
Abstract
Parents of children with a disability experience elevated levels of stress compared to parents of typically developing children, which represents a risk for their couple relationship. Research on families where a child has a disability is principally based on mothers. More knowledge is needed about the paternal perspective. We conducted semi-structured interviews with seven fathers (aged 36–54 years) of children with a disability (primary school age to early twenties). We analyzed the material using qualitative conventional content analysis, focusing on participants’ descriptions of couple relationships. We categorized the participants’ descriptions in two main categories: Couplehood and Co-parenting. Throughout the material, partners were described as romantic partners, co-parents, and collaborators. Participants described that couple communication and emotional expression within couples were affected by parenting a child with a disability. Moreover, participants described influence by cultural masculinity norms on their involvement as partners and parents, and on the dynamic within their couple relationships. An uneven division of labor was described. A practice implication is that communication and emotional expression styles within the parental couple should be a key focus when working with families of children with a disability. The findings also suggest more active involvement of fathers in children’s health care.
Life stressors have been shown to have a negative impact on couples’ relationship quality (Buyukcan-Tetik et al., 2016; Kulik & Liberman, 2022). A recent systematic review showed that parental couple relationship quality is related to various aspects of family health, such as level of flexibility or conflict, co-parenting quality and parent-child relationships (Jiménez-Picón et al., 2021). Parents of children with a disability may experience more demanding parenting tasks than parents of typically developing (TD) children (Miodrag et al., 2015; Tøssebro & Paulsen, 2014). Consequently, parenting a child with a disability represents a risk for higher levels of stress and mental and physical health problems (Cohn et al., 2020; Oelofsen & Richardson, 2006). In this article, the term disability refers to developmental, physical, or psychological impairments or disorders that are congenital or appears before the age of 18 years. Knowledge on how couple relationships may be affected by extended parenting demands is essential for health professionals working to support and protect families where a child has a disability. Studies on parenting in families where a child has a disability are principally based on mothers or have a disproportionate female respondent bias (Cohn et al., 2020). Therefore, more research on the paternal perspective is needed, and fathers should be incorporated and studied concurrently (Thackeray & Eatough, 2018).
Fathers, as well as mothers, of children with a disability have been shown to report higher levels of mental health problems compared to the general population, but fathers report lower levels of mental health problems than mothers do (Gau et al., 2012; Zahl et al., 2023). Fathers have also been found to report less parenting stress than mothers (Pinquart, 2018), and to seek less social support than mothers when experiencing life stressors (Chesler & Parry, 2001). However, Seymour et al. (2022) found that fathers tended to prefer informal social support as opposed to seeking professional help, and that fathers relied heavily on support from their partner when experiencing psychological distress. Pelchat et al. (2009) found that fathers of children with a disability tended to repress rather than express negative emotions, and to use avoidance strategies such as spending more time at work. Other studies show that norms, stereotypes, and expectations based on gender roles directly impact paternal parenting (Chesler & Parry, 2001; Lashewicz et al., 2016; Thackeray & Eatough, 2018). Further, fathers report to receive less flexibility from their employers (Vatne et al., 2023) and are generally less involved with service providers than mothers (Thackeray & Eatough, 2018). Fathers of children with a disability have described feeling excluded from health care discussions about their child and feelings of being perceived as a “lesser parent” than the child’s mother (Docherty & Dimond, 2018; Vatne et al., 2023). Medical services and other support systems expect mothers to be more involved than fathers, and consequently contribute to maintaining traditional roles in these families (Docherty & Dimond, 2018; Jenhaug, 2018).
Research has demonstrated the potential negative impact of parental stress on marital relationship satisfaction (Latham et al., 2022; Williams & Parra, 2019). A study of parents of children with disabilities found that more daily stressors were associated with lower marital adjustment for both mothers and fathers (Stoneman & Gavidia-Payne, 2006). A possible factor affecting the relationship between stressors and marital adjustment is co-parenting quality. The term co-parenting refers to how partners that raise children together relate to each other in the role of parent (Feinberg, 2003). Parents of children with a disability has been shown to have lower co-parenting quality than controls (Norlin & Broberg, 2013). This specific part of the parental relationship has been described as an important mediator and moderator of the impact of external stresses on the family relationships (Feinberg, 2003). Thus, potential challenges from an extended caregiving burden will impact the co-parenting relationship, which in turn could impact the parental couple relationship. On the other hand, well-adjusted co-parenting may protect parental wellbeing and overall quality of the parental relationship. Research has shown that marital quality is associated with supportive co-parenting (Jiménez-Picón et al., 2021), and both marital quality and co-parenting quality have been shown as important predictors of parental wellbeing (Kersh et al., 2006; Norlin & Broberg, 2013). Satisfaction with the division of burden within the co-parenting unit has been found to serve as a stress buffer for mothers, reducing the negative impact of parenting stress on their wellbeing (Lehr Essex & Hong, 2005) The body of research on couple relationships in the context of parenting a child with a disability is relatively small. Moreover, the existing research mainly comprises quantitative studies. To our knowledge, there are no qualitative studies of men’s perceptions of their couple relationship in the context of parenting a child with a disability.
The current study was conducted in Norway. The Scandinavian countries are viewed as egalitarian compared to other high-income countries, with high female employment rates and active policies against gender inequality (Tøssebro & Wendelborg, 2017). Since the 1990’s, active policies have been implemented in Norway to increase paternal involvement in childcare and support a dual-earner family model (Brandth & Kvande, 2013). The Norwegian context has been shown to foster less gender inequality in families of children with increased care needs compared to other high-income countries (Vinck & Brekke, 2020). Nevertheless, Norwegian women reduce their work hours more than men do to care for family members, working on average 7.5 hours less per week compared to men outside the home (Jenhaug, 2018). A majority of the above cited studies on families of children with a disability are conducted in English speaking, high-income countries (Latham et al., 2022; Seymour et al., 2022; Stoneman & Gavidia-Payne, 2006). A Swedish study (Norlin & Broberg, 2013) showed similar findings of the studies conducted outside Scandinavia. However, this study is ten years old and knowledge from the current Scandinavian context is needed. All family socialization is embedded in an environmental context, as proposed by systemic-ecological theory (Anderson et al., 2013). A constructivist epistemological position is thus appropriate for investigating couple relationships in the context of parenting a child with a disability.
We have previously conducted a qualitative study based on the data presented in the current article (Vatne et al., 2023). The aim of the first study was to describe men’s experiences of being a father in families where a child has a disability. See Vatne et al. (2023) for analysis and results. In the analytic process of the first study, we noted that fathers often included statements about their partner and their couple relationship when asked about their own role as a father. These dimensions were not investigated systematically in Vatne et al. (2023). Therefore, we conducted a secondary independent analysis of the material. A secondary analysis offers the opportunity to do an in-depth analysis of themes that were identified, but not addressed in the primary analysis applying a new perspective or a new conceptual focus to the original research issues (Heaton, 2008; Hinds et al., 1997).
Our main aim for this study is to understand more about men’s perceptions of their couple relationship in the context of parenting a child with a disability. Further, this qualitative study aims to contribute with depth and nuance to the principally quantitative pool of research on this topic. We pose the following research questions: (1) How do fathers of children with disabilities describe their couple relationship? (2) What aspects of the couple relationship do fathers perceive are affected by parenting a child with a disability?
Methods
Participants
Seven White-Norwegian fathers aged 36–54 years (M = 47.6, SD = 5.8) from families where a child has a disability participated. One participant was an adoptive father, the remaining six were biological fathers of the child with disability. All the fathers lived with female partners. All but one father were cohabiting or married to the mother of the child with a disability. One was divorced and had a new female cohabiting partner with whom he also had children. Four participants were employed fulltime, and two were on long time sick leave. One participant was a student. Five of the children had an intellectual disability; three of whom had a co-morbid conduct disorder. One child had a progressive genetic disorder affecting intellectual and physical functioning. One child had a progressive physical disability. The age range of the children with disabilities was from primary school age to the early twenties. One child lived in residential care (child of participant number 2), the remaining six children lived in the parental home. All participants also had TD children. The mean number of children per participant was 3 (range 2–5). All the participants lived in urban areas in Norway. Given the small sample size and the qualitative nature of the study, the analyses were done without distinguishing the material based on these background factors.
Recruitment
The study was approved by the Regional Committees for Medical Research Ethics South East Norway as part of a larger research project, project number 2013/2118. The overarching goal of the project was to map family experiences and develop interventions for families of children with disabilities. The participants were recruited by convenience sampling. A study information letter with consent form was sent to a total of nineteen fathers that lived within a one-hour drive from the study site. Three of the consenting participants had previously contributed in various parts of the project as user representatives. The remaining four participants came from families where the mother had participated in an open trial of a sibling-parent intervention (Haukeland et al., 2020). Five fathers declined and seven did not respond. There was not collected any data from the eligible participants who declined/did not reply.
Data collection
The data collection was conducted through individual in-depth semi-structured interviews using an interview guide. Empirical and clinical knowledge about fathers in families where a child has a disability and a pilot focus group with fathers of children with a disability informed the interview guide. Fathers who had previously contributed as user representatives reviewed a first draft of the interview guide. They were asked how they perceived the relevance, accessibility, and sensibility of the questions. A final version of the interview guide was completed based on the user feedback.
Questions in the interview guide.
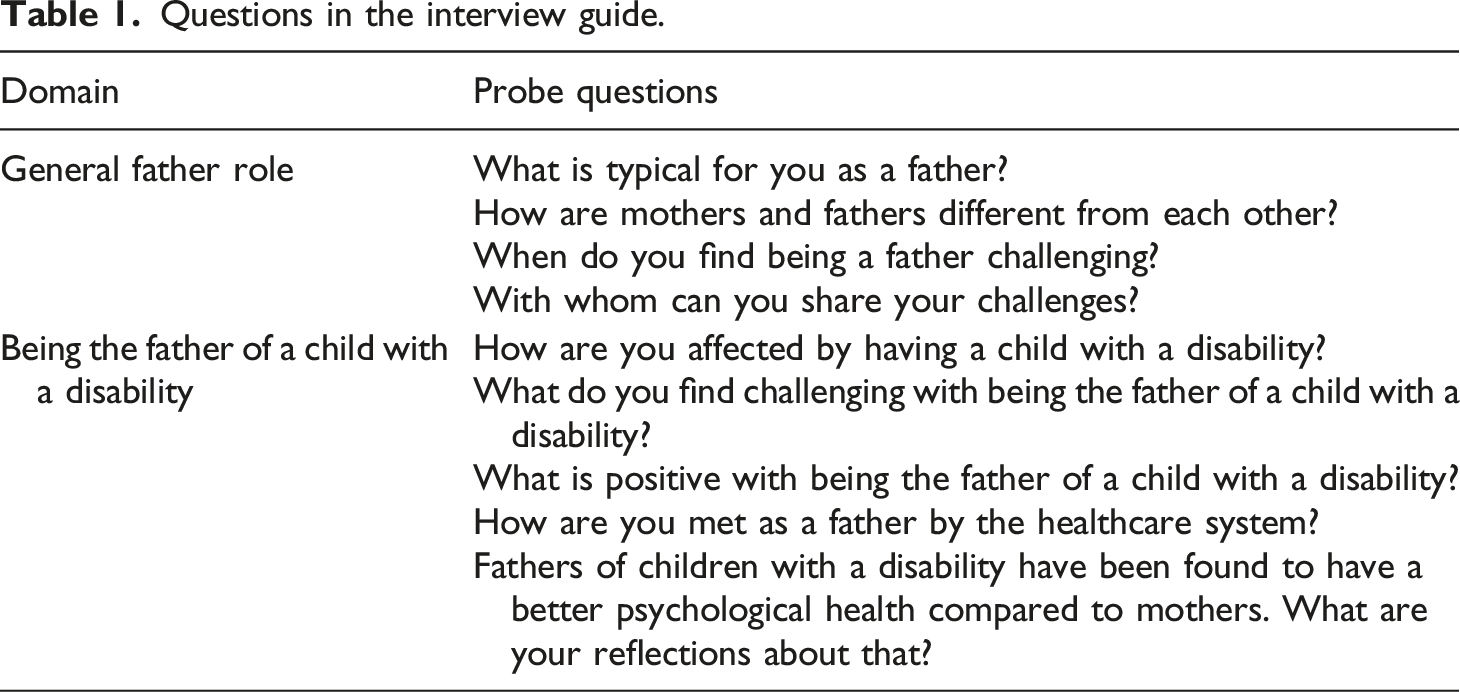
The interviews were conducted face to face and were audiotaped. The interviews were conducted and transcribed verbatim by the second author, an advanced clinical psychology student. Four participants were interviewed at home, one at a competence center, one at the participant’s workplace, and one in a park, all at the participants’ choice. The duration of the interviews was from 76 to 196 minutes (mean = 132 minutes).
Data analysis
The material was analyzed through conventional content analysis (CCA) (Hsieh & Shannon, 2005). CCA is characterized by subjective interpretation of topics in a text, aiming to identify categories through systematic classification. Categories are derived from the material as opposed to using preconceived categories based on existing theory or empiricism, as is recommended when former studies about the phenomenon in question is limited (Elo & Kyngäs, 2008). Thus, CCA is also described as an inductive category development (Hsieh & Shannon, 2005).
The main analysis was conducted by first and last author. The first author read through the material as a whole, to get a general impression and to identify sections where participants talked about their partner or couple relationship. In this first step, the first author made brief notes on what themes the participants talked about in relation to their partner and made a first set of categories based on these notes. Next, the first author coded the material using the NVivo 12 Pro software (QSR International Pty Ltd., 2018). The first set of categories was used in the first round of coding, and then developed through repeated consensus meetings with last author. The foci of the consensus meetings were: identifying unintended interpretation, making sure that only explicit expressions and words guided the coding, and sorting categories into main and subcategories. In each round of coding/consensus meeting, some categories were changed, moved, renamed or merged. Coding/consensus meeting were repeated five times.
Findings
Through the analysis of participants’ descriptions of their couple relationships we identified two main categories: Couplehood, with corresponding subcategories, and Co-parenting. See Figure 1 for an overview of main categories and subcategories. The categories were not treated as exclusive and descriptions were sometimes placed into more than one category. Categorization of participants’ descriptions of couple relationship.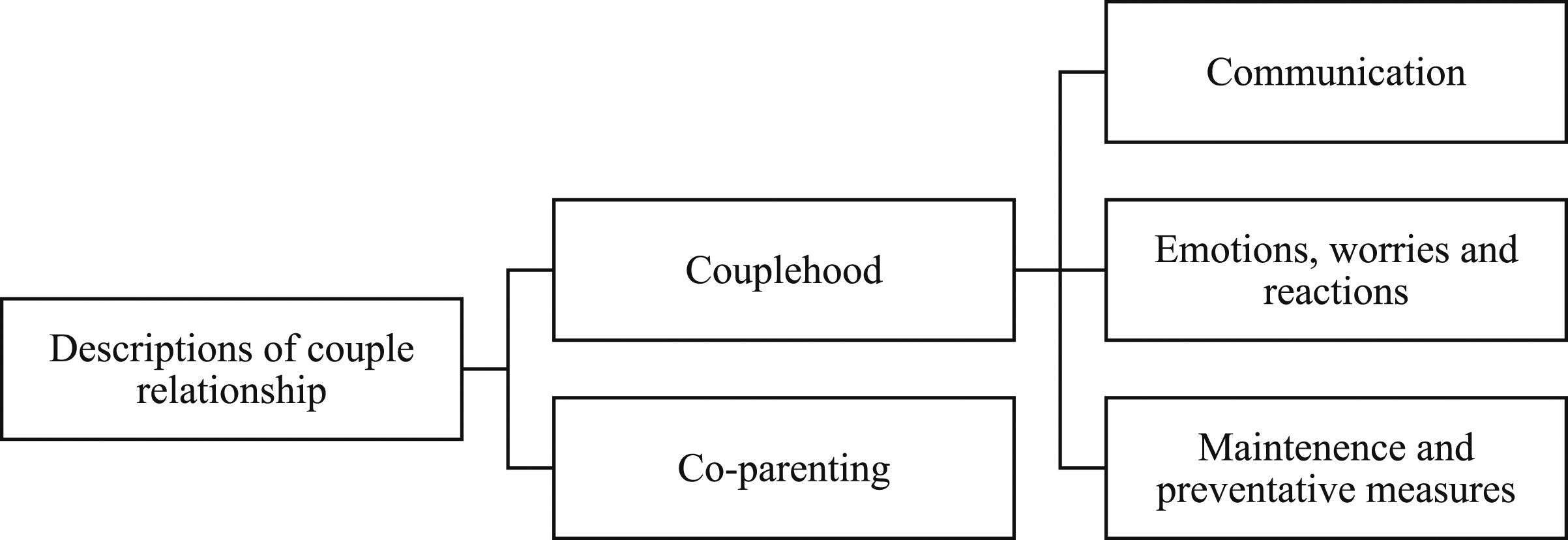
Couplehood
In this category, we grouped all descriptions of how participants perceived their couplehood and themselves as parts of their couplehood. Herein, we sorted the descriptions into the following subcategories: (1) Communication, (2) Emotions, Worries and Reactions, and (3) Maintenance and Preventative Measures to Protect the Couplehood. We chose the construct couplehood for category name in order to specify that we herein grouped descriptions of the dyad and romantic relationship between the partners, as opposed to the more general construct couple relationship that is used elsewhere in this article, and describes more globally two adults in a committed relationship sharing an everyday life and raising children together.
Communication
In this subcategory, we grouped participants’ descriptions of style, strengths and challenges of communication in their couplehoods. Participants gave descriptions of how opposite communication styles in their couplehoods limited the communication in different ways. Being more withdrawn than one’s partner, and uncomfortable with the thought of talking more openly was described. Here, silent agreement and non-verbal communication around the need to withdraw was also described: I suppose I can bar myself in a little too much sometimes. But, after all, we have been together for twenty-four years or something like that – we know each other inside out. So, she accepts it, if I sit down with headphones on not wanting to talk, there’s a reason why [chuckles] (…) And we know each other – there’s a lot of non-verbal communication, you know? (1)
The participants gave descriptions of what the couple could share with each other.
Descriptions of open communication and being able to talk to partners about anything were given. However, a limited communication due to a complicated family situation was also described. Participants explained that they could inhibit their own expression of thoughts in order to spare their partner of potential pain. I remember the decision that “I’m not sharing this with Mona [partner]”, that’s how I thought. I simply wanted to spare her, and I think it was about, sort of, that if I hit skid row, then she is holding the fort by herself. (1).
A feeling of being spared for their partner’s pain, and a longing to know more about their partners inner thoughts, was also described. I think my wife suffers more in silence than I do, really. Once in a while, I realize that she has seen her GP and that there are issues that she hasn’t…Well, shared. And I guess it’s because she wants to spare me and stuff. And indeed, you can say a lot about that strategy, but that…[laughs] (…) I don’t think I’m going to try to train her to…Change. Even though I would very much like to have a little more insight in… In that. (3)
The participants also described that a demanding family situation forced couples to limit their communication, stressing the feeling of not having sufficient mental space for reciprocal emotional dialogue. We are two people who are living with some challenges, you know, and we both have our own sets of challenges. I don’t know, but it takes a little effort to turn oneself off for a little bit and see the needs of the other right there and then. And that is not always easy, sort of, to do that adaption in everyday life. (…) Time and space are one thing, but it is also a question of mental time and space. I mean, to adapt, to see the other and think “oh, shit. Now I actually have to turn myself off for a little bit and then I’m going to…Listen for a little bit” [laughs]. (…) I mean, because it is also something about our circumstances of life, they are very demanding. So, in some areas, you have to sort the important from the non-important. (3)
Some of the descriptions of opposite communication styles emphasized that the fathers perceived different ways of communication to be typical for respectively men and women. You can analyze things to death, you know. And I think that is something men are a little better at not doing. We maybe don’t analyze everything to death. We look at what happened, and then we don’t necessarily wonder why or consider all the things that could have happened. My wife is very in to all those things that could have happened, and sort of analyzing things to death. If someone says something, and interpretations, you know? (…) So, I guess we are very different when it comes to how much we interpret things. (5)
A feeling of being a somewhat untypical man due to talking openly about emotions in the family was also described. “I keep reading that men have a harder time talking about feelings than women, but that’s not my own experience. In our home, I think we talk a lot about feelings. Both men and women.” (2).
Emotions, worries and reactions
In this subcategory, we grouped descriptions of emotionality within the couples in general, and appraisals of one’s own and spouses’ worries and reactions related to their critical life situation with a child with a disability. The participants described both differences and similarities in emotional expression style and reaction patterns within the couples. In terms of similarities, participants talked about severity of reaction to their critical life situation, rather than specific style of reaction. They described that both themselves and partners was severely affected by their child having a disability, yet in different ways. In our case I think both of us are in fact at the very end of the rope. But we are indeed different, we have different reactions. But both of us are without permanent employment as a consequence of Einar’s [child with a disability] disease. We both struggle. (2)
In terms of differences, participants described opposite emotional expression styles or styles of reactions. They expressed that opposites represented somewhat of a challenge in their couplehoods. She is a lot better than me when it comes to controlling her mind. She’s really strong, like “these thoughts are not allowed to settle with me”, you know? (…) So, in that way, that is maybe our biggest challenge. That she is so damn strong, that she has a little trouble realizing and accepting that I can’t get out of the swamp, you know. Like, “why can’t you just think like me?”. So, that’s our challenge, with being different personalities. (1)
When it came to worry, participants described that they worried just as much as their partners, but worried about different issues or different aspects of their situation. They linked worry to perceived role in the family, stressing that they worried about issues that they saw as their main responsibility. Perception of main responsibility seemed to be influenced by socially defined gender roles, which participants reflected on explicitly. If I don’t consider it my responsibility, I can turn it off a little. So, she worries about school if I don’t have anything to do with school. But I rather worry about if the house is going to fall down, you know. Because that is my responsibility, to make sure the house doesn’t fall down, or that the car is running. So, it depends on how you define your role, I guess. And what constitutes the different roles. (5)
A feeling of their emotional expression not being recognized because it is different from the emotional expression of their female partner was described. The participants expressed a feeling of ‘right’ and ‘wrong’ emotions based on their female partners’ emotions as the norm. A real slap in the face, you know. I think that’s how it is for men sometimes. Things get rough and nobody gets you. And you can’t have the feelings you have either, because those are not the feelings that your wife has. (5)
A feeling of paternal grief not being recognized by society was also described. “Mother, mother. Mothers die of grief”. I’ve cut out so many newspaper articles… In our situation, it’s me that has had the bigger role. Not that I blame her for that at all. But I would like to claim the right to die of grief, so to say. Like any woman would have. (2)
Further, participants problematized how social expectations of masculinity shaped their coping strategies to ‘being strong’ for their wife and family. I guess it’s that stigmatization thing. That the appearances break down and you’re not Superman – so now what? And then you feel like you have to be strong because your wife just cries all the time, so you have to stay strong for the kids. So, you don’t allow yourself to… (5)
Maintenance and preventative measures to protect the couplehood
In this subcategory, we grouped descriptions of measures taken to prevent challenges and protect the couplehood from strain. The necessity of maintaining and protecting their romantic relationship, and how challenging it can be to find the time to do so was also described. “We are very conscious of working on our couplehood, you know. We have a demanding everyday life and thus have to set aside time for each other too. I think we need timeouts like that, consider ourselves a little.” (6)
Attending couple’s course to prevent expected challenges from co-parenting a child with a disability was described. When we moved together and got married, we knew about the potential challenges that could come from “my kids, your kids”, but especially with my son who is sick. We knew that that could be a strain on our relationship. So, we attended a prep-course for parents of children with disabilities. That was quite interesting, because my impression was that most of the other couples at the course, were there because problems had piled up in their marriages. We were there because we knew that problems could pile up. (2)
Co-parenting
In this category, we grouped all descriptions of how the participants appraised themselves and their partners as a co-parenting unit. We chose the construct co-parenting for category name in order to capture the relationship between two individuals that share a child raising responsibility, and navigate parenting together.
The participants described having common goals in childrearing, e.g., in terms of emotional sensitivity or views on children’s independence. In terms of reaching common goals, the participants described ongoing discourse with their partners about how to best facilitate the desired development. We are both occupied with the emotional lives of our children. Our own emotional lives as well. But she is probably a lot better at pointing out the emotional aspects. If we have a fight, which we rarely do… But if we do have a discussion, I often argue that it is a little too much “wrapping in cotton wool”. While she would criticize me for pushing a little too hard. (2)
However, the participants also described how complementing each other was a strength when solving the parenting task together. “Well, I think there is a difference and I think that that is an advantage, and… I sort of think that we are strong together. (Yes, a good team?). A Good team. That’s the thing.” (1)
Agreement and similarity in how to approach practical aspects of parenting was also described. “When we look at the father- and mother role… We are very similar, in terms of what’s important. We interact very well. That probably leads to… We are managing quite well, really.” (7)
The necessity of both parents taking on responsibility across traditional mother- and father roles in order to be a team was described. “You have to be a team, really. You have to. You can’t just be a mother or a father. You have to be both – especially when you have several children.” (7)
The participants described complimentary emotional communication styles in their own and partners’ interaction with their children. They would get comfort from me too, but they would get more comfort from my wife. I think, in general, that I would be quicker to say that “ok, but if you’re sad, what if you think…?” I would be quicker to suggest a solution. She would be quicker to think that maybe they’re not interested in a solution, maybe they just want to say what it is. Having someone listen to them. (2)
Further, the participants appraised their own and partners’ intensity, degree or character of involvement, in interactions with children. She is a lot closer by in the children’s lives, and a lot more… asking lots of questions. Like, actively curious. And very good at following up. I mean, she is close by all the time. She has a good overview over what’s going on in their lives and where they are and such… (3)
The participants described how different roles within the co-parenting unit had developed over time. They referred to both life events such as long-time illness or societal regulatory conditions such as paid parental leave rights in their descriptions. I had several rounds of paid sick leave. So, I got to stay at home with him [child with a disability] more. That made us realize that being one on one with him works really well. So, that sort of became my role. I take most of the fights with him, with his challenges. And then she deals more with the other two. (7).
The participants described an uneven burden between partners. They described that the parent being more at home was typically taking on a bigger part of the family life labor. There is no doubt that it is Nina [partner] that has had the main responsibility, or at least taken the main responsibility. As I mentioned, it can be months at a time when she deals with 90 or 80% of what is going on at home. And then she will probably find that stressful. Even though it has been better the last few years, I still think that she sometimes finds it stressful. (4)
The participants further described that one of the parents had stayed out of employment to take care of the child with a disability. Herein, descriptions of female partners losing opportunities for employment and work life participation were given. I have a wife who has not been in ordinary employment since our youngest child, which is our child with a disability, was born. (…) And that is - she took a huge responsibility in the beginning when our child was often physically ill. And that had major consequences for her and… Her opportunity, and ability, to work – or for work life participation. (3)
The participants also described taking on a majority of family life tasks due to their partner having poor health. It is indeed a little more responsibility on my end, that is, it’s me that get up and deal with more in the morning and… Often, when she is tired, I deal with everything around bedtime too, and… Going a little further, I think, than average. (7)
The participants also referred to partners’ competence from being nurses or special needs educators to explain how certain tasks were distributed, for example why their partners took all of the responsibility for attention to, and communication with, support system professionals. It’s mostly Nina [partner] who’s handled that [cooperation with support services], so…I haven’t been so involved in that. She is after all the expert among the two of us. Yes, it has been…something that has made me not take part that much, because she knows it, knows the right way with words to get the things that you want and need done. So, she has dealt with all that. (…) I have talked about it, but she’s the one that has picked up the phone, written the letter, fixed all that. (4)
Some of the patterns were explicitly connected to a gender perspective by participants. There is no doubt that Nina [partner] is dealing more with the children than I am. And I guess she always has. With Ingrid [child with a disability], it has always been like that because Nina was a student when we had her, so I wasn’t eligible for paid parental leave. Consequently, it was only Nina who stayed at home with Ingrid. And so, they got a very close relationship, the two of them. I never really managed to catch up with that, not in any way. And mothers are the people that children get attached to immediately. And that bond is never broken, and you can never as a father get a closer relationship to your children than mothers, I doubt that. I have a good relationship with the children, but Nina definitely has a closer relationship. They tend to go to her, if they want to ask something. (4)
Suggesting gendered expectations from support systems, participants talked about how practitioners failed to involve them equally to their female partners, and how this led to an uneven division of responsibility between partners. I feel like I am put on the sideline. Things are channeled through the mother. Correspondence is always addressed to the mother; I don’t think I have ever seen it addressed to me. (…) It always has her name on it, never my name. And we are talking about a lot of envelopes. (5)
Participants described a feeling of mothers being seen as the primary caregiver by support systems, also in their presence. I have a clear impression that it is the mother that traditionally is seen as the primary parent [by support system professionals]. And it actually has hit me sometimes when we have been asked different questions, we were both there but they only talked to Mona. (1)
Discussion
The aim of this qualitative study was to gain knowledge on how fathers of children with a disability perceive their couple relationships, and how this is affected by parenting a child with a disability. The participants’ descriptions were categorized into the two main categories Couplehood and Co-parenting. Our analysis showed that participants described their partners as romantic partners, co-parents and collaborators, discussing the nature of their communication, emotionality, parenting, and family life administration in the context of their family situation.
When describing couplehood, participants discussed how communication and emotional expression was limited, or had to be adjusted, as a consequence of their parenting situation. Opposite styles of reaction or emotional expression were not described as problems in and of itself, but that lack of understanding and acceptance for each other’s differences was described as a challenge. The participants described that both mothers and fathers could withhold their own emotions in order to spare the partner or due to lack of time or capacity to share. The participants’ descriptions showed reciprocal adjustments and understanding within couples. Also, we found that fathers actively limited or adjusted their emotional expressions in order to conform to perceived norms. These findings can be linked to research on sensitivity and emotional communication in close relationships. Sensitive responses from a partner towards one’s emotional expressions has been found to facilitate more open emotional communication within couples (Ruan et al., 2020). Open and strong family communication is related to decreased distress and improved adaption to stressful life experiences (den Heijer et al., 2011). Further, adaptive expression of negative emotions can serve as a means to elicit social support or improve social relationships (Kennedy-Moore & Watson, 2001). Seeing our findings in light of earlier studies, we may speculate that parents who adjust their emotional expressions in order to spare their partner, or due to lack of capacity, are at risk of withdrawing from distress relief and partner support. The descriptions of communication found herein are in line with previous research that has shown that communication in families where a child has a disability can be more withdrawn compared to families with only TD children (Murphy et al., 2017). Whereas child age, conversation topic, and severity of the disability have been suggested as potential influencers on withdrawn family communication (Murphy et al., 2017), our findings demonstrate how the demanding family situation in itself can hinder communication, and that there seems to be some influence by cultural expectations of masculinity on fathers’ expressions.
In sections that concerned the couple as a co-parenting unit, the participants described both agreement and ongoing discourse. Also, participants gave comparative descriptions of their own and partners interaction with children. Herein, how parent roles and patterns of interaction with children had developed over time, often resulting in an uneven share of responsibility for children and/or one parent being currently unemployed. These findings are in line with research on family policies in Norway and Scandinavia. Norway has active dual earner policies, for example a specified father’s quota in the set-up for paid parental leave (Duvander et al., 2020). Still, the labor market has persisting gender and wage inequalities and family choices regarding childcare still tend to be traditional compared to the intentions of policies (Leira, 2006). In our analysis, we found that both mothers and fathers had the role of significant parent after staying at home, from the perspective of fathers. Thus, it is important to distinguish between pragmatic choices made by an individual family and societal patterns of gender (in)equality. Still, our findings reflect the same pattern as shown by Tøssebro and Paulsen’s (2014). Their findings show a systematically lower employment rate for mothers of children with a disability compared to mothers of TD children, while the same difference is not seen for fathers (Tøssebro & Paulsen, 2014). There is a documented negative relationship between daily stressors and marital adjustment (Stoneman & Gavidia-Payne, 2006) Considering the potential protection that lies in a satisfaction with the division of burden, and in the overall co-parenting relationship (Feinberg, 2003; Lehr Essex & Hong, 2005), an unequal division between parents which leaves one parent with a bigger burden represents a risk factor for family wellbeing.
Gender was a reoccurring theme in the participants’ descriptions. Reference to gender roles was made both to describe the nature of their relationships, and to explain differences between participants and their partners - not only regarding personal traits like communication and emotionality but also practical differences in division of labor and degree of involvement with children. The descriptions represented various understandings of gender attributes and gender roles, including gender as fluctuant, gender as socially defined, and gender as inherent and biological. Descriptions stressed that the external expectations of women and men, or mothers and fathers, were unequal.
From a constructivist standpoint on gender, it has been argued that when people identify with the socially constructed understanding of gender, this guides their behavior and leads to conform to gendered expectations (Bohan, 1993; Crawford & Unger, 2000). From the standpoint of social role theory (Eagly, 1987), family choices and distribution of care tasks can be understood as an expression of mandates. That is, structural social roles guide fathers’ and mothers’ intrinsic expectations of themselves, perceived expectations from health professionals, employers, and others. However, in our analysis, participants showed a critical awareness of gender perspectives in the sense that they gave descriptions to explain what they saw as imbalance of burden within their relationships, instead of conforming to the traditional expectations towards mothers and fathers. We also found that participants expressed discomfort with gendered expectations, expressing feelings of limitations and being hindered by such norms. Studies of social roles have shown that there is little correspondence between perceptions of respectively men and fathers, whereas perceptions of respectively women and mothers are largely overlapping (Park & Banchefsky, 2018). In other words, the social mandates assigned to men are in greater conflict with a caring paternal role, compared to those of women and mothers. Our findings reflect this conflict for fathers. One may ask whether fathers of children with extended caring needs could find themselves in a stronger conflict between cultural norms and their own wishes or instincts, than fathers of TD children. The ambivalence described by our participants is a relevant contribution on the constructivist understanding of gender in the context of parenting a child with a disability.
Our findings can be understood in light of systemic and ecological theory. Bronfenbrenner’s (1977) bioecological model explains the multiple levels of context within which an individual operates. The model explains how the individual is in reciprocal development with surrounding systems, and how surrounding systems are in reciprocal development with each other over time. Although in a progressive Scandinavian society, with high levels of women in employment and paternal involvement in child care, the idea of men as protectors and breadwinners is still a part of our cultural consciousness. In our analysis, we found that cultural expectations of mothers and fathers (the macrosystem) affected both emotionality, communication and division of burden within the couple and family (microsystems), and flexibility from employers and involvement from health care professionals (micro- and ecosystems). According to Bronfenbrenner’s (1977) model, participants’ ambivalence towards perceived cultural expectations has an impact on surrounding systems and will in turn contribute to change. At the same time, the described ambivalence could stem from egalitarian norms in the Scandinavian societies. From a systemic-ecological standpoint, the parental couple relationships of parents of children with a disability is closely connected to social and cultural factors.
Our study showed that fathers (and according to fathers, also mothers) may withdraw their emotionality in order to spare their partner or adjust to the situation. Nevertheless, the participants referred to cultural expectations of masculinity when describing their own withdrawal. This suggests interesting nuance to previous studies showing that fathers of children with a disability report less stress (Pinquart, 2018), and seek less social support (Chesler & Parry, 2001) than do mothers. That is, the withdrawal of emotion may help explain why fathers report less stress and seek less social support. Our study suggests that cultural norms may be an important influence on fathers’ expression of stress and support needs. Based on this we can speculate about whether cultural expectations of masculinity and fatherhood limits fathers’ coping and mastering of their parent and partner role in time of family crisis. Further, it can be asked how this in turn affects parental couple relationships, e.g., how parents are expected to master one’s parent and partner role when society limits and defines your role. To protect and support parental couple relationships in families where a child has a disability, changes in society’s ideas of masculinity and fatherhood would be advantageous.
Limitations
This study was not designed with the aim of investigating perceptions of couple relationships. The theme was nevertheless major in our interview material of which main aim was to capture men’s perceptions of their role as a father. Had the study been designed with the current research questions as guide, the interview template would have contained specific questions on couple relationships and how the parental couple relationship was affected by parenting a child with a disability. This could have resulted in clearer findings. Although there are advantages in doing a secondary analysis, in terms of studying previously excluded topics (Long-Sutehall et al., 2011), and so avoiding underuse of valuable qualitative data, the advantages of investigating the mentioned topics in an open manner, with the potential for in-depth answers and relevant follow-up questions, are obvious.
Second, the term ‘father role’ may appear abstract to fathers, and they may struggle to distinguish parenting in general from parenting a child with a disability. Indeed, this may also be indistinguishable from a parent experience perspective. Moreover, gender segregated parenting was not explicitly discussed with fathers. A clearer division in the interview guide between pragmatic differences on the family level, and more structural and problematic gender inequalities in society could have been helpful to make the term ‘father role’ more meaningful to participants.
Third, four of the participants came from families where the mother previously had participated in a sibling-parent intervention, aiming to improve communication between healthy siblings and parents. This might have affected descriptions captured by the Co-parenting category. Lastly, the small sample size coupled with the wide age range of the children, and one child being in residential care needs to be addressed as a limitation. The parenting demands of these fathers at the time of the interviews were in all likelihood quite different. This could have affected the level of strain or exhaustion that participants expressed
Reflections around generalizability of the findings are also opportune: Qualitative research seeks generalizability within cases, as opposed to across cases (Tracy, 2010). The limitations discussed above could potentially challenge generalizability across cases. However, within all cases, the construct of couple relationship was given meaning by the descriptions of the participants. The role of communication, emotionality, norms, and burden filled the couple relationships in different ways across cases.
Implications and conclusion
Our findings have implications for practice. We found that parental couple relationships were affected by parenting a child with a disability. Most of all, couple communication and mutual expression of emotion seemed to be at risk. Clinicians working to support and protect families where a child has a disability should be attentive towards communication and emotional expression within the parental couple relationship, to find potential for distress relief and partner support for both parents. Our study suggests focus towards potential conflict between fathers’ own intrinsic expectations as partners and parents, and external norms and expectations. Clinicians’ sensitivity towards potential impact from cultural norms on fathers’ involvement or expression of emotions or needs would be beneficial for practice. Fathers of children with a disability might respond to different approaches than do mothers in order to express their emotionality and support needs. To protect the family and consequently children, finding ways to ensure support and stress relief for both mothers and fathers is essential.
Keeping the active involvement of fathers in mind is crucial. Fathers being left out of the health care of their children represents a risk for the parental couple relationship in the way that mothers may be left with a bigger burden, which in turn may lead to elevated levels of stress and couple relationship dissatisfaction. Health professionals are in a good position to encourage the family to investigate possibilities and obstacles for a more equal distribution of family life labor where this is considered appropriate.
Our findings offers examples of the previously documented link between life stressors and family wellbeing (Buyukcan-Tetik et al., 2016; Carlson et al., 2011; Kulik & Liberman, 2022). Considering that couple relationship quality has been found to be affected when parenting a child with a disability, more studies of the nature of this influence is needed. Future studies should aim to directly investigate perceptions of couple relationship in the context of parenting a child with a disability. To protect families where a child has a disability, knowledge about specific risk factors for couple relationship dissatisfaction in these families is essential.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Norwegian Women’s Public Health Association under Grant number 40404.
Open Research Statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research are not available. Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available. Further, interview data are in Norwegian, and of limited value for revision. The materials used in the research are available. Questions from the interview guide is provided in ![]() in the manuscript. The interview guide can be obtained by emailing:
in the manuscript. The interview guide can be obtained by emailing: