
Abstract
Quality of life (QoL) measures are often used to assess the effectiveness of services and interventions. For individuals living with vision impairment (VI) this is potentially problematic, given that QoL is characteristically assessed using instruments designed with non-VI norms and may not accurately represent issues specifically associated with VI. Hence, the authors designed an instrument (Vision Impaired Quality of Life [VIQoL]) tailored for adults living with VI. This article reports on VIQoL’s psychometric properties and outlines its utility for the VI sector. Principal Axis Factoring (PAF) was used to assess VIQoL’s construct validity, conducted on a combined dataset of adults with VI (n = 582), and adults without VI (n = 1992). To assess factor integrity, analyses were conducted on these groups separately. Reliability was assessed using Cronbach’s alpha. VIQoL display high construct validity and reliability. PAF analysis presented a two-factor solution: ‘functional confidence’ (items encompassing autonomy and frequent demands of life), and ‘personal flourishing’ (items related to affect and feeling). VIQoL is a valid and reliable tool for assessing QoL for people living with VI. It affords a basis for meaningful evaluations and insights into how differences in QoL are appraised by VI and non-VI populations; although factors were fundamentally similar, the importance of the two factors was reversed across the groups, which highlights the importance of condition-specific QoL measures and implies the need for research to assess other variables that can affect the QoL of people living with VI.
Introduction
Quality of life (QoL) is defined as an individual’s subjective appraisal of their affective, social, and physical functioning (Felce & Perry, 1995) that accounts for external factors such as environment or socioeconomic status (Karimi & Brazier, 2016; Skevington et al., 2004). These measures provide insight into an individual’s appraisal of their lived experience (Verdugo et al., 2005). Thus, areas of individual circumstance that might be enhanced can be elucidated; for example, if physical functioning and mental health facets of QoL are low, physical activity programmes can be encouraged (Ilhan et al., 2021).
Vision impairment (VI) affects factors contributing to QoL, such as social participation, work, and physical health (Brown & Barrett, 2011; Langelaan et al., 2007). However, to assess QoL in VI populations, health-related QoL measures (Langelaan et al., 2007), or vision-related QoL questionnaires (De Boer et al., 2004) that insufficiently reflect the potential impacts of VI are often employed.
Health-related quality of life (HRQoL) is typically defined as the subjective appraisal of wellbeing related to one’s health status, incorporating the effects of medical conditions and ongoing treatment (Ebrahim, 1995). Hence, HRQoL-measures may inadvertently assess physical health instead of QoL (Moons, 2004). Indeed, individuals with disabilities often report high QoL despite their health status (Ford et al., 2001; Tennant & McKenna, 1995). Therefore, using HRQoL-measures to assess QoL in those with VI is inappropriate; they emphasise VI and do not provide an accurate representation of overall functioning.
Similarly, visual status does not necessarily reflect how VI is experienced (Margolis et al., 2002) despite many vision-specific questionnaires incorporating visual status as a facet of QoL (Lamoureux & Pesudovs, 2011). For example, one item in the National Eye Institute-Visual Function Questionnaire (NEI-VFQ-25; National Eye Institute, 2000; for example, Choi et al., 2022) interrogates the difficulty experienced when reading ordinary print newspaper but does not consider the importance of reading to the individual in terms of their QoL. The implicit assumption that inability to function according to non-VI norms reduces QoL (Horner-Johnson et al., 2009) overlooks compensatory adaptations that may afford individuals with VI equitable experiences, such that their life is not as impeded as non-VI norms may lead one to believe (Lucas & Nguyen, 2022). That is, people living with disability can achieve positive QoL through alternative pathways, which implies the utility of a capabilities and functioning approach to understanding QoL (Alkire, 2016; Nussbaum & Sen, 1993).
Consequently, measures of QoL that do not specify how tasks may be completed may be more suitable for use with VI populations, thus allowing for greater inclusivity. As such, QoL measures for VI populations should focus on the ability to achieve a desired outcome, as opposed to the impairment itself; a position supported by research indicating non-visual factors to be stronger predictors of QoL than vision-specific items for those with VI (Trillo & Dickinson, 2012).
Generic QoL measures may not address characteristics that are (unproblematically) considered intrinsic for QoL, for example, managing tasks such as shopping (Jones et al., 2019) or confidence to do so (Tay et al., 2014), and may not account for the role of assistive devices such as a guide dog or white cane (Margolis et al., 2002) that can significantly enhance QoL (McIver et al., 2020). Notably, when evaluating the ability of generic measures to indicate QoL for those with VI, research suggests overall poorer performance (Tosh et al., 2012) and lower responsiveness to changes (Wiebe et al., 2003). Hence, the need for a measure that reflects what VI populations consider important for QoL; especially in relation to assessing the effectiveness of services and interventions.
Against this backdrop, Guide Dogs has developed an instrument, Vision Impaired Quality of Life (VIQoL), that reflects the experiences of people living with VI and what they identify as important in achieving positive quality of life (Supplemental Table 1). This study reports on the psychometric properties of VIQoL by using data from a large and nationally representative sample of people with and without VI.
Design and methodology
Measure development
Development of the VIQoL instrument was informed throughout by people living with VI and experts working in the field. Participants rated the degree to which an item reflected their everyday experiences and perceptions, on a 10-point numerical response scale; with 0 = none of the time and 10 = all of the time. A timeframe was followed by the item and examples where applicable; for example, ‘In the last month . . . I was able to manage everyday tasks for myself. For example, shopping, cleaning the house, completing forms’.
Participants
Non-VI (n = 1992) and VI (n = 582) adults above the age of 18 (1283 female, 1267 male) were recruited from the United Kingdom, of which 2262 were White British (see Supplemental Table 2 for participant characteristics).
Within the VI sample, 376 were Guide Dogs clients. This is representative of those in the United Kingdom with VI given that not all are affiliated with Guide Dogs (GD). Non-GD participants were recruited using quota sampling through an accredited third-party organisation. Having a non-VI sample provided a baseline for the measure. Alongside facilitating validation of the measures’ ability to assess QoL, testing with VI and non-VI can elucidate differences in the appraisal of QoL when functioning and capabilities becomes the focus.
The sample of 2574 participants was an acceptable sample size for factor analysis; over 1000 is considered excellent for producing results that are generalisable and reliable (Comrey & Lee, 2013). Moreover, a sample of over 1000 is comparable to other studies validating QoL measures for VI (e.g., Erickson et al., 2004; Vélez et al., 2023) such as the NEI VFQ-25 that has been extensively validated and used (Margolis et al., 2002).
Administration of vision impaired quality of life measure
VIQoL was formatted as a VI-accessible Qualtrics survey comprising 14 QoL items followed by demographic items. For those that requested it, the researchers completed the survey with the participant by telephone, adhering to standardised instructions.
Analytic procedure
Data analysis was conducted using SPSS version 26. Preliminary analysis assessed the suitability of the data for factor analysis. To substantiate factor extraction following PAF, parallel analysis, a method which compares the eigenvalues of the conducted analysis to eigenvalues from a randomly generated dataset of the same size was used (Lim & Jahng, 2019).
Construct validity
Factor analysis (principal axis factoring [PAF]), was performed on the VI and non-VI data combined to assess construct validity, factor solution integrity, and generalisability (Gruijters, 2019; Strickland, 2003). An oblique (promax) rotation was employed as this assumes factor correlation (Dancey & Reidy, 2014). Items were retained that had communalities greater than 0.2 (Child, 2006) as well as factor loading of 0.30 or greater (Tavakol & Wetzel, 2020).
Reliability
Cronbach’s alpha was calculated to assess internal consistency and reliability (Boateng et al., 2018). An alpha value of 0.7 is an acceptable threshold (Cortina, 1993). Differences between trimmed mean and mean were used as indicators of outlier effects (Pallant, 2016).
Ethics
Ethical approval was granted by the University of Bath Psychology Research Ethics Committee (PREC reference number: 22-006) and Guide Dogs’ Research Ethics Committee (REC code: HBS02-21).
Results
The majority (n = 2541) of participants completed the survey online; 33 participants with VI requested administration by telephone. Descriptive data for the 14 items for all 2574 participants are shown in Supplemental Table 3.
VIQoL reflected QoL in terms of two separate factors: ‘functional confidence’ and ‘personal flourishing’; below. These factors map onto functioning in relation to everyday experiences, and how people ‘feel’. Sub-scale scores range from 0 to 60 and 0 to 80, respectively; aggregate scores range from 0 to 140. Higher scores suggest higher QoL.
Construct validity
A spot-check of scatterplots between variables suggested linear relationships across the 14 items; meeting the assumption for factor analysis. Differences between trimmed mean and mean were no more than 0.27; cases were not excluded. Although 4% (n = 105) of the current sample straight-lined responses, the nature of QoL measures and subjectivity of perception means these responses can be valid. Given the low presence and possible validity of these instances, no exclusions occurred.
Principal axis factoring of combined data (VI and non-VI)
All 14 VIQoL items demonstrated a correlation coefficient of at least 0.3 with at least three other items, indicating suitable factorability. Bartlett’s test of sphericity was significant, X2 (91) = 19,761.229, p < .001, and the Kaiser-Meyer-Olkin measure of sample adequacy (KMO = 0.939) exceeded the recommended minimum of 0.6.
Two factors were extracted through consideration of initial eigenvalues greater than 1, corroborated by visual inspection of the scree plot. The first factor explained 46.53% of the variance, the second factor 6.27% (Supplemental Table 4). Parallel analysis confirmed the extraction of two factors (Supplemental Table 5).
The items ‘I have been physically and mentally healthy enough to do what I want to do’ and ‘I am able to remember things and think clearly’ cross loaded (Table 1). Subsequent factor analysis conducted with both items individually removed resulted in marginal changes to the total variance explained; a small decrease to 52.06%, and a small increase to 53.33%, respectively. Exclusion of both items also resulted in a small decrease to 52.07%. As these changes in explained variance were marginal, and preliminary literature reviews (e.g., Brunes et al., 2021) reported these items to be of importance to people with sight loss, both items were retained.
Principal axis factoring solution using a promax rotation with Kaiser normalisation: pattern matrix of combined dataset.
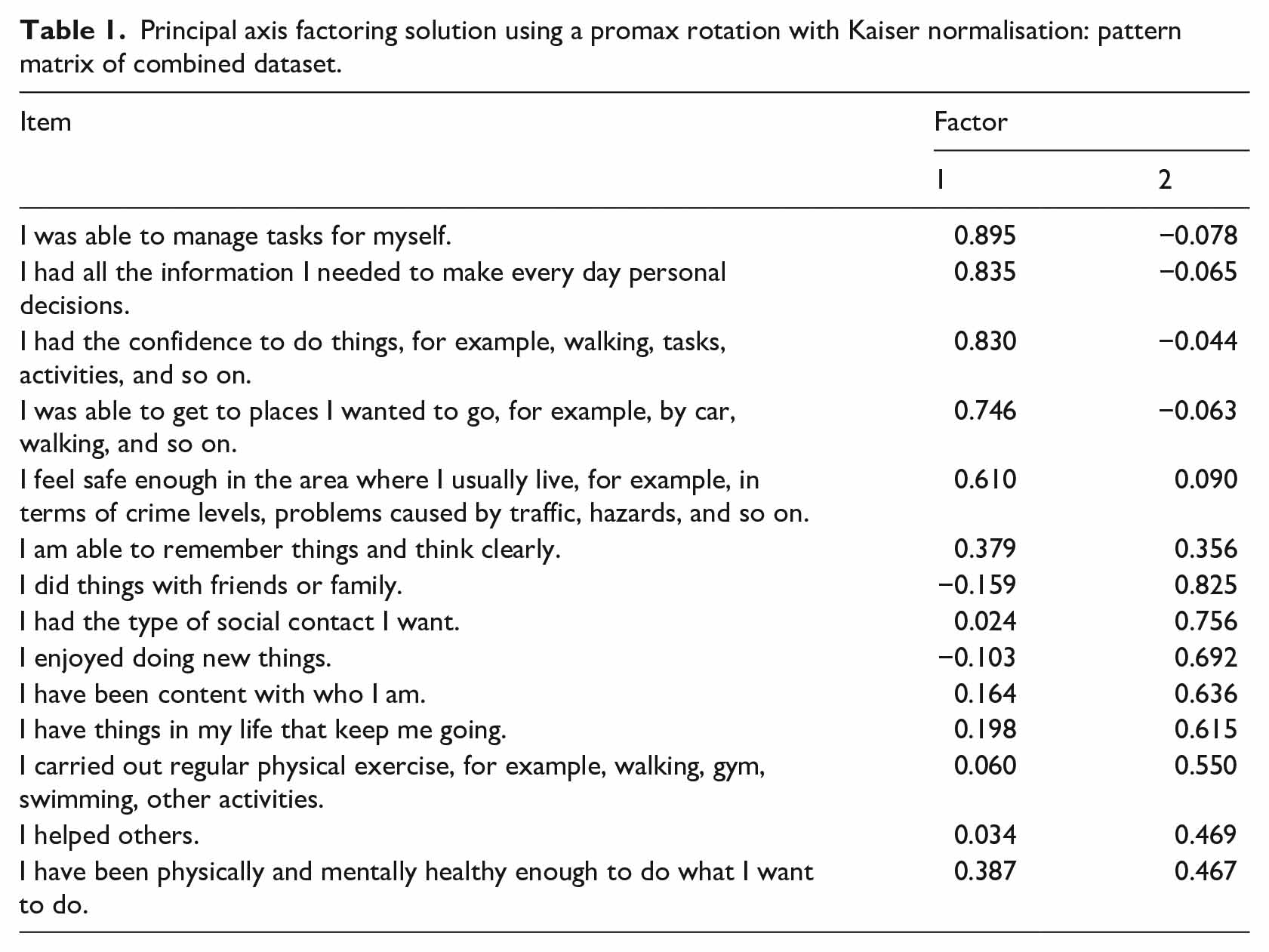
Factor 1 (‘functional confidence’) consists of six items. Items comprising this factor reflect autonomy and the individual’s physical and cognitive capabilities to carry out tasks; for example, ‘I was able to manage tasks for myself’. Factor 2 (‘personal flourishing’) consists of eight items. Items comprising this factor are associated with having purpose and meaning in life, for example, ‘I have things in my life that keep me going’; positive social interactions for example, ‘I had the type of social contact I want’; and engagement, for example, ‘I have been physically and mentally healthy enough to do what I want to do’.
Principal axis factoring – vision impaired sample only
All items demonstrated a correlation coefficient of at least 0.3 with at least three other items; Bartlett’s test of sphericity was significant, X2 (91) = 3756.359, p < .001; the Kaiser-Meyer-Olkin measure of sample adequacy (KMO = 0.911) exceeded 0.6. Three factors were initially extracted through consideration of initial eigenvalues greater than 1 (Supplemental Table 6). However, visual inspection of the scree plot was ambiguous, and parallel analysis indicated the presence of two factors (Supplemental Table 7).
Further inspection of the factor loadings indicated that the item ‘I carried out regular physical exercise’ did not have a loading greater than 0.3 onto any factor (Table 2). Given that sport participation has been suggested to be an important contributor to quality of life in individuals with VI (Ilhan et al., 2021), as well as improving aspects of autonomy, such as mobility and cognitive flexibility (Hackney et al., 2015; Hwang & Braun, 2015), this is an important item to consider. Subsequent factor analysis forced a two-factor solution. Although the total variance explained was lower (46.55% relative to 50.92%; Supplemental Table 8), the results were consistent with the combined dataset analysis; thus, the two-factor solution was favoured.
Principal axis factoring solution using a promax rotation with Kaiser normalisation: pattern matrix of VI dataset.
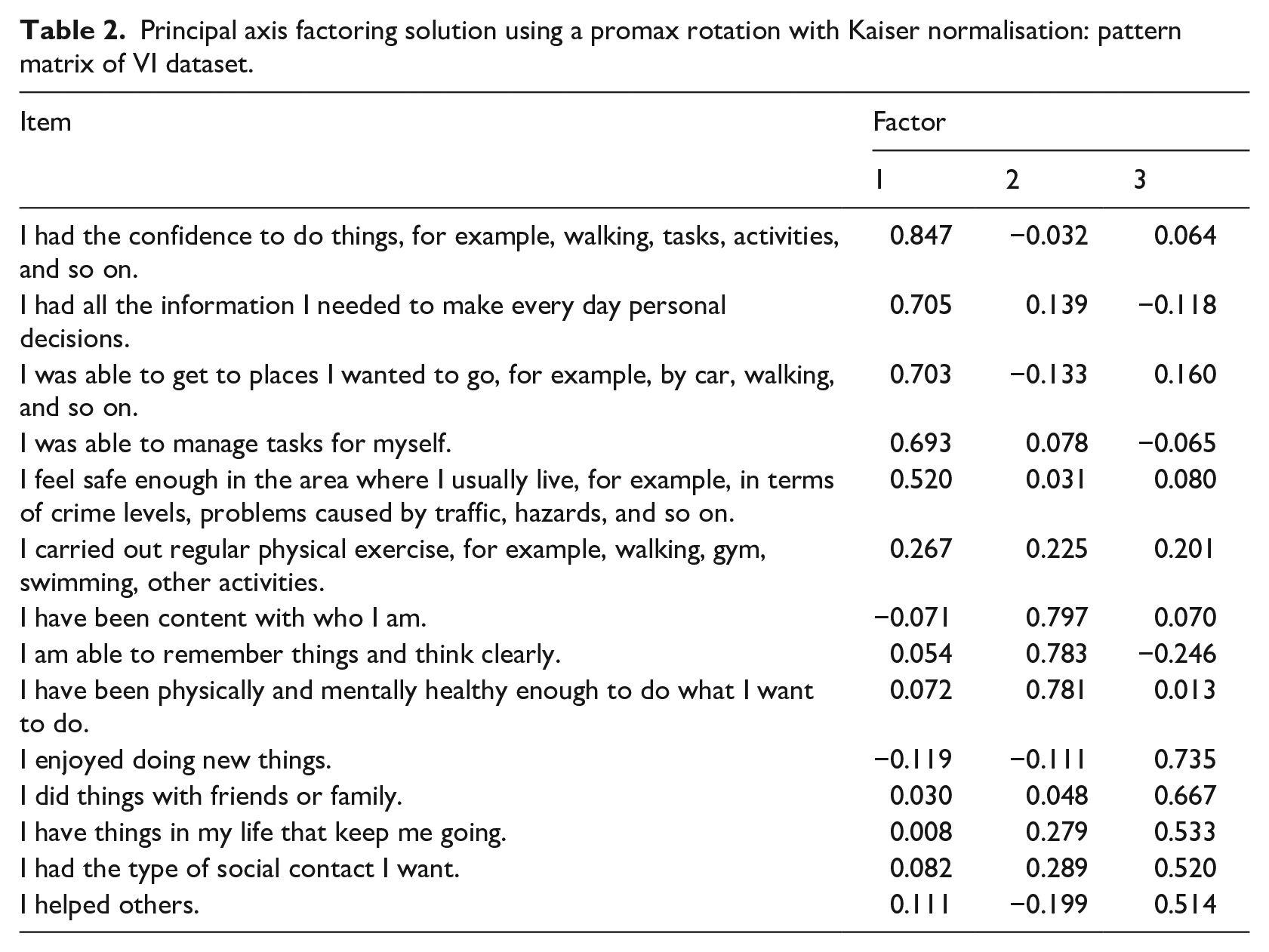
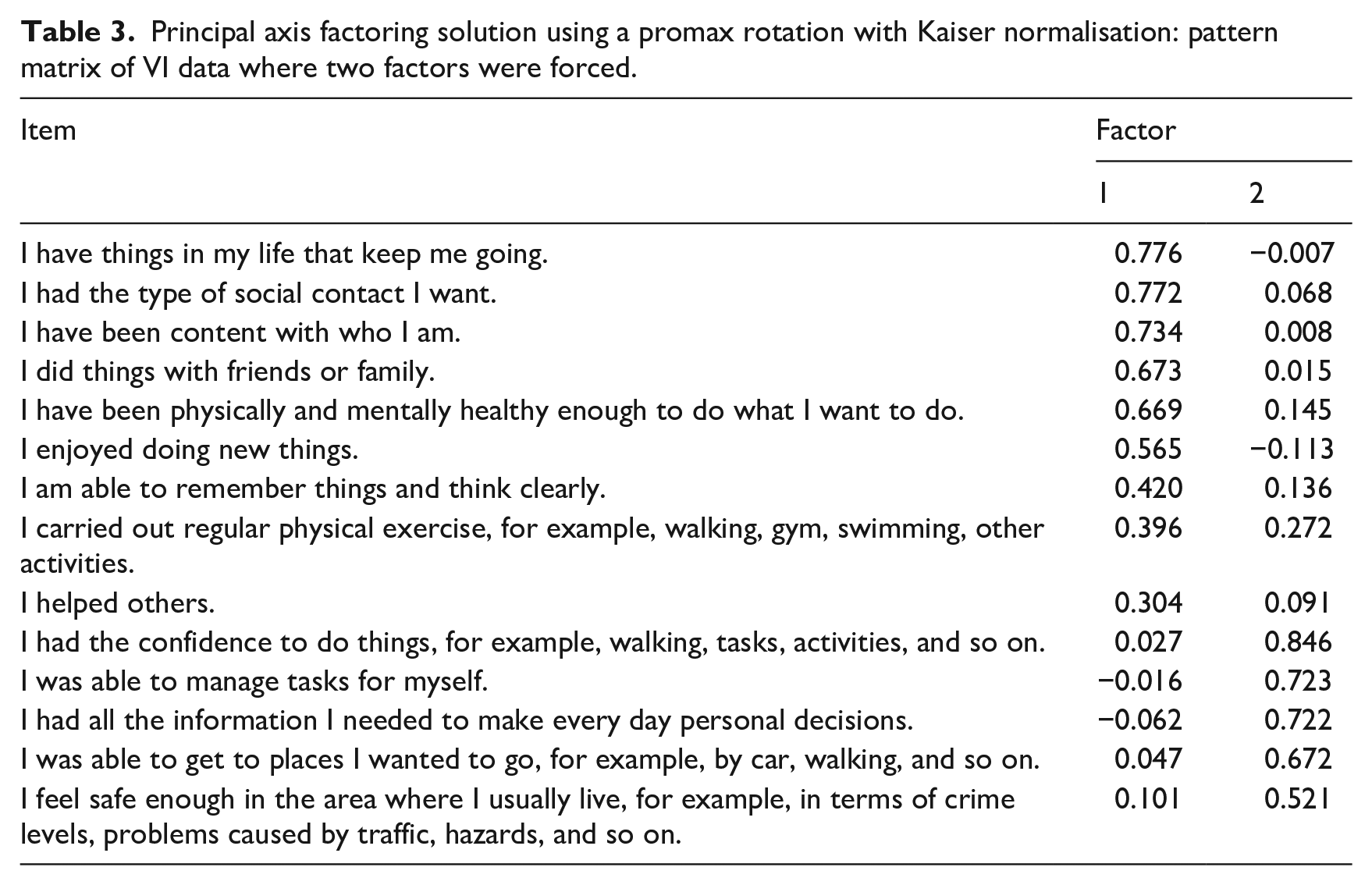
In contrast to the analysis of the combined VI/non-VI data, the ‘personal flourishing’ factor explained a greater amount of variance (41.45%) relative to the ‘functional confidence’ factor (5.11%) (Supplemental Table 8). In addition, the items ‘I am able to remember things and think clearly’ loaded onto the ‘personal flourishing’ factor instead of ‘functional confidence’ (Table 3).
Principal axis factoring solution using a promax rotation with Kaiser normalisation: pattern matrix of VI data where two factors were forced.
Principal axis factoring – non vision impaired sample only
Items demonstrated a correlation coefficient of at least 0.3 with at least three other items. Bartlett’s test of sphericity was significant, X2 (91) = 116,336.729, p < .001, and the Kaiser-Meyer-Olkin measure of sample adequacy (KMO = 0.941) exceeded the recommended minimum of 0.6. As such, the suitability of the data for factor analysis was confirmed.
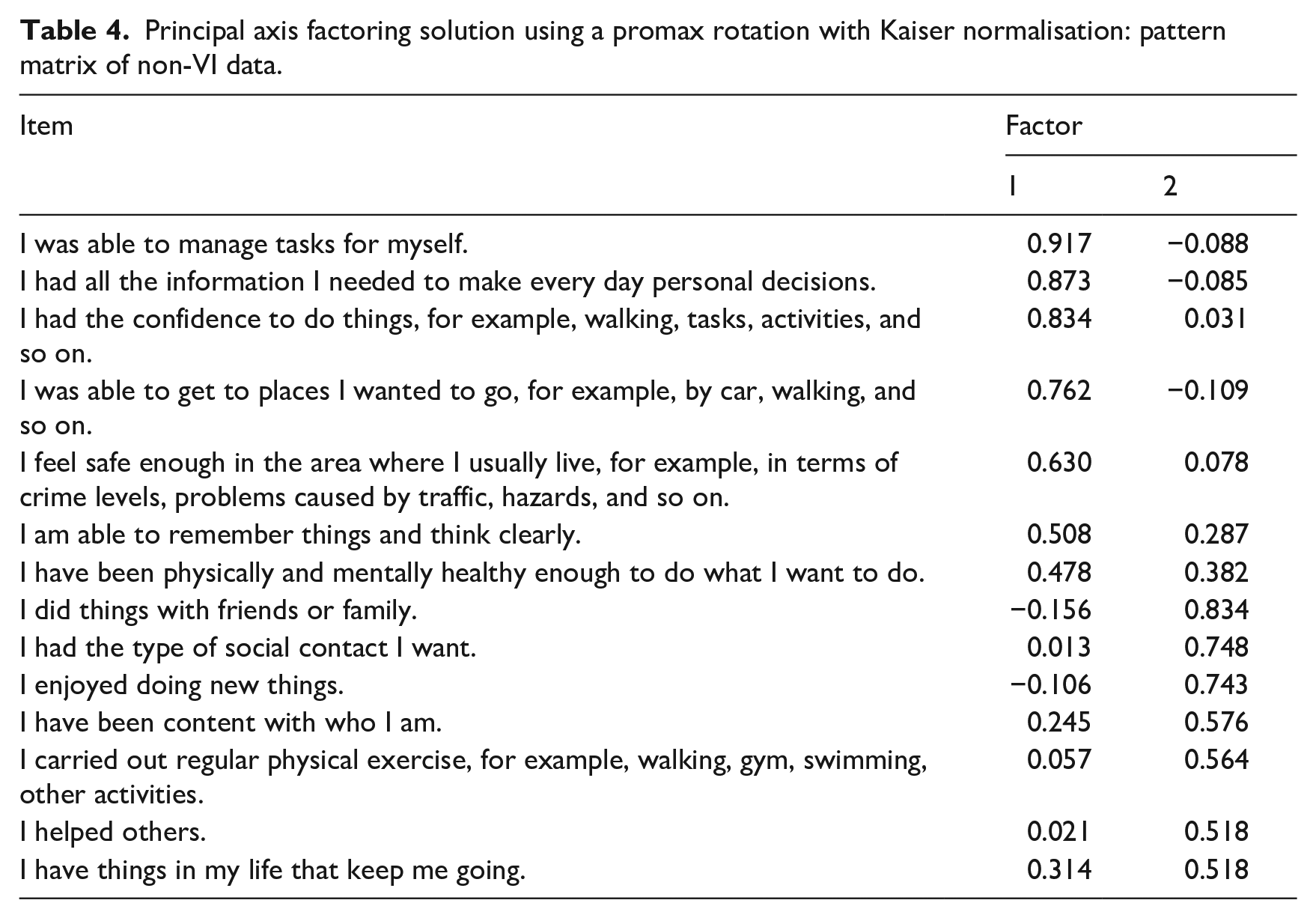
Two factors were extracted through consideration of initial eigenvalues greater than 1 (Supplemental Table 9), and inspection of the scree plot. Extraction of two factors was confirmed by parallel analysis (Supplemental Table 10). Two items cross loaded: ‘I have been physically and mentally healthy enough to do what I want’ and ‘I have things in my life that keep me going’ (Table 4). Each item cross loaded with values >0.4 on only one factor and were retained on the factor with a loading of >0.4. The two factors extracted were as per the combined dataset, except for the item ‘I have been physically and mentally healthy enough to do what I want’, which moved to ‘functional confidence’.
Principal axis factoring solution using a promax rotation with Kaiser normalisation: pattern matrix of non-VI data.
Factor integrity
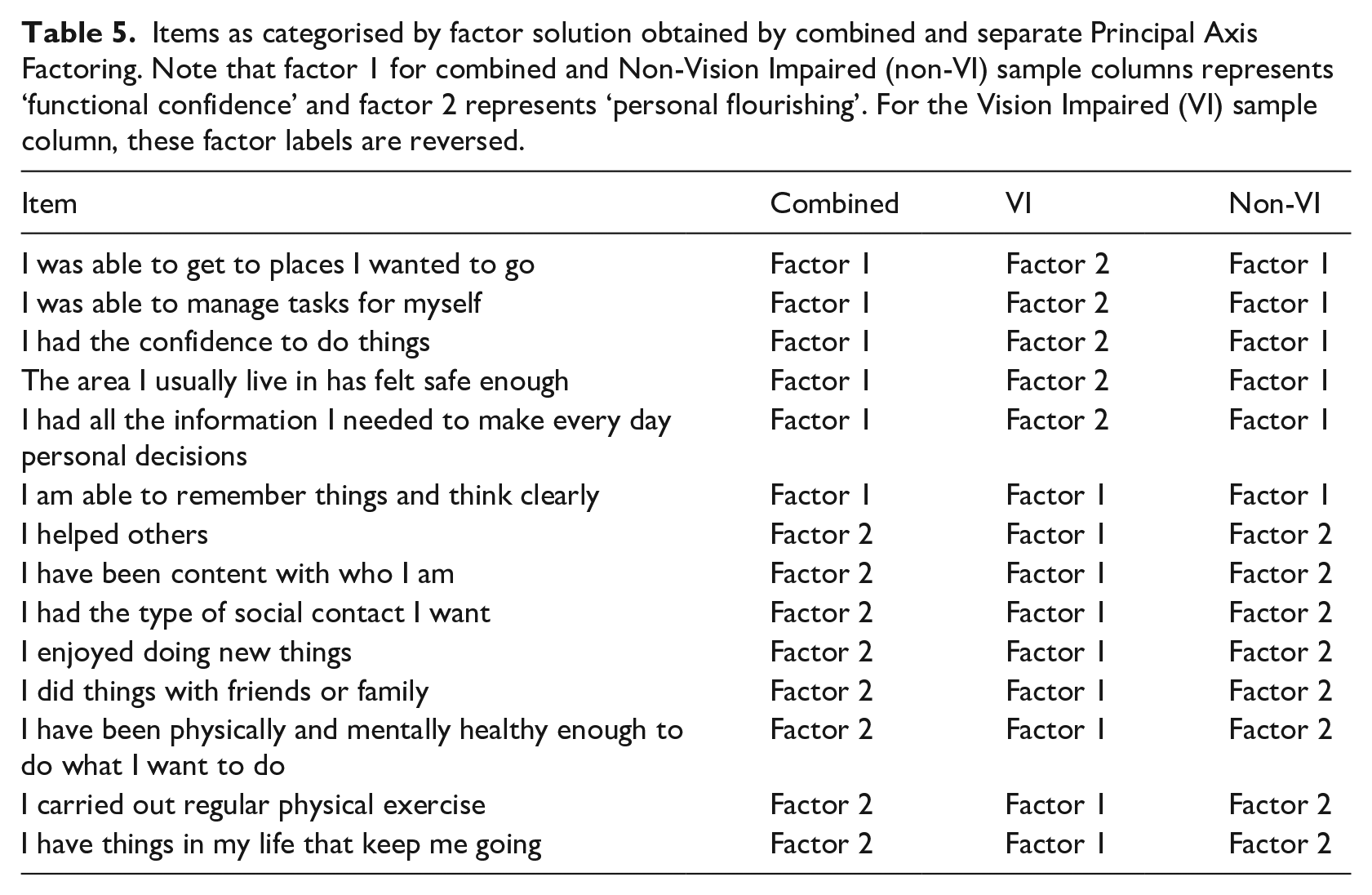
Overall, the integrity of the factors derived from the initial combined factor analysis remained (Table 5). Groupings remained consistent, with the exception of one item when the sample was analysed separately based on vision. As such, the two-factor solution derived from the combined data analyses was accepted.
Items as categorised by factor solution obtained by combined and separate Principal Axis Factoring. Note that factor 1 for combined and Non-Vision Impaired (non-VI) sample columns represents ‘functional confidence’ and factor 2 represents ‘personal flourishing’. For the Vision Impaired (VI) sample column, these factor labels are reversed.
Factor reliability
As per the combined dataset results, further principal axis factoring was conducted on each of the factors using a promax rotation to validate the two-factor solution. Irrespective of whether the ‘I have been physically and mentally healthy enough to do what I want’ item was in the ‘functional confidence’ or ‘personal flourishing’ category, each analysis of the separate factors resulted in a one-factor solution and no-subfactors were extracted. Hence, factor reliability is indicated.
Internal consistency
For the combined data, Cronbach’s alpha for both ‘functional confidence’ (α = .88) and ‘personal flourishing’ (α = .87) were between 0.7 and 0.95; that is, high reliability. Deletion of the item ‘I helped others’ led to an increase in alpha of .001 which was considered negligible, thus all items were retained.
Discussion
This study conducted validation of VIQoL measure with a sample of 2574 participants consisting of VI and non-VI individuals. As VIQoL is a newly developed measure, an approach was adopted to assess construct validity through exploratory factor analysis. A two-factor solution was identified that explained 52.8% of variance. Factor integrity was demonstrated when further PAF analyses were conducted with the VI and non-VI groups separately. Factor reliability was also determined by subsequent analyses on each of the extracted components. VIQoL yielded good internal consistency. The current validation study finds VIQoL to be a promising measure of QoL for individuals with VI.
The two factors extracted from VIQoL were termed ‘functional confidence’ and ‘personal flourishing’. These reflect existing literature for VI and QoL, broadly mapping onto how people are functioning in relation to their everyday experiences. The first factor of ‘functional confidence’ is defined as the respondents’ beliefs in their ability to manage on an intrapersonal level, implicating autonomy and ability to function as one would like, for example, ‘I had the confidence to do things’ and ‘I was able to manage tasks for myself’. As items are not vision-specific, this factor evaluates an individual’s perception of how well they navigate everyday life despite VI and implies the importance of self-efficacy in QoL (Brunes et al., 2021).
The item ‘I have been physically and mentally healthy enough to do what I want to do’ cross loaded onto both factors and loaded differently based on vision. This item was constructed to enable a holistic appraisal whereby distinction between physical and mental health was not forced. Interestingly, this item is accommodated within the factor of ‘personal flourishing’. Comparatively, ‘functional confidence’ comprises ostensibly cognitive aspects. Thus, it is important to remain circumspect regarding how respondents orientate to broad concepts such as ‘mental health’ and their relationship with lower level constructs that otherwise imply a distance between cognition, affect, and behaviour.
The second factor, ‘personal flourishing’, reflects themes identified in the Flourishing Scale (Diener et al., 2010); an 8-item measure designed to assess subjective wellbeing. The Flourishing Scale captures aspects of purpose and meaning, self-acceptance, and relationships, as observed in VIQoL items ‘I have been content with who I am’ and ‘I had the type of social contact I want’. Evidence suggests that high flourishing is associated with better health outcomes (Duggan et al., 2016). Specifically, high flourishing has been associated with decreased likelihood of impairments in instrumental activities of daily living, such as basic self-care tasks as well as enhanced overall functioning apropos managing chronic disease and lower life-course disability (Laditka & Laditka, 2018).
In terms of VI-specific QoL research, non-visual factors appear to be stronger predictors of QoL than visual factors (Trillo & Dickinson, 2012). ‘Personal flourishing’ reflects this as items interrogate personal growth and wellbeing rather than physical abilities per se. Given these areas lie within a broad definition of QoL, ‘personal flourishing’ is an appropriate construct within measures of QoL.
When conducting further PAF to assess integrity of factors for the VI and non-VI samples separately, the factor that accounted for most variance differed. For the non-VI, ‘functional confidence’ accounted for more variance, while for VI it was ‘personal flourishing’. This may implicate different priorities between the two groups, suggesting that a focus on vision-related factors and physical ability are not appropriate when exploring QoL for people living with VI; specifically regarding physical and mental health where non-visual factors are highly influential (Trillo & Dickinson, 2012).
Previous research using generic QoL measures where individuals with VI tend to score lower may be due to differences in how QoL is appraised compared to typical norms. Consequently, the present findings serve as a model for how QoL might be assessed for other conditions such as hearing loss; where specific QoL measures remain predominantly grounded in hearing ability (e.g., Servidoni & de Oliveira Conterno, 2018; Umansky et al., 2011).
Past literature suggests a discrepancy in perceived importance of certain QoL dimensions observed between younger and older people; the former considered mental health as more important while, for the latter, it was independence and autonomy (Ratcliffe et al., 2017). However, the variance between groups is unlikely to be attributable to differences in the age of participants; the mean age of VI group participants was 52.2 years and non-VI was 48.4 years in this study.
Although the sample used in this study is large, the demographics of the participants are skewed. Thus, the present findings may not be. Specifically, the general skew towards older age may affect items related to cognition and sociability. Age-related cognitive decline is a normal process (Lenehan et al., 2015), as is decreasing sociability (Singh & Misra, 2009). In addition, the sample is predominantly white British; past research has indicated differences in dimensions and how they are prioritised in QoL across cultures (Kagawa-Singer et al., 2010). As such, further testing may be needed to assess the validity of VIQoL in different populations.
The results of this validation study suggest VIQoL to be a valid and reliable tool to assess QoL in individuals with VI. The UK Vision Strategy has recently highlighted the need for eye care to be more consistent overall (Bosanquet & Mehta, 2020), and having a standardised and applicable measure to assess the impact of interventions is one way to achieve this consistency. While VIQoL was designed for use with clients of Guide Dogs to assess their ongoing wellbeing, with the effectiveness of Guide Dogs’ services in mind, VIQoL has potential application across vision-related intervention research. The VIQoL instrument is tailored for VI and, given its validity and reliability, can provide a comparable means to assess effectiveness for all vision-related interventions beyond Guide Dogs. VIQoL is an appropriate measure to assess QoL, as well as providing a foundation for future research to evaluate effectiveness of related interventions.
Future research
To determine long-term stability of outcome responses, test–retest reliability should be assessed; the instrument would be applied to the same population across a timeframe of 6 months to 1 year. This period reflects typical service review points for VI organisations. Moreover, for older people with VI, for example, aged above 65, associations between QoL and age-related declines in mobility and cognition may become apparent. Furthermore, 33 (5.6%) VI respondents completed the instrument by phone. The impact of the mode of survey administration should be investigated to determine any effect on responses.
Demographic factors such as marital (Bookwala, 2011) and employment status (Lund & Cmar, 2019) should also be considered in relation to VIQoL, as these may affect QoL constructs. There may be utility for VIQoL beyond a VI population; future work could explore VIQoL in relation to other health-related conditions that may affect QoL. Specifically, future work could consider differences in how facets of QoL are prioritised between a target group and a national representative sample; as implicated by the present findings, VI and non-VI individuals may appraise areas of QoL differently. Consequently, it may be of interest how and why the weight of specific QoL composites may shift as well as how interventions can be tailored to these needs.
Conclusion
This study conducted a validation of the VIQoL instrument, designed to explore QoL for adults living with VI. A two-factor solution was found, with the factors defined as ‘functional confidence’ and ‘personal flourishing’. Factor integrity was observed through separate factor analysis conducted on the VI and non-VI sample only. This also revealed differences in how QoL is construed between these populations. Current findings suggest VIQoL is a valid and reliable tool to assess QoL for people living with VI.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196231203367 – Supplemental material for Validation of a quality of life measure (VIQoL) for adults living with vision impairment
Supplemental material, sj-docx-1-jvi-10.1177_02646196231203367 for Validation of a quality of life measure (VIQoL) for adults living with vision impairment by Hoi Ying Cheng, John Fellenor, Ffion Parry and Michael Proulx in British Journal of Visual Impairment
Supplemental Material
sj-docx-2-jvi-10.1177_02646196231203367 – Supplemental material for Validation of a quality of life measure (VIQoL) for adults living with vision impairment
Supplemental material, sj-docx-2-jvi-10.1177_02646196231203367 for Validation of a quality of life measure (VIQoL) for adults living with vision impairment by Hoi Ying Cheng, John Fellenor, Ffion Parry and Michael Proulx in British Journal of Visual Impairment
Supplemental Material
sj-docx-3-jvi-10.1177_02646196231203367 – Supplemental material for Validation of a quality of life measure (VIQoL) for adults living with vision impairment
Supplemental material, sj-docx-3-jvi-10.1177_02646196231203367 for Validation of a quality of life measure (VIQoL) for adults living with vision impairment by Hoi Ying Cheng, John Fellenor, Ffion Parry and Michael Proulx in British Journal of Visual Impairment
Supplemental Material
sj-docx-4-jvi-10.1177_02646196231203367 – Supplemental material for Validation of a quality of life measure (VIQoL) for adults living with vision impairment
Supplemental material, sj-docx-4-jvi-10.1177_02646196231203367 for Validation of a quality of life measure (VIQoL) for adults living with vision impairment by Hoi Ying Cheng, John Fellenor, Ffion Parry and Michael Proulx in British Journal of Visual Impairment
Supplemental Material
sj-docx-5-jvi-10.1177_02646196231203367 – Supplemental material for Validation of a quality of life measure (VIQoL) for adults living with vision impairment
Supplemental material, sj-docx-5-jvi-10.1177_02646196231203367 for Validation of a quality of life measure (VIQoL) for adults living with vision impairment by Hoi Ying Cheng, John Fellenor, Ffion Parry and Michael Proulx in British Journal of Visual Impairment
Supplemental Material
sj-docx-6-jvi-10.1177_02646196231203367 – Supplemental material for Validation of a quality of life measure (VIQoL) for adults living with vision impairment
Supplemental material, sj-docx-6-jvi-10.1177_02646196231203367 for Validation of a quality of life measure (VIQoL) for adults living with vision impairment by Hoi Ying Cheng, John Fellenor, Ffion Parry and Michael Proulx in British Journal of Visual Impairment
Footnotes
Acknowledgements
Commissioning of the work depended on the support and guidance of Guide Dogs Research Planning Group and the Research Ethics Committee. In addition, development and piloting of materials relied on the support of Guide Dogs’ Accessibility Team and numerous Guide Dogs service users. We are also thankful to the Department of Psychology at the University of Bath for the help and support in laying the groundwork for this project. We are extremely grateful for the support of all these individuals, without whom the work could not have been completed.
Data availability
Restrictions apply to the availability of these data. Data were obtained from Guide Dogs UK. Guide Dogs do not routinely release raw data but will allow its use within high quality research proposals that have been approved under Guide Dogs research governance process. Requests to access the datasets should be directed to research@guidedogs.org.uk.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from Guide Dogs. Michael. J. Proulx was supported by CAMERA 2.0, the EPSRC Centre for the Analysis of Motion, Entertainment Research and Applications (EPSRC grant EP/T022523/1). MJP is also a Research Scientist at Meta Reality Labs Research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.