
Abstract
Individuals with visual impairments and intellectual disabilities (ID) often do not wear glasses, although this may improve functioning. We present (1) a single-subject multiple baseline study that examined the effects of wearing distance glasses on viewing behaviour, adaptive functioning, and well-being in a participant with severe ID, and (2) a Delphi study that examined the perspectives of 12 professionals on wearing glasses by individuals with ID. The participant adapted to wearing glasses with the Glasses Habituation Programme. Wearing glasses indoors decreased attention to objects further away, possibly because objects were recognised faster. Interviews with the caregiver and father showed that visual (related) behaviours improved, especially outdoors. Caregiver-reported questionnaires revealed better adaptive functioning but decreased well-being. Professionals identified key factors for the provision and successful wearing of glasses and agreed on the potential positive effects in different domains. Findings, if replicated in larger randomised controlled trials, point to the added value of glasses.
Introduction
Visual impairments (VI) can be defined as a decimal Snellen visual acuity between 0.05 and 0.30 and/or a visual field between 10° and 30° (World Health Organisation, 2018). Individuals with ID often experience VI caused by refractive errors, such as myopia (near-sightedness) and hyperopia (far-sightedness) (Donaldson et al., 2019; Hsieh et al., 2025; Van Splunder et al., 2003; Warburg, 2001). Refractive errors can be detected through visual screening and are typically correctable with glasses. Yet, many individuals with refractive errors and ID do not wear glasses and remain visually impaired (Van Splunder et al., 2003). One contributing factor is that eye care specialists do not prescribe glasses because the diagnosis is missed (de Wit et al., 2019; Li et al., 2015). In addition, studies with children with and without additional support needs have shown that after the initial vision screening, there was a relatively high rate of missed follow- appointments, which reduced the likelihood of children receiving glasses (Bruce & Outhwaite, 2013; Tooth & Rogowski, 2025, see also Cassetti et al., 2019). Also, family members and caregivers may not provide glasses because they assume that their child or client will not tolerate glasses or will not benefit from wearing glasses (Haugen et al., 1995; Li et al., 2015). Furthermore, individuals with ID may struggle to wear glasses, possibly because of changes in visual workload, visual perception, and sensory input (Haugen et al., 1995; Li et al., 2015), which highlights the need for (professional) support during the habituation process. This paper builds on a comment article published in this journal, which addressed the challenges and opportunities of researching the impact of wearing glasses in individuals with ID (B. Hilberink et al., 2024). Here, we present two studies: (1) a single-subject multiple baseline study that examined the effects of wearing glasses on viewing behaviour, adaptive functioning, and subjective well-being in a male adult with severe ID, and (2) a Delphi study that examined professionals’ perspectives on wearing glasses by individuals with ID.
Individuals with an impaired ability to compensate for VIs using cognitive strategies, and for cognitive impairments using visual strategies, experience difficulties across various domains of functioning. Research showed that individuals with VI and ID displayed more communication deficits, exhibited higher rates of insecure movement, and were more dependent on others to perform daily activities compared to individuals with ID only (Dijkhuizen et al., 2016; Evenhuis et al., 2009; van der Aa et al., 2023). Other evidence indicated that children with VI and ID showed more emotional and behavioural problems than children with ID only (Alimovic, 2013). Furthermore, a systematic review found associations of VI with self-injurious behaviour in individuals with ID (de Winter et al., 2011).
Wearing glasses may lead to improvements in daily functioning among individuals with VI and ID, even when VI cannot be fully eliminated. In a non-experimental study, individuals with ID noted that when they wore glasses, they were better able to see people’s faces, watch television, read small print, and go to the park. Some individuals also reported that wearing glasses led to improved self-confidence and well-being (McGlade et al., 2010). In addition, a randomised controlled trial (RCT), although not focusing on individuals with ID, showed that wearing glasses improved quality of life and decreased depression symptoms in older adults with refractive errors residing in nursing homes as compared to those who did not wear glasses (Owsley et al., 2007). Finally, a systematic review found that wearing glasses improved well-being and quality of life in children with VI (Pirindhavellie et al., 2023). It remains unclear whether the findings of the latter two studies can be generalised to adults with ID.
Individuals with VI and ID often need support to wear glasses. Yet, evidence-based interventions to promote the wearing of glasses are scarce. Here, we focus on the Glasses Habituation Programme (H. Hilberink et al., 2020), which can be implemented with adults. The programme is developed by psychologists from Bartiméus, a Dutch organisation specialised in care for individuals with VI (and ID). The programme has been implemented since the ‘90s and takes between 3 and 6 months to complete. Six intervention components are described: (1) increasing awareness about VI and the potential benefits of wearing glasses, (2) empowering caregivers by involving them in the decision-making process, (3) developing individualised action plans, (4) gradual exposure to wearing glasses, (5) making the client aware of visual improvements, and (6) increasing the client’s intrinsic motivation by creating positive experiences with wearing glasses.
To date, it is not known whether individuals participating in the Glasses Habituation Programme demonstrate improvements in daily functioning, and no studies have examined professionals’ perspectives on the wearing of glasses by individuals with ID. This is surprising, as demonstrating that glasses improve functioning would further underscore the importance of integrating vision services into primary care. Furthermore, habituation to wear glasses requires time, effort, and dedication from clients, caregivers, and family members. A better scientific understanding about the effects of wearing glasses may increase motivation to participate in intervention programmes. In addition, professionals are directly involved and have firsthand experience of supporting people to wear glasses. Professionals can provide valuable insight into the factors that impact the decision to provide glasses and the factors that contribute to wearing glasses. Finally, professionals may offer understanding about the perceived benefits and they may identify strengths and areas for programme improvements.
In sum, we report on two studies: (1) a single-subject multiple baseline study that examined the effects of wearing distance glasses on viewing behaviour, adaptive functioning, and subjective well-being in a male adult with severe ID, and (2) a Delphi that examined professionals’ perspectives on wearing glasses by individuals with ID. It was hypothesised, albeit cautiously because of the limited number of studies, that wearing glasses would improve viewing behaviour, adaptive functioning, and subjective well-being.
Method – single-subject multiple baseline study
Design
Initially, we planned to conduct a randomised multiple baseline study with 12 participants, but this was not feasible due to recruitment difficulties (B. Hilberink et al., 2024). We were able to include two participants, but one participant dropped out due to resistance to wearing glasses. Therefore, this study reports on complete data from one participant. An independent researcher conducted randomisation of the baseline period (15, 20, or 24 days) using an online random number generator. The baseline phase (20 days) was followed by an intervention phase (6 months). Due to the open-label design, researchers were not blinded to enrolment in the Glasses Habituation Programme. Observations were conducted during the baseline phase (n = 7 observations; roughly one every 3 days) and intervention phase (n = 12 observations; one every 2 weeks) in a quiet room at the participant’s home-care facility. The participant wore glasses during all measurements in the intervention phase. Prior to the baseline phase and after the intervention phase, the caregiver filled in online questionnaires. Finally, after the intervention phase, interviews were conducted with the participant’s caregiver and father. No adverse events occurred. The Single-Case Reporting Guideline In BEhavioural Interventions (SCRIBE) 2016 Checklist (Tate et al., 2016) was used for reporting.
Participant description
‘Tony’ (pseudonym) is a 41-year-old male who lives in a home-care facility in the Netherlands with 24-hr access to professional caregivers. Tony is diagnosed with severe ID and Malan syndrome: a rare genetic disorder characterised by overgrowth, macrocephaly, developmental delay/ID, and anomalies in skeletal structure and behaviour (Malan et al., 2010). Tony can walk but feels more confident with his walker. He enjoys playing with sand, and riding and cleaning his tricycle. A behavioural specialist determined that Tony met inclusion criteria for participation, which included a diagnosis of ID (mild to profound), aged ⩾ 18 years, registered to take part in the Glasses Habituation Programme, and a recommendation to wear glasses to correct myopia (near-sightedness) or hyperopia (far-sightedness). Exclusion criteria were severe medical conditions that required treatment within 6 months and a recommendation to wear reading glasses, computer glasses, bifocal glasses, or multifocal glasses. During a multidisciplinary consultation, Tony’s caregiving system was informed about the study. They received an information letter and responded positively. Tony was advised to wear glasses with a −2.00 prescription to correct myopia. During the visual function assessment, no signs of accommodation lag or cerebral visual impairment (CVI) were found, although it is difficult to fully exclude these conditions in this population. Tony’s father provided written informed consent for himself and Tony. The caregiver also provided written informed consent. The Medical Ethical Review Board of the VUmc, The Netherlands provided approval (no. 2022.0603).
Glasses Habituation Programme
Bartiméus and Visio provide a description of the programme online (www.kennisoverzien.nl; currently available only in Dutch). Figure 1 presents an overview of the programme phases: (1) Intake: based on findings from a visual function assessment and multidisciplinary consultation, an interview (intake) takes place with the client’s caregiving system. The professional provides information about the refractive error and the recommended glasses. The professional explains why glasses might be beneficial and evaluates feasibility. The professional introduces the Glasses Habituation Programme and explains the principles on which the programme is based. (2) Perception: the professional gathers a broad spectrum of information about the client so that an individualised treatment plan can be developed. The primary goal and working goals are set, and it is determined which environments and activities are most optimal for habituation. (3) Action plan: the professional outlines the goals and agreements in a personalised action plan, whereby the principles (pillars) of the intervention are outlined and translated into concrete goals and activities. (4) Implementation: the glasses are purchased and provided by the client’s daily caregivers, parents, and/or other family members in accordance with the action plan. (5) Evaluation: a few days after the start of the programme, the professional meets with the client’s caregiver system to evaluate their experiences. The working goals and/or the action plan are adapted (if necessary) and the next evaluation moment is scheduled. (6) Adaptation of action plan: implementation and evaluation of the action plan is repeated until the programme is successfully completed. The programme may be terminated when the client is, despite all efforts, not able to wear glasses. (7) Final evaluation: the professional discusses with the client’s caregiver system whether the primary goal and working goals have been achieved. It is also discussed whether there are still barriers that make wearing glasses difficult or impossible. (8) Final call: after 4 months, there is a call to discuss any remaining questions.
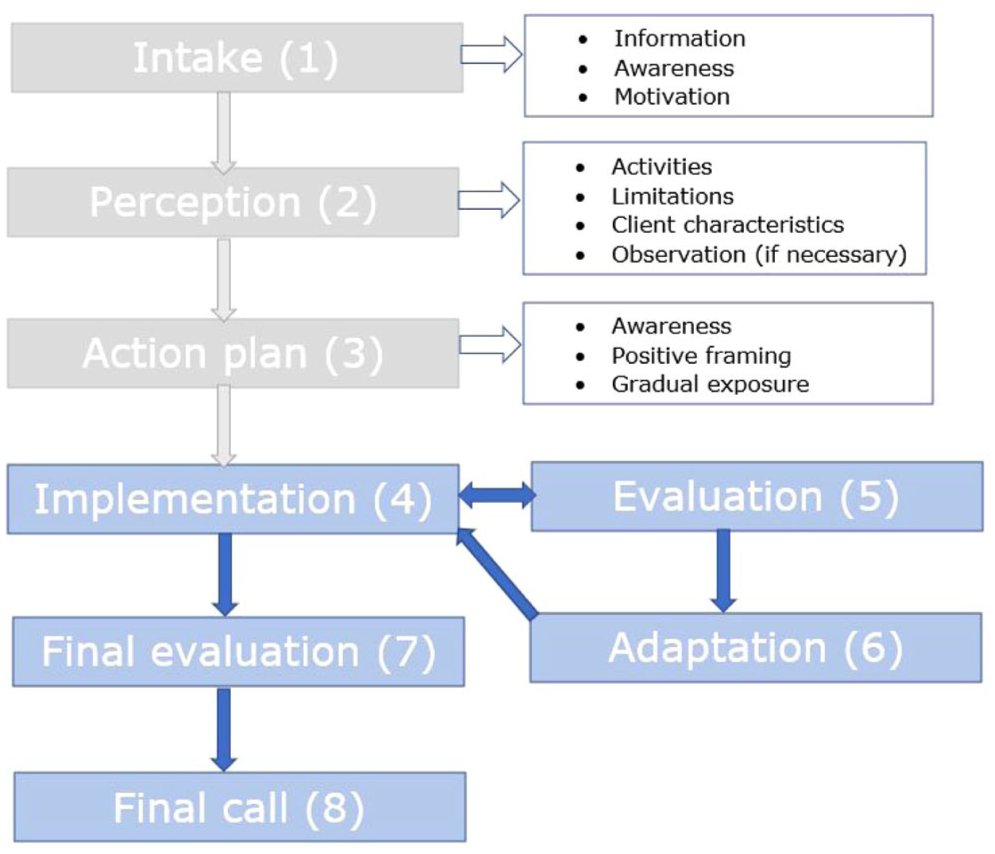
Overview of the phases in the Glasses Habituation Programme.
Programme phases 1–3 were conducted during the baseline phase, and programme phases 4–8 were conducted during the intervention phase. A professional from Visio was responsible for the implementation of the Glasses Habituation Programme. This professional was informed but not involved in the study. Intervention fidelity was ensured by training and manualisation of the programme.
Viewing behaviour
Viewing behaviour was observed 19 times (baseline phase; n = 7 measurements, intervention phase; n = 12 measurements) during semi-structured interactions between Tony and his caregiver. The participant and caregiver were seated at a table, opposite each other at approximately 50 cm (i.e., 19.69 inch) distance. The interaction consisted of five activities. For each activity there was a close-range and a long-distance version, during which the caregiver moved two seats to the side. For example, during the first activity the caregiver offered the participant a book with pictures of everyday objects (1; close-range) and then offered the book again (1; long-distance) (for more details see Supplemental Materials). To our knowledge, there was no observational scale for viewing a behaviour in individuals with ID, so we used a self-developed scale (see Supplemental Materials). One of the scale developers (K.F.) and a university master student used the first version of the scale to code video recordings of participants with ID who were not enrolled in this study. Codings were discussed with the other scale developers (B.H., J.V.-L., and T.v.D.) after which the scale was modified to its current version. The scale describes different viewing behaviours, including (1) attention for object nearby, (2) attention for person nearby, (3) attention for object further away, (3) attention for person further away, (4) attention to the environment, (5) no visual attention, (6) eye-hand coordination, (7) usage of distance shortening, and (8) squinting or frowning with the eyes. An independent observer (university master student) was trained by one of the scale developers (K.F.). The observer received an explanation of the coding procedures and then coded practice videos prior to coding one video for reliability purposes. The percentage of agreement between the scale developer and observer was 89.2%. The observer was blind to the phase of the study and coded the videos in random order. Coding was performed using Noldus the Observer version 10.5 software (Noldus Information Technology, Wageningen, the Netherlands). Since the videos varied in length, a percentage score for duration and frequency of each viewing behaviour was calculated.
Adaptive functioning
To measure adaptive functioning, the caregiver reported at the start of the baseline phase and at the end of the intervention phase on the Dutch version of the Vineland Adaptive Behaviour Scales–Third edition (VABS-3; Sparrow et al., 2016). The VABS-3 includes three domains: Communication (subdomains: Receptive, Expressive, and Written), Daily Living Skills (subdomains: Community, Domestic, and Personal) and Socialisation (subdomains: Coping Skills, Interpersonal Relationships, and Play and Leisure Time). In the present study, we administered only items from the subdomains Receptive (23 items), Expressive (7 items), Personal (32 items; measuring eating, dressing, and personal hygiene skills), and Interpersonal Relationships (16 items) as these domains were expected to be impacted by wearing glasses. Items were rated on a 3-point scale ranging from 0 (never), 1 (sometimes), to 3 (usually). Items were administered in a developmental order using basal and ceiling criteria. For each subdomain, raw scores and norm-referenced V-scale scores (M = 15, SD = 3) were calculated. Higher scores reflect higher levels of adaptive functioning. The VABS-3 is a psychometrically sound instrument with excellent Cronbach’s alpha values across all domains (range 0.90–0.98). Furthermore, the VABS-3 correlates with other instruments measuring adaptive functioning (Sparrow et al., 2016).
Subjective well-being
To measure subjective well-being, the caregiver reported at the start of the baseline phase and at the end of the intervention phase on the Dutch version (Petry et al., 2010) of the Mood, Interest, and Pleasure Questionnaire for individuals with severe and profound intellectual disabilities (MIPQ; Ross & Oliver, 2003). This version of the MIPQ includes 23 items which are divided across 3 subscales: Positive Mood’ (9 items), Negative Mood (7 items), and Interest (7 items). Items were rated on a 5-point Likert-type scale, ranging from 0 (never) to 4 (always). Ratings were based on behaviour in the preceding 2 weeks. An item example on the positive mood subscale is: ‘In the last two weeks, how often did you hear positive vocalisations when the participant was involved in an activity?’. Items were summed to create a score for each subscale (positive mood; 0–36, negative mood; 0–28, and interest; 0–28). An overall score for subjective well-being was created by summing the total subscale scores (0–92). Negatively phrased items were recoded so that higher scores reflect higher subjective well-being. The MIPQ shows good psychometric properties (Petry et al., 2010; Ross & Oliver, 2003).
In depth-interviews
In-depth semi-structured interviews were conducted with the caregiver and father after completion of the intervention phase. Interviews lasted approximately 30 min. Questions were organised into three broad categories: (1) general experiences with wearing of glasses, (2) effects of wearing of glasses on functioning, and (3) experiences with the Glasses Habituation Programme. Interviews were conducted via Microsoft Teams, audio recorded, transcribed verbatim, and checked by university master students.
Data analysis plan
A descriptive approach was used to examine the effects of wearing glasses on adaptive functioning and subjective well-being. The statistical technique of the Nonoverlap of All Pairs (NAP; http://www.singlecaseresearch.org/calculators/nap) was used to examine effects of wearing glasses on viewing behaviour. NAP is a sound technique to determine intervention effects (Parker & Vannest, 2009). P-values of <.05 reflect a significant effect. Interpretation of NAP effect sizes are weak effect: 0–0.65, medium effect: 0.66–0.92; strong effect: 0.93–1.0 (Parker & Vannest, 2009). To interpret NAP accurately, calculation was reversed when scores were lower during the intervention phase than those in the baseline phase (Dyzel et al., 2023). Finally, an adapted reflexive thematic approach was used to analyse the interviews. That is, a researcher (B.H.) and a licenced psychologist (not involved in the study) read the transcripts carefully to familiarise themselves with the data, after which they both highlighted important comments (all independent of each other). The researcher then selected all comments that were highlighted by both of them, generated initial codes, and organised the codes into broader (sub)themes to allow meaningful interpretation of the data. The psychologist reviewed and approved the identified (sub)themes and data interpretation.
Method–Delphi study
Design
This Delphi study was conducted alongside the single-subject multiple baseline study. The Delphi method (Keeney et al., 2011) is a suitable method to examine professionals’ perspectives on wearing glasses by individuals with ID as it is designed to systematically gather expert opinions to develop consensus. Main components include anonymity of experts, repeated rounds of controlled feedback, and an equal representation of opinions in the results (Rahmani et al., 2020). The Delphi study was conducted by an interdisciplinary team, including clinical experts in the field of VI and ID, behavioural scientists, and master students in the field of child and family sciences. The Delphi study took place from February 2024 to March 2024. We adopted a modified Delphi design (Hasson & Keeney, 2011), which included two rounds and online interviews. A priori, it was decided to terminate rounds when ⩾70% consensus was reached. The authors did not consult third parties on methodology. The Delphistar guidelines were used for reporting (Niederberger et al., 2024).
Participants
The Delphi group included 12 female professionals from two Dutch organisations specialised in care for individuals with VI (and ID) (i.e., Bartiméus; n = 8, Visio; n = 4). The eight professionals from Bartiméus provide the glasses habituation programme to individuals aged ⩾18 years. The four professionals from Visio provided the programme to both children and adults. It was specified to all professionals that the Delphi focused specifically on individuals aged ⩾18 years. Professionals were purposively sampled; ambulatory caregivers, behavioural experts, and consultants of individuals with VI and ID were informed via email and those who expressed interest received an information letter. Participants were eligible and considered professionals when they implemented the Glasses Habituation Programme within the last 2 years, had at least 1 year of experience with clients with ID ⩾18 years, and worked for Bartiméus or Visio. These criteria ensured that professionals had sufficient experience to represent a broader group of practitioners working with the programme. Professionals involved in the design of the study and those participating in the advisory boards of the respective organisations were excluded. Professionals had an average of 1.83 years (SD = 8.28) of experience and implemented 7.50 programmes (SD = 7.50, range 1–25) annually. Professionals provided written informed consent before the study. The Scientific and Ethical Review Board (VCWE) of the Vrije Universiteit Amsterdam, the Netherlands (no. VCWE-2024-003) provided approval.
Procedure and data-analysis
Delphi round 1: semi-structured interviews
In the first round, independent researchers (university master students) conducted semi-structured interviews with the 12 professionals to explore their experiences with supporting individuals with ID to wear glasses. Semi-structured interview questions were guided by our research questions and developed by B.H., K.F., J.V.-L., and T.v.D. Interviews were structured around five themes: (1) the decision to provide glasses or not; (2) factors affecting the successful adaptation; (3) behavioural changes; (4) perspectives on the experiences of clients, caregivers, and parents/legal representatives; and (5) the Glasses Habituation Programme. Interviews were conducted via Microsoft Teams, as this was most convenient for the professionals. Interviews lasted between 43 min and 73 min (M = 60 min, SD = 10 min). Interviews were audio recorded and subsequently transcribed verbatim. Transcripts were checked for completeness and accuracy. Any identifying information was anonymised.
Delphi round 1: thematic analysis
Transcripts were analysed using reflexive thematic analysis (Braun et al., 2022). Researchers (n = 3; university master students) read the transcripts carefully to familiarise themselves with the data. A general coding approach was used by selecting areas of text and assigning them to specific codes in the software programme Atlas.ti version 24.1.1. Subsequently, researchers reviewed the codes and combined codes with similar meaning to create meaningful (sub)themes. Finally, researchers determined whether identified (sub)themes formed a coherent pattern and allowed for a reliable and valid interpretation of the data. Identified (sub)themes were reported to and discussed with another researcher (B.H.), who created a summary report of the results for the professionals. Intercoder reliability was not calculated as disagreements were solved by consensus.
Delphi round 2: feedback of professionals
The summary report was emailed to the 12 professionals. Professionals were asked for online feedback within 2 weeks. There was consensus among the 12 professionals regarding the report, and consequently, no revision was made. A flowchart of the Delphi study is presented in Supplemental Figure 1.
Results – single-subject multiple baseline study
Viewing behaviour
The NAP analyses for viewing behaviour indicated a significant decrease in the duration and frequency of attention to objects further away, with NAPreversed = 0.81, p = .028 and NAPreversed = 0.80, p = .031, respectively. No other significant differences in viewing behaviour from baseline to post-intervention emerged (see Figure 2 and Supplemental Table 1).
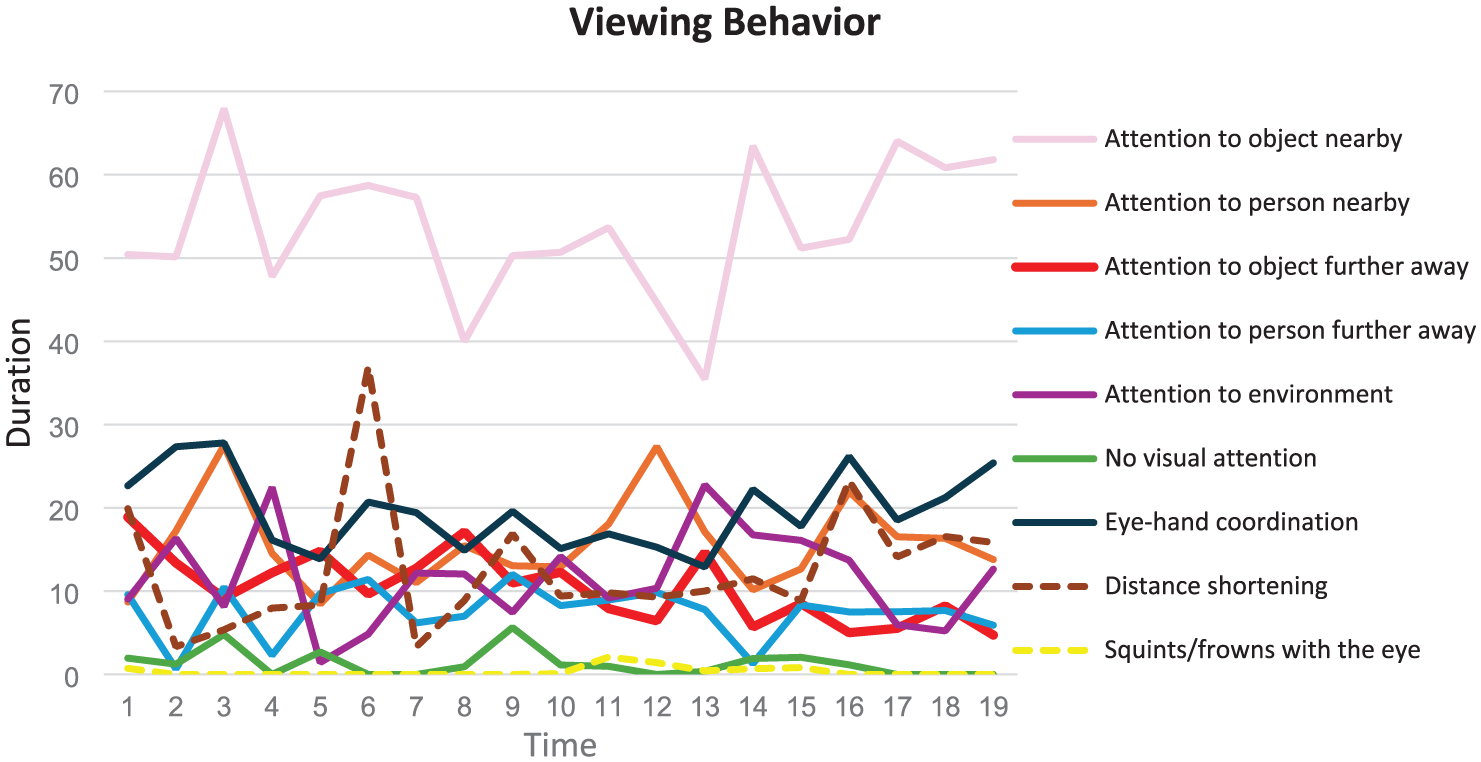
Changes in the duration viewing behaviours from baseline to post-intervention.
Adaptive functioning
Table 1 presents the raw and standard scores for the subdomains measuring adaptive functioning at baseline and post-intervention. The participant showed a 12-point increase in the raw subdomain score for personal (i.e., personal hygiene, eating habits and dressing skills) from baseline to post-intervention. Furthermore, the participant showed slightly better receptive communication from baseline to post-intervention, as evident by a 4-point increase in the raw subdomain score for receptive. There were no changes in expressive communication. Finally, there was a 1-point decrease in the raw subdomain score for interpersonal relationships from baseline to post-intervention.
Changes in adaptive functioning from baseline to post-intervention.
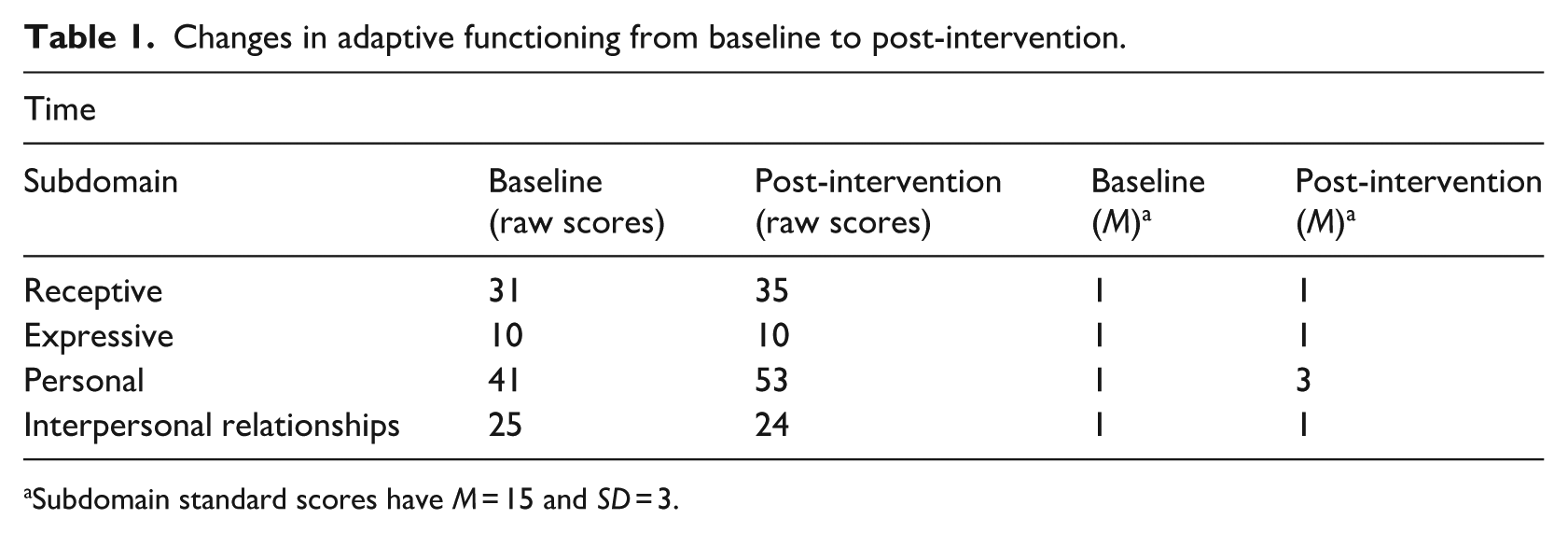
Subdomain standard scores have M = 15 and SD = 3.
Subjective well-being
Figure 3 presents the raw change for positive mood, negative mood, interest (subscale scores), and raw change score for subjective well-being (total score). The scores for positive mood, negative mood, interest and subjective well-being decreased over time, with 9, 7, 1, and 17 points, respectively, reflecting lower levels of subjective well-being at post-intervention compared to baseline.
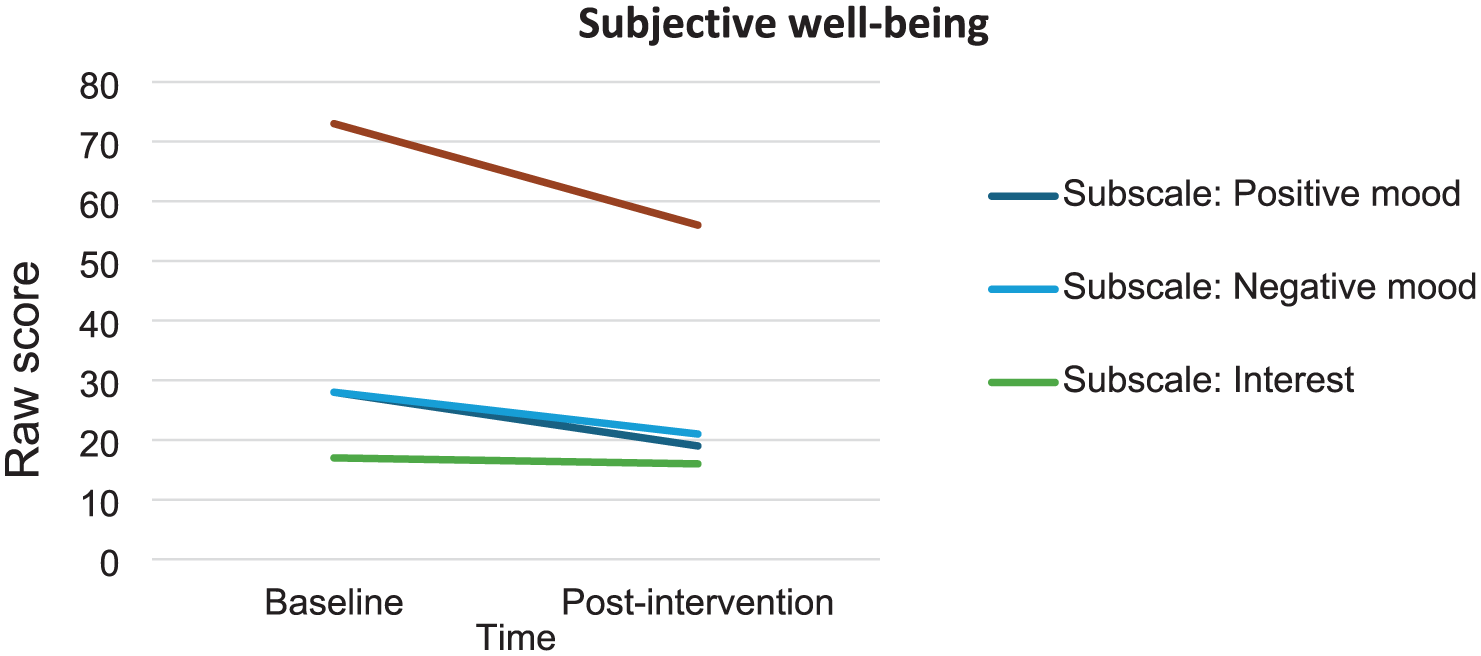
Changes in subjective well-being from baseline to post-intervention.
In-depth interviews
General experiences with wearing of glasses
Neither the father, nor the daily caregiver observed negative effects (e.g., stress, resistance) in the participant when he wore glasses; rather, it seemed a positive experience as the participant enjoyed the extra attention. Nevertheless, the participant needed time to adjust to wearing glasses. This was particularly evident at the beginning, when the participant put on and took off the glasses and needed reminders to put them back on. His father mentioned: I think that you need to be very straightforward if you want to teach Tony something. He cannot reason why it is important to wear glasses, you need to make clear that he needs to wear them, and then he will.
Effects on (viewing) behaviour
The caregiver observed changes in visual behaviour when the participant wore glasses when outdoors, but not indoors. She mentioned: When we sit at the table to play a game indoors, I don’t get the impression that he sees better or anything like that. But when he is outside walking, you can tell that he looks up and notices the stork. He points at things. But indoors, not at all. So, I do not think the glasses add any value for him indoors.
Tony’s father mentioned that he believed his son could see more, particularly in the distance: ‘He can walk very well, but he always walks as if he has to maintain his balance. And I think that has improved’. According to the caregiver and father, wearing glasses did not affect other visual behaviours, such as eye-hand coordination. Furthermore, the caregiver and father did not observe any changes in how activities were carried out, the support needed to undertake activities, the attention given to activities, or the types of activities initiated. Neither did the caregiver and father observe any intervention effects on the participant’s communication skills, interpersonal relationships, self-reliance, or mood. The caregiver did mention that there were many changes occurring within the participant’s home-care facility which significantly impacted him. It remained unclear in what way the participant was affected.
Experiences with the Glasses Habituation Programme
The caregiver reported positive experiences with the programme. The caregiver was stimulated to focus on how the participant perceived things and reacted to new stimuli, which she referred to as a learning experience. She mentioned that the programme requested extra effort, planning, and time, but that it was rewarding to contribute to the process. She mentioned that negative presumptions may exist: ‘When we started, everyone told me: “He will never do this, or he will stop”. But now, when I see that he puts on the glasses himself when he goes outside (sometimes we have to remind him), and he really looks around, I would definitely recommend it to other clients – just give it a try’. Tony’s father reported that he and his other children (who insisted on an eyecare examination) were glad that they started the programme. The father found the programme helpful because his son was now able to successfully wear glasses. During the course of the programme, he was attentive that his son wore glasses, but he did not find this burdensome.
Results – Delphi study
Glasses provision and wearing
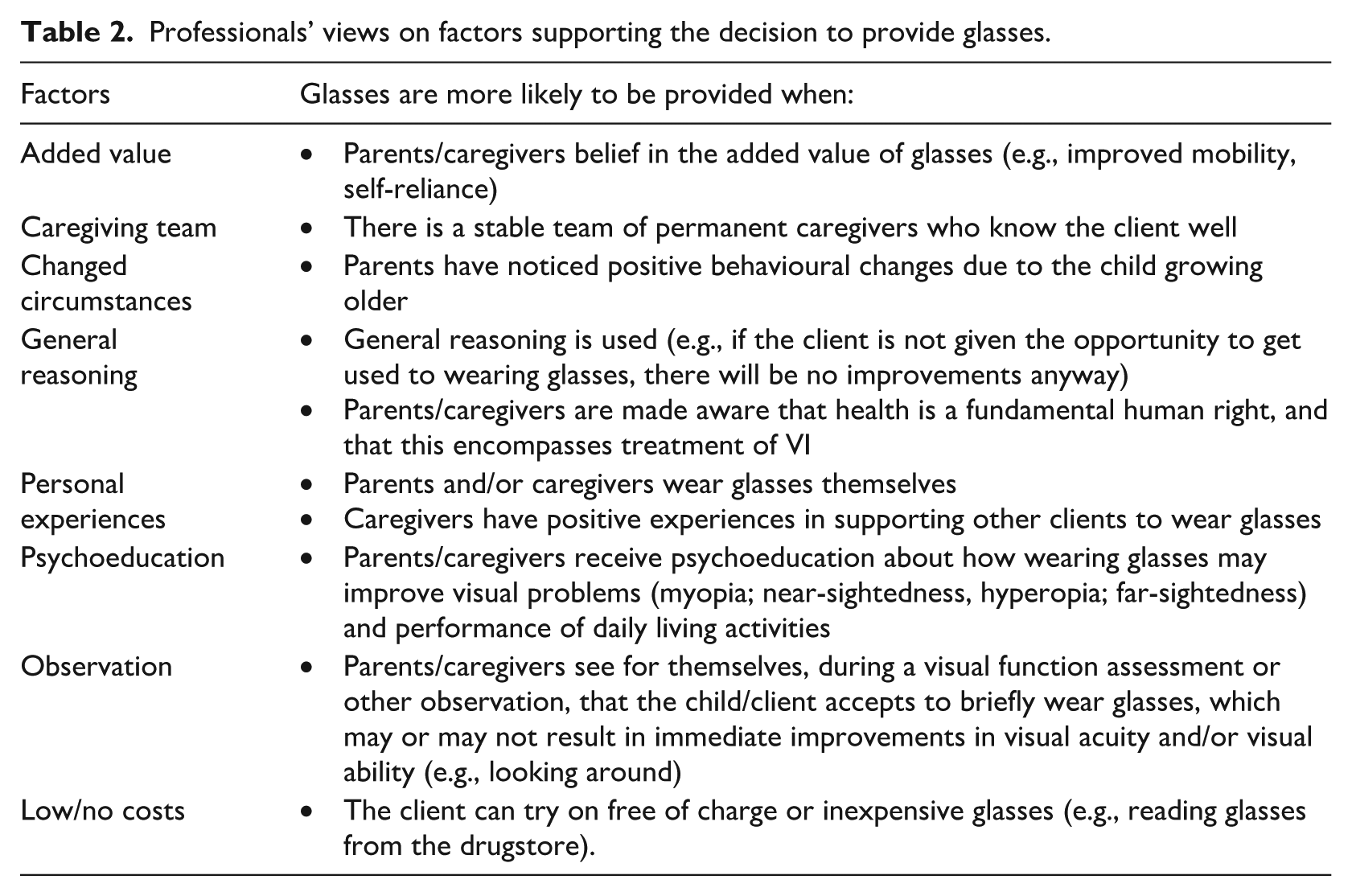
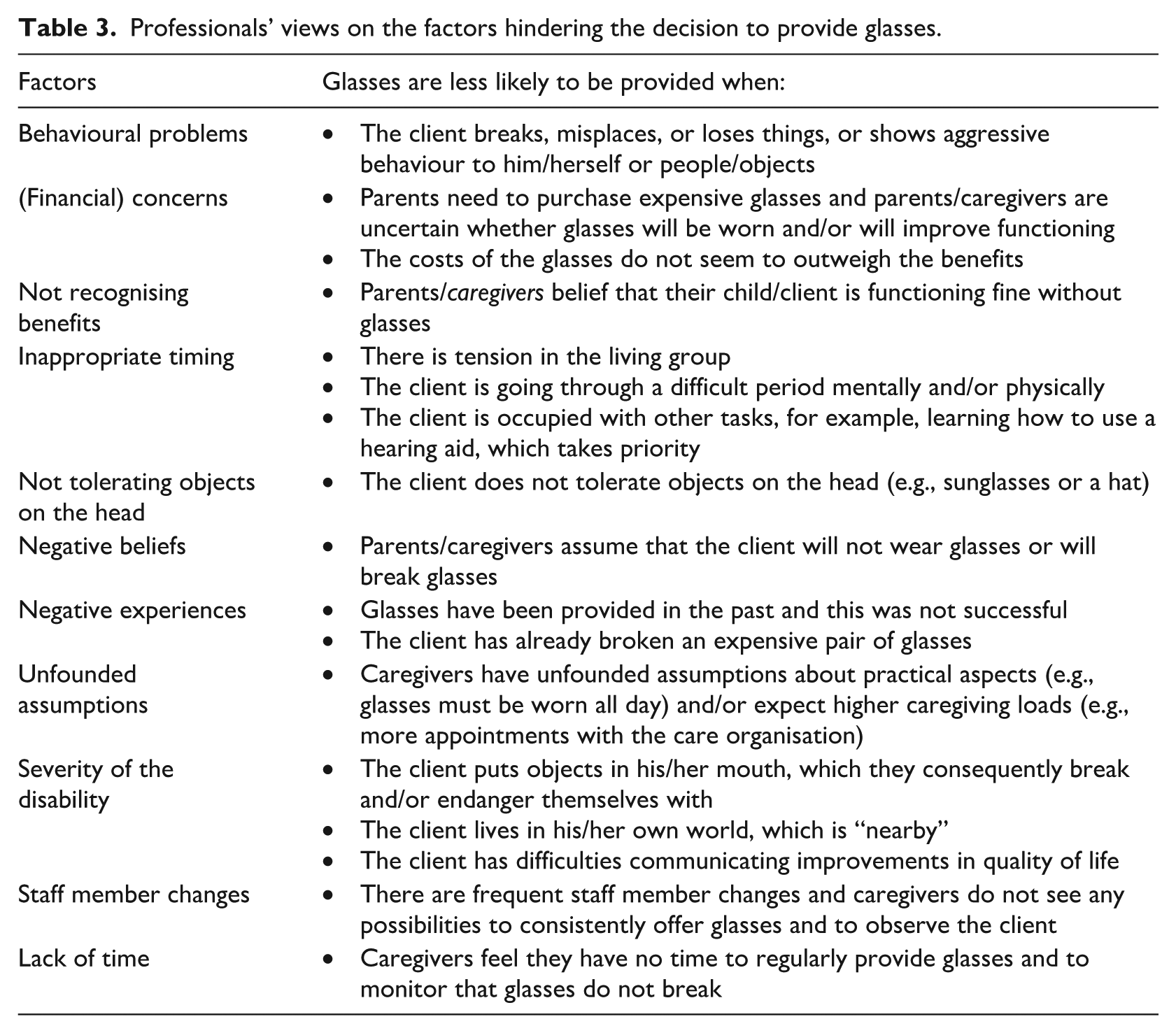
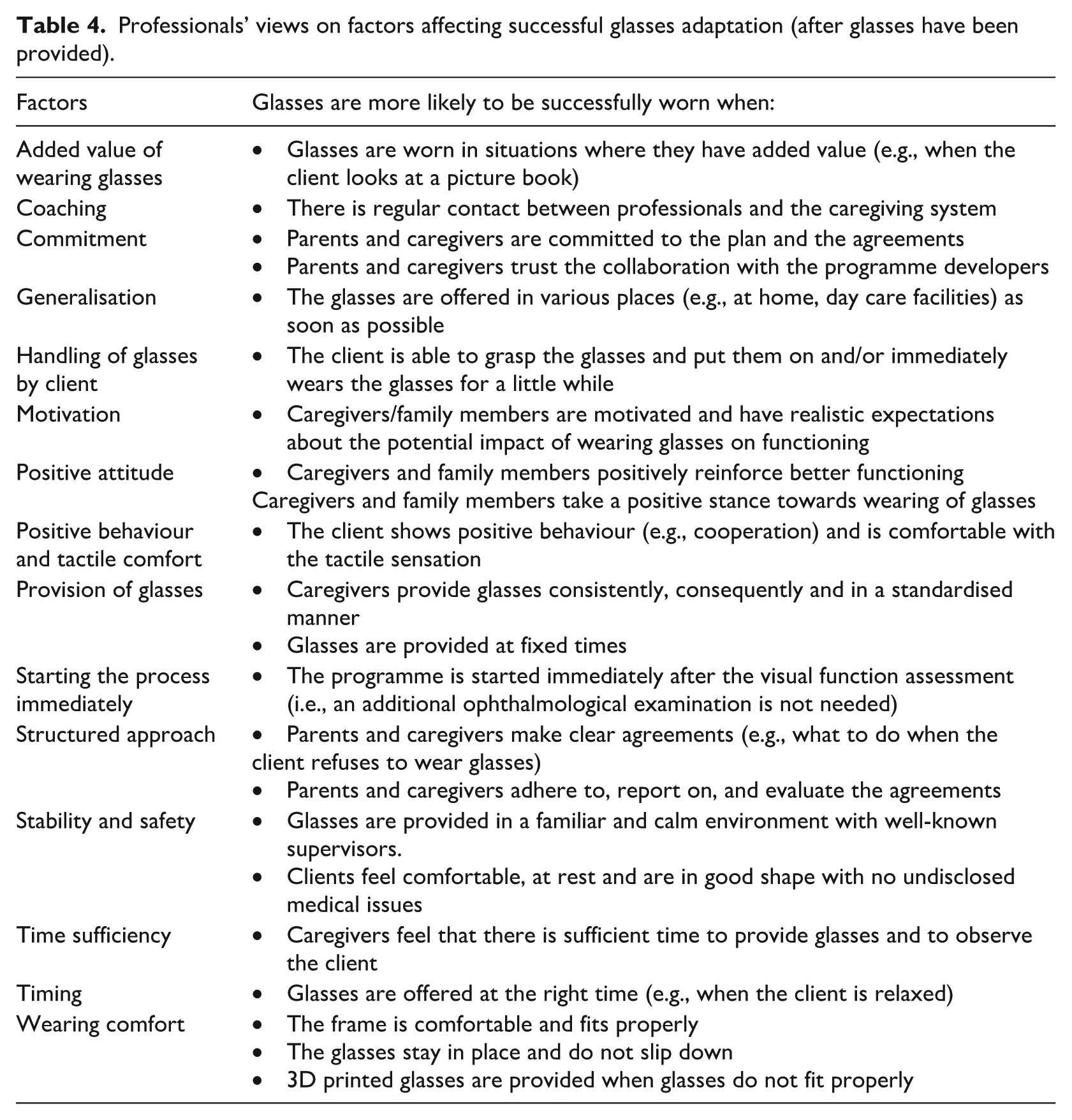
The Delphi consultation process resulted in the identification of key factors that support (Table 2) and hinder (Table 3) family members and/or caregivers in their decision to provide glasses. Professionals also identified key factors that impact adaptation to wearing glasses (see Table 4).
Professionals’ views on factors supporting the decision to provide glasses.
Professionals’ views on the factors hindering the decision to provide glasses.
Professionals’ views on factors affecting successful glasses adaptation (after glasses have been provided).
Perceived effects
Visual functioning
Professionals agreed on the observed positive effects of wearing glasses on visual functioning, which included (1) increased attention to the environment, activities, objects, and persons; (2) improved eye-hand coordination and/or eye-foot coordination (e.g., less stumbling, better able to load food onto a fork); (3) faster and better processing of visual information; (4) increased visual curiosity and alertness; and (5) decreased usage or no distance shorting (e.g., the client does not lean forward to see objects more clearly).
Social interactions
Professionals reached consensus on the observed effects of wearing glasses on social interactions, which included (1) increased (eye) contact with caregivers, (2) showing fewer demanding and clinging behaviours towards caregivers, (3) improved awareness of what is happening, and (4) more reciprocity in social situations.
Emotional state
Professionals agreed on the observed positive effects of wearing glasses on emotional state: feelings of pride, joy, happiness, calmness, and relaxation, as well as lower levels of anxiety, being friendlier towards others, and overall improvements in mood resulting from compliments.
Self-reliance
Professionals concurred on the observed positive effects of wearing glasses on self-reliance, which included (1) increased mobility and less falling and stumbling, (2) increased independence and autonomy (e.g., being able to pick up food with a fork, take something out of a cupboard), (3) increased ability to perform activities, (4) increased ability to communicate, for example, through pictograms, and (5) increased attention for personal hygiene and physical appearance.
Negative effects/disadvantages
Professionals agreed on the observed negative effects of wearing glasses on emotional state: increased tension, resistance, and/or frustration. Professionals reached consensus that glasses may cause irritation, necessitating a return to the optician for proper adjustment, which could be stressful for the client. Other disadvantages mentioned were broken or dirty glasses, the risk of losing glasses, investing in expensive glasses that may not be worn, additional demands on caregivers when the client regularly takes off glasses, and professionals needing to cope with preferences of parents and/or caregivers to slow down or speed up the process, which may not be possible.
Glasses Habituation Programme
Details on the strengths and areas for improvement in the Glasses Habituation Programme are reported in the Supplemental Materials.
Discussion
This paper reported on two studies: (1) a single-subject multiple baseline study that examined the effects of wearing distance glasses on viewing behaviour, adaptive functioning, and subjective well-being in a male adult with severe ID, and (2) a Delphi study that examined professionals’ views on wearing glasses by individuals with ID. Observations revealed that Tony showed less attention to objects further away while wearing glasses compared to not wearing glasses. Interviews with the caregiver and father showed that visual (related) behaviours of Tony improved. Caregiver-reported questionnaires revealed better adaptive functioning but decreased subjective well-being from baseline to post-intervention. Finally, professionals identified key factors in the provision and successful wearing of glasses and agreed on the potential positive effects in various areas of functioning. Professionals also identified strengths and areas for improvement in the Glasses Habituation Programme.
Observations indicated that wearing glasses indoors resulted in a decrease in the duration and frequency of attention to objects further away. Prior work shows that fixation duration is sensitive to the level of attention devoted to a stimulus (Henderson, 2007; Just & Carpenter, 1980), and that that fixation duration increases when visual processing is more demanding (He & McCarley, 2010; Negi & Mitra, 2020; Peterson et al., 2008). In line with this, we speculate that faster recognition of distant objects reduced the need for prolonged attention. However, this explanation remains tentative. Unexpectedly, we found no effects of wearing glasses on other viewing behaviours. Future studies might examine whether more effects emerge when participants wear glasses with stronger prescriptions. In-depth interviews with the caregiver and father revealed improvements in visual (related) behaviours. More specifically, Tony’s father noted that he was better able to maintain his balance while moving around. In addition, the caregiver noted Tony pointed at things and was more attentive to his outdoor surroundings. The caregiver reported no visual improvements when Tony wore glasses indoors. Outdoors, individuals are exposed to greater physical distances, whereas indoors the distances are typically shorter, making improvements in distance vision possibly less observable. Future studies may consider conducting both indoor and outdoor observations to better understand whether the impact of wearing distance glasses varies in different contexts.
With respect to adaptive functioning, the caregiver reported improvements in personal self-care (e.g., independently putting on shoes). These findings are in line with previous research showing that individuals with ID were more capable of performing basic activities when wearing glasses (McGlade et al., 2010). There were little improvements in receptive communication, a negligible decrease in the quality of interpersonal relations, and no changes in expressive communication. Similarly, interviews revealed that the caregiver and father noticed no improvements in these areas. Of note, communication skills and interpersonal relationships may be more difficult to change, and as such, intervention effects may require additional time to emerge. Future studies may explore the longer-term effects on adaptive functioning.
Surprisingly, the caregiver reported a decrease in subjective well-being over time for which reasons remain unknown. Interviews showed that there were no signs of stress or resistance when Tony wore glasses. The caregiver did mention that there were changes occurring in Tony’s home-care facility, which significantly impacted him. We therefore speculate that the decrease in subjective well-being may be explained by external stressors rather than wearing glasses. Needless to say, individuals with ID may have difficulties expressing feelings and emotions and it therefore remains important to monitor behaviour and non-verbal cues.
The Delphi study revealed various factors that make it more likely that parents and/or caregivers provide glasses, including (1) parents and/or caregivers being aware of the added value, (2) having positive experiences with wearing glasses, and (3) having indications, for example, through observations, that wearing glasses might be successful. Furthermore, it seems helpful when professionals use general reasoning and provide psychoeducation to inform parents and caregivers how wearing glasses may help to improve visual problems and one’s ability to perform daily living activities. Finally, parents and/or caregivers seem more willing to provide glasses when there is a stable caregiving team and when the child/client has shown positive behavioural changes.
The Delphi participants also identified hindering factors for glasses provision, which could be organised into client-, parent- and caregiver-, and system-related factors. Client-related factors included behavioural problems, not tolerating objects on the head, inappropriate timing, and severity of ID. Parent- and caregiver-related factors included financial concerns, unfounded assumptions, not recognising the benefits of glasses provision, and negative beliefs and experiences. System-related factors included staff member changes and a lack of time. We recommend targeting behavioural problems and intolerance to objects on the head before purchasing glasses as this may increase the likelihood of success. Furthermore, we encourage professionals to identify, clarify and challenge misunderstandings and incorrect beliefs. Finally, problems with staff member changes and lack of time may be further exacerbated by budget cuts, at least in the Netherlands. Therefore, it seems important to invest in and foster effective collaboration between professionals and families so that glasses can still be provided.
Delphi participants agreed on the factors that foster successful habituation to glasses, including glasses are being worn in situations where they can be beneficial and glasses fitting properly. It is out of the scope of this paper to discuss all factors; however, the relatively long list of factors shows that successful habituation depends on multiple processes and requires an individualised and collaborative approach. A next step could be to examine which factors are the strongest predictors of successful wearing, and whether factors vary across different populations, settings, and types of glasses.
Importantly, professionals agreed that wearing glasses has the potential to improve visual functioning, social interactions, emotional well-being, and self-reliance. RCTs are needed to confirm these perceptions and to test specific pathways through which glasses impact functioning (B. Hilberink et al., 2024). That is, whether effects are direct (e.g., improved vision leads to better social interactions) or indirect (e.g., better vision leads to greater confidence, which in turn improves social interactions). Of course, glasses habituation may come with challenges (e.g., broken glasses) and is not always successful. When negative effects are observed, immediate adjustments should be made to the programme. Habituation can always be resumed at a later stage, for example, after behavioural issues have been addressed.
Strengths and limitations
Strengths included the extensive and comprehensive approach to data collection, whereby both quantitative (i.e., observations, questionnaires) and qualitative (i.e., in-depth interviews) measurements were used. Nevertheless, several limitations should be noted. Initially, we aimed to utilise a randomised multiple baseline design with 12 participants, but recruitment difficulties resulted in participation of one individual. This limits generalisability and the ability to draw firm conclusions. International collaborations are important to test larger and more diverse datasets (e.g., participants wearing different types of glasses). We further note that viewing behaviour was observed 19 times during a semi-structured task. Although this approach enabled a systematic comparison, increased familiarity, preferences, and dislikes for the activities may have impacted behaviour. Similarly, preferences and dislikes for the activities may have impacted the participant’s viewing behaviour. In addition, a self-developed manual was used to observe viewing behaviour, which awaits validation. Furthermore, professionals’ beliefs about the importance of wearing glasses may have biased their responses. Triangulating findings with input from caregivers, parents, and other stakeholders will increase validity. Finally, future studies may benefit from measuring how often glasses are worn to examine a dose response between wearing glasses and intervention outcomes.
Conclusion
This study found that wearing glasses may result in promising improvements in visual behaviour and adaptive functioning. Findings, if replicated in larger RCTs with follow-up measures, point to the added value of glasses. Professionals agreed on the key factors that play a role in the provision and successful wearing of glasses. Importantly, professionals recalled positive effects of wearing glasses in various areas of functioning. This highlights the importance of supporting individuals with ID to wear glasses, for which programmes such as the Glasses Habituation Programme can be used. As the caregiver would say: ‘Just give it a try!’.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196251390486 – Supplemental material for Just give it a try: A single-subject multiple baseline study and a Delphi study to support individuals with moderate to profound intellectual disabilities to wear glasses
Supplemental material, sj-docx-1-jvi-10.1177_02646196251390486 for Just give it a try: A single-subject multiple baseline study and a Delphi study to support individuals with moderate to profound intellectual disabilities to wear glasses by AM Witte, B Hilberink, K Frederiks, J Verwey-Lakerveld, T van Duijvenboden and PS Sterkenburg in British Journal of Visual Impairment
Footnotes
Acknowledgements
We thank the participant, his father, and his caregiver for their time, effort, and contribution to this study. We thank Affect-Us, Alliade, Visio, and in particular, Anita Bies for their support. We thank all professionals from Bartiméus and Visio. We also thank the master students for their contribution.
CRediT author statement
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by ZonMw (fund number: 637005118) and Bartiméus Fund (fund number P00748):
Ethical Considerations
The Medical Ethical Review Board of the VUmc, The Netherlands approved the single-subject multiple baseline study (no. 2022.0603).
Consent to Participate
The caregiver provided written informed consent, and the participant’s father provided written informed consent for himself and his son. The Scientific and Ethical Review Board (VCWE) of the Vrije Universiteit Amsterdam, the Netherlands approved the Delphi study (no. VCWE-2024-003). Professionals provided written informed consent.
Data availability statement
Anonymised data is available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.