
Abstract
While meditation is commonly practiced by individuals on their own, several programmes have incorporated dyadic forms, too. However, the setting – meditating alone or in dyads – and its impact on the effects of meditation have not yet been examined. We expected that dyadic compassion meditation (CM) may improve perceived social closeness more compared to closely-matched individual CM. N = 50 couples were randomly assigned to do a brief 15-min CM induction either together with their partner or individually. Social closeness was rated by both partners. Secondary outcomes were positive and negative affect as well as parasympathetic response, indicated by heart rate variability (HRV). Due to the dyadic data structure, multilevel models were tested. We found no difference between dyadic and individual CM in self-report. After both forms social closeness and positive affect were improved, while negative affect decreased. Only HRV differed between the two conditions over time: while HRV significantly decreased in the individual condition, there was no such change in the dyadic condition. The accompanying physiological profile suggests that CM may involve effort at least in the individual CM. Done individually or with a partner, brief CM can foster social closeness and improve affect and can be employed to improve socio-emotional well-being.
Keywords
Introduction
Belonging to close and meaningful relations is regarded as a fundamental human need and as essential for our health, mental wellbeing and survival (Holt-Lunstad et al., 2010). Since our wellbeing is closely linked to both, social closeness and affect regulation (Lukas et al., 2018), finding effective ways to foster them is imperative. Both mindfulness- and kindness-based meditations have been regarded as an effective method to achieve this. While most meditations are practiced solitarily, dyadic forms (e.g. dyadic compassion meditation (CM), contemplative dialogues and eye-gazing exercises) have been integrated in various programmes. Although dyadic forms might be particularly suited to improve social closeness, they have hardly been investigated (Kok & Singer, 2017). Thus, this study is motivated by the question whether the setting – alone or in dyads – has an impact on the extent to which social closeness, affect and the parasympathetic response can be enhanced through a CM.
Compassion
Compassion has been described as an affective state that is evoked through witnessing others’ suffering and that motivates a wish to help (Goetz et al., 2010). Gilbert (2019) emphasizes that compassion requires attuning to personal or others’ suffering before taking steps to alleviate it – which is relevant to our operationalization including a negative mood induction (see methods). This notion of compassion also underlies the tripartite affect regulation system model (Gilbert, 2014), which is derived from a neuroscientific and evolutionary perspective (i.a. Depue & Morrone-Strupinsky, 2005). In short, it differentiates three systems: (1) the drive system, linked to activating positive affect; (2) the threat system, for protection against threats through negative affect like anger, disgust or anxiety and (3) the soothing and contentment system, associated with calm positive affect and feelings of care, safety, and being connected to others, known as social safeness (Gilbert, 2014; Gilbert et al., 2008). Showing compassion through attention, care or support stimulates the soothing and contentment system, which down-regulates the other two systems and leads to a greater balance. The physiological underpinnings of this model are rooted in the Polyvagal perspective (Porges, 2007; for a critical evaluation see Grossman & Taylor, 2007). Briefly, it posits that physiological states and social processes are connected: Vagal pathways can increase parasympathetic activation, which facilitates calm soothing. In turn, this can facilitate feelings of social connectedness, positive engagement and feelings of compassion. Heart rate variability (HRV), i.e. the beat-to-beat variation in the heart rate, mirrors parasympathetic activity and its assessment is important in compassion research (Kirby et al., 2017). Higher HRV mirrors higher parasympathetic activity or cardiac vagal tone (Kirby et al., 2017; Laborde et al., 2017), while HRV is reduced when the sympathetic nervous system is activated, e.g. for general activation or defence (Kim et al., 2020).
Evidence from kindness-based Interventions
Evidence from individual settings on social closeness, affect and heart rate variability
Compassion can naturally arise or be evoked in CM. Similarly, kindness can be practiced in loving-kindness meditation (LKM; Galante et al., 2014). In application and research, CM and LKM are often intertwined (Kirby, 2017). While LKM focuses on a loving and kind attitude towards all beings, CM focuses on the alleviation of suffering (Brito, 2014). Both forms have their origins in Buddhist traditions and are regarded as ways to feel connected and to experience positive and less negative affect (Brito, 2014; Galante et al., 2014). While cross-sectional studies have linked compassion to positive relationship aspects (e.g. Neff & Pommier, 2013) and longitudinal meditation training studies have shown positive effects of CM and LKM, for example decreases in loneliness (Mascaro et al., 2018) or increases in social closeness (Kok et al., 2013), limited literature exists on brief CMs alone. Therefore, evidence from LKMs is also taken into account.
Regarding social closeness, Hutcherson et al. (2008) compared a brief LKM imagination to an affect-neutral imagination control. Both resulted in increased positivity and connectedness towards a person on a photo with a stronger effect for the LKM. Noteworthy, no significant changes of more positive responding toward the self or a close other were observed. Concerning affect, the brief LKM led to significantly greater positive mood compared to control. A second study, which included another positive affect condition replicated the outlined findings (Seppala et al., 2014) and found that only LKM significantly increased other-focused positive affect, while all three conditions (LKM, positive affect, neutral) showed a decrease in negative mood. A more recent study compared a brief loving-kindness and an interconnectedness condition to an affect-neutral control and found increased feelings of connectedness and caring for the first two (Gentile et al., 2019).
Focusing more on brief compassion inductions, one early study found that compassionate imagery (compared to relaxation or control imagery task) led to increased HRV, however to a decline for those with less perceived social safeness, higher self-criticism or attachment-related anxiety (Rockliff et al., 2008). Petrocchi et al. (2017) found compassionate self-talk to increase soothing positive affect and HRV, with higher levels when this was done in front of a mirror, a condition which was linked to social signs, such as a facial expression, warm voice tone, arguing that soothing affect and higher HRV benefit from such signals of social connectedness. Recently, Kirschner et al. (2019) presented evidence by experimentally testing conditions closely mapped on the tripartite model (two self-compassion conditions = soothing system, negative rumination condition = threat system, a positive excitement condition = drive system, and a neutral control). Results have shown increased parasympathetic activation, indexed by HRV, in the self-compassion conditions, while this was not the case, or even the opposite, for the other conditions.
Further studies incorporating brief compassion inductions have shown that greater vagal activity is more specifically associated with state feelings of compassion when encountering others’ suffering rather than with general positive affect (Stellar et al., 2015). Related to this, Duarte and Pinto-Gouveia (2017) found that only safeness and contentment-related positive affect was related to vagal activity. Di Bello et al. (2020) described in their meta-analysis a significant positive association of compassion and HRV (g = .54) and concluded that indices such as HRV are representative of the degree of feeling safe and connected in social environments, facilitating compassionate orientations. Hence, they conclude it is less likely to feel compassionate in conditions of low HRV, which points to reduced perceived safety.
Evidence from dyadic settings on social closeness, affect and heart rate variability
Focussing more on the interpersonal setting, Kok and Singer (2017) investigated dyadic exercises as an element on its own in the ReSource Project (Bornemann & Singer, 2013). The 9-month longitudinal study investigated three 3-month modules: a Presence module (mindfulness), an Affect module (compassion-based), and a Perspective module (socio-cognitive). In the latter two, dyadic exercises were daily practices. The affect dyad was a 10-min contemplative conversation with a partner, in which both partners disclosed their feelings/thoughts in a structured interaction (in person and online) while promoting an attentive focus without responding (non-)verbally. For the perspective module, a similar dyadic exercise focused more on socio-cognitive aspects. Kok and Singer (2017) found that social closeness increased during one session of the affect dyads as well as over the timespan of 3 months; this increase was stronger than for perspective dyads in one of three cohorts. While they only compared these two forms of dyadic practices for social closeness, for affect, they actually compared dyadic versus content-matched individual LKM. They found that both forms, affect dyads and LKM, evoked comparable changes in affect, but that affect dyads were experienced as more affectively positive than LKM. Authors concluded “that intersubjective abilities and social cognition could be more easily cultivated in real contact with other people than through imaginary encounters, as common in single meditation practices” (Bornemann & Singer, 2013, p. 453). A recent study on empathy (Järvelä et al., 2019) supports this impression. Participants (pairs, not couples) generated compassionate feelings towards a non-active avatar (solitary condition) or to an active avatar representing their partner (dyadic condition) in virtual reality. Results indicate that it is significantly easier to evoke empathy in the dyadic condition.
As research has just started to integrate the dyadic setting with neurophysiological markers (e.g. Järvelä et al., 2019), studies on HRV within the dyadic setting are limited. However, one study assessed heart rate during couple conversation on losses and the naturally occurring compassion (Corner et al., 2018). Results showed that higher compassion of the listener was associated with a lower heart rate of the listener. For those with an avoidant attachment orientation, higher compassion was associated with higher average heart rate. Additionally, this study found that heart rate increased over the course of the discussion.
Better together than alone? – the current study
Having outlined a wide range of evidence, we expect brief kindness-based interventions, such as CM to be efficacious in increasing social closeness, improving affect and increasing HRV, while first studies point to the value of dyads. Besides these findings, further considerations strengthen the expectation that dyads could even improve the effect of CM through the interpersonal setting. First, compassion is generally understood to flow in three directions: to others, received from others, to ourselves (Gilbert, 2014). Dyadic CM combines these foci so that a meditator directs and receives compassion at the same time. Secondly, a dyadic CM that allows for eye contact and perceiving one another could strengthen the perception of responsiveness, which is linked to closeness (Reis & Clark, 2013) and to feeling cared for, even for non-verbal responsiveness (Kane et al., 2012). This way, a dyadic CM might be a specific setting that creates social safeness and this way activates emotions (social closeness, positive soothing affect) and physiological patterns connected to the soothing and contentment system beyond the effects of the individual form. Against this background of empirical findings and theoretical considerations, we expected that dyadic CM induction would lead to a stronger increase in social closeness from before to post meditation compared to the individual CM (H1). Second, we expected that dyadic CM would lead to a stronger increase in positive affect (H2) and a stronger decrease in negative affect (H3) from before to post meditation compared to individual CM. Dyadic CM should result in a stronger parasympathetic response (higher HRV) compared to individual CM during the meditation compared to before (H4).
Method
Sample characteristics
Sample characteristics.
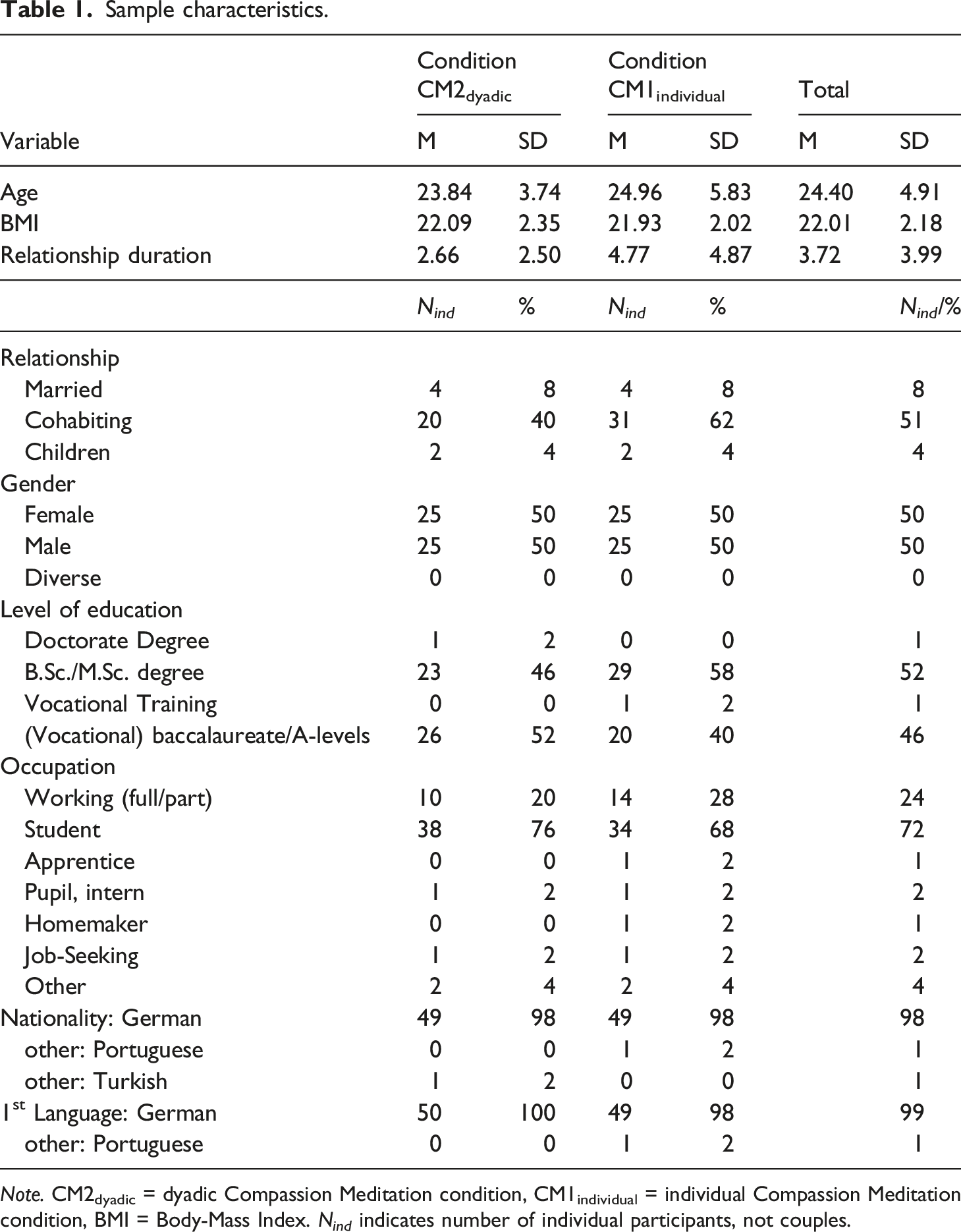
Note. CM2dyadic = dyadic Compassion Meditation condition, CM1individual = individual Compassion Meditation condition, BMI = Body-Mass Index. N ind indicates number of individual participants, not couples.
Procedures
Participants were recruited through flyers/posters containing information on a “Study on relationship and meditation” as a cover story without information about the investigated different modes of CM. They were recruited in Mannheim and Heidelberg, via social media and an online participation system of the University of Mannheim, and via mailing lists. A total of N = 79 couples responded to the study announcement and N = 50 couples participated. A flow chart can be found in supplementary materials B. Data were collected over a 7-week period (03-05/2019) in Mannheim and Heidelberg. All participants received 10€ (optional course credit (1.25hrs) for psychology students). CM audio files, analyses of self-reports and a 1-month licence for the app 7Mind were offered.
Multilevel modelling accounted for dyadic data structure. Calculating the number of participants needed for multilevel models (MLMs) requires simulation models that depend on a priori plausible values for intra-class correlations (ICCs), which were not available for this emerging field. For dyadic research, Du and Wang (2016) have shown that MLMs need 50 dyads for valid and reliable analyses, high convergence rates and lower bias of estimates, when there are no missing data for one partner (i.e., singletons) together with ICCs as low as .1. However, this does not guarantee power to be high enough for statistical inferences.
Research design and procedure
After expression of interest, couples received an e-mail on eligibility criteria and necessities for HRV assessment (following recommendations: Laborde et al., 2017). When partners gave written informed consent, the couple was randomized to either individual CM condition (CM1individual) or dyadic CM condition (CM2dyadic), using block-randomisation (computer-generated with fixed block sizes of 10). A pseudonymized code was generated by participants to match partners. First, participants answered questionnaires on demographic information and trait variables (t0) on tablets/computers via SoSci Survey (Leiner, 2019). A 10-min baseline HRV assessment followed in a standardized manner (Laborde et al., 2017). A negative mood induction procedure (MIP) followed for both conditions. Participants in the CM1individual then did an individual CM, while participants in the CM2dyadic did a dyadic form. Self-reported outcome variables were assessed before (t1) and after (t2) the negative MIP and after the CM (t3). Task adherence was assessed twice, after the negative MIP (t2) and following the CM (t3).The procedure lasted up to 1.25 hr. See Figure 1 for the detailed procedure and points of measurement. Procedure and measurement time points. Note. The procedure of the laboratory session for the individual Compassion Meditation condition (CM1individual) and dyadic Compassion Meditation condition (CM2dyadic) and the duration of the various elements are depicted. For heart rate variability (HRV) analyses intervals 1 to 4 were defined.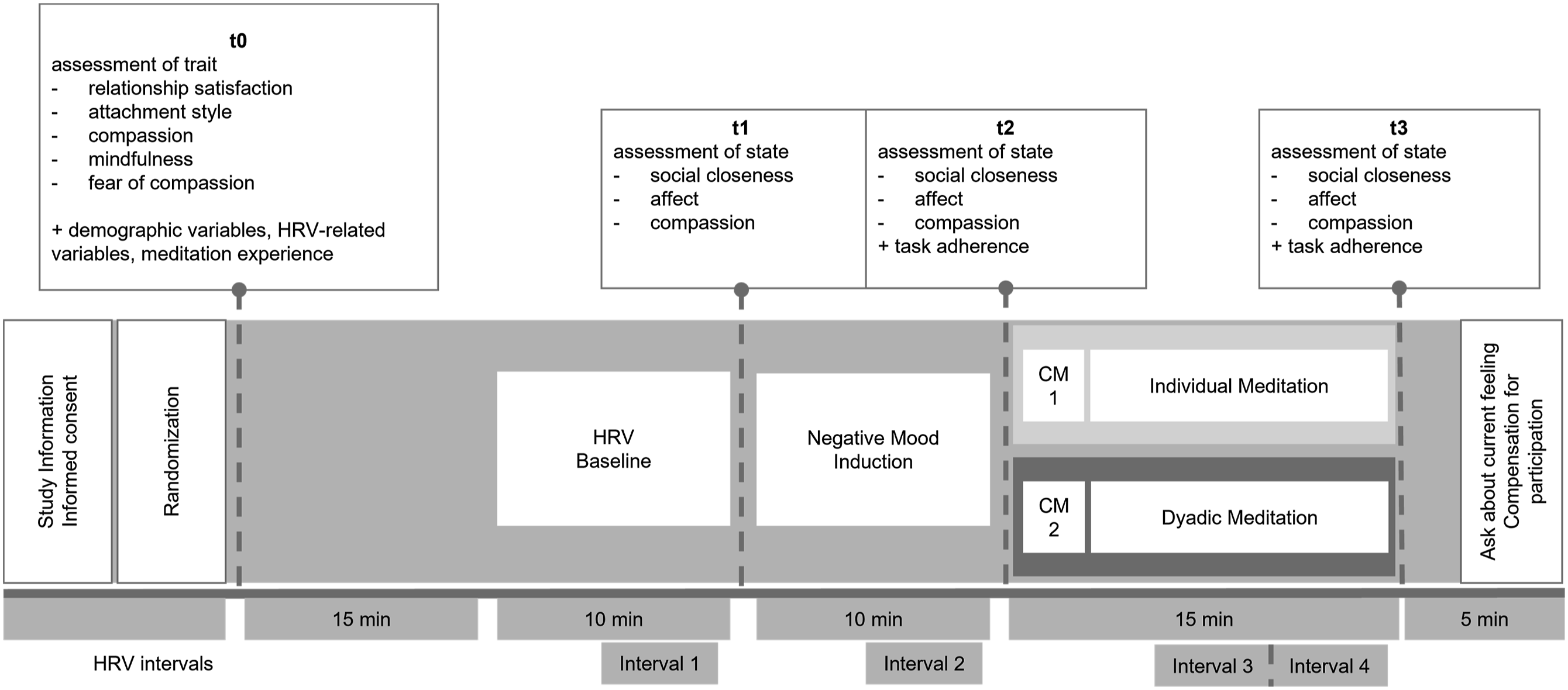
Negative mood induction procedure
The purpose of a negative MIP before the CM induction was derived from the theoretical conceptualisation of compassion: an affective state evoked in the face of one’s own or another’s suffering. By using a negative MIP suffering was induced in both partners, that could evoke compassion in the counterpart. Sadness could be such a compassion evoking state of suffering (Goetz et al., 2010) and thus its induction was supposed to build the basis for the following CM. The MIP consisted of autobiographical recall while listening to a mood-suggestive music piece via headphones. This combination was found to be effective for inducing temporary negative mood states (e.g. Kuehner et al., 2009). Participants noted down and dwelled for about seven minutes on a specific sad experience (having felt lonely, sad, humiliated, rejected). Afterwards partners were informed that their partner had done the same task to raise awareness for the other’s feelings. Intentionally, this experience should not involve the partner to exclude relationship-relevant partner distress as we expected this to be too difficult for beginners in CM.
Individual and dyadic compassion meditation
The CM lasted about 15 minutes in both conditions and was presented via headphones for both partners simultaneously. Instructions were based on the Cognitively-Based Compassion Training for couples (Aguilar-Raab et al., 2018). Participants in the CM1individual sat with a partition in between them, while meditating individually. For the CM2dyadic, this partition was removed before the CM so that participants could sit face-to-face without touching each other. The arrangement was as similar as possible and avoided effects of re-uniting partners from separate rooms. During CM2dyadic participants were asked to open their eyes for four times, to look at one another and to become aware of each other. There were no instructions on the own facial expression to allow for a natural response to the CM. In parallel, the CM1individual was instructed to imagine the partner. As intended, the two conditions differed only in the set-up of including non-verbal interactions in addition to the imaginative elements but not in the content or affective elements, resulting in a closely-matched experimental variation. The exact timeline of the meditation, exemplary instructions and the duration of the elements are depicted in supplementary material C.
Measures
Trait variables as potential control measures
We assessed potential variables that we regarded relevant to the operationalization of this study and those that have been shown to have an influence in compassion inductions, such as attachment orientation (e.g. Corner et al., 2018; Kirby et al., 2017).
Relationship satisfaction
To assess relationship satisfaction, one item of the German Version of the Relationship Assessment Scale (Dinkel & Balck, 2005) was used: “In general, how satisfied are you with your relationship?”. It was answered on a 5-point Likert scale (1 = not satisfied to 5 = very satisfied).
Meditation experience
Items from Bergomi et al. (2015) were used to cover a retrospective assessment and the current meditation practice, together with the type of meditation, typical duration, and frequency. In addition, openness towards and expectations regarding meditation were rated on 10-Point Likert Scales (e.g. 0 = I am not open towards meditation to 10 = … very open …/). Finally, practicing relaxation exercises or yoga was assessed.
Attachment orientation
Attachment orientation (attachment-related anxiety, attachment-related avoidance) was assessed using the short version of the Experiences in Close Relationships Revised questionnaire (Ehrenthal et al., 2021). Items are rated on a 7-Point Likert Scale (1 = strongly disagree to 7 = strongly agree). Cronbach’s alpha was αanx = .68 (anxiety subscale) and αavo = .61 (avoidance subscale) in this sample.
Compassionate love scale
The extent of trait-levels of compassionate feelings towards their partner was assessed via the Compassionate Love Scale, specific close other version (Sprecher & Fehr, 2005). The scale was translated into German (Aguilar-Raab et al., 2018; validation in preparation). Twenty-one items are rated on a 7-Point Likert Scale (1 = not at all true to 7 = very true) and a mean score was computed. Cronbach’s alpha for the CLS was αCLS = .88 in this sample.
Mindfulness
Levels of mindfulness were assessed using the German Version of the Comprehensive Inventory of Mindfulness Experiences (CHIME, see Bergomi et al., 2015). Of eight subscales those four subscales (18 items) that were regarded essential for the CM induction were used: inner awareness, outer awareness, acting with awareness, acceptance. These were answered on a 6-Point Likert Scale (1 = almost never to 6 = almost always). Cronbach’s alpha was αCHIME = .78.
Fear of Compassion
The Fear of Compassion Scale (FOC, Gilbert et al., 2011) was used. While the items used were derived from a forward-backward translation done by Krieger et al. (in preparation), a German version has recently been validated and published by Biermann et al. (2021). The 38 items are rated on a 5-Point Likert Scale (0 = strongly disagree to 4 = strongly agree). A sum score for each subscale was computed. Cronbach’s alpha for subscale (1) was αFOC1 = .80, αFOC2 = .85 for subscale (2) and αFOC3 = .87 for subscale (3).
Manipulation check and task adherence
Compassion
Visual analogue scales (VAS) were used to indicate current feelings of compassion with a slider on dimensions from “not at all” (1) to “completely” (101).
Task adherence
For task adherence, participants indicated after the MIP (t2) and the CM (t3) how well they could engage in the task (10-Point Liker Scale, 0 = not at all to 10 = very well) and how often they were distracted during the task (0 = not at all to 10 = extremely often). Participants rated the vividness of imagined pictures (0 = no internal image to 10 = absolutely clear and vivid internal image). These aspects were aggregated to a mean score after inverting frequency of distraction. Cronbach’s alpha for task adherence at t2 was α = .74, respectively α = .67 at t3.
State variables
Social closeness
The Inclusion of the Other in the Self-Scale is a pictorial 1-Item scale, which correlates highly with other scales for relationship closeness (IOS, Gächter et al., 2015). Participants chose from non-overlapping to more overlapping circles the one that best mirrored current feelings of social closeness to their partner. The scale was coded from 1 (non-overlapping) to 7 (most overlapping).
Affect
VASs were used to indicate current affect by responding to “Right now I feel… not at all – completely …” for three positive (calm/happy/loving) and three negative terms (angry/anxious/unhappy). For comparability, we selected terms used in previous studies, such as those employed by Hutcherson et al. (2008). Our aim was to assess soothing positive affect rather than activating positive affect. Similarly, Kirschner et al., 2019 used terms such as loved and safe, calm and sense of togetherness for positive affiliative affect. Responses were averaged to form a positive and a negative affect composite. Cronbach’s alpha ranged from αpos = .68/αneg = .61 to αpos = .85/αneg = .76 for the three points of measurement.
Heart rate variability
To assess HRV, a single-channel sensor, eMotion FarosTM 180° by Bittium, was used as a chest strap to collect RR intervals and electrocardiogram (ECG, sampling rate 1000 Hz) in European Data Format (EDF).
Statistical analyses
Analysis of self-report data
For descriptive analyses and data processing SPSS was used. Although from a conceptual perspective, the data mirror three levels (repeated measures within participants within couples), the measurement time-points were simultaneous for each partner, which results in time as a fully crossed factor within each dyad requiring two-level models (Kenny et al., 2006).
Therefore, two-level hierarchical models were fitted with dyads at level 2 and persons at level 1 using the R package lme4 (Bates et al., 2015). Random intercepts allowed for the estimation of variation at the individual participation and the couple level, respectively. No random slopes were included given the group size of two units per couple. Restricted Maximum Likelihood estimation method was used due to small sample size. Fixed effects were included for condition (CM1individual = 0, CM2dyadic = 1) and time (as a factor variable) and their interaction term. To obtain ICCs, as the proportion of a variable’s total variance accounted for by group membership (i.e. level-2 units: couples), intercept-only models were specified for each outcome. For manipulation checks, the ICCs for the couple level were all ICC < .1. For hypothesis testing, the ICC for social closeness amounted to .08. Generally, the amounts of dependence were small in this sample. For affect from t2 to t3 and for all HRV indices, the MLMs indicated variance at the couple level to be (very close to) zero. When this was the case, the random intercept for the dyad was removed from the model.
As extensive meditation experience may affect findings, previous studies have excluded participants who practice >30 minutes per day. This did not apply to anyone in the sample. Due to this and due to problems resulting from singletons, i.e., when one partner would be excluded, no subgroup analyses were conducted.
Control variables (see methods) were grand-mean centered and included in the intercept-only model for each outcome variable. For reasons of parsimony, only those that had a significant association with the outcome were kept in the final model and thus differ for the respective outcome. Outcome self-report variables were not transformed. All models were visually checked for equality of variance of the residuals and for normality, indicating that MLMs can be adequately specified. For self-report data, there were no missing data. For all analyses, p values < .05 were considered statistically significant.
Analysis of heart rate variability data
For HRV, parameters were determined from the raw ECG in Kubios HRV Premium using the automatic QRS detection algorithm and artefact correction algorithm (Tarvainen et al., 2019). After visual inspection for erroneous signal and boxplots for extreme values, data for HRV analyses consisted of n = 49 couples with n ind = 93 individuals.
As recommended (Laborde et al., 2017), 5-min intervals were defined excluding times of beginning/ending a task, resulting in four 5-min intervals with two separate intervals from the meditation period. Interval 1 represents baseline assessment, interval 2 the negative MIP and interval 3 and 4 are part of the CM. Mean values for indices were extracted for each interval. The square root of the mean squared differences between successive RR intervals (RMSSD in ms) has among other indices a theoretical underpinning for reflecting vagal tone (Laborde et al., 2017) and was taken into account. For additionally extracted indices (pNN50 in %, and high frequency indices) the respective MLMs can be found in supplementary materials G.
Multilevel models fitted for the comparison of HRV as outcome variable included data from interval 1 and 2 for to the manipulation check and interval 2 and interval 3 for hypothesis testing. Exploratively, additional MLMs were fitted for the comparison from interval 2 to interval 4 with regard to the longer duration of the meditation.
Results
Descriptive analyses
For the primary outcome, social closeness, mean values at t1 and t2 ranged from 4.24 to 4.78, indicating relatively high levels on the IOS-scale (1 to 7): 29% of participants already reported 6 or 7 both before and after the MIP, leaving little room to indicate possible changes after the CM. (See supplementary material E for tables on self-reported variable’s mean values, standard deviations, correlations and supplementary materials D for HRV indices and correlations.)
Manipulation checks and task adherence
During the negative MIP, the vast majority (78%) mentioned at least sadness as the accompanying feeling. MLMs revealed that the negative MIP worked in the intended direction on the self-report variables, i.e., a significant increase of negative and a significant decrease of positive affect. The negative MIP was expected to result in negative affect, which would be mirrored in decreased vagal tone. MLMs were specified to test this. RMSSD values point to a significantly increased vagal tone from baseline to the MIP, which is in contrast to what would be expected for a negative MIP.
For both conditions, an increase in compassion from t2 to t3 was expected. The respective MLM revealed that compassion increased slightly and not significantly during the negative MIP, but increased significantly during the CM, independent of condition. Task adherence did not differ between conditions, t(98) = −1.10, p = .276, Cohen’s d = .219. See supplementary materials F for full manipulation check MLMs.
Outcomes
Changes in social closeness
Results of multilevel models for hypothesis testing of the effect of the respective meditation on Social Closeness, Positive, and Negative Affect.
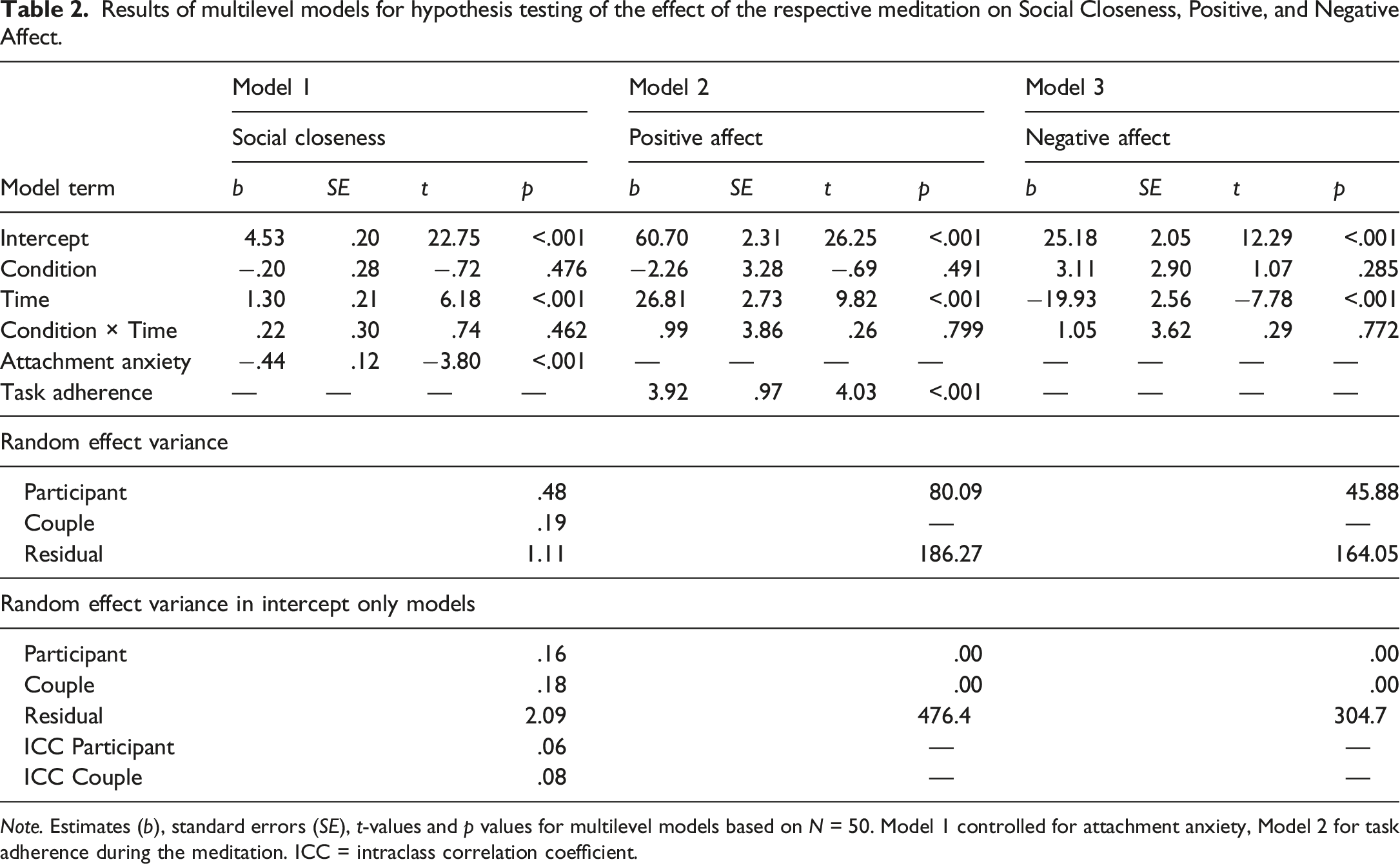
Note. Estimates (b), standard errors (SE), t-values and p values for multilevel models based on N = 50. Model 1 controlled for attachment anxiety, Model 2 for task adherence during the meditation. ICC = intraclass correlation coefficient.
Changes in affect
For both affect composites, the MLMs did not include a couple level random intercept because couple level variation was estimated to be zero. For positive affect, the MLM, controlling for task adherence during meditation, yielded a similar pattern as for H1: A significant positive main effect of time on positive affect, b = 26.81, SE = 2.73, p < .001, denoting the mean difference of positive affect in the CM1individual from t2 to t3. This main effect was not qualified by an interaction, b = .99, SE = 3.86, p = .799, suggesting no significantly different effect of time on positive affect depending on condition. For negative affect, the main effect of time was significantly negative, b = −19.93, SE = 2.56, p < .001, denoting the mean difference of negative affect in the CM1individual from t2 to t3. This suggests a decrease of negative affect from before to post meditation, which again was not further qualified by an interaction, b = 1.05, SE = 3.62, p = .772. H2 and H3 have to be rejected.
Changes in heart rate variability
In a first step, MLMs were specified to test whether the dyadic CM led to a stronger increase in HRV compared to the individual CM from during the negative MIP (interval 2) to during the meditation (interval 3). The respective MLMs did not include the couple level random intercept due to variance estimates being (very close to) zero. A MLM that tested the effect of time, condition, and their interaction term on RMSSD yielded a significant negative main effect of time, b = −5.50, SE = 1.58, p = .001, denoting the mean difference of RMSSD in the CM1individual from interval 2 to 3. Other than in previous models, this effect was qualified by the significant interaction term time
Exploratively, the same models as above were calculated for the comparison from during the negative MIP (interval 2) to the final stage of the meditation (interval 4) to see whether trends in HRV changed throughout the duration of meditation. This indicated a significant negative main effect of time on RMSSD, b = −6.95, SE = 1.76, p < .001, denoting the mean difference of RMSSD in the CM1individual from interval 2 to 4. This main effect was qualified by a significant time
Discussion
This study tested whether a dyadic CM improved social closeness, affect and parasympathetic activity beyond the effects of individual CM in an experimental design. Results indicate that even a brief CM induction was sufficient to significantly increase social closeness towards a close other, to improve positive affect, and to decrease negative affect. These effects were independent of the dyadic or individual condition. Results concerning HRV during the CM indicate a significant reduction in the individual CM and no significant change in the dyadic CM. As we hypothesized that the dyadic CM would outperform the individual form, our four hypotheses were not supported. As we did not test for equivalence of the settings, we cannot conclude, whether the two settings of CM were comparably effective in increasing social closeness towards a close other, positive affect, and decreasing negative affect. Results of this study add to the existing literature with new findings, indicating that the setting of the meditation may not make a difference. Evaluating the results of this study requires considering the chosen experimental approach, which will be discussed in different aspects.
Negative mood induction procedure
Although the negative MIP did significantly increase negative affect, as intended, and significantly decrease positive affect, the latter was still higher than negative affect. That positive affect remained high might also be reflected in the HRV pattern: From baseline to the negative MIP, HRV significantly increased, though marginally for two indices. Therefore, it could be that a negative MIP, focusing on sadness, was not as reliable as self-criticism (Kirschner et al., 2019) in activating negative affect and the accompanying physiological pattern of decreased HRV. Some participants mentioned that they perceived the music rather calming. On the contrary, one participant commented that he was hardly able to follow the CM due to intense sadness. Other participants might have had similar experiences but did not report them. Finally, it cannot be ruled out that participants have, intuitively or intentionally, employed meditative or breathing techniques during the MIP. Then, comparisons to the CM would be misleading.
Social closeness
Results suggest that the dyadic CM did not differ from the individual CM in increasing social closeness. Contrarily to our hypothesis, there were no extra benefits of the dyadic setting in this experimental procedure. For the individual CM, this study replicated outlined findings, altogether suggesting that even brief sessions of CM or LKM can lead to increased connectedness. Different to a study by Hutcherson et al., (2008), this study has shown that social closeness could be significantly intensified also for a close other (partner) and even in a sample with high average closeness.
For the dyadic CM, the increase of social closeness is in line with Kok and Singer’s (2017) finding so-called ‘loud’ dyadic meditations. Therefore, this is the first study to show, that also silent dyadic meditations can elicit feelings of connectedness. Contrary to the hypothesis, the dyadic CM was not more advantageous in improving social closeness than the individual CM. Although we expected that the real social encounter would consist of stimuli to create feelings of social safeness and connectedness as described in the tripartite model, the imaginative form came with a possible advantage. Through participants’ feedback, it was revealed that in internal images during the CM individuals may imagine the partner as a loving/resonant partner, while in a real encounter they were confronted with the other person as they presented themselves. This could involve sad/neutral or even dismissive facial expressions rather than signs of social safeness. Some couples mentioned to the experimenter that they had to cry or laugh during interactions. Such states could arise for various reasons such as feeling overwhelmed with the task as a beginner. Being intensely focused by one’s partner in the dyadic CM may also create interactions different from regular experiences (e.g. demanding eye-contact). This can of course create variation other than in studies that employ virtual reality avatars with neutral faces (Järvelä et al., 2019). However, Risko et al. (2016) highlighted that investigating social interactions might need a shift from high stimulus control to live settings in order to draw conclusions beyond the laboratory.
Further on, various studies have found that simply imagining a close other, as it was done in the individual CM, can be a powerful tool. Poerio et al. (2015) found that daydreaming about a close other was associated with increases in love, connection and happiness. Although CM is regarded as distinct from daydreaming, the pattern of results resembles the effects of the individual CM, here, but do not lend further explanation for why the dyadic CM was not more advantageous. Following their line of argument (Poerio et al., 2015), dyadic CM can be a good option, when the close other is available, but that the individual form can be practiced on one’s own without different effects.
Affect
Concerning affect, it was found that positive affect significantly increased from after the negative MIP to post meditation, while negative affect decreased, with no difference between conditions. This was again contrary to the expectation that the dyadic CM would be more beneficial. From a theoretical perspective, the tripartite affect regulation system model suggests that compassion is able to stimulate the contentment and soothing system. The manipulation check found that levels of compassion did not differ between conditions, which might have led to the activation of the soothing system and could explain the effect on affect in both groups.
For the individual condition, findings are again in line with outlined findings on brief LKMs and CMs. For dyads, Kok and Singer (2017) found that dyadic and individual meditation led to comparable changes in affect, but that the dyads were experienced as more affectively positive than individual LKM. This study suggests that both forms did not differ in improving affect. Kok and Singer (2017) suggested for contemplative dialogues, that an intrinsically rewarding effect of self-disclosure can also play a role (Tamir & Mitchell, 2012). This might have resulted in the found superiority of the dyads, but was not part of this silent dyadic CM. This could be a mechanism to intensify the effect of dyads. Expanding the literature to discuss our results, we drew upon insights from research on eye-gazing, which was a distinguishing element of the two conditions. Hietanen (2018) reviewed evidence that eye contact evokes positive affective reactions. Our data, however, suggest that the dyadic CM with eye-gazing did not surpass the positive affective improvement observed in the individual form.
Heart rate variability
To our knowledge, this is the first study that investigated HRV as a physiological correlate for compassion and parasympathetic activation together with interpersonal meditation in a real encounter. With regard to HRV, results suggest partially differential physiological profiles in the CM1individual and CM2dyadic throughout the CM. They seem to indicate a certain superiority of the dyadic form as no significant decrease of HRV was observed. However, findings are not supporting Hypothesis 4 as an increase in both forms, and a stronger one for the dyadic form was expected. It is crucial to interpret this with caution since HRV increased unexpectedly during the negative MIP before the CM.
The significant decrease of HRV during the individual CM is contrary to what was expected based on theory and to many findings of CM to result in parasympathetic activation (Kirby et al., 2017). However, taking into account evidence from LKM, it is in line with one study that found LKM to result in decreased HRV and higher subjective effort (Lumma et al., 2015), suggesting that also this brief CM induction might have required effort. For the middle part of the meditation, it is conceivable that the dyad context might have buffered this negative effect on HRV in that sense that at least partners had to do it together, resulting in the non-significant positive trend in (three of four indices of) HRV.
For the final stage of the meditation, exploratory analyses revealed that HRV significantly decreased in the CM1individual, while the CM2dyadic also showed a non-significant negative trend. In line with this, Corner et al. (2018) found that heart rate, not HRV, increased over the course of a loss discussion, suggesting that offering compassionate support again can be physiologically demanding over time. Future research could clarify effects on physiology by asking participants how they experienced the form of meditation in terms of effort.
A more recent study illuminates an aspect that may have been overlooked in our study and in early stages of compassion research and its physiological indicators. In essence, Di Bello et al. (2021) emphasize the need to consider both facets: the sensitivity to or resonance with suffering and the desire to help alleviate it. Based on a small sample, their results indicate lower HRV linked to a sensitivity to suffering, while perceiving action to reduce suffering led to increased HRV. Although they did not investigate CM itself, their perspective enables a possible conclusion: the HRV result pattern in the individual CM may reflect heightened sensitivity to emotional suffering, which could have been less intense in the dyadic form. However, this is not supported by the reported affect after the CM. An important learning from this is the need for a clear operationalization of these two aspects of compassion in future research. Although we have thoroughly integrated HRV with RMSSD as a specific indicator of vagal tone (Laborde et al., 2017), it is essential to acknowledge that capturing vagal tone and emotion regulation via HRV is complex (Di Bello et al., 2021; Kirby et al., 2017) and a multimethod assessment of should be considered in future research.
Limitations and strengths
This study does not come without limitations. Firstly, the MLMs were ‘defensible’ models as the most appropriate solution, given the data. With a larger sample two-intercept two-level growth curve models would be optimal. Secondly, this study built a starting point employing two conditions. However, without further control conditions one cannot conclude whether the CM itself or sitting together in the same room over time without a CM would have similar results. Employing a partition might have prevented effects of re-uniting participants in the dyadic condition but might have also resulted in feeling the partner’s presence in the same room in the individual condition beyond the effect of imagination. Third, this sample consisted not only of predominantly young, highly educated couples, they were also interested in a study on “meditation and relationship”, resulting in selection effects that limits generalizability. To better understand the sample composition, we should have included additional demographic variables, specifically, ethnicity, sexual orientation and disability information as well as a clear differentiation in assessing gender identity and sex.
Limitations notwithstanding, this study employed a well-planned experimental randomized control design. The CM1individual was a closely-matched condition: aspects such as relaxation, mental imagery, duration and wording were very similar. Only the element of dyadic interaction was varied, as intended. Another strength was the inclusion of a negative MIP before the CM to generate feelings of suffering to facilitate compassion. However, as outlined above, a sad negative MIP might not have been the best choice. Among the few studies that investigated HRV during CM, this study is the first to do so for dyadic CM, implementing the current recommendations for HRV assessment in compassion research (Kirby et al., 2017; Laborde et al., 2017).
Implications and future research
Our findings inform the development of mindfulness- and compassion-based and couple interventions. Future research should examine the transfer of the effects of the induction from the lab to real life (Kuehner et al., 2017). For example, one could consider potential long-term effects of regularly practiced individual or dyadic CM in daily life on the behavioural expression of compassionate acts. These have been found to be beneficial for caring interaction of couples (Reis et al., 2014). While our study regarded effects for each individual, it would be especially interesting to analyse effects of emotional contagion or co-regulation over time. This has been investigated for mindfulness meditation (May et al., 2020), finding that negative affect decreased for a non-meditating partner during weeks, when one partner meditated for 15 minutes per day. As findings with regard to physiological synchrony (Järvelä et al., 2019) or linkage (Timmons et al., 2015) are mixed (as outlined in Corner et al., 2018), future studies could use a similar approach as we did to clarify possible beneficial patterns. Besides this interplay between partners, the interplay of assessed outcomes is of interest. Literature suggests for instance, that effects of LKM on vagal tone were mediated by changes in positive emotions, which also predicted perceptions of social closeness (Kok et al., 2013). Such an interplay might be especially pronounced in interpersonal meditation.
Conclusion
This study provides first evidence that dyadic forms of a brief CM induction do not outperform individual CM in fostering social closeness and improving affect.
Supplemental Material
Supplemental Material - Better together than alone? Investigating dyadic compassion meditation in an experimental study
Supplemental Material for Better together than alone? Investigating dyadic compassion meditation in an experimental study by Leonie Schültke, Marco Warth, Georg W. Alpers, Beate Ditzen, and Corina Aguilar-Raab in Journal of Social and Personal Relationships.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a funding from the Steffen Lohrer Foundation for Holistic Medicine and the 7Mind GmbH supported this research. Both had no role in design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review, or approval of the manuscript. The Center for Psychosocial Medicine supported this study financially with their means for master theses.
Ethical statement
Trial registration
This study was pre-registered in the German Clinical Trials Register (DRKS00016870).
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This study was pre-registered at the German Clinical Trials Register: DRKS00016870. The data used in the research are available. The data can be obtained by emailing:
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.