in women’s sexual satisfaction and 19% of men’s sexual satisfaction. Men’s perception of partner contributions to sexual self-esteem explained 35% of the variance in men’s sexual satisfaction and 18% of the variance in women’s sexual satisfaction. These associations were stable when excluding influential cases, but the explained variance dropped to 28% for men’s and 14% for women’s sexual satisfaction.
Equity in partner contributions to sexual self-esteem and sexual function
For sexual function, there was no support for a broad equity effect between women’s perceptions of partner contributions to sexual self-esteem and sexual function (significant positive a1, nonsignificant a4). In women with higher levels of received and provided partner contributions to sexual self-esteem, both members of the couple reported higher sexual function (significant positive a1). The model explained 19% of the variance in women’s sexual function and 10% of the variance in men’s sexual function. These associations were stable when excluding influential cases, however, the explained variance dropped to 17% for women and 4% for men.
Men reported lower sexual function when they perceived inequity compared to equity in partner contributions to sexual self-esteem (significant negative a4). Nevertheless, they reported significantly lower sexual function in the case of an overbenefit of partner contributions to sexual self-esteem compared to an underbenefit (significant negative a3), which contradicts a broad equity effect. Higher levels in men’s perceived received and provided partner contributions to sexual self-esteem were associated with higher sexual function in both men and women (significant positive a1). The model explained 21% of the variance in men’s sexual function and 15% of the variance in women’s sexual function. When influential cases were excluded, results did not change, apart from the response surface parameter a4 being not significant, and the explained variance dropped to 11% in men’s and women’s sexual function.
How is equity in partner contributions to sexual self-worth versus sexual self-efficacy associated with sexual satisfaction and sexual function?
Equity in partner contributions to sexual self-worth and sexual satisfaction
For sexual satisfaction, there was a broad equity effect between women’s perception of partner contributions to sexual self-worth and sexual satisfaction (significant positive a1, significant negative a2, significant negative a4; see Figure 1(a)). Women who perceived contributions of their own and their partner’s sexual self-worth as equal reported higher sexual satisfaction compared to women who perceived these contributions as unequal. Furthermore, matching at higher levels of perceived received and provided sexual self-worth was associated with higher sexual satisfaction for both women and their partner, compared to matching at lower levels (see Figures 1(a) and 1(b)). Women’s perception of partner contributions to sexual self-worth explained 32% of the variance in women’s sexual satisfaction and 16% of men’s sexual satisfaction. When influential cases were excluded, only the linear effects (significant positive a1 for men and women) remained significant, and the explained variance dropped to 20% for women and 11% for men. DRSA Model with provided and received partner contributions to sexual self-worth as perceived by women predicting women’s (A) and men’s (B) sexual satisfaction. Note. *p < .05. **p < .01. ***p < .001. CSSW = Contributions to Sexual Self Worth. The z-axis represents sexual satisfaction. The x-axis represents women’s perception of provided contributions to sexual self-worth, whereas the y-axis represents women’s perception of received contributions to sexual self-worth. Dots represent individual measurements of women (A) and men (B) over which the surface is placed. The line on the surface leading from front to back is the line of equity (i.e., where contributions to sexual self-worth are perceived as equal). The line on the surface leading from left to right is the line of inequity (i.e., where contributions are not perceived as equal), leading from cases where women perceive underbenefit to cases where women perceive overbenefit.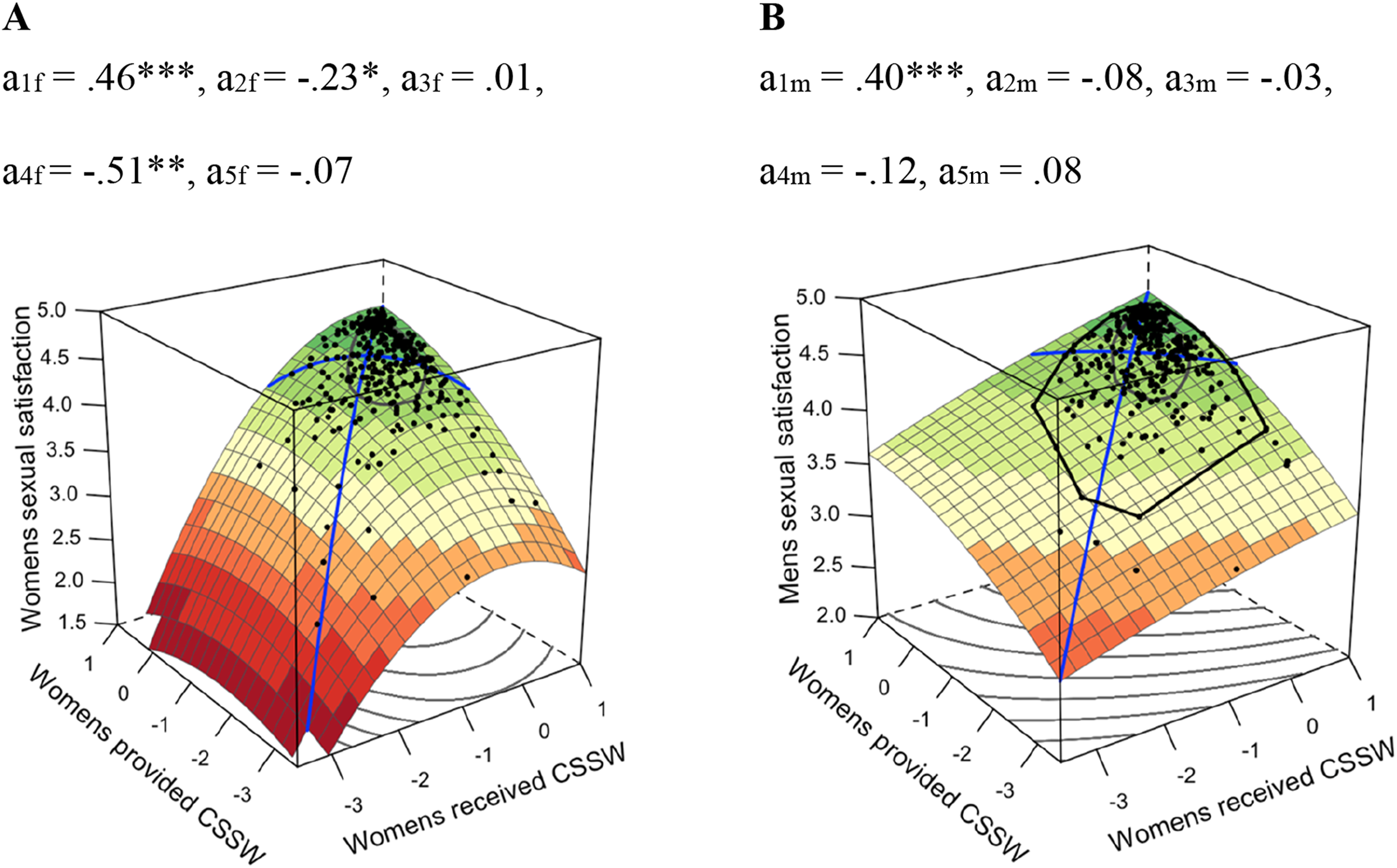
For men’s perception of partner contributions to sexual self-worth, there was no indication for a broad equity effect in the association with men’s and women’s sexual satisfaction (significant positive a1, nonsignificant a4). Higher levels in men’s perceived provided and received partner contributions to sexual self-worth were related to higher levels in their own and their partner’s sexual satisfaction (significant positive a1). The model explained 36% of the variance for men’s sexual satisfaction and 19% of the variance for women’s sexual satisfaction. When influential cases were excluded, results revealed a broad equity effect (significant positive a1, significant negative a4). Men who perceived contributions to their own and their partner’s sexual self-worth as equal reported higher sexual satisfaction compared to those who did not perceive contributions as equal. The model explained 20% of the variance in men’s sexual satisfaction and 13% of the variance in women’s sexual satisfaction.
Equity in partner contributions to sexual self-efficacy and sexual satisfaction
For sexual satisfaction, there was no support for a broad equity effect between women’s perception of partner contributions to sexual self-efficacy and sexual function (significant positive a1, nonsignificant a4). Higher levels of provided and received partner contributions to sexual self-efficacy as perceived by women were related to higher levels of men’s and women’s sexual satisfaction (significant positive a1). The model explained 27% of the variance in women’s sexual satisfaction and 16% of men’s sexual satisfaction. When influential cases were excluded, partner effects revealed a U-shaped association between the women’s predictor variables and men’s sexual satisfaction (significant positive a1 and a2). This means that, compared to high and low levels, moderate levels in provided and received partner contributions to sexual self-efficacy as perceived by women are related to moderate levels of male sexual satisfaction. The model explained 23% of the variance in women’s sexual satisfaction and 12% of the variance in men’s sexual satisfaction.
For men’s perception of partner contributions to sexual self-efficacy, there was no support for a broad equity effect (significant positive a1, nonsignificant a4). Higher levels of provided and received partner contributions to sexual self-efficacy as perceived by men were related to higher levels of men’s and women’s sexual satisfaction (significant positive a1). The model explained 33% of the variance in men’s sexual satisfaction and 15% of the variance in women’s sexual satisfaction. When influential cases were excluded, effects stayed the same and the explained variance dropped to 31% for men and 14% for women.
Equity in partner contributions to sexual self-worth and sexual function
For sexual function, there was no support for a broad equity effect in the association between women’s perception of partner contributions to sexual self-worth with women’s sexual function (significant positive a1, nonsignificant a4, significant negative a5) and men’s sexual function (significant positive a1, significant negative a4, significant negative a5). Higher levels of provided and received partner contributions to sexual self-worth as perceived by women were associated with higher women’s and men’s sexual function (significant positive a1). The model explained 16% of the variance in women’s sexual function and 12% of the variance in men’s sexual function. Excluding influential cases did not reveal a broad equity effect either, and the explained variance dropped to 12% for women and 4% for men.
For men’s perception of partner contributions to sexual self-worth, there was no support for a broad equity effect in the association with sexual function (significant positive a1, nonsignificant a4). Higher levels of provided and received partner contributions to sexual self-worth as perceived by men were associated with higher sexual function in men and women (significant positive a1). The model explained 15% of the variance in men’s sexual function and 12% of the variance in women’s sexual function. Excluding influential cases did not change these results, and the explained variance dropped to 8% for men’s sexual function and 9% for women’s sexual function.
Equity in partner contributions to sexual self-efficacy and sexual function
For sexual function, there was no support for a broad equity effect in the association between women’s perception of partner contributions to sexual self-efficacy and women’s sexual function (significant positive a1, nonsignificant a4) as well as men’s sexual function (significant positive a1, significant positive a3, nonsignificant a4). Higher levels of received and provided partner contributions to sexual self-efficacy as perceived by women are associated with women’s and men’s higher sexual function (significant positive a1). Overbenefitting compared to underbenefitting as perceived by women was linked to better sexual function for men (significant positive a3; see Figure 2(a) and 2(b)). The model explained 15% of the variance in women’s sexual function and 9% of the variance in men’s sexual function. Results did not change when influential cases were excluded, and the explained variance dropped to 13% for women and 6% for men. DRSA Model with provided and received partner contributions to sexual self-efficacy as perceived by women (A, B) and men (C, D) predicting women’s and men’s sexual function. Note. *p < .05. **p < .01. ***p < .001. CSSEff = Contributions to Sexual Self-Efficacy. The z-axis represents sexual function. The x-axis represents provided contributions to sexual self-efficacy as perceived by women (A, B) and men (C, D), whereas the y-axis represents received contributions to sexual self-efficacy as perceived by women (A, B) and men (C, D). Dots represent individual measurements of women (A, D) and men (B, C) over which the surface is placed. The line on the surface leading from front to back is the line of equity (i.e., where contributions to sexual self-efficacy are perceived as equal). The line on the surface leading from left to right is the line of inequity (i.e., where contributions are not perceived as equal), leading from cases where underbenefit is perceived to cases where overbenefit is perceived.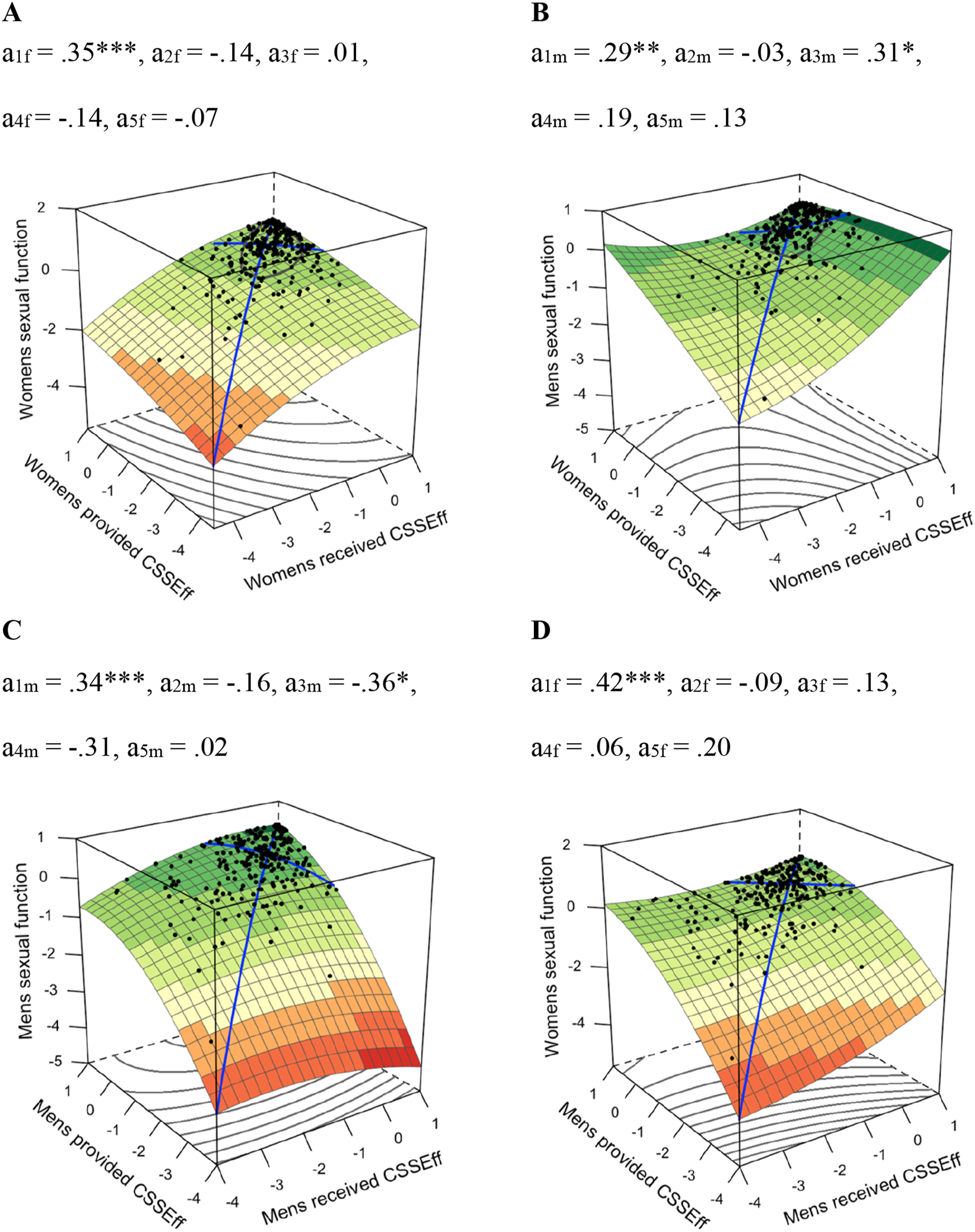
For men’s perception of partner contributions to sexual self-efficacy, there was no support for a broad equity effect in the association with men’s sexual function (significant positive a1, significant negative a3, nonsignificant a4) and women’s sexual function (significant positive a1, nonsignificant a4). Higher levels of received and provided partner contributions to sexual self-efficacy as perceived by men were associated with higher levels of men’s and women’s sexual function (significant positive a1). Overbenefitting compared to underbenefitting as perceived by men was linked to worse sexual function for men (significant negative a3; see Figure 2(c) and (D)). The model explained 14% of the variance in women’s sexual function and 18% of the variance in men’s sexual function. When influential cases were excluded, only the linear association remained significant (significant positive a1), and the explained variance in men’s and women’s sexual function dropped to 10%.
Discussion
This study aimed to examine a broad equity effect between received and provided partner contributions to sexual self-esteem and key sexual outcomes in couples, such as sexual satisfaction and sexual function. We found evidence that perceiving high, but not necessarily similar (i.e., equitable), levels of partner contributions to sexual self-esteem were associated with higher sexual satisfaction and function of both partners. These results show that high levels of partner contributions were consistently linked to higher sexual satisfaction and sexual function. Men reported lower sexual function when they perceived unequal partner contributions to sexual self-esteem, compared to equal contributions. Specifically, men’s overbenefitting was associated with worse male sexual function compared to underbenefitting. Equity effects became more apparent when partner contributions to sexual self-worth and sexual self-efficacy were considered separately.
In general, no broad equity effects were found, which led us to reject H1 and H2. However, the results consistently indicate that greater perceived partner contributions to sexual self-esteem were associated with greater sexual satisfaction. The same pattern was found for sexual function, but less variance was explained. Likewise, greater perceived partner contributions to sexual self-efficacy and sexual self-worth were associated with greater sexual satisfaction and sexual function. While these findings contradict a previous study on equity effects in regard to sexual aspects of romantic relationships in a non-clinical sample (Schoeb et al., 2013), they echo studies finding that high levels in sexual desire, rather than matching levels in sexual desire, were associated with relationship and sexual satisfaction (Kim et al., 2021), as well as with behavioral sexual outcomes (Pawłowska et al., 2024). Additionally, the results are in line with studies reporting that higher levels in motivation to meet one’s partner’s sexual needs (i.e., sexual communal strength) were associated with higher levels in sexual desire, sexual, and relationship satisfaction (Impett et al., 2019, 2020; Muise et al., 2013). This suggests that an overall high level of positive contributions to one’s partner’s sexual self-esteem is associated with sexual satisfaction and function. Higher sexual satisfaction and function might support more positive and reciprocal partner contributions to sexual self-esteem, while they might in turn increase sexual satisfaction and function. This might particularly be the case in in non-clinical samples and when considering a more global evaluation of sexual self-esteem.
Interestingly, when examining the subscales separately, broad equity effects became apparent for partner contributions to sexual self-worth and sexual satisfaction. This was the case for women in the total sample and men in the sample excluding influential cases. Additionally, men’s overbenefit in partner contributions to sexual self-efficacy was related to worse sexual function in men. This supports our H3a and H3b, postulating different associations with sexual satisfaction and sexual function when considering partner contributions to sexual self-worth and efficacy separately. This suggest that equity effects might be masked or compensated for when sexual self-worth and sexual self-efficacy are considered simultaneously (Kong et al., 2024). Additionally, previous research has suggested that self-worth is likely to be more closely linked to affective components such as satisfaction, while self-efficacy is expected to have a stronger connection with motivational components and behavioral reactions such as sexual performance (Chen et al., 2004). This might explain why equity in sexual self-worth was associated with sexual satisfaction, but not sexual function.
As mentioned above, overbenefit in partner contributions to sexual self-esteem in men was linked to lower sexual function in men, while this was not the case for women. This can be attributed to sexual self-efficacy, as the subscale analysis revealed that overbenefit in partner contributions to sexual self-efficacy, but not sexual self-worth, was associated with decreased sexual function. While this was not considered a broad equity effect according to more strict definitions (Humberg et al., 2019; Schönbrodt et al., 2018), other authors interpret this as a sign of inequity and point towards the benefit of interpreting these results (Bar-Kalifa et al., 2018). Research has shown that sexual difficulties affect both partners (Kaya et al., 2015; Pascoal et al., 2018; Velten & Margraf, 2017) and partners often engage in various supportive behaviors to manage challenges together (Bodenmann, 1997). Partners of men experiencing reduced sexual function might, therefore, attempt to put in additional effort to help manage the challenges arising from these difficulties, leading to a perceived overbenefit for men. This way reduced sexual function might lead to a temporary increase in women’s contributions to their partner’s sexual self-esteem.
Additionally, a perceived overbenefit in sexual self-efficacy might cause stress by conflicting with traditional sexual gendered scripts. Indeed, sexual script theory (Wiederman, 2005) posits that men are expected to initiate and dominate sexual activities with a partner, while women play a more passive and responsive role. The ability to maintain an erection, delay ejaculation, and ideally satisfy their female partners is therefore associated with men’s perceived desirability as a sexual partner (Savoury et al., 2022; Wiederman, 2005). Interestingly, research has shown that sexual performance is closely linked to men’s sense of self (Hawley et al., 2024; Savoury et al., 2022). This indicates that reduced sexual performance (experienced through perceived overbenefit in sexual self-efficacy) might inflict stress through experience of shame, personal failure, and disappointment (Gordon, 2018) as well as cognitive distraction during sexual activities (Bockaj et al., 2024). These factors are known to contribute to decreased sexual desire and higher sexual distress, especially when sexual scripts are rigid (Bouchard et al., 2023). At the same time, self-broadcast theory suggests that social interactions are determined by how an individual sees themselves (Srivastava & Beer, 2005). Decreased sexual function might reduce men’s sexual self-efficacy, which in turn would lead to reduced contributions of men towards their partner’s sexual self-efficacy.
Similarly, perceived inequity in partner contributions to sexual self-worth—the sense of feeling sexually valued by a partner—may create a dynamic that conflicts with traditional gendered scripts, potentially compromising sexual satisfaction for both partners (Bouchard et al., 2023; Machette & Montgomery-Vestecka, 2023; Scappini & Fioravanti, 2022). For example, if women feel entitled to experience equity in partner contributions to sexual self-worth, they may be less sexually satisfied if they are not receiving as much partner contributions to sexual self-worth as they expect to. On the other hand, when women receive more partner contributions to sexual self-worth than they provide, this might result in them feeling less desirable as a sexual partner since the female sexual script would expect them to provide pleasure to a partner rather than receiving it. This suggest that sexual script theory should be considered alongside equity theory in research on couples’ sexual interactions.
Nevertheless, the equity effect between partner contributions to sexual self-worth and higher sexual satisfaction were sensitive to influential cases among both men and women, likely due to an undersampling of couples facing sexual health challenges. In fact, the couples flagged as influential showed significantly higher age, lower levels of perceived received and provided partner contributions to sexual self-esteem, decreased sexual function, and lower sexual satisfaction. The equity effect between partner contributions to sexual self-worth and sexual satisfaction was apparent for women only when influential cases were included. Women might be more sensitive to dyadic inequality compared to men (Meier et al., 2020; Pawłowska et al., 2024), particularly when sexual health challenges are present in the couple. Indeed, in this study only 38% of women perceived equity while 56% of men perceived equity, and associations were generally stronger for women. Additionally, a previous study has highlighted that women stressed the importance of reciprocity in sexual interactions for sexual satisfaction (Tomaszewska et al., 2023).
In contrast, the equity effect for men was only evident when influential cases were excluded. In our sample, influential cases were significantly older and might therefore identify more likely as more conservative couples adhering more to traditional gendered sexual scripts where equity might be less important for men (Ricoy-Cano et al., 2020). However, these findings should be replicated before drawing final conclusions.
Limitations and future research
Despite the strengths of this research, there are a number of limitations to this study that suggest promising directions for future research. The first limitation is the correlational nature of the research design. As such, we do not know whether equity in partner contributions to sexual self-esteem shapes sexual satisfaction and function or vice versa. Future research should incorporate longitudinal designs such as daily diary studies or intervention studies targeting partner contributions to sexual self-esteem (e.g., enhancement of providing partner contributions to sexual self-worth and -efficacy while similarly targeting sexual scripts within couples) to uncover the underlying associations with sexual satisfaction and function in more detail.
Second, older couples or those experiencing sexual health challenges were underrepresented in our sample. Additionally, there was a ceiling effect for sexual satisfaction, which may have limited the predictive power of the partner contribution to sexual self-esteem variables. It would be valuable for future research to replicate these findings in a more clinical sample and identify differences between clinical and non-clinical samples. Analyzing a more clinical sample categorizing by individuals with sexual function issues and their partners, rather than categorizing by gender (i.e., Meier et al., 2021), could potentially reveal equity effects more clearly.
Third, both partners were required to participate in the study, which made recruiting more difficult compared to when only individuals are required to participate. Although the study was conducted anonymously, it is possible that participating couples may have had more permissive sexual attitudes, greater openness in sexual communication and consequently higher levels of equality, satisfaction and sexual function than the general population. This may have limited our ability to detect curvilinear effects within the sample, and equity effects might be stronger in the general population than in our sample.
Another limitation is that we did not assess information on employment status, income, socioeconomic status, and pregnancy. Additionally, we did not control for masturbation, which has been shown to contribute to sexual satisfaction and sexual function in partnered interactions (Cervilla & Sierra, 2022). However, research is conflicted about whether masturbation is independent of sexual activities with a partner or used to compensate for unsatisfying sexual partner interactions (Fischer & Træen, 2022; Herbenick et al., 2023; Regnerus et al., 2017). While we instructed participants to answer questions about sexual satisfaction and sexual function regarding their partnered sexual activities, future research should include masturbation as a control variable. Additional control variables could include experience of psychological stress and physical health challenges. Our study specifically focused on sexual self-esteem due to its interpersonal nature and relevance for behavioral, motivational, and affective components of sexuality. Future studies could directly examine these components and explore the role of equity in specific behaviors, such as initiating sexual activity and sexual communication. Moreover, studies could investigate similarities in approach and avoidance motivations as well as emotions such as sexual desire and sexual anxiety. Additionally, examining equity in other aspects of sexual self-concept domains, such as contributions to sexual body-esteem, would be a valuable area for future research.
Finally, we used subjective measures that may be prone to recall bias and social desirability. Although we attempted to mitigate social desirability bias by using an anonymous research design, we cannot rule out the possibility that these biases influenced participants’ perceptions of received and provided partner contributions to sexual self-esteem and sexual function.
Implications for clinical practice and conclusion
The implications of this research for clinical practice emphasize the importance of carefully considering how partners interact within the sexual domain. Clinicians and prevention campaigns should generally encourage couples to cultivate higher levels of both partner contributions to sexual self-worth and sexual self-efficacy, while considering individuals’ sexual scripts to address potential conflicts. For enhancing sexual satisfaction specifically, fostering balanced interactions in partner contributions to sexual self-worth may be important. When addressing sexual function, clinicians should be attentive to male overbenefit in partner contributions to sexual self-efficacy and explore how individual gendered sexual scripts might contribute to conflict or interact with sexual function within these couples. Overall, our study underscores the importance of considering both individual and dyadic effects in understanding sexual health within couples.
Footnotes
Acknowledgements
We would like to thank Prof. Dr. Felix Schönbrodt and Prof. Dr. Eran Bar-Kalifa for their inputs with statistics. Additionally, we would like to thank all couples who participated in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
No funding was received for conducting this study. Open access funding provided by the University of Zurich.
Open science statement
In line with the IARR’s encouragement of open research practices, this research was pre-registered prior to data analysis. We preregistered all hypotheses, statistical analyses, inference statistics, questionnaires used and power analyses on OSF (https://doi.org/10.17605/OSF.IO/YTMK2). Consent to publish the data was obtained by all participants. The data can be viewed at: ![]() and is available to interested people via email (
and is available to interested people via email (