
Abstract
Both parental psychological well-being (e.g., depressive symptoms) and parental relationship functioning (e.g., negative communication) are common parental risk factors for dysfunctional parenting. The spillover process from these parental characteristics to dysfunctional parenting is assumed to be amplified by parental stress, which is particularly common among mothers and fathers of young children. However, few studies have examined dyadic spillover processes from parental risk factors and parental stress on parenting in early childhood. In the current study, we first examined direct actor and partner effects of parents’ depressive symptoms and negative communication at 10 months postpartum on dysfunctional parenting at 48 months postpartum in 168 primiparous mixed-gender couples. Second, we analyzed indirect effects via one’s own and the partner’s parental stress at 36 months postpartum using Actor-Partner Interdependence Mediation Models (APIMeM). We found direct actor effects for mothers’ depressive symptoms and negative communication on their dysfunctional parenting. Additionally, indirect actor effects were found for depressive symptoms and negative communication among mothers and fathers. Specifically, mediating effects of depressive symptoms and negative communication on one’s dysfunctional parenting through one’s parental stress were found. There were no indirect partner effects through parental stress. These findings highlight the important role of parental stress in early childhood as a mediator between both individual and relationship parental risk factors and dysfunctional parenting. These results further underscore the importance of longitudinal dyadic analyses in providing early and tailored interventions for both mothers and fathers of young children.
Keywords
Positive and effective parenting, such as parental warmth and behavior control, contribute to positive child adjustment (Foster et al., 2022; Pinquart, 2017). In contrast, dysfunctional parenting (i.e., parenting behaviors that are harsh, overreactive, lax, or inconsistent) hinders child adjustment and increases the risk of mental health problems in children (Anthony et al., 2005; Pinquart, 2017). Therefore, identifying factors that impair effective parenting may help to reduce dysfunctional parenting and to enable positive child development. In this study, we focused on parental risk factors that can deliberately be modified by parents (with or without professional support) and, as a result, may actively reduce dysfunctional parenting to promote their children’s adjustment.
The extent of dysfunctional parenting behavior in the family context is shaped by various family characteristics, as proposed by the process model of parenting (Belsky, 1984; Taraban & Shaw, 2018). Besides the characteristics of the child itself (e.g., temperament; Clark et al., 2000), the main parental predictors of parenting are parents’ individual characteristics (e.g., personality, depression, developmental history) and relationship characteristics (e.g., relationship quality, social support, family structure; Erel & Burman, 1995; Krishnakumar & Buehler, 2000; Lovejoy et al., 2000; Wilson & Durbin, 2010). Concerning parental characteristics, this study focused on depressive symptoms and negative communication due to their modifiability and because they are at risk of aggravation during the early period of parenting (Doss et al., 2009; Epifanio et al., 2015; Rauch-Anderegg et al., 2020; Vismara et al., 2016). Additionally, there is evidence of indirect effects between parental risk factors and parenting. One potential indirect effect has been found via parental stress (Durtschi et al., 2017; Le et al., 2017), which is likely experienced by parents of infants and toddlers and could further increase the likelihood of dysfunctional parenting (Deater-Deckard & Panneton, 2017).
Increasing risk factors in the early period of parenting
After the first child’s birth, parents experience increased mental health issues, such as depression and anxiety (Don et al., 2014; Mitchell et al., 2019). Particularly during this early period of parenting, approximately 20% of mothers and 10% of fathers report clinically relevant levels of depressive symptoms (Cameron et al., 2016; Epifanio et al., 2015; Vismara et al., 2016). Additionally, most parents not only experience a deterioration of psychological well-being across the transition to parenthood but also a substantial deterioration of relationship functioning (Doss et al., 2009), especially negative communication in conflict is known to increase after childbirth (Doss et al., 2009; Rauch-Anderegg et al., 2020). Finally, as family members are highly interdependent, emotional and behavioral patterns in the early years of parenting could spill over from one subsystem to another (Erel & Burman, 1995). In other words, negative or positive emotions and behaviors occurring in one subsystem (e.g., interparental conflict) could transfer to another (e.g., parent-child) and promote dysfunctional parenting behavior. Thus, reduced well-being (e.g., higher rates of depression or anxiety) and reduced relationship functioning (e.g., more conflicts and fewer positive interactions) are common risk factors for harsher and more disengaged parenting (Krishnakumar & Buehler, 2000; Ponnet et al., 2013; Van Eldik et al., 2019; Wilson & Durbin, 2010).
Depressive symptoms and parenting
Parental depressive symptoms, specifically maladaptive cognitions, affect, and behaviors, are associated with dysfunctional parenting behavior (Goodman, 2007). A meta-analysis of 46 studies using observational measures of parenting behavior showed a consistent positive correlation between maternal depression and harsh parenting as well as more disengaged parenting (Lovejoy et al., 2000). Among fathers, paternal depression has comparable deleterious effects on parenting as among mothers (Wilson & Durbin, 2010).
Results from longitudinal studies have documented the deleterious effects of parental depression on parenting after the transition to parenthood and in early childhood (e.g., Guyon-Harris et al., 2022; Le et al., 2017). For first-time mothers, higher depressive symptoms during pregnancy were associated with less warm responsiveness toward their child 4 months postpartum (Mitchell et al., 2019). Fathers’ depressive symptoms during pregnancy and 10 months postpartum were linked to more negative parenting among fathers (i.e., lower childcare involvement) with their 19 months old children, while this effect was not found among mothers (Fentz et al., 2023). Furthermore, women with more depressive symptoms showed more dysfunctional parenting with their 2- and 3-year-old children than women with fewer depressive symptoms (Guyon-Harris et al., 2022). However, no direct associations between depressive symptoms at 6 months postpartum and harsh parenting at 3 years postpartum for both mothers and fathers were found (Le et al., 2017). While depression can be conceived as an individual risk factor affecting early parenting and childcare behavior, relationship functioning can be considered an additional risk factor that increases dysfunctional parenting (Krishnakumar & Buehler, 2000; Taraban & Shaw, 2018).
Negative communication and parenting
Negative communication includes hostile communication behaviors (e.g., verbally or nonverbally expressed anger, yelling, undermining, belligerence, contempt) and disengaged communication (e.g., withdrawal, detachment; Gottman, 1994). These dimensions of negative communication have been found to predict various parenting behaviors in early childhood (Belsky, 1984; Cox & Paley, 2003; Krishnakumar & Buehler, 2000). For example, parental conflict (e.g., disagreement, arguing) among parents of preschool children (2–4 years) has been cross-sectionally associated with harsher discipline and lower parental involvement (e.g., playing with the child; Buehler & Gerard, 2002). In addition, over the course of 2 years, increases in negative communication between parents were positively related to later dysfunctional parenting in mixed-gender couples with 5–8 years old children for fathers but not for mothers (Davies et al., 2009). Furthermore, interparental hostility and withdrawal were linked to more parental emotional unavailability for their 7-year-old children over 1 year (Sturge-Apple et al., 2006).
Parental stress as a mediating link
Contextual factors, such as parental stress, might mediate the effects of parental risk factors on parenting. Parental stress is linked to reduced psychological well-being, reduced relationship functioning, and greater dysfunctional parenting (Berryhill et al., 2016; Cina & Bodenmann, 2009). This distinct type of stress arises because of a mismatch between the perceived demands of parenting and the resources available to meet those demands (Abidin, 1992; Deater-Deckard & Panneton, 2017). Because it originates outside the parents’ couple relationship, it is classified as an external stressor (Randall & Bodenmann, 2017). Numerous studies have found that higher levels of parental stress are associated with more dysfunctional parenting (Deater-Deckard & Panneton, 2017) such as stricter discipline (Anthony et al., 2005) and higher demandingness (Ponnet et al., 2013).
Parental stress is highly prevalent during early childhood (Crnic et al., 2005; Hildingsson & Thomas, 2014). Effective parenting of young children is challenging and prone to dysfunctional mechanisms (i.e., harsh parenting) due to the child’s intensive caregiving and nurturing needs, the handling of health and safety issues, and the changing nature of the parenting role (Anthony et al., 2005; Hildingsson & Thomas, 2014). Parents with fewer emotional and cognitive resources may be more likely to experience everyday stressors in childrearing, making parenting an even more demanding task (Crandall et al., 2015). Additionally, children are highly dependent on their caregivers during early childhood. Accordingly, associations between parenting and child development are particularly strong during early childhood compared to later developmental periods (Le et al., 2017; Van Eldik et al., 2019). Therefore, examining the interactions between parental risk factors and dysfunctional parenting may be particularly relevant in fostering child development. First-time parents may be especially prone to such dysfunctional mechanisms, and strong associations between individual characteristics, relationship characteristics, parental stress, and parenting may be present.
In early childhood, both individual (e.g., depressive symptoms) and relationship behaviors (e.g., negative communication) can amplify parental stress, thereby impairing effective parenting behavior through a spillover process (Erel & Burman, 1995). Studies have consistently shown links between parental depression and parental stress (Rollè et al., 2017; Thomason et al., 2014; Vismara et al., 2016). At 3 months postpartum, more depressive symptoms in mothers and fathers have been associated with higher levels of parental stress (Vismara et al., 2016). Parental stress has been also associated with both mothers’ and fathers’ dyadic adjustment (e.g., closeness, agreement, satisfaction) and lower mental health at 12 months postpartum (Rollè et al., 2017). Moreover, in a longitudinal study of primiparous mixed-gender couples, mothers’ and fathers’ depressive symptoms 10 months after birth were positively related to their parental stress 9 months later (Fentz et al., 2023). Mothers’ depressive symptoms positively predicted fathers’ later parental stress. Another longitudinal study found differential effects for various subscales of parental stress and postpartum depressive symptoms in women (Thomason et al., 2014). Unidirectional effects were found from overall parental stress to depressive symptoms over time (3, 7, and 14 months). Bidirectional associations were found between depressive symptoms and parental stress regarding parent-child interactions. These studies underscore that depressive symptoms are related to parental stress, even in non-clinical samples and in both genders.
Even though parental stress may be particularly deleterious during early childhood, it has only been analyzed in the context of depressive symptoms but not in the presence of relationship risk factors (e.g., negative communication). In a cross-sectional study of mothers and their infants, Fernandes et al. (2021) found that more depressive symptoms were indirectly associated with lower levels of mindful parenting mediated by greater parental stress. No direct associations were found and their study did not include fathers. In addition, a longitudinal study of mother-infant dyads found that lower maternal sensitivity was associated with higher parental stress and lower positive parenting (Dau et al., 2019). A longitudinal study examined parental stress as a mediator between negative affect and parenting in primiparous mixed-gender couples at 6, 12, and 36 months postpartum and found that negative affect after birth was positively associated with one's own and one's partner parental stress in fathers and mothers (Le et al., 2017). Similarly, parental stress mediated the association between harsh parenting and negative affect among mothers and fathers. Additionally, one’s parental stress mediated the link between the partner’s negative affect and one’s harsh parenting, establishing parental stress as an essential direct and indirect mechanism between parental negative affect and parenting in early childhood.
Family interdependence
Although both mothers and fathers with young children can be involved in childcare, the role of parental stress in early childhood has not been well studied in fathers (Taraban & Shaw, 2018; Van Eldik et al., 2019). Research on the role of fathers is still scarce, and dyadic approaches are even less frequent (Fernandes et al., 2021). However, from a family systems perspective (Cox & Paley, 2003; Minuchin, 1985), individuals within a family are not independent. Negative moods, affects, and behaviors are closely linked within families and are likely to spill over to other family members (Erel & Burman, 1995). For example, parental stress has been established as an interdependent phenomenon within couples (Randall & Bodenmann, 2017; Zemp et al., 2017), meaning that if one partner experiences high levels of parental stress, the other partner is also likely to experience parental stress. Especially in early childhood, parental stress may be highly interdependent, as couples generally have lower psychological resources to cope with stress individually (Epifanio et al., 2015) and as a couple (i.e., dyadic coping; Stadelmann et al., 2022). Thus, accounting for the interpersonal nature of the parenting process and its predictors within the family is essential and calls for appropriate methods that allow testing spillover processes and considering both parents within a dyadic framework (e.g., APIM; Kenny et al., 2006; Ledermann & Kenny, 2017). Consequently, this study examined multiple aspects of individual and relationship characteristics of both parents (i.e., depressive symptoms, negative communication) and the mediating role of parental stress on dysfunctional parenting in the early childhood period.
Purpose of the study
By addressing the interdependence within families and including multiple predictors, this study aims to enhance knowledge about the dyadic spillover process on parenting in mixed-gender couples after the birth of their first child. First, we applied an APIMeM framework (Kenny et al., 2006; Ledermann & Kenny, 2017) to examine the longitudinal direct actor and partner effects of parents’ depressive symptoms and negative communication within the couple relationship 10 months after birth on dysfunctional parenting at 48 months postpartum in first-time parents. Furthermore, we examined the indirect actor and partner effects of parental stress at 36 months postpartum as mediators within the link between parental risk factors (i.e., depressive symptoms and negative communication) and dysfunctional parenting.
First, we hypothesized that depressive symptoms (H1a) and negative communication (H2a) were positively associated with parental stress and dysfunctional parenting (see Figure 1). Second, we examined the potential mediating effect of parental stress in mothers and fathers, resulting in eight indirect paths per model. We expected longitudinal positive indirect actor effects of both parents’ depressive symptoms (H1b) and negative communication (H2b) on their dysfunctional parenting, mediated by parental stress. Finally, we explored whether there were partner effects and parental gender differences in these effects, without specifying any hypotheses. Conceptual Actor-Partner Interdependence Mediation Model (APIMeM) with depressive symptoms and negative communication as parental risk factors, and parental stress a mediating link on dysfunctional parenting. Note. a, b, c’ = a, b, and c’ paths from mediation analysis notation; f = women; m = men; A = actor effect; P = partner effect; e = residual error. For ease of presentation, covariances between women and men, and control variables are not depicted. Models were computed separately for each predictor.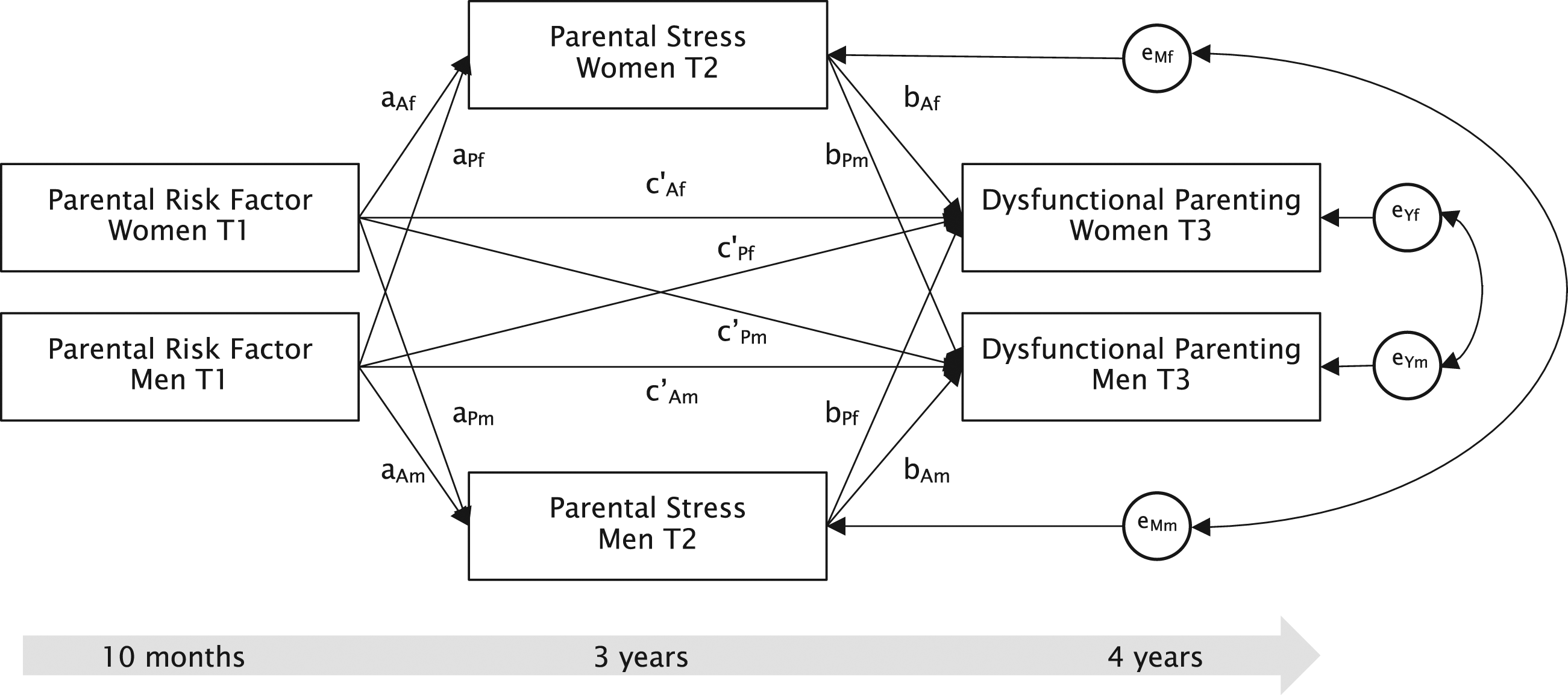
Methods
Procedure and participants
Data were collected within a longitudinal, prospective study in Switzerland to examine parental relationships and child development from pregnancy up to 4 years after birth in first-time parents (Bodenmann et al., 2019). Data for the present study were drawn from the measurement timepoint when children were 10 months (T1), 36 months (T2), and 48 months (T3) old. A total of 307 mixed-gender couples were recruited in Switzerland through hospitals, professionals, and social media platforms. Couples were included in the second or third trimester of pregnancy, expecting their first common child. The inclusion criteria were to be in a committed mixed-gender relationship for at least 1 year, German-speaking, and not concurrently in treatment for psychological disorders or relationship problems. Exclusion criteria were having prior children, expecting twins, or one partner refusing participation. Both partners were asked to complete paper-pencil or online questionnaires at each time point. Participants provided informed consent at every time point and were eligible to receive 300 Swiss Francs (330 USD) per couple as an incentive at the end of the study. The Ethics Committee of the Department of Psychology, University of Zurich, approved all study procedures and materials. Due to the dyadic analyses, we excluded couples that separated during the study (n = 15) and couples with twins (n = 10). For 114 couples, one or both partners did not provide any data at T1 and were therefore excluded. The final sample consisted of N = 168 primiparous couples. To address missing data, full-information maximum likelihood estimation (FIML) was used as the MCAR-test (Little, 1988) was not significant for women [χ2(13) = 6.45, p = .928] and men [χ2(12) = 11.71, p = .469].
At the initial time point, women averaged 33.1 years of age (SD = 3.5; range = 24–44), and men averaged 35.1 years of age (SD = 4.7; range = 27–55). Relationship duration was 7.6 years (SD = 4.0; range = 2–21). Regarding relationship status, most couples were married at T1 (68%) and all cohabitated. Fifteen couples reported going to couples therapy within 12 months before T2 or T3. Most participants were Swiss (77% women, 80% men) or German (15% women, 13% men). Seventy-nine percent of women and 72% of men held a higher education or bachelor’s degree. Despite one woman and one man having no degree, the remaining participant held a professional or high school degree. Most women (59%) and men (97%) were employed between 50% and full-time. The annual income per person ranged from 0 to over 120,000 CHF per year. Among women, 42% earned less than 40,000 CHF and 18% earned more than 80,000 CHF annually. Among men, 3% earned less than 40,000 CHF and 75% earned more than 80,000 CHF annually. On average, the participants belonged to the Swiss middle-class.
Most women (87%) reported a planned pregnancy, and 9% reported in vitro fertilization. Women gave birth by vaginal (72%) or cesarean delivery (28%). Only 3% of the children showed proximate health problems after birth. Fifty-one percent of the children were assigned male, and 49% were assigned female at birth. At T3, 76% of the families had at least a second child. Some data from the longitudinal study has been incorporated into previous publications (Meier et al., 2020; Rauch-Anderegg et al., 2020; Stadelmann et al., 2022). However, the present study is the first to apply APIMeM and investigate parental stress, depressive symptoms as well as negative communication in combination with dysfunctional parenting.
Measures
Predictor: Depressive symptoms
Depressive symptoms were measured at T1 with seven slightly adapted items from the Depression-Anxiety-Stress Scale (DASS; Lovibond & Lovibond, 1995). The subscale depression assesses the frequency of depressive symptoms in the past 2 weeks, from never (0) to most of the time (3). Example items were I felt that I had nothing to look forward to, and I found it difficult to work up the initiative to do things. In previous studies, the DASS has demonstrated excellent internal consistency in non-clinical samples and during the postpartum period (Crawford & Henry, 2003; Cunningham et al., 2013; Lovibond & Lovibond, 1995). In the current study, the scale had good internal consistencies for women
Predictor: Negative communication
Negative communication (e.g., interrupting the partner, defending yourself, withdrawal) was assessed at T1 with five items of the Marital Communication Questionnaire (MCQ; Bodenmann, 2000) ranging from never (1) to always (6). The mean was calculated with higher scores indicating more negative communication. The MCQ is based on the Specific Affect Coding System (Gottman, 1994) and showed satisfactory Cronach’s alphas (
Mediator: Parental stress
Parental Stress was assessed at T2 using the Parental Stress Scale (PSS; Berry & Jones, 1995), an 18-item self-report questionnaire. Parents rated their feelings and perceptions of their experience of being a parent from strongly disagree (1) to strongly agree (5). Item examples were having a child allows little time and flexibility in my life, it is difficult to balance different responsibilities because of my child, or I enjoy spending time with my child. The mean scores for women and men were calculated, with higher scores indicating greater parental stress. The scale has shown excellent internal consistency in previous studies (Berry & Jones, 1995; Louie et al., 2017; Nordahl et al., 2016). Internal consistency in the present study was high (
Outcome: Dysfunctional parenting
At T3, dysfunctional parenting was measured using an adapted version of the German Parenting Scale (Arnold et al., 1993; EFB; Naumann et al., 2010). Both parents rated multiple aspects of dysfunctional parenting behaviors on 13 items with a 7-point anchor scale. These aspects ranged from reactions to misbehaving of the child (e.g., If my child is naughty or behaves inappropriately…) with anchors from I speak calmly to my child (1) to I raise my voice or yell at my child (7) over inconsistent parenting behavior (e.g., When I issue an appropriate threat or warning…) with anchors from I also put them into practice (1) to I often don’t put them into practice (7) to set limits (e.g., I am a parent…) with anchors from who sets limits and tells my child what is allowed and what is not (1) to who lets my child do what it wants to do (7). The total mean score was calculated for women and men, with a higher score indicating dysfunctional parenting. Given this broad construct, the total scale showed adequate internal consistency for women (
Statistical analyses
To test the hypotheses, we used an APIMeM (Ledermann et al., 2011), an extended version of the Actor-Partner Interdependence Model (Kenny et al., 2006). This approach allows for the modeling of interdependence within a dyad (e.g., mothers and fathers), including actor, partner, and indirect effects (see Figure 1). Data were analyzed using Mplus 8.3 (Muthén & Muthén, 2012–2019). The full-information maximum likelihood estimator (FIML) was used to deal with missing data. To assess model fit, the models were evaluated according to the criteria formulated by Hu & Bentler (1999): A non-significant chi-square test, root mean square error of approximation (RMSEA) < .06, comparative fit index (CFI), and Tucker-Lewis index (TLI) > .95 indicated a good model fit. To test the indirect effects, we applied a bias-corrected bootstrapping procedure with 1,000 iterations (Preacher & Hayes, 2008). We relied on bootstrapped bias-corrected 95% confidence intervals for statistical interference testing of the mediation hypotheses (MacKinnon, 2008). We ran separate statistical models for both predictors owing to sample size restrictions.
Based on previous studies, we did not expect specific gender differences (Le et al., 2017). To test whether the paths differed by parental gender, they were constrained to be equal across gender. Therefore, we tested stepwise (paths a, b, c’) to determine whether the more parsimonious model still fits the data by examining the estimates, comparative fit indices, and chi-square difference tests and by comparing models with freely estimated paths with models in which the specific paths were constrained to be the same across gender.
We included relationship duration in years, parental physical problems, child gender, and the presence of younger siblings as control variables in all models. Additional covariates regarding socioeconomic status (e.g., family income, employment status) did not change the effects, and were therefore not included in the final models. In addition, we initially included parental stress at T1 as a control variable, but the model estimation suffered from multicollinearity issues, and parental stress had to be excluded at T1.
Results
Descriptive statistics and bivariate correlations for study variables.
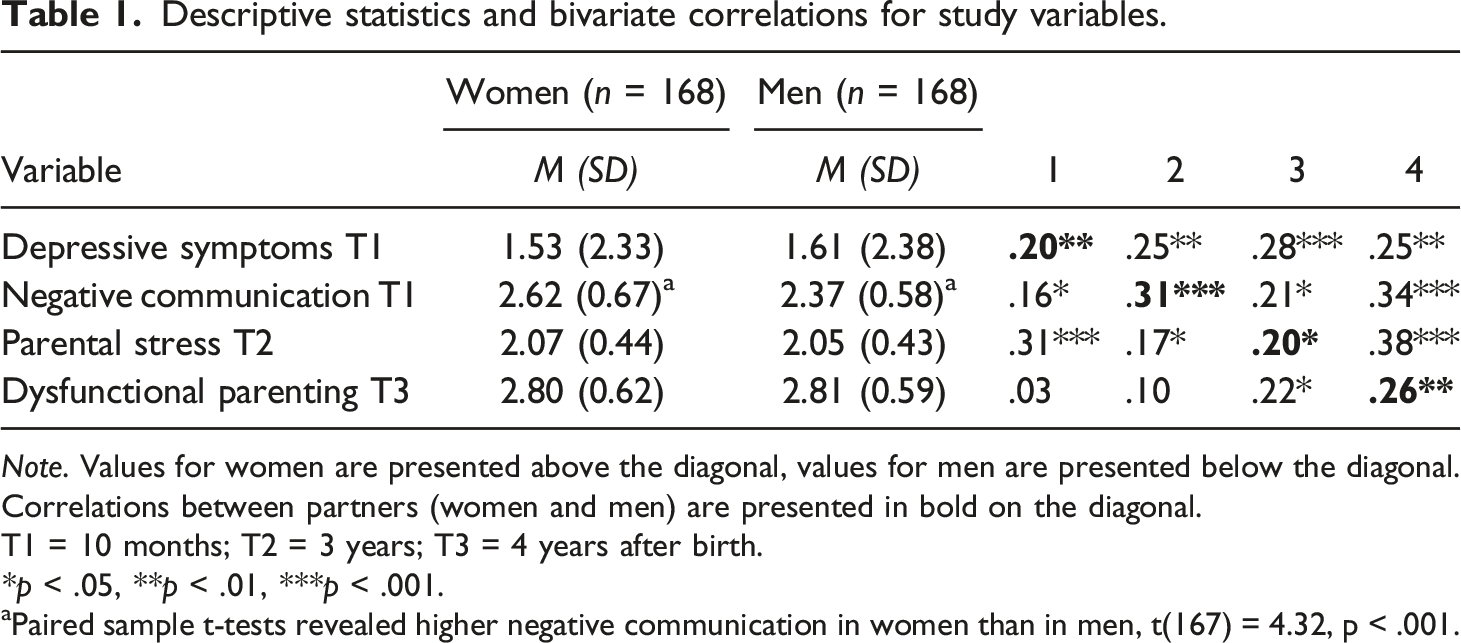
Note. Values for women are presented above the diagonal, values for men are presented below the diagonal. Correlations between partners (women and men) are presented in bold on the diagonal.
T1 = 10 months; T2 = 3 years; T3 = 4 years after birth.
*p < .05, **p < .01, ***p < .001.
aPaired sample t-tests revealed higher negative communication in women than in men, t(167) = 4.32, p < .001.
Depressive symptoms
Actor–Partner Interdependence Mediation Model with direct and indirect effects between depressive symptoms, parental stress, and dysfunctional parenting.
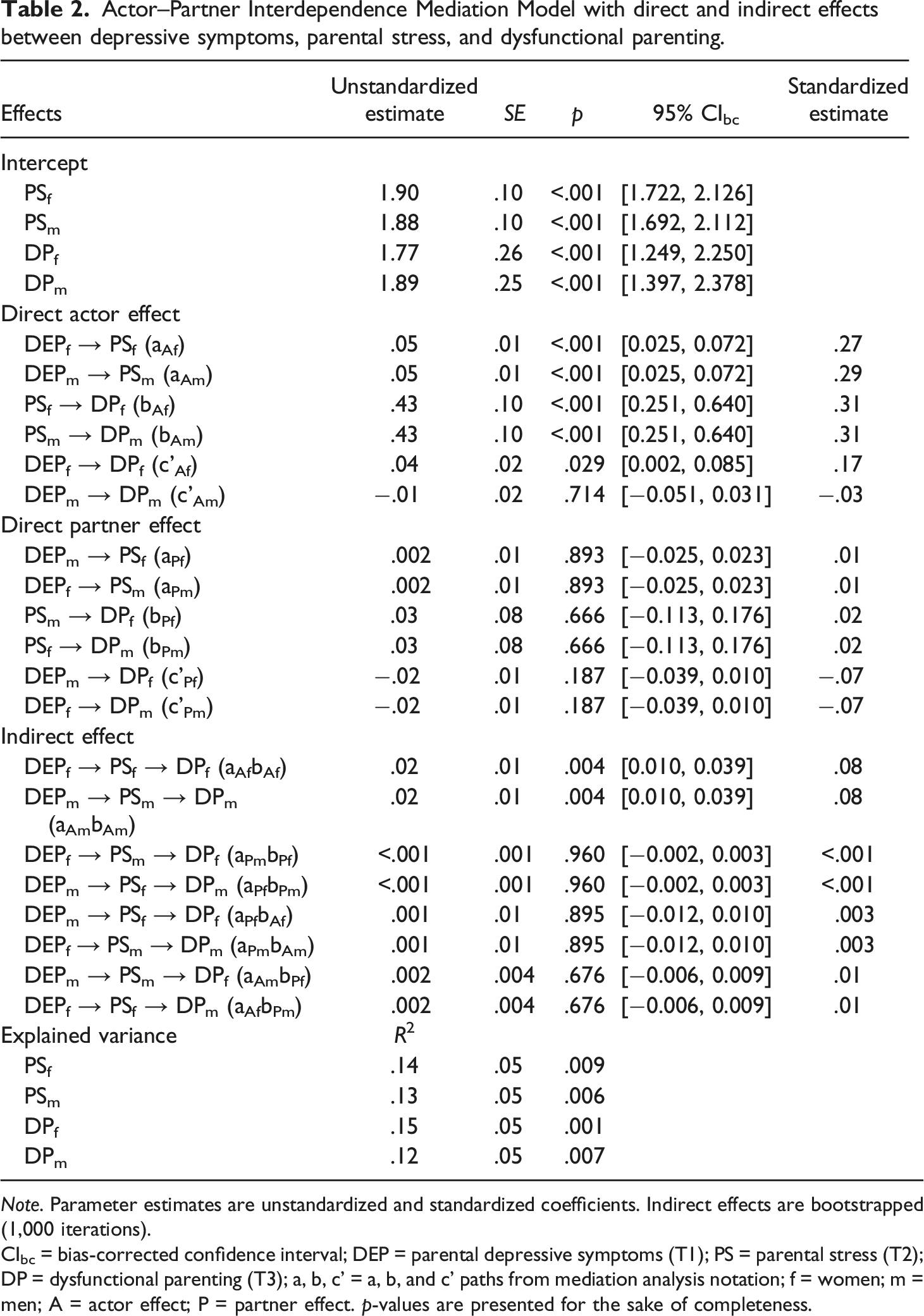
Note. Parameter estimates are unstandardized and standardized coefficients. Indirect effects are bootstrapped (1,000 iterations).
CIbc = bias-corrected confidence interval; DEP = parental depressive symptoms (T1); PS = parental stress (T2); DP = dysfunctional parenting (T3); a, b, c’ = a, b, and c’ paths from mediation analysis notation; f = women; m = men; A = actor effect; P = partner effect. p-values are presented for the sake of completeness.
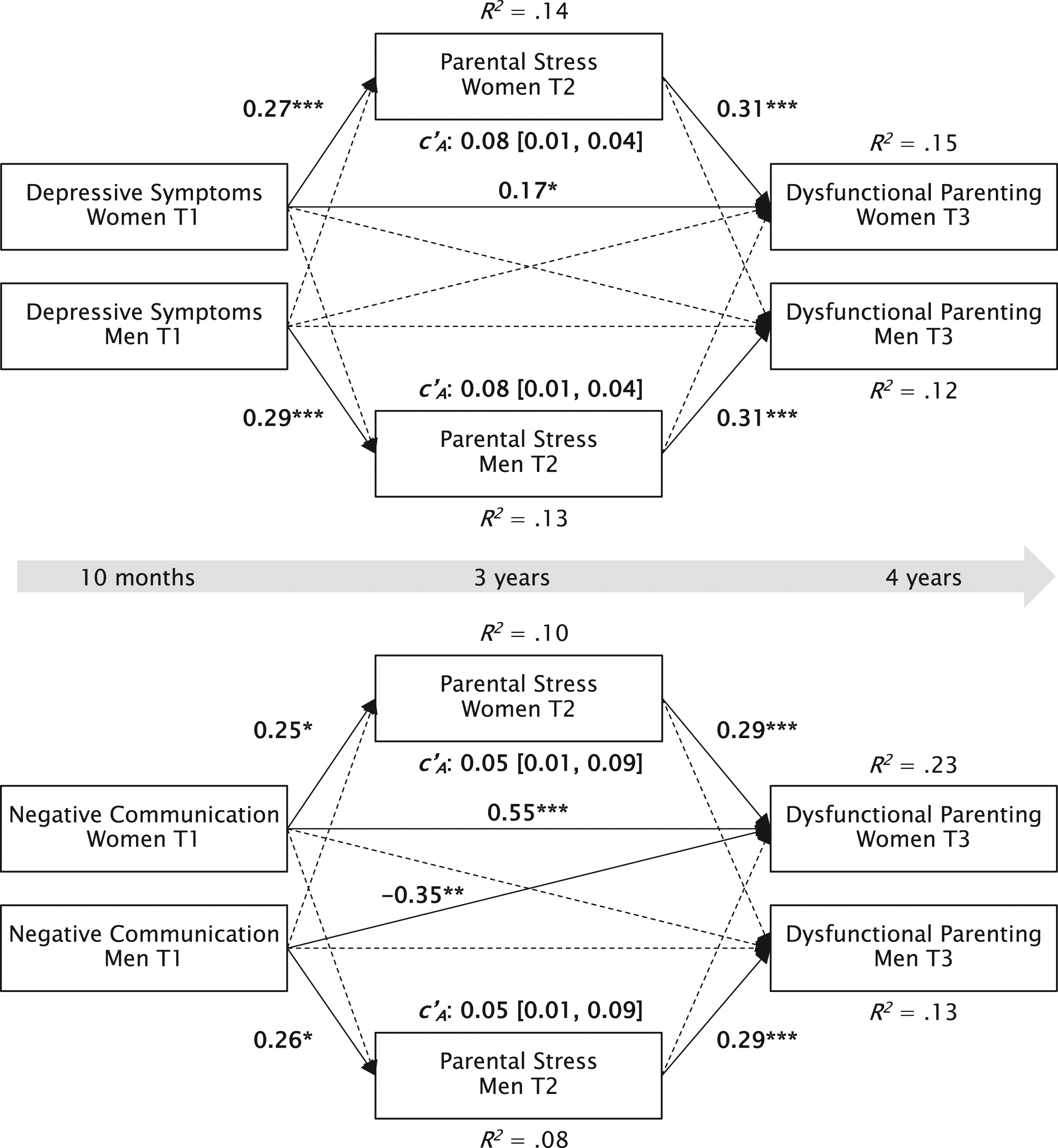
Actor-Partner Interdependence Mediation Models (APIMeM) with depressive symptoms and negative communication as parental risk factors, parental stress as mediator, and dysfunctional parenting as outcome. Note. T1 = 10 months; T2 = 3 years; T3 = 4 years after birth. Unstandardized coefficients and R 2 values are displayed. For ease of presentation, covariances between women and men are not depicted. Significant paths are shown in bold. *p < .05, **p < .01, ***p < .001.
Regarding indirect effects (H1b), parental depressive symptoms were related to more dysfunctional parenting through each person’s parental stress (b = 0.02; SE = 0.01; 95% CIbc [0.010, – 0.039]; aAbA), which indicates that parental stress mediated the association between own depressive symptoms and own dysfunctional parenting longitudinally. No other indirect effects were significant, meaning that the indirect effects were only significant within-person and not between-person. All predictors in the depressive symptoms model (including covariates) accounted for 15% of the variance in women’s and 12% of the variance in men’s dysfunctional parenting.
Negative communication
Actor–Partner Interdependence Mediation Model with direct and indirect effects between negative communication, parental stress, and dysfunctional parenting.
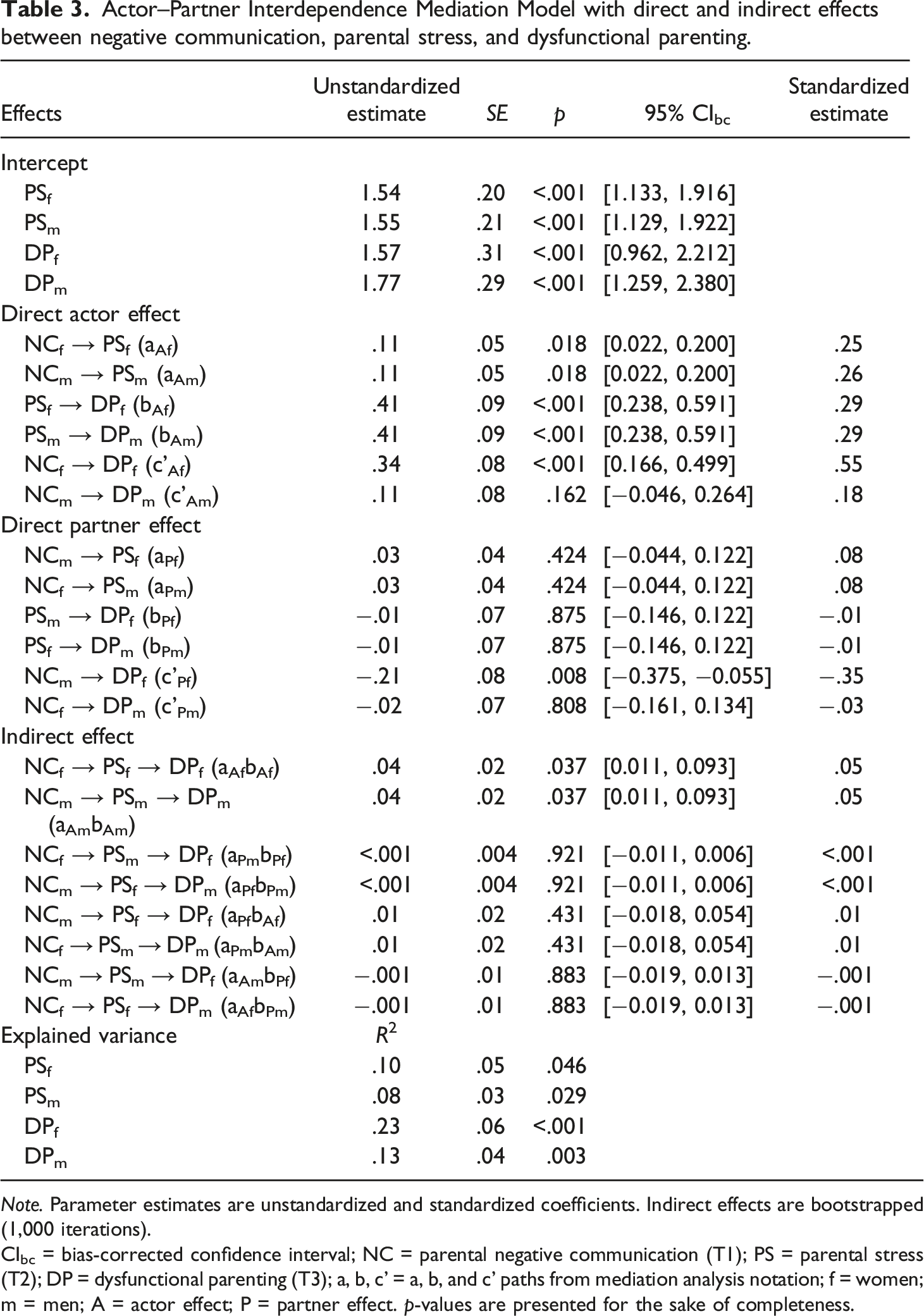
Note. Parameter estimates are unstandardized and standardized coefficients. Indirect effects are bootstrapped (1,000 iterations).
CIbc = bias-corrected confidence interval; NC = parental negative communication (T1); PS = parental stress (T2); DP = dysfunctional parenting (T3); a, b, c’ = a, b, and c’ paths from mediation analysis notation; f = women; m = men; A = actor effect; P = partner effect. p-values are presented for the sake of completeness.
Regarding the indirect effects (H2b), the indirect actor effects of negative communication on dysfunctional parenting through parental stress (aAbA) were significant for both women and men (b = 0.04; SE = 0.02; 95% CIbc [0.011, –0.093]), indicating that parental stress mediated the association between parents negative communication and dysfunctional parenting longitudinally. The indirect effects were only significant within persons (actor effects) but not across persons (partner effects). In general, all predictors in the negative communication model (including covariates) accounted for 23% of the variance in women’s and 13% of the variance in men’s dysfunctional parenting. Considering covariates, the presence of siblings was associated with greater parental stress at T2 for both parents in the negative communication model. This supports the notion that having more than one child is associated with more parental stress but not necessarily with more dysfunctional parenting.
Discussion
This longitudinal, prospective study investigated whether parental risk factors (i.e., depressive symptoms, couples’ negative communication) at 10 months postpartum predicted dysfunctional parenting at 4 years postpartum and whether parental stress at 3 years postpartum mediated these associations in mixed-gender first-time parents. To our knowledge, this is the first study to combine individual and relational parental risk factors for dysfunctional parenting in early childhood and investigate parental stress as a mediator in the interpersonal parenting process. In addition, a dyadic perspective considering both parents’ perceptions of individual and relationship aspects was applied to better understand the hypothesized spillover of parental risk factors on parenting behavior within and between parents over time (Cox & Paley, 2003).
Associations between parental risk factors and dysfunctional parenting
In line with our assumptions, we found evidence for within-person spillover of both parental risk factors on parenting. Specifically, among mothers, their depressive symptoms (H1a), their negative communication (H2a), and their partner’s negative communication directly predicted mothers’ dysfunctional parenting, whereas no such direct effects were found on fathers’ dysfunctional parenting. Additionally, more depressive symptoms and negative communication were linked to greater parental stress, which in turn, were related to more dysfunctional parenting in both parents. Consistent with the process model of parenting (Belsky, 1984; Taraban & Shaw, 2018), both individual and relationship characteristics were associated with parenting behavior over time. According to our results, however, parental stress is critical for this process. Consistent with previous findings (Le et al., 2017), our study confirmed that parental stress in early childhood increased later dysfunctional parenting in primiparous couples. Previous longitudinal and dyadic studies have found similar patterns—direct actor-only effects – of parental stress on later dysfunctional parenting among parents with school-aged children (Ponnet et al., 2013).
Mediation by parental stress
Regarding the mediating link, mothers’ and fathers’ parental stress mediated the association between parents’ depressive symptoms and dysfunctional parenting (H1b), as well as between negative communication and dysfunctional parenting (H2b) from 10 months to 4 years postpartum. These findings underline the longitudinal mediating effect of psychological well-being and parental stress on parenting (Le et al., 2017). Furthermore, we conclude that parenting deteriorates as a consequence of low parental relationship functioning and that this deterioration is more pronounced in parents who experience high levels of stress regarding their parental role.
In contrast to our results, Le et al. (2017) additionally found mediated partner effects of mothers’ and fathers’ negative affect on the partner’s parenting via the partner’s parental stress. Possible explanations for these differences may be that they conceptualized parenting more broadly and investigated a shorter period (from 6 months to 3 years postpartum). Furthermore, suppressor variables (e.g., dyadic coping, coparenting) could have covered such spillover effects for individual and relationship characteristics beyond the actor-mediation effects in our analyses (Durtschi et al., 2017; Hilpert et al., 2013). Rucker et al. (2011) recommended that investigating suppression effects would provide a deeper understanding of the variables’ association. Future studies on predicting parenting should consider parental stress and dyadic coping because of their associations with better relationship functioning, coparenting, and parenting (e.g., Bodenmann, 2005; Zemp et al., 2017).
Gender differences and partner effects
We further tested whether paths differed by the gender of the parent. Specific direct but no indirect effects differed significantly between mothers and fathers. For example, the direct actor effect of negative communication and dysfunctional parenting was found in mothers but not in fathers. Negative couple communication may influence mothers’ parenting more than fathers’ parenting because, on average, fathers in mixed-gender relationships may be less involved in childcare than mothers. Therefore, paternal parenting may be less influenced by interparental relationship factors. Furthermore, mothers reported more negative communication with their partners 10 months postpartum than fathers did. This dissimilarity could also explain the finding of the association due to the occurrence of more negative behaviors in mothers.
Moreover, the negative communication model explained a higher variance of dysfunctional parenting among women than men. Thereby, men may differ in their spillover process of relationship aspects and stress on dysfunctional parenting in early childhood from their partner regarding various unconsidered aspects. For example, another study found that having a demanding and difficult child makes fathers more prone to dysfunctional parenting than mothers (McBride et al., 2002). As stated by the father-vulnerability hypothesis, fathers’ interactions with their children may be affected more by interparental conflicts than mothers’ interactions (Cummings et al., 2010). Accordingly, fathers’ parental stress was previously found to spill over into the couple’s relationship, with stronger effects for fathers’ parental stress than for mothers’ (Durtschi et al., 2017). However, in line with most recent studies, we did not substantiate this assumption in general (Le et al., 2017; Ponnet et al., 2013; Van Eldik et al., 2019). Future research should consider children's behavioral problems and bidirectional effects of parental stress and individual and relationship variables to better understand such spillover effects in mothers and fathers.
Regarding interdependence within families and parents, we found only one partner effect: Less negative communication in fathers was associated with more dysfunctional parenting in mothers. This finding was surprising because less negative communication is anticipated to buffer dysfunctional parenting. However, this negative association indicates that distressed mothers may not benefit from reduced negativity in their interactions with their partners but instead show even more dysfunctional parenting. Although this effect was weaker than the actor effect of mothers’ negative communication, it was significant. Presumably, mothers feel less supported due to fathers’ reduced engagement in childcare, thereby showing ineffective parenting practices. It is also plausible that an individual’s parenting might deteriorate because of a combination of both partners’ negative interactions and other variables (e.g., child gender, siblings, own depressive symptoms, and positive communication; Stevenson et al., 2019). For example, couples with more than one child reported more parenting stress than parents with an only child, whereas the gender of the child did not affect parental stress or parenting. This suggests that having multiple children might be stressful, especially for mothers taking the primary responsibility for childcare.
Interestingly, men in our study reported similar levels of depressive symptoms at 10 months after birth as women. This finding contradicts the majority of studies reporting higher levels of depressive symptoms in mothers than in fathers after birth (Vismara et al., 2016). However, more recent studies on paternal depression have found that paternal depression may occur later than maternal depression, often with a rise in depressive symptoms towards the end of the first year postpartum (Gedzyk-Nieman, 2021; Low et al., 2022).
Limitations
Although the present study enhances our understanding of mechanisms predicting parenting in a dyadic context, our results are also limited. First, our sample consisted of mixed-gender, White, predominantly well-educated, and middle-class couples. However, cross-cultural differences in parenting (e.g., norms for expected behavior, family structures for childcare, and cultural values) could shape the spillover process of individual and parental functioning on parenting (Lansford, 2022). Furthermore, economic stress, which was not prevalent in this sample, was found to be a risk factor for interparental conflict (Wickrama & O’Neal, 2019). Thus, the findings cannot be generalized to parents from non-western cultures, with low socioeconomic status and financial problems, or to same-gender couples, single parents, or parents of twins. In addition, most participants reported depressive symptoms below a clinical cutoff and low levels of negativity, stress, and dysfunctional parenting. However, chronic depression, episodes of major depression, or hostile and violent interparental conflict are common in first-time parents and are risk factors for dysfunctional parental and child behavior (Lovejoy et al., 2000; Petch et al., 2012; Van Eldik et al., 2020). Groups at risk and more heterogeneous samples should be examined to determine whether the pattern of findings can be generalized to more diverse samples. We did not ask for information on gender identity or parental disability status, which should be necessarily considered in future studies. Second, the temporal order of the given models does not imply unidirectional or causal effects. Due to bidirectionality and mutual interdependence in the family system, ineffective parenting behavior (i.e., low parental self-efficacy) could also increase parental stress over time (Schoppe-Sullivan et al., 2021). Third, sample size restrictions prevented us from simultaneously estimating a complete model with multiple risk factors. Hence, the differential effects of depressive symptoms and negative communication cannot be compared directly. However, this is the first study addressing these predictors in one study in men and women in early childhood, providing an essential basis for future studies to conduct power analyses for specific effects. Finally, all measures were collected as self-reports capturing parents’ perception of depressive symptoms, communication, stress, and parenting behavior, which may be prone to same-method bias. To reduce the bias of social desirability and shared method variance, future research should implement observational data and intensive longitudinal assessments to further examine interpersonal processes of parenting (Kouros et al., 2014).
Implications and conclusion
Our results carry important implications for parenting interventions and clinical practice. For most parents, parenting in early childhood is challenging, especially during times of increased stress. A better understanding of mechanisms predicting parenting behavior in early childhood could also provide more specific information on psychological well-being and relationship functioning, aiming to reduce parental stress and foster effective parenting early on. Enhancing and maintaining effective parenting practices could be promoted directly but also through appropriate individual and dyadic coping as well as communication skills. The Couples Coping Enhancement Training (CCET; Bodenmann & Shantinath, 2004) represents a preventive intervention that fosters communication and coping skills and might increase effective parenting. Previous results illustrated that such interventions could help parents to better handle parental tasks during the first year after a child’s birth (Halford et al., 2010) and that children exhibit less externalizing behavior post-intervention (Bodenmann et al., 2008b; Zemp et al., 2016). Positive long-term effects on parent-child interactions can unfold by minimizing parental individual and relationship risk factors. Our results highlight that this might be important even for parents with a lower burden, who are probably not in counseling or therapy, and indicate the additional value of low-threshold services and early interventions. Therefore, early interventions for effective parenting may be promising and should not be limited to families with high-risk profiles. Additionally, we found effects for both maternal and paternal parenting, which strongly supports the enclosure of both partners in interventions and treatment. Thus, both parents should be addressed with tailored information and interventions by public health practitioners and counselors, as our results revealed comparable effects regarding parental stress for mothers and fathers. Overall, our results demonstrate that the risk factors for dysfunctional parenting, such as depressive symptoms, negative communication, and parental stress, are already of great importance for parenting quality in the first years after birth.
Footnotes
Acknowledgements
We especially thank all parents and project collaborators for engaging in this study. We thank Selina Landolt for proofreading.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection and preliminary analysis were funded by the Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (No. 100014_146775/10001C_173270).
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research cannot be publicly shared but are available upon request. The data can be obtained by emailing: