
Abstract
The presence of childhood vision impairment has cascading effects on educational provision and global development across cognitive, physical, and mental health domains. Effective, appropriate, and targeted support in education is legislated across the United Kingdom, influenced by the ‘access to learning, learning to access’ model. Despite reasonable adjustment and specialist provision legislature, anecdotal parental reports suggest inconsistent and insufficient provision culminating in poor physical and mental health outcomes for school-aged children and young people with vision impairment in the United Kingdom. This pilot study aimed to evaluate the perceived effectiveness of provisional arrangement/specialist support from a parental viewpoint. We examined the questionnaire responses of parents/caregivers of children and young people with vision impairment to harness their views regarding provisional entitlement. An online questionnaire was developed in collaboration with parents/caregivers of children with vision impairment who identified a distinct need for research in this field. Forty-six parents/caregivers completed the questionnaire. Most parents reported their child accessing specialised provision; however, frequency of provision and qualification of staff administering provision was inconsistent. Parents reported that available provision more negatively impacted their child’s mental health, and resultingly, most parents lacked confidence in the arrangements their child received. We concluded that parental perception of provisional arrangements is seemingly influenced by the quality of the team supporting their child in educational domains. Future work triangulating parental views with that of the children receiving the support, and support staff, is needed for corroboration.
Introduction
Inconsistency in provision for children and young people with vision impairment (CYPVI) in the United Kingdom is relatively well-documented (Hewett et al., 2022; Hogg et al., 2017). The recent publication of the Curriculum Framework for Children with Vision Impairment (Hewett et al., 2022) is a direct response to detailing the range and specific types of holistic provision that CYPVI need, and are entitled to, under relevant UK legislation (SEND CoP; Department for Education & Department of Health [DfE & DoH], 2014; Equality Act; UK Government, 2010), and the broader Convention on the Rights of Persons with Disabilities (United Nations, 2006). Despite the curriculum framework detailing the types of support and identifying those responsible for providing support, it remains in infancy, meaning many CYPVI in the United Kingdom continue to be ostracised from holistic provision for various personal and political reasons, that is, budget cuts to local authorities, lack of centralised funding, and provision based on a postcode lottery (Ofsted, 2021).
The presence of childhood vision impairment has cascading effects on different domains of development including but not exclusive to; mobility (moving around physical space), orientation (knowing one’s place in space), and independent living skills (feeding, cleaning, dressing, and social skills), mental health, cognition, and attainment. The Equality Act (UK Government, 2010), Special Educational Needs and Disabilities Code of Practice England (DfE & DoH, 2014), and equivalent versions across the devolved nations of the United Kingdom (Special Educational Needs and Disability Act (Northern Ireland Assembly, 2016); Additional Learning Needs and Educational Tribunal (Wales) Act (Welsh Government, 2021); Additional Support for Learning Code of Practice (Scotland), (Scottish Parliament, 2017), endorse the principle of ‘reasonable adjustment’ for educational and public areas to ‘reduce the disadvantage’ for persons with disability. In the context of the current article, the project will explore reasonable adjustment within the context of educational settings, including mainstream and specialist school environments.
In the educational context, reasonable adjustment is defined as ‘providing additional support and services to ensure CYP are not disadvantaged compared with their peers’ (SEND CoP; DfE & DoH, 2014). The access to learning/learning to access model (McLinden et al., 2016) and the curriculum framework for vision impairment (Hewett et al., 2022) echoes the sentiment. This means that provision ranging from workforce support (i.e., specialist teachers, habilitation specialists, teaching/learning assistants) to materials in alternative/accessible formats should be provided to the CYPVI to support their learning in educational spaces.
The quality of support staff (i.e., qualified teacher for the visually impaired [QTVI] habilitation professionals [assistants or specialists], teaching assistants (TAs)/learning support assistants) is essential for understanding the various needs of CYPVI in addition to adapting and sourcing essential materials to support engagement in school subjects. The mandatory role of the QTVI should not be overlooked here. As reported by McLinden et al. (2016), the integral role of the QTVI is to ensure appropriate curriculum design and delivery in addition to reducing barriers for curriculum access in school. While not yet mandatory, the work of the habilitation professional oversees CYPVI development across all domains, that is, school, home, and public settings. All supporting staff, including habilitation professionals, classroom teachers, support assistants, and QTVIs, are responsible for the holistic provision for each CYPVI on their caseload. Research by Reinhardt (2001) reported that adequate provisional support yields positive mental health effects and outcomes in CYPVI. Yet with the prevalence of childhood VI increasing in the United Kingdom (approximately, 19,154 CYPVI in the United Kingdom; Bhangoo, 2022), and the decrease of centralised funding (Keil, 2016; Bhangoo, 2022), many CYPVI are not, in fiscal nor practical terms, receiving the support they are entitled to.
The economic crisis has suffocated educational provision. Budget cuts to local authorities and sensory services have led to a drastic change regarding the quality of provision. Recruitment of ‘cost-effective’ alternatives, that is, hiring TAs to cover the day-to-day work of a QTVI or habilitation specialist, often without any formal specialist training in vision impairment (Keil, 2016) or ‘buying in’ support from charity/third-sector organisations, often at a higher cost than in-house provision, all affects quality of provision. This implication of quantity over quality will undoubtedly affect CYPVI development at arguably one of the most crucial developmental stages in their lifespan. Access to habilitation provision is a postcode lottery, much like that of the QTVI, of which neither role can feasibly be replaced by an un(der)qualified, cheaper alternative. So, with decreasing funding, underqualified staffing, limited qualified personnel, and a caseload of CYPVI who are at increased risk of mental health issues, such as anxiety and depression (compared with the general population), the impact of the culmination of ‘bad luck’, ‘wrong postcode’, and sparse provision is likely to yield adverse effects and plot holes in each CYPVI’s developmental journey, in practical and psychological terms. We therefore turn to parents/caregivers, who are the consistency among the inconsistency, arguably the people whom the CYPVI will turn to for advice and support, to share their worries, concerns, and hopes for the future.
Parents/caregivers directly witness the developmental, psychological, and social impact that a VI has on their child/ren. Parents/caregivers of CYPVI often advocate for educational and mental health provision to ensure their child/ren has sufficient access to the education and daily life of which they are entitled to. While continuously fighting and advocating for their child/ren’s needs and rights, familiarising themselves with case law, legislation, paperwork, and creating a community of likeminded individuals, it is perhaps easy to overlook the direct impact of parenting a CYPVI. Sola-Carmona et al. (2013, 2016) reported that parents of CYPVI had significantly higher levels of anxiety compared with parents of sighted children. The elevated parental anxiety was related to their child’s VI (i.e., uncertainty of development, worries about their child’s progression, school (Lupón et al., 2018), and related to their level of knowledge about their child’s VI; all indicating a lack of support for the parents of CYPVI. This indicates an association between parenting and provision for CYPVI; however, other research (Rainey et al., 2016; Tadić et al., 2016) shows that parental perception may be discordant with the perception of their CYPVI. For example, on a measure of Quality of Life (Tadić et al., 2016), parents reported lower quality of life (of their child) and higher functional vision scores compared with self-report of CYPVI. This discordance suggests that parental perception of quality of life and provision may be overexaggerated compared to the self-report of CYPVI. However, parental perceptions should be taken seriously when considering parental support and intervention. Furthermore, irrespective of the discordance between scores, there is justifiable basis for collecting parent/caregiver views particularly when considering future avenues for research and discussion.
This pilot study, initiated by parents and driven by areas of parental concern, seeks to explore the current provisional arrangements in the United Kingdom and the potential impact this has, in their view, on educational outcomes of CYPVI.
Method
Ethics were approved by IOE UCL’s Faculty of Education and Society research ethics committee. Full informed consent was obtained by the parents/caregivers prior to completing the questionnaire. All participants were informed of their rights to confidentiality, anonymity, and withdrawal of data. No participants requested their data be withdrawn.
Participants
Of the 90 respondents that started the questionnaire, 47 did not complete in its entirety. Therefore, data were collected from 46 parents and carers of CYPVI in the United Kingdom (female = 40; male = 2; 1 = non-binary; and 3 = undisclosed), 18 years old and above (min. age = 32, max. age = 59). Forty of whom were the primary caregivers, two were non-primary caregivers and four did not disclose. Participants were mainly from England with three respondents from elsewhere in the United Kingdom (location not reported for General Data Protection Regulation [GDPR]) (Table 1).
Participant demographics for parents of children with vision impairment; and associated demographic information for the children with vision impairment they were reporting for.
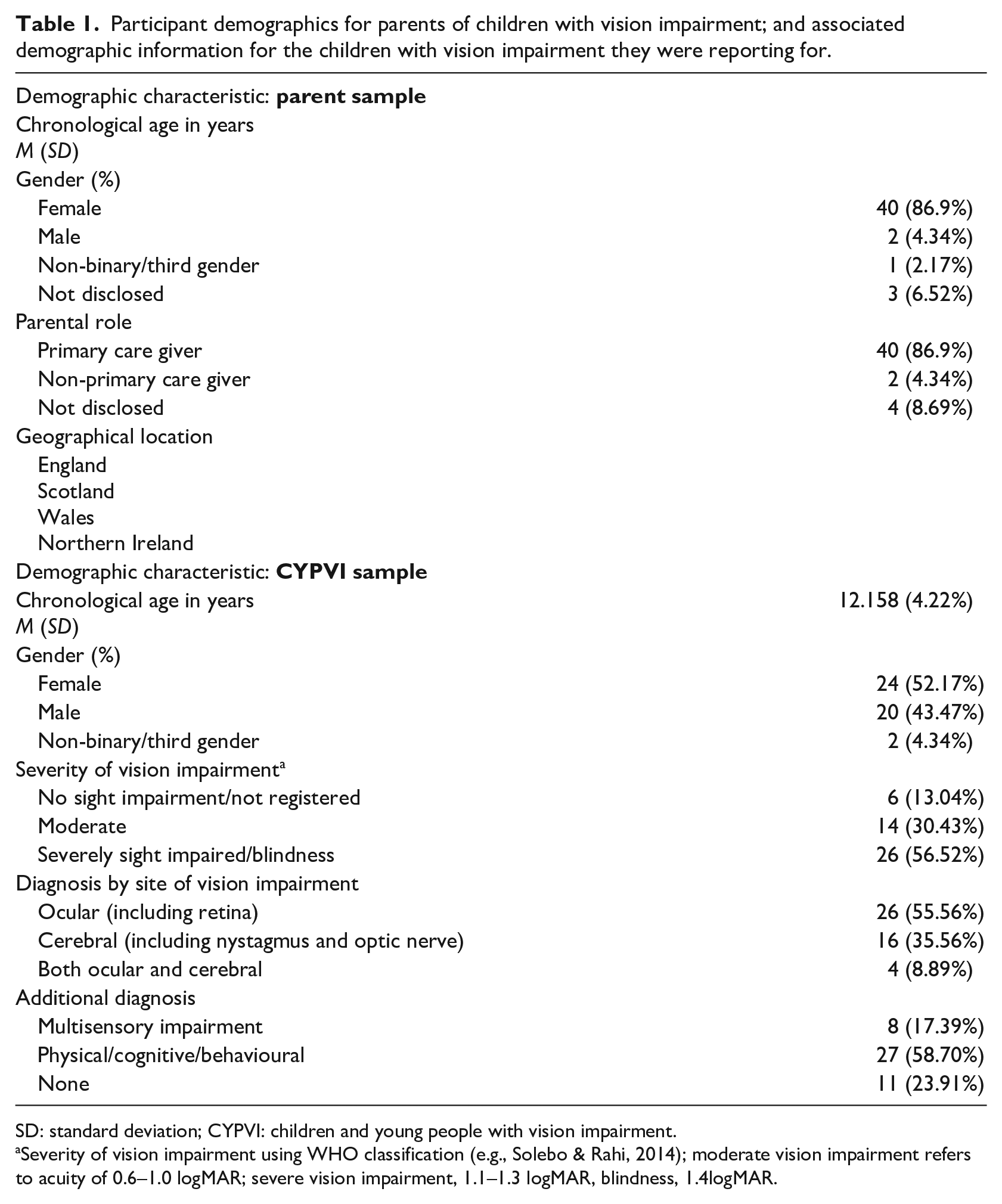
SD: standard deviation; CYPVI: children and young people with vision impairment.
Severity of vision impairment using WHO classification (e.g., Solebo & Rahi, 2014); moderate vision impairment refers to acuity of 0.6–1.0 logMAR; severe vision impairment, 1.1–1.3 logMAR, blindness, 1.4logMAR.
Materials
An online questionnaire was developed in collaboration with parents/caregivers of CYPVI. A 2-week consultation period was initiated prior to launching the online questionnaire, whereby advice was sought from VI charities, organisations, and parent/carer groups from across the United Kingdom. The survey used was based on the agreed protocol from the consultation period. The questionnaire had focus on the following topics: VI provision, TA (or equivalent) support, educational health care plans (or equivalent), legal support, alternative education, IT support, VI education improvements, and background/demographic information of the respondents (i.e., parents/caregivers) and their CYPVI.
Procedure
After a consensus was agreed for questionnaire items, the questionnaire was made available via Qualtrics (an online survey tool). The questionnaire was live for 9 weeks from 13 May 2022 to 15 July 2022. An anonymous survey participation link was distributed to parents/caregivers via charities and organisations. The landing page detailed the information sheet and consent form, of which all items for consent had to be checked before participation in the main questionnaire.
Results
The results are split into two parts. Part 1 details the descriptive statistics associated with provisional entitlement, covering questions regarding VI provision, TA (or equivalent) support and educational health care plans (EHCPs; or equivalent) from the questionnaire. Part 2 presents the thematic analysis from open-ended short-answer responses.
Part 1: quantitative data analysis
Education (schooling)
In total, 38 (82.61%) CYPVI had an EHCP or equivalent. Parents reported that over half of the sample (63%; 29 CYPVI) used large print to access educational materials. Eleven children (23.9%) used Braille, and three children (6.52%) used screen readers. Two children were reported to use multiple methods of engagement.
Most CYPVI were reported to attend a mainstream school with no VI unit. Second to mainstream settings, parents reported a blend of mainstream and home schooling while awaiting confirmation for a place in a specialist provision.
Education (provision)
QTVI support: Of CYPVI, 87% had access to a QTVI within their local area, of this, 17.5% has access to two QTVIs. In terms of school-based QTVI’s, only 6.67% of schools were reported to have an in-house QTVI provision. According to parental report, the QTVI provided educational access and support skills for 47.73% of CYPVI, equating to approximately 4.64 hr of general support per week, 3.5 hr (on average) was direct 1:1 QTVI support for the CYPVI. It was noted that these contact hours were consistent with information specified in EHCP (or equivalent) documentation. Parents reported that on average the QTVI would contact them at least once per week, typically via email communication, though other forms of communication (e.g., phone call, (in)formal meeting, text and letter) were reported and offered.
Teaching Assistant Support: The range of TA support was between 1 and 15 lessons per week (M = 10.80, SD = 5.32). Approximately, 70% of TAs offered general support with no training in vision impairment/visual need(s); 21.62% of areas surveyed deployed specialist multisensory support workers in the local authority, and some CYPVI did not require TA support. Of the identified TA support, 40.81% of TAs were reported not to have specialist VI knowledge/qualifications, and only four TAs were reported to have specialist VI knowledge/qualification in more than one area (i.e., Braille and large print diagrams). Of parents, 69.05% reported that the TA supporting their child did not have specialist subject knowledge, and of those asked, 21.43% of parents did not know the qualification/skill set of the supporting TA. Resulting from this, 37.84% of parents were not confident in the TA knowledge to support their child, 8% were confident, and 32% were split between somewhat (un)confident.
Accessible materials: Half of parents (50%) reported that their child ‘sometimes’ had access to the same/adapted materials as their peers. In relation to tactile diagrams, 50% of parents reported that their child ‘sometimes’ had access; 17% ‘rarely’ had access; 23% ‘never’ had access; and 10% ‘always’ had access to tactile diagrams, mainly across maths, science, and English classes. In relation to homework materials, 41.86% parents had to assist homework and support translating of materials into either Braille or large print. Naturally, this did not reflect the 23.26% CYPVI who were home-schooled; 4.44% parents reported that they rarely received additional external support from the school, rather any external support was from private tutors.
Habilitation (provision)
On average CYPVI received 1.57 hr of habilitation (mobility, orientation, and independent living skills) input per week. It was reported that 65.52% of these sessions were run by a qualified habilitation assistant or qualified habilitation specialist. The local authority was the main provider of habilitation input, followed by charitable organisations. Of those that received habilitation support, 34.88% of participants engaged in habilitation outside of the school setting.
Quality of provision and mental health outcomes
Parents reported that the quality of their child’s provision affected their mental health positively (24%), negatively (40%), or both positively and negatively (19%). Positive effects were attributed to; the support of the VI team, including QTVI, sensory support, and inclusion into wider school events (i.e., sports). The negative effects were captured in report of mental health conditions, though it is important to note that 71.43% of these conditions were not formally diagnosed (Table 2).
Diagnosed/suspected mental health conditions of CYPVI related to quality of educational provision.
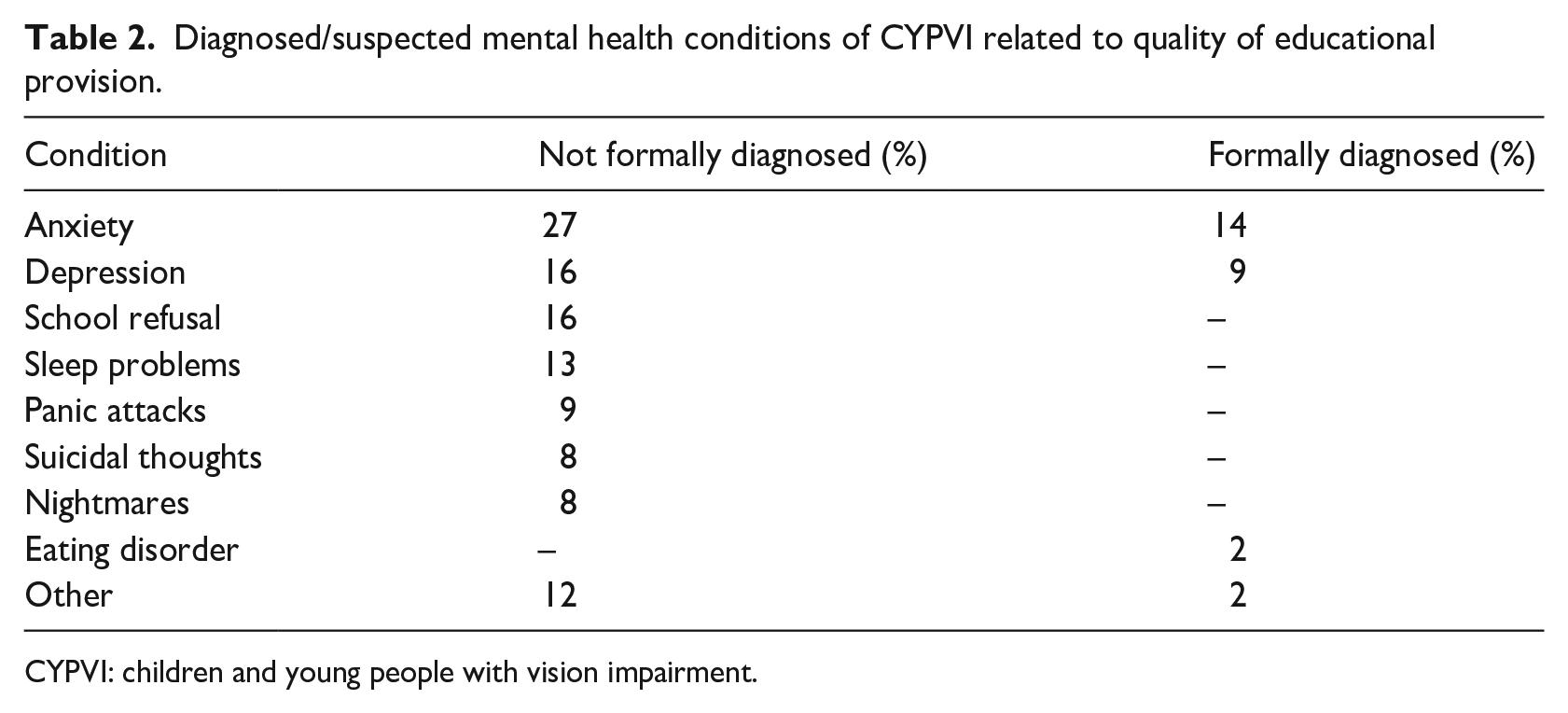
CYPVI: children and young people with vision impairment.
Part 2: qualitative data analysis
To add context to the descriptive statistics above, thematic analysis was applied to the short answers offered by parents. Three main themes were identified from the short-answer responses: insufficiency, support, and child-centred.
Theme 1: insufficiency
Echoing the quantitative findings, parents felt that school staff had a ‘lack of training, lack of awareness, lack of time’. This corroborated with detail regarding the training of professionals in supporting CYPVI. ‘Total lack of understanding of the impact of VI on access to learning, on mental health, on independence, on their whole life’. The qualitative data reported a synergy between the effects of insufficient training, poor knowledge (of VI) and how this was detrimental to the child/ren receiving provision.
Theme 2: support
Parents reported that support from the QTVI, school staff, and charities had an important influence on their child’s education. Parents identified support from a QTVI and a ‘trained and qualified TA’ as facilitative to meeting their child’s needs. Parents also reported the benefit of multidisciplinary collaboration regarding provision that is, ‘the dedication of the school in general to support my child’. Support was also identified in ensuring each child had appropriate access to education materials. For example, ‘working IT, enlarging materials, and reasonable adjustments’. This demonstrated that support ranges from those delivering the provision to the materials that are used to enhance learning.
Theme 3: child-centred
Both aforementioned themes contribute to the final identified theme regarding a child-centred approach. Parents stressed the importance of including their child in decision-making based on their individualised need(s); ‘take time to check in with my child about what they need and act on what they need’. Parents corroborated the idea that actively listening to each CYPVI enables autonomy and encourages the CYPVI to ‘advocate for themselves’. Parents also reported that ‘taking time’ means speaking with and listening to the voice of the child during decision-making processes, as opposed to checking in as an afterthought when a plan is already in effect. This continued to involve parents/caregivers in the decision-making process, especially as parents have a holistic understanding of their child’s needs and goals. One parent reported ‘listen, learn, help’ in response to the question. These three words carry power by ensuring that the child is at the centre of provision, enabling them to be an active participant in their learning and development while encouraging and fostering self-advocacy.
Discussion
The aim of the study was an exploratory evaluative approach examining the effectiveness of specialist VI support in educational contexts. Both qualitative and quantitative results indicate that school support staff are not always fully trained or equipped to support CYPVI that can lead to inconsistencies in provision, reduced inclusion, and disparate receipt of provision reducing parental confidence in the educational system. Parents of CYPVI (who attended school) appeared to compensate for this, in part, by creating accessible resources for their child/ren to support curriculum access. A task additional to their role as a caregiver, and likely to impact their time, capacity, and potentially their relationship with their child/ren. Results indicated that parental concerns could be alleviated by adequate training of staff, and a consistent ‘joined-up’ approach which accommodates the voices of the CYPVI themselves, and parent/caregiver perspectives. Most parental reports were made on behalf of their child/ren who were diagnosed with severe sight impairment/blindness, educated in mainstream settings with no VI unit. This, combined with the remainder of the sample (moderate sight impairment/not registered; educated in specialist/home settings), arguably captures the ‘low incidence, high need’ sample, of which reasonable adjustment ought to be prioritised.
The strength of the results was that almost all CYPVI had access to a QTVI, habilitation input, and adaptations to educational materials. This aligns with provisional entitlement as legislated in the SEND Code of Practice, England (DfE & DoH, 2014). Not all CYPVI had access to these arrangements, however, which can then negatively impact education and independence outcomes. The inconsistency of support may reflect the ‘postcode lottery’ or provisional entitlement and echoes the conclusions of previous published work (Hogg et al., 2017).
Examination of specific areas for enhancement revealed that most TAs deployed to support CYPVI, were seconded to schools. While this does not come as a surprise (see Bhangoo, 2022; Keil, 2016), the same issues surface; namely, TAs not having sufficient specialist subject knowledge, and little to no formal training or experience in working with CYPVI. These elements combined reduce parental confidence in the skills and ability of those identified to provide reasonable adjustments to support their child/ren in educational contexts.
Qualitative and quantitative results showed that most CYPVI were involved in the EHCP (or equivalent) review process, and over half of the respondents felt ‘listened to’. Considering it is a statutory requirement to involve and consult CYPVI and parents/caregivers in the review process, the number of respondents who reported they were involved, is shockingly small. This is consistent with the Ofsted (2021) report and indicated that not all statutory requirements have been met, and arguably, lack of direct involvement in decision-making is an understandable reason as to why parents/caregivers largely reported dissatisfaction with processes and outcomes.
Analysis of the qualitative data enabled a more in-depth exploration regarding parental perception. The global theme ‘Access and Inclusion’ consisted of three subthemes: ‘insufficiency’, ‘support’, and ‘child-centred’. Though three salient themes were identified, they are not mutually exclusive. Insufficient training, awareness of staff, and lack of support led to a perception that education was neither accessible nor inclusive for CYPVI, and, resultingly, parents/caregivers reported detrimental effects on their CYPVI’s (un)diagnosed mental health conditions. Support was considered key to CYPVI access to the curriculum, particularly when support was holistic, that is, accommodating the needs and wants of the child, not solely addressing their VI. This strategy was considered enabling for a positive school experience. Staff willingness to listen, learn, and help, not only the CYPVI but their parents/caregivers too, was considered a strong facilitator to ensuring the child’s needs are met. Thus, it must be stated that staff willingness to support is not a fundamental issue here. Rather, it is the formal training of the staff that, combined with willingness, would be a true mechanism for support and enhance provisional entitlement. This may then encourage a shift of parental/caregiver attitude from negative to positive.
The exploratory nature of this pilot study meant that the sample was intentionally niche. Most respondents were mothers of CYPVI, though the findings would certainly be enhanced with paternal contributions and perspectives including, but not exclusive to, the demands on parent/caregiver time to compensate for insufficient provision (e.g., creating accessible documents) and how this affects the parent/child relationship. Future work would benefit from targeted sampling (e.g., approaching fathers’ support groups) to ensure fathers’ voices are also captured in discussion of their child/ren’s provisional entitlement and mental health outcomes. In the current study, formally diagnosed mental health conditions were made by a clinician (e.g., general practitioner [GP]/mental health professional). Non-formally diagnosed conditions were based on parent/child reports of symptoms, and in some cases, CYPVI’s were awaiting referral to Mental Health Services. The formality of diagnosis, however, did not dissuade parental opinion that provisional entitlement had negative effects on CYPVI mental health. It was considered unethical to harness and triangulate CYPVI opinions regarding mental health until a baseline picture of current circumstances could be better understood. Therefore, future work in this area would be enhanced with a triangulated approach from local authorities, schools, and CYPVI themselves.
Despite limitations of the current study, the results are considered useful and pertinent to parents/caregivers, CYPVI, and all educationalists/specialists involved in VI provision. The findings presented in this study corroborate with previous published works. Exploring parental perceptions of specialist VI provision highlighted that, within the sample, parents/caregivers were not confident in the quality of support received by their child/ren. There are, however, identified tangible areas for practitioners, educationalists, and multi-disciplinary teams to consider when hiring, training, and maintaining staff working with CYPVI.
Conclusion
Findings in the current study were consistent with parental perceptions in published works. In the current study, generally, parents did not feel confident in the quality of support that their child receives, and subsequently linked this to poorer mental health outcomes. The questionnaire regarding mental health outcomes was not sensitive enough to corroborate this claim, however, the project offers an overview regarding parental perception that should now be triangulated with educationalist and CYPVI perspectives. The results echo that of previous work regarding provision, indicating that the quality of educational provision still requires work, funding, training, and collaboration.
Footnotes
Data availability statement
The data generated for this study will not be made publicly available. The ethics form states that only processed data will be presented in manuscripts. Data are not available to maintain anonymity and confidentiality of participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval statement
The project received ethical approval from UCL IOE Research Ethics Committee
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent statement
All participants and their parents gave written consent and verbal assent to anonymised/depersonalised data presented in the manuscript.