
Abstract
Couples are typically affected by Multiple Sclerosis (MS) as a dyad, with both partners involved in managing the disease. This study explored couples’ shared experiences of coping with MS, with a focus on the dyadic narrative. Eleven couples participated in joint interviews and individual follow-on interviews. Interpretative Phenomenological Analysis (IPA) identified three themes: Interacting individual and dyadic coping experiences, evolving communication and understanding, and regaining control through the dyadic experience. The findings highlighted the interconnected individual and dyadic coping processes, which shaped each couples’ unique experience of MS. When stress was not clearly communicated, couples often misinterpreted the others’ needs and difficulties, which often led to a period of emotional distancing in the relationship. Developing new ways to communicate over time supported couples to move towards a more aligned approach to coping with MS as a dyadic coping system. Limitations are discussed, including the use of a well-educated, self-selected sample of couples, where all relationships exceeded seven years. Clinical and research implications are discussed, including the value of exploring a diverse range of communication strategies, that may continue to evolve over the disease course.
Keywords
Introduction
Multiple Sclerosis (MS) is a chronic degenerative disease (Demirtepe-Saygılı, 2022), affecting 2.9 million people worldwide (Multiple Sclerosis International Federation, 2024). MS is characterised by inflammation, demyelination, and neurodegeneration of the central nervous system (CNS), which affects the motor and sensory functions of patients (Lewis & Spillane, 2019). While there is currently no cure for MS, several effective pharmacological treatments exist, and survival time with the disease has improved (Koch-Henriksen & Magyari, 2021). Symptomology varies depending on the size, number and location of lesions in the CNS (Busch & Fringer, 2022), and the majority of patients can expect to experience cognitive and physical impairments (Hunter et al., 2021) which may become significant over time. MS symptoms impact the daily life, employment, relationships and psychological wellbeing of patients (Gerhard et al., 2020) and often lead to higher rates of dependence on others for their day-to-day functioning (Kołtuniuk et al., 2023). In many cases, informal care is provided by the patient’s spouse or romantic partner (Rajachandrakumar & Finlayson, 2022). It appears that couples are typically affected by MS as a dyad, with both patients and their partners involved in responding to and managing the disease (Helgeson et al., 2018).
Due to the variability in MS symptoms, caregiving responsibilities are multidimensional, often including instrumental support (e.g., transport, shopping), personal assistance (e.g., bathing), and more general social and emotional support (Rajachandrakumar & Finlayson, 2022). Partners may also play a fundamental role in disease management, supporting patient treatment adherence, attending medical appointments, and participating in medical decision-making. The uncertainty, variability and unpredictability unique to MS inevitably changes the lives of both the patient and their partner (Carberry et al., 2024). Previous research reports an increased risk of mental health difficulties for both MS patients and their partners (Busch & Fringer, 2022), as well as increased risk of marital stress and divorce (Landfeldt et al., 2018).
Overall, the context of the spousal or romantic relationship appears to be central in developing a coherent understanding of the dyadic experience of coping with MS. Adopting a dyadic perspective on disease may enrich our understanding of couples’ experiences of coping with illness (Golan & Vilchinsky, 2023), particularly in the case of MS, where patients often require increasing support from their partner, as the disease progresses over time. This research aimed to provide an in-depth exploration of the dyadic experience of couples coping with MS, to better understand the couples’ underlying dynamics when coping with the challenges that often accompany this disease. The use of dyadic interviews is one method that may assist us to understand how the couple, as a unit, generate a shared narrative around their MS experience.
Background
While it has been argued that the couple relationship is the most significant relationship in terms of its impact on wellbeing (Fincham et al., 2018), within the coping literature the spouse is often viewed as merely assisting the coping efforts of the patient (Berg & Upchurch, 2007). This perspective fails to consider the important role that both partners play in managing and coping with MS. An emerging body of health research has begun to recognise the interpersonal context of coping with chronic illness (for a scoping review of this literature, see Weitkamp & Bodenmann, 2022). The concept dyadic coping refers to the multidimensional complex and interactive processes involving how couples communicate about stress, support each other, and deal with stressors together (Falconier et al., 2015).
Several theories of dyadic coping have been applied within the health literature. The Systemic Transactional Model (STM) focused on examining couples’ joint processes of coping with stress, emphasising the importance of the stress communication process. According to the STM (Bodenmann, 1997; Bodenmann et al., 2016), each partner may express their stress in an implicit or explicit manner, and the other partner perceives, interprets, and responds, often using emotion-focused or problem-focused coping strategies. The communal appraisal of stress has been recognised as an integral part of the interpersonal coping process (i.e., the appraisal of the illness as “our problem” as opposed to “mine” or “yours”) (Lyons et al., 1998). Shared illness appraisals have been associated with greater collaborative, instrumental and emotional support between partners coping with diabetes (Helgeson et al., 2019) and other concealable chronic illnesses (Shrout et al., 2024). The Developmental-Contextual Model of couples coping with chronic illness (DCM) conceptualises dyadic coping from a life-span developmental perspective, highlighting the temporal nature of coping across different illness stages and across the life span, indicating that couples cope in different ways depending on their age and life stage (Acquati & Kayser, 2019). A more recent addition to the literature, the Dyadic-Regulation Connectivity Model (DR-CM) is novel in recognising the dynamicity, flexibility and complexity of the self- and dyadic-regulation mechanisms involved in couples coping with illness (Karademas, 2022). The DR-CM provides an overview of how cognitive-emotional representations, coping behaviours and outcomes continuously interact with each other at the individual and dyadic levels, with the aim of achieving ‘coherent’ dyadic regulation. For a more in-depth review of the major aspects of the dyadic adaptation/dyadic coping models see Karademas (2022).
Research exploring couples coping with chronic illness suggests that couples utilise several dyadic strategies to manage the illness and co-regulate their emotions, including normalizing, fighting, denial, avoidance, wishful thinking, seeking social support, positive re-appraisal, cognitive reframing, and planning (Wawrziczny et al., 2017; Weitkamp et al., 2021). While some studies have suggested that certain styles of coping (i.e., seeking support) may be more effective in reducing individual stress and increasing cohesion in couples relationships, thereby improving relationship functioning (Shrout et al., 2024), as suggested by Golan and Vilchinsky (2023), the relationship between dyadic coping and outcomes may be more complex than previously considered. Dyadic coping research has largely focused on cancer, cardiovascular disease, and diabetes (Chen et al., 2021; Lee et al., 2020; Valente et al., 2021). However, it should be considered that illnesses differ widely in terms of their timeline, trajectory, controllability, and consequences (Berg & Upchurch, 2007; Bertschi et al., 2021; Weitkamp et al., 2021). MS appears to be unique to other illnesses given the associated uncertain prognosis, unpredictable disease course, and wide variability in symptom presentation. In addition, the onset of MS in early adulthood often coincides with important developmental stages for couples, such as trying to establish careers or reproductive decision-making. Thus, it appears that the dyadic experience of MS diverges from more-commonly studied populations of older dyads with other chronic neurological conditions which typically emerge later in life, such as dementia (Wawrziczny et al., 2017). The descriptions and characterisations of a specific condition such as MS, may allow for greater understanding of context-specific dyadic coping.
While it is undeniable that MS impacts the quality of life of both patients and their partners, and both partners typically assume a role in managing the disease, existing research exploring couples’ experiences of coping with MS are mainly based on input from only the partner (Appleton et al., 2018), only the person with MS, or both partners interviewed separately (Boland et al., 2018; Demirtepe-Saygılı, 2022). The use of joint or dyadic interviews may support a more in-depth understanding of how the couple, as a unit, provide meaning to their experience in an interactive, or process-orientated, manner (Wawrziczny et al., 2021) and has provided valuable insight into couples’ experiences in other health conditions and procedures (Golan et al., 2023).
To summarize, MS presents perhaps a different level of physical and mental challenges and uncertainty than other often-studied illnesses, and most research around the dyadic experience of MS only explores one partner’s point of view. The descriptions of a specific condition such as MS may serve to deepen our understanding of how the couple, as a unit, generates a shared narrative around their joint experience, and may offer additional insights into the couples’ underlying dynamics when coping with MS. The present study addresses these unique challenges by exploring couples’ shared experience of coping with MS from the perspective of the dyad.
Study aims
The following research questions guided the research, in our aim to understand how couples jointly negotiate the aforementioned challenges that often accompany MS, in the context of their relationship: • What are couples’ shared experiences of facing adversity with MS? • How do couples cope with MS, in the context of the dyad? • What are the positive influences on couples’ shared experiences of coping with MS?
Method
This study utilised a cross-sectional, qualitative research design by means of semi-structured dyadic (couple) interviews, employing Interpretative Phenomenological Analysis (IPA) as a methodological framework, as outlined by Smith et al. (2022). Guided by phenomenology, IPA is concerned with understanding and interpreting how humans experience and make sense of the world. IPA also has an idiographic sensibility, focused on the nuanced analysis of the particular through in-depth analysis on a case-by-case approach. The idiographic approach to the data allowed for a detailed analysis of each couple’s transcript as a single case in its own right, to gain a deeper understanding of the unique experience of each dyad. Finally, using IPA, the researcher is trying to make sense of the participant trying to make sense of their world, through a dual interpretative process, referred to as a double hermeneutic cycle. The use of IPA for multiple-perspective design research, as per couple interviews in this study, allowed for the triple hermeneutic, whereby the researcher attempts to understand how each partner makes sense of the interpretation of their partner, in order to understand the couple experience (Mavhandu-Mudzusi, 2018). Ethical approval for the study was granted from the Research Ethics Committee at the University of Limerick.
Participants
Participant characteristics.
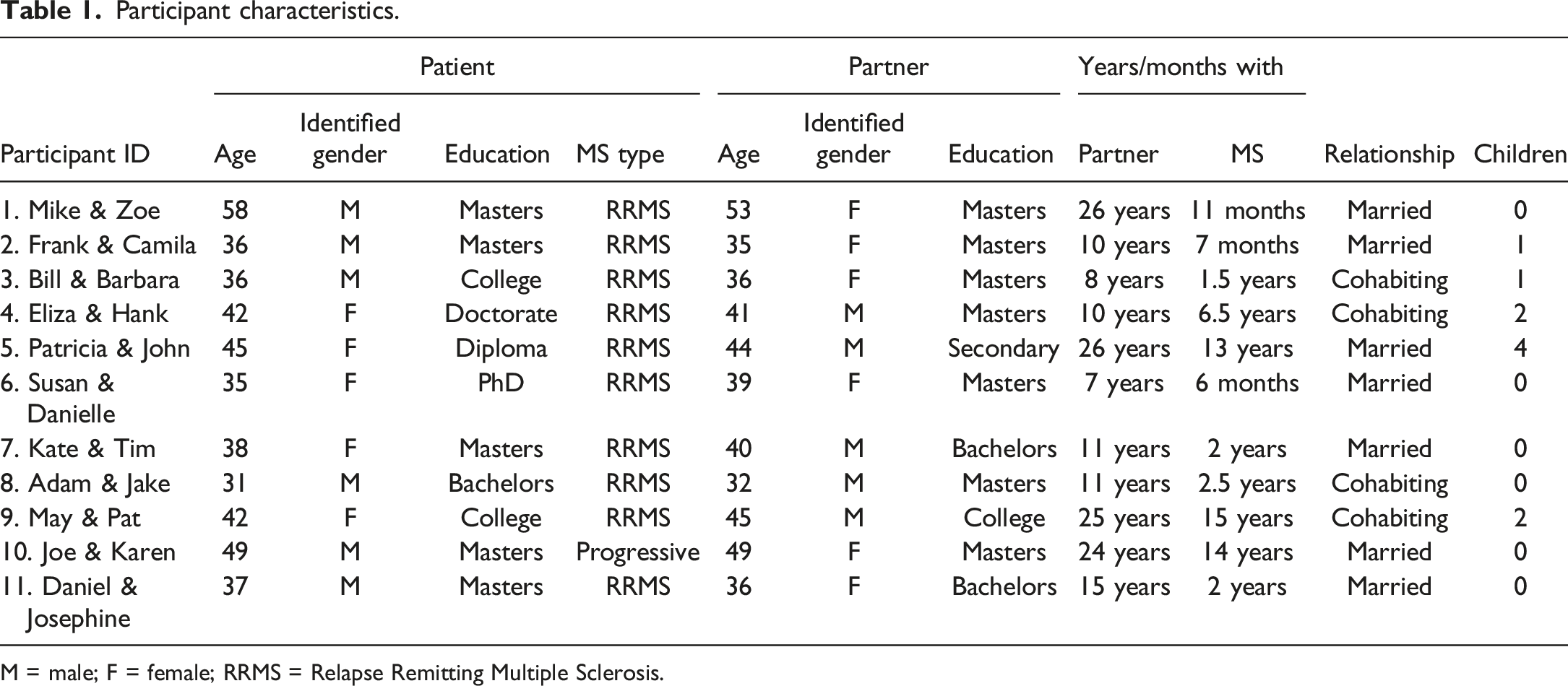
M = male; F = female; RRMS = Relapse Remitting Multiple Sclerosis.
Interviews
Participants were made aware of the study using a lay summary and information sheet, advertised through multiple online channels of Irish and UK-based voluntary organisations, including MS Ireland, MS Trust UK and MS-UK. Participants provided written and verbal consent prior to interview, and were offered a 15 euro/pound shopping voucher on completion. All interviews took place using an online video platform, Microsoft Teams, and were audio-recorded for transcription.
The semi-structured interview schedule was developed through knowledge of the literature, and two experts by experience from MS Ireland (see supplemental material). This study adopted the dyadic interviewing approach to capture the perspective of both members of the couple, and generate a shared narrative. Joint couple interviews were used to discuss a range of topics, broadly related to the couple’s relationship and their shared experience of MS, their coping resources/strategies, and their view of the future. Joint interviews lasted between 58 – 103 minutes (M = 78). All participants took part in follow-on, individual interviews to overcome potential limitations in joint interviewing, allowing participants the opportunity to offer further discussion should they feel that they were encumbered by the dyadic process.
Data analysis
The “couple experience” was the focus of analysis, whereby individual perceptions and understanding were considered in the context of the dyad, with additional insights gained from matters of congruence and contrast between partners’ accounts (Larkin et al., 2019). Following Smith et al. (2022), analysis began with the researcher immersing themselves into the transcript through a process of active engagement, reading and re-reading the transcript, recording personal observations and initial impressions. Next, detailed exploratory notes were completed on each transcript, involving in-depth, line-by-line analysis with a clear phenomenological focus, at descriptive, conceptual and linguistic levels. Through the analysis of the exploratory notes, experiential statements were developed to capture and reflect the essential aspects of the couples’ experiences through “a synergistic process of description and interpretation.” The researcher then engaged in a process of searching for conceptual connections across all experiential statements, leading to the development of higher-order, Personal Experiential Themes (PETs) related to that interview. This process was repeated for each interview. Finally, a dynamic, cross-case analysis was conducted, searching for points of convergence and divergence across interviews, to highlight the shared and unique features salient across all interviews and develop a set of Group Experiential Themes (GETs). The GETs provided the structure and organisation for reporting of analysis. For the purpose of protecting participant confidentiality in individual interviews, pseudonyms were removed from quotes extracted from the individual interviews in the reporting of results in this study.
Reflexivity
As per the IPA approach, a number of strategies were used to ensure reflexivity in this study and maintain the trustworthiness of findings (Engward & Goldspink, 2020). The first author (SC), who adopted the primary role of data analysis, was an Irish, female, Psychologist in Clinical Training within the Irish Public Health Service. Recognising the researcher’s perspective and position in shaping the findings inherent within the analytic process of IPA, SC made a conscious effort to acknowledge the impact of her preconceived biases, positionality and sociocultural context, on subjectivity. SC maintained a reflective diary throughout the collection and analysis of the data, recording personal feelings around the participants and research process. Regular supervision with DGF was used to discuss interviews and theme development, and included credibility checks of the process and data. These were undertaken by reviewing a number of the transcripts to ensure that the initial and final themes reflected the data.
Findings
Three overarching group experiential themes (GETs) conveyed the essence of couples’ shared experiences of dyadic coping with MS: a) “Interacting Individual and Dyadic Coping Experiences,” b) “Evolving Communication and Understanding,” and c) “Regaining Control through the Dyadic Experience”. At times, each partner faced their own unique challenges related to MS and had different ways of coping. These differences often resulted in partners intentionally isolating in their coping and emotionally distancing themselves from the relationship. Over time, couples described developing new ways to communicate which appeared to underpin a more unified approach to managing MS as an aligned, dyadic coping system. Moving towards an alignment in their perspectives on the disease, appeared to support couples to regain a sense of control with MS. Despite the continuous threat of possible disease progression and uncertainty they faced, couples also reported individual and dyadic growth through their joint experiences.
GET 1: Interacting Individual and Dyadic Coping Experiences
GET 1 conveys the different challenges and individual coping strategies used by each partner (Subtheme 1: Differences in coping creating disconnection or balance) and how the intentional disguising of their true emotions (Subtheme 2: Attempting to conceal the individual MS experience) often led to a disconnect between partners when coping with MS. These subthemes are described in detail in the following sections.
Subtheme 1. Differences in coping creating disconnection or balance
It appeared that each partner contended with unique challenges in being the partner experiencing MS versus being in a relationship with someone who has MS. For example, Eliza (couple 4) highlighted the different challenges faced by each partner in administering daily injections as part of her MS treatment: “…the medication is difficult. Umm, because it's painful and it's impactful for me each time. And it puts Hank into that position where he's the one giving me the injections.” As indicated by Eliza, while the person with MS contended with difficulty adjusting to a wide variety of MS treatments and unpredictable symptoms, particularly pain and fatigue, their partner often assumed greater responsibility in the household, and assumed a more active role in supporting the person with MS, including administering medication and providing daily care.
In many cases, differences in each partner’s coping appeared to stand between the person and their partner emotionally processing the news of the MS together, which was perceived as “challenging” for the person with MS. Several couples referenced unique cultural backgrounds, early life experiences (e.g., experiences of parental illness, schooling, and caregiving role in early life) and innate personality characteristics which shaped their individual response to coping with MS that often differed from their partners. For one couple, their differing perspectives on how to approach coping with MS were attributed to the “cultural differences” between partners. This was highlighted by the person with MS, in their individual interview: “… in [their culture] they’re more, they’re present. So, I think that that mentality at first probably came from that. That difference of approach came from that…” From the perspective of this person with MS, the contrast in this couples’ cultural backgrounds shaped their differing mentalities on dealing with MS in the present, versus planning ahead for potential challenges in the future.
Yet, for other couples, having a “contrast of approaches” (Frank, couple 2) provided a sense of balance and emotional equilibrium in the dyad. For example, for couple 7, being presented with her partner Tim’s alternative perspective on MS was considered a helpful cognitive strategy for Kate to cope with intense emotions related to their uncertain future with the disease. Kate: “He does put things into perspective… It’s easy to overthink and read too much. So you do need reminding… it definitely does help.” Tim: “…I try to put it in perspective what she's thinking… Rather than overwhelming herself with what could happen or what will happen, which we don't know. So it is always trying to bring her back to the present.”
While Kate struggled to cope with the uncertainty related to MS, Tim attempted to re-assure Kate about the wide variability in how MS presents and progresses between patients. Despite the apparent differences in their approaches to coping with their uncertain future, it appeared that communicating an alternative perspective allowed Tim to shape and influence Kate’s approach to coping with MS over time. Yet, for other couples, their partner’s rationalisation, or positive attitude around the uncertainty that comes with MS, was perceived to be “dismissive” (anonymous quote extracted from individual interview) or even invalidating.
Subtheme 2. Attempting to conceal the individual MS experience
Many couples spoke of feeling isolated in their coping, particularly in the immediate aftermath of the MS diagnosis. Some participants spoke of intentionally concealing their emotions around MS, and choosing not to seek support, as a means to protect themselves or their partner from emotional distress related to the disease. At times, having an initial period of personal reflection and individual coping was considered to be a necessary, and even beneficial, phase for both partners to come to terms with and adjust to the diagnosis and the possible implications of MS on their shared future, as reflected by couple 2: Camila: “At this point, it was all about him like he had… He was lifting himself up.” Frank: “…I think the only person who could have helped me in that initial phase would have been the me of a year later.”
Remaining isolated in his coping for a period of time was perceived by the couple to be the “right approach” for Frank, to “get prepared for a fight against MS.” Yet, other couples struggled to understand the other’s response to MS, particularly where the inner experience or needs of each partner were not clearly communicated, exemplified by couple 9: May: “…I think it was harder at like at the very, very beginning… I think I wrote you a letter. And I just said, I know this isn't what you signed up for, and if you want to leave I understand and this is your opportunity…” Pat: “I closed up. I know I went and barely said a word to anyone for weeks, and I think that's what May was reading as, he wants out… but actually it was on the way around. It was me constantly thinking, what can I do? How can I fix this?. I don’t have the answers and that's why I have nothing to say you know.”
For couple 9, Pat’s initial muted response to the diagnosis was misinterpreted by May as a form of emotional abandonment. It appeared that intentionally disguising their true emotions led to a disconnection between the support desired by May, and the support provided by Pat. From the perspective of many people with MS, their partners’ attempts to fix or provide solutions to the problem of MS were often perceived to be misguided, particularly when the person with MS simply sought their partner’s emotional presence: Anonymous quote extracted from individual interview: “… [my partner] does try to be solution-focused and sometimes it's kind of… you can’t always be solution focused, we, we can't change what this is... Stop trying to find solutions to this problem right now and just sit down and just be here… you know you can’t make this go away.”
While the person with MS recognised their partner’s attempts to provide practical support were well-intentioned, they also expressed frustration when their partner was unable to be emotionally present with their distress around MS.
GET 2: Evolving communication and understanding
GET 2 highlights the couples’ process in developing more open communication around MS over time, which ultimately appeared to underpin a more intertwined, or unified approach to coping. Verbal, non-verbal and para-verbal communication were used by couples to develop a more acute awareness of, and sensitivity towards, their partners’ difficulties, and thus, more attuned support provision. Susan and Danielle (couple 6) discussed using more formal check-ins to ascertain a deeper understanding of their partner’s emotional wellbeing, and reflect on their needs and expectations: Susan: “We also do check-ins. We do talk frequently about our needs…. We both wrote a list of ways that we want the other to love us. And that was because it was something we were missing. So we kind of check what is or isn't happening at the moment, why is it or is it not happening…” Danielle: “What's feeling good, what's not feeling good.” Susan: “Yeah, what unmet needs are there. What expectations are reasonable and unreasonable.”
For this couple, making the implicit experience explicit may have lessened or even prevented feelings of contempt or disappointment in the dyad, by having “clarity of what’s available from each other” (Susan), particularly when the person with MS was experiencing symptoms like pain and fatigue.
Most couples acknowledged that communication in their relationship had become increasingly open and transparent since the MS diagnosis, describing how their process of communication evolved over time and over the disease course. Couples acknowledged that having the “tough conversations” around the “scary” parts of MS, including the uncertain prognosis, potential for physical mobility issues or premature death, and the related implications, was difficult, and even uncomfortable at first. Danielle recalled how she previously “hated check-ins,” while her partner Susan joked “…in the beginning, I’d nearly have to pin her into a car to agree to do it with me.” For this couple, it appeared that one partner provided encouragement for the other to communicate more openly around MS over time.
Following his initial MS diagnosis, Joe (couple 10) found it difficult to directly communicate his symptoms and emotional response to his partner Karen. Yet, Joe felt more able to share his feelings publicly using an online blog. Paradoxically, Joe’s blog provided a means for the couple to develop more open communication, and an opportunity for Karen to become aware of his emotional process around MS: Interviewer: “Would you have any advice or words for another couple?” Joe: “…My instinct is to tell them to communicate with each other…” Karen: “In the early days when you were blogging, you would communicate, you were finding a way to communicate. It might not have been directly to me. But you knew I was reading your blog. You know it’s, if that’s the, if that's the workaround that we had. OK, that’s, that’s the workaround… I really value the blog because, I know that it helped you process, but it also helped me know what was going through your head in a way that you weren't, at the time, able to just talk about it.”
Many couples described their communication as an evolving process that continued to change and unfold alongside MS progression. For Joe, the progression of his MS symptoms and increasing mobility issues provided a trigger for him to make a more conscious effort to communicate his symptoms more directly to his partner Karen: “…I think that it is helpful, as I have become more affected, it is helpful to continue to communicate that…” Similarly, Barbara (couple 3) described the communication around MS as an “ongoing, work in progress.” Many of these couples continued to work towards establishing the level and mode of communication that worked best for them.
GET 3: Regaining control through the dyadic experience
Within GET 3, three subthemes were identified: a) joint loss of control to MS; b) moving toward an alignment of perspectives to create the secure base; and c) dyadic growth through a shared experience of adversity. While communication was present throughout participants’ narratives, GET 3 specifically highlights the couples’ process of working to align their perspectives and collaboratively manage the uncertainty that is unique to the disease of MS. This theme depicts the process by which the dyad moved to regain a collective sense of control through shifting their joint narrative towards the positives in their dyadic experience. The subthemes demonstrate the process of development of dyadic coping that couples often moved through - while couples struggled to cope with the loss of control of their lives and their futures to MS (subtheme 1), they gradually moved towards an alignment of their perspectives that allowed couples to regain control of their lives, and make more collaborative efforts to manage the disease as a more open, dyadic system (subtheme 2). Despite the continuous uncertainty they faced with MS, all couples described experiencing some level of growth through the coping process (subtheme 3). These subthemes are described in detail in the following sections.
Subtheme 1. Joint loss of control to MS
The joint loss of “control” and “safety” to MS underpinned participants narratives, as they encountered persistent difficulties in managing uncertainty around MS symptom exacerbation, while attempting to reconcile an unknown prognosis and potential further unpredictable symptom exacerbation. For Mike and Zoe (couple 1), coping with the uncertainty around their shared futures was perceived as the “most difficult aspect” of the disease, that made MS “not like any other disease…” This couple spoke of their fear around the potential symptoms Mike may experience in the future, including vision, speech, bladder, cognitive and mobility issues common in MS, and the possible caregiving implications of disease progression on his partner Zoe. Susan and Danielle (couple 6) referenced how “everything and nothing” had changed with MS. This contradictory statement appeared to attenuate the emotional loss the couple was experiencing, that was often unobservable from the outside. Danielle: “…Umm. Whereas now, I suppose, not that I can’t rely on her but…” Susan: “…But it's very different though. Yeah. And you can't, let's be honest. Like, like some days I can't get out of bed. So you can't rely on me if I can't even get out of bed.”
This extract encapsulates a shift in Susan’s availability in the relationship, as a result of MS-related fatigue. The essence of loss was also present in this couple’s discourse of the imagined future they previously shared, and uncertainty in letting go of this possible future: Susan: “…that fantasy for you of having, like, a together partner with something you hadn't had before, at home, even someone that was together. So I think that togetherness has kind of fallen away a good bit now.” Danielle: “… in my fantastical mind I had this idea of who I was going to spend like… We were gonna go travelling a lot more and doing lots of things… And that might have to change now…”
Adjusting to loss in MS appeared to be an ongoing and evolving process as the disease progressed, as couples anticipated further potential loss in the future. This was exemplified by Mike and Zoe (couple 1), who spoke of feeling a loss of control over their ability to plan their shared lives in the future: Mike: “… The neurologist said to me, look the next couple of years is gonna show just how active this disease process is with you. So there’s a lot of uncertainty… I share with Zoe what my concerns are. Am I gonna get another one of these attacks? You know, next week or next year or?” Zoe: “And that’s the difficult part.” Mike: “… our future plans are that we want to travel and spend six months in Africa…. We don't know if we can do what we want to do now… We wanna talk to the neurologist and say well look, you know what if we go to Africa for six months and then I get a relapse? What, what happens then you know? It.. is it as simple as get a flight home?”
Like many other dyads, this couple’s narrative sheds light on the medical, emotional, and financial uncertainty MS brings to both partners, and their struggle in letting go of, or adjusting their shared vision for their lives together.
Subtheme 2. Moving towards an alignment of perspectives to create the secure base
The majority of participants drew strength from their couple relationship to cope with continuous loss and change that was often encountered with MS. A strong sense of togetherness in facing these challenges was evidenced by participants reiterating each other’s responses, often using joint storytelling to support and affirm each other’s views. Having a strong partnership was considered by many of these couples to provide some sense of “control” and “safety” when navigating uncertain territory and coping with losses related to MS. Overall, it appeared that openly discussing MS, and working to align their perspectives, supported a more unified approach to dyadic coping, as reported by couple 2: Camila: “The thing is, we kind of agree in the way of seeing it… it's better to be proactive in approach and I think we both agree on that sense. So for example, when we talked about medication it was like, OK, let's see what's the best medication for you.” Frank: “…I think what's useful for me is now that Camila is fully on board. It's really useful in terms of… If I see something about MS, you know might be a new medication, might be a new trial, might be something from a neurologist, she's more interested to look at it and process it and give me her opinion and all that which is really, really helpful.”
For this couple, the shared perspective of MS as a joint challenge appeared to be central to dyadic coping, particularly when making important decisions on MS treatments and care. Having processed the initial “shock” of diagnosis, several couples moved to regain control of the disease through collaborative and proactive coping efforts. Couples focused on proactively taking steps to cope with MS by maintaining a healthy diet and exercise regime together, use of medication or supplements, attending therapies, researching clinical trials, and seeking evidence-based information from reputable sources. Engaging in collaborative coping appeared to benefit both the person with MS and their partner, exemplified by Karen (couple 10) “… cause when his, when his spasms keep him up at night… There’s nothing I can do, yeah. But like learning [new sport] together, that's something that I can do.” For Karen, accompanying Joe in his physical pursuits was both a demonstration of her support, while providing her with a sense of control in an often uncontrollable situation. While couples used several strategies to navigate an uncertain future with MS, many discussed the futility of anxiety around the future, and reminded each other to maintain a shared focus on the present. Despite the approach taken, the overwhelming majority of couples reported confidence in their dyadic ability to cope with the challenges that may lie ahead, within the context of their partnership, described by couple 11 as the “concrete base” when coping with MS-related challenges.
Subtheme 3. Dyadic growth through shared experience of adversity
While couples experienced shared adversity around the losses and uncertainty related to MS, they also described growth through the dyadic coping process. In many cases, couples aligned in their focus on the positives in the situation, describing a greater sense of natural appreciation through engaging in downward comparison with others, who they perceived as worse off. When asked about the various impacts of MS, many couples appeared to consciously shift the narrative of their joint interview towards the positives in their experience. Participants described themselves as more appreciative, attentive, empathic, patient, optimistic, humbled and resilient as a result of their experience of coping with MS, highlighted by couple 2 in the following extract: Frank: “…So I think overall it [MS] has been positive because it makes me a better person, makes me a happier person and a happier person is a better contributor to a relationship.” Camila: “…well he is also much more attentive in a sense, because he now understands that... Like if I say I have back pain it’s awful… he is helping a little bit more than what he would usually do…”
The personal changes, or increased level of empathy, experienced by Frank appeared to have contributed to dyadic growth, and in turn, benefitted their couple relationship. In many other cases, the ongoing threat of future decline with MS was considered as a catalyst for couples to reassess their priorities in life, which often led to making adjustments to their shared lives, which was exemplified by couple 10 in the following extract: Karen: “…the gift that MS gave us is that it helped us… So, as you get older, you realize that life is precious and life is short. But we were confronted with that stark reality at a much earlier age than you might normally be, and rather than being despairing at it, we were like, well, we’re gonna squeeze every little bit out of what we can.” Joe: “… And I think, yeah, it’s, it’s, you know, don’t, don’t waste your energy worrying about it [MS].”
Joe and Karen (couple 10) described feeling gratitude for the uncertainty that MS brought, for reframing their perspective on the preciousness and fragility of life. Other couples made more conscious efforts to slow down and learn to be more present as a result of learning to live with MS symptoms, including pain and fatigue. Couples placed greater value in “just being,” by themselves, or together following the MS diagnosis, exemplified by Susan and Danielle (couple 6): Susan: “We definitely rest better now as well as a couple… Like, there's just more appreciation for just being sometimes.” Danielle: “…sometimes Susan nearly needs the permission to just rest. So it's like, just let it be.”
This extract highlights the dyadic process engaged in this case, as Danielle provided the “permission,” or perhaps encouragement, for her partner to live a slower pace of life with MS. While some couples were unable to explain how such a dramatic shift in perspective had occurred, many dyads discussed a joint, intentional shifting of their joint narrative from the uncertainty and loss related to MS, towards the positives in their experience. For some, their joint efforts to “help other people with MS” (Mike, couple 1) provided the dyad with a new sense of meaning in an otherwise significantly challenging experience.
Discussion
This was the first study to date to utilise dyadic interviews and individual follow-on interviews to explore couples’ experiences of coping with MS. Three overarching group experiential themes a) “Interacting Individual and Dyadic Coping Experiences,” b) “Evolving Communication and Understanding,” and c) “Regaining Control through the Dyadic Experience,” conveyed the essence of couples’ shared experiences of coping with MS. Overall, the continuous interplay of the individual and dyadic coping experiences appeared to shape each couple’s unique experience of coping with MS. It appeared that each partner faced unique challenges, and had different ways of coping with MS, and at times, couples had difficulty understanding the other’s individual coping process. Yet, learning new ways to communicate over time, allowed partners to develop a more unified approach to managing MS as a dyadic coping system. While couples jointly contended with a high level of uncertainty related to the unpredictable nature of this chronic and progressive disease, the convergence of perspectives and use of collaborative coping efforts allowed the dyad to regain a sense of control over their shared lives with MS.
While couples considered MS to be a shared experience, at times partners differed in their approach to coping with the disease. Couples often attributed the differences in their coping to their innate personality characteristics, developmental experiences and individual cultural backgrounds. These findings may be perceived to provide support for models of dyadic coping which incorporate aspects of both partners’ developmental and cultural backgrounds in shaping the dyadic stress and coping process in couples with MS, such as the DCM (Berg & Upchurch, 2007) and the DR-CM (Karademas, 2022). At times, individual differences appeared to preclude the person with MS and their partner coping with, or emotionally processing MS together. Yet for others, having a “contrast of approaches,” viewpoints or attitudes to coping with MS were considered beneficial for creating balance in the overall dyadic coping system, as each partner appeared to shape and influence one another’s approach over time. Heterogeneity in partners’ appraisals of illness have been considered as a central guiding principle in many dyadic coping models, such as the Theory of Dyadic Illness Management (Lyons & Lee, 2018). Congruent illness appraisals have been associated with greater collaborative symptom management, shared health activities, and open communication in couples coping with other illnesses such as diabetes and cystic fibrosis (Lau et al., 2023; Lyons et al., 2023; Shrout et al., 2024).
The findings of this study demonstrate that at times, incongruence in couples’ approaches to or perspectives on MS, may be perceived as beneficial for providing a sense of emotional equilibrium in the dyad. Having an alternative perspective available appeared to be particularly important when managing difficult emotions related to their uncertain future of possible symptom exacerbations, disability or premature mortality rates often associated with MS. Our findings may suggest that the dynamic in individual partner differences prior to the onset of MS, may influence how couples managed their opposing viewpoints. Both partners’ ability to tolerate the others’ perspective, rather than viewing this as a threat to their own point of view, may have allowed their contrasting approaches to be beneficial for creating an overall balanced dyadic system. The findings of this study make a significant contribution to the literature by recognising the variability in couples’ coping with MS. These findings move beyond the universal viewpoint of congruence in couples’ appraisals of MS as imperative for “successful” or adaptive dyadic coping.
Unsurprisingly, common emotional reactions of shock, fear, depression or helplessness were experienced by both people with MS (Mehraban et al., 2023; Persson et al., 2023) and their partners (Benini et al., 2023; Starks et al., 2010). Yet, some participants chose to intentionally isolate themselves when coping with difficult emotions around MS as a means to protect themselves or their partner. For some, a period of isolation and individual coping was considered to be an important phase to make sense of and come to terms with the MS diagnosis alone. However, concealing their emotions often resulted in one or both partners not getting their needs met by the relationship. For example, when communication of needs and emotions was unclear, partners’ well-intentioned attempts to provide practical support or “fix” the problems of MS were perceived as frustrating by the person with MS. Indeed, in a number of cases, what was required by the person with MS was simply the emotional presence of their partner, to “just be here.” Attachment theory may be a useful framework to conceptualise the caregiving and care-seeking processes in this context (Crangle & Hart, 2017). Attachment theory suggests that individuals internalize working models of relationships that shape their beliefs, behaviours, and expectations within relationships, particularly in times of high stress (Bowlby, 1988). When faced with a threat such as MS, the attachment system may become active and lead some adults to seek closeness and comfort from a close other such as a romantic partner (Crangle & Hart, 2017). This may have implications for understanding how some couples may perceive the security or emotional containment of the familiar partner relationship as providing a sense of safety or comfort when coping with the distressing emotions related to MS. For some, emotional closeness and sharing may support them to cope with the changes and uncertainty related to MS.
In terms of dyadic communication, couples appeared to engage in a reciprocal stress communication process in which they made shared appraisals of their joint illness experience together, as outlined by the STM (Bodenmann, 1997). Couples developed new ways to communicate around MS over time, by having the “tough” conversations around the possibility of MS symptom exacerbation, physical or cognitive decline for the person with MS, and the related additional caregiver responsibilities for their partner. Similar to findings reported in other illnesses such as pancreatic cancer (Zhang et al., 2024), dyadic communication around MS appeared to be an evolving process that changed over time. Increasingly open and transparent stress communication around MS was often triggered by symptom exacerbation or disease progression. Developing a more acute awareness of, and sensitivity towards one another’s needs around MS in turn, appeared to allow for more attuned support and emotional responsivity between partners and a more unified approach to coping with the disease as a unit.
In this study, the joint loss of “control” and “safety” to MS underpinned participants narratives, as they encountered persistent difficulties in managing symptom exacerbation, while struggling to reconcile with an uncertain prognosis and unpredictable disease exacerbation. These findings highlight the medical, emotional, and lifestyle uncertainty related to this chronic and progressive disease that, by its nature, carries uncertainty as a hallmark characteristic (Alschuler & Beier, 2015). However, the stability of the couple relationship appeared to support both partners to regulate difficult emotions around MS, and to gain a sense of control over their shared lives and futures. While previous studies have suggested that a sense of control may reduce feelings of helplessness in patients with MS, and thus aid in the restoration of wellbeing (Ackroyd et al., 2011), in this study, many couples attempted to gain control of the disease by aligning their perspectives on MS and making collaborative or dyadic efforts to manage the disease. Framing illness as a shared challenge (“we-stress”) has been associated with positive outcomes for couples coping with diabetes and cancer (Kayser et al., 2007; Lee et al., 2020). The findings of this research align with theories highlighting the importance of the communal perception of illness as a shared experience (“our disease”) to support collaborative coping (Rentscher, 2019). This was exemplified by many couples in this study, who spoke of jointly engaging in positive health behaviours to manage the shared problem of MS together, for example by jointly maintaining a healthy diet and exercising together.
Despite the adversity they faced, all of the couples in this study appeared to experience some level of dyadic growth through the process. While the perception of life as precious and fragile was framed as a common aging experience (i.e., not specific to MS), the threat of possible disease progression in the future led couples to confront, reassess and re-prioritise their life values at an earlier age (“We were confronted with that stark reality at a much earlier age than you might normally be…”). The acknowledgement that symptom exacerbation could onset at any time, resulted in the dyad taking joint action on life goals with a greater sense of urgency, or encouraging one another to live a slower paced life. The individual experience of adversarial growth of each partner may have also served as a contributor to overall dyadic growth of the couple (“a happier person is a better contributor to a relationship”), which aligns with previous quantitative research reporting a correlation between MS patient and partner growth (Ackroyd et al., 2011). The findings of this study contribute that couples may experience both growth and distress sometimes at the same time, together when coping with MS as a dyad.
While a number of mechanisms have been implicated in fostering growth in patient-caregiver dyads (e.g., stress communication, emotional exchange, a communal sense of illness experience) (Henson et al., 2021; Neate et al., 2018, 2019), couples in this study were often unable to explain how such a shift in perspective had occurred. Some couples appeared to engage in a conscious shifting of their joint narrative towards a search for the positives in their MS experience. It is possible that the person with MS and their partners use each others’ cognitive-emotional perceptions of their condition as a source of key information to amend their own beliefs or behaviour, in a manner that shapes the overall joint cognitive emotional model of MS and ultimately the emotional adaptation of the unit (Carberry et al., 2024). The “contrast of approaches” or “perspectives” of each partner may have contributed to the development of a more-balanced dyadic narrative around the illness. However, it should be acknowledged that couples’ ability to draw on the positives in their shared MS experience often co-existed with the distress around their joint losses and uncertain future related to the disease.
Limitations
Considering the idiographic nature of IPA research, the generalisability of these findings is limited to the context of the couples included in this study (Boland et al., 2018). While there appeared to be no obvious differences in the nature of the data based on relationship length (7–26 years), all of the relationships in this study were established prior to disease-onset which may have influenced the dyadic coping experience. This was referenced by many couples as having a mutual affinity prior to MS diagnosis. In addition, the variability in the nature of MS symptoms and care trajectories may have presented differences in the extent to which couples were impacted by MS. The study sample was well-educated and self-selected, and we cannot rule out the possibility that participants’ willingness to share their experiences may be related to their educated status or to particular valences in their relationships or experiences with MS. With regard to the latter, the offering of an additional individual interview may have allowed for the inclusion of additional experiences, thus providing a more balanced perspective on dyadic coping with MS. Some information regarding participant characteristics were not collected in this study including the precise location of the participants (all interviews took place on Microsoft Teams), race/ethnicity, sexual orientation, and disability status. While the impact of the aforementioned demographic factors on couples’ coping was not the focus of this study, it is acknowledged that these factors may have influenced the data to an unknown extent, and should be explored by future research in this area.
Clinical and practical contributions
These findings may assist couples, researchers and clinicians to better comprehend the dyadic processes underpinning couples coping with MS, and how this in turn affects their experience of coping with the disease. Overall, it seems that creating an understanding of MS as a shared experience may support couples to align their perspectives and take a more collaborative approach to disease management. While communication appears to be a key factor for helping partners to understand the other’s needs and align their perspectives on MS, couples described communication as a process that evolved over the disease course. As such, global recommendations of open communication for couples coping with MS may not always be a good match to the needs of a dyad. Instead, couples coping with MS may find it more useful to explore a more diverse range of communication strategies over time, and at different stages of the disease process.
In this study, all couples described experiences of growth related to the adversity and distress of living with MS. While the dyadic growth process did not necessarily negate couples’ experiences of distress, a strong partnership may be experienced as a vehicle which allows couples to maintain a sense of control when faced with an uncertain future of possible symptom exacerbation, disability or premature mortality. Future research should consider exploration of the processes underlying dyadic growth in couples coping with the high level of uncertainty inherent to MS.
Conclusion
The aim of this research was to explore couples’ experiences of coping with MS, using dyadic interviews. Our findings provide key information on the evolving process of dyadic coping with MS. When communication around MS was unclear, this often led to misinterpretation or emotional distancing in the relationship. Partners’ well-intentioned attempts to “fix” the problem of MS were often perceived to be unhelpful, when what was required by the person with MS was simply to “just be here.” Ultimately, a strong dyadic partnership and aligned perspectives on how to best manage MS provided a sense of safety for couples in coping with their uncertain future with MS.
Supplemental Material
Supplemental Material - “Just be here”: An interpretative phenomenological analysis of couples’ experiences of dyadic coping in multiple sclerosis
Supplemental Material for “Just be here”: An interpretative phenomenological analysis of couples’ experiences of dyadic coping in multiple sclerosis by Serena Carberry, and Donal G. Fortune in Journal of Social and Personal Relationships
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research cannot be shared with any person because participant permissions to share their provided data were not sought. As such, the raw data generated and analysed in this study are not publicly available. The materials (interview schedule) used in the research can be publicly posted. The materials can be obtained in the supplementary data file.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.