
Abstract
People with blindness and visual impairments have reduced access to exercise compared to the general population during typical societal functioning. The Coronavirus-19 pandemic completely disrupted daily life for most individuals worldwide, and in the United Kingdom, a stay-at-home order was enforced. One of the sole reasons an individual could leave their home was for the purpose of daily exercise. Here, we examined how the UK national lockdown impacted access to exercise for people with blindness and visual impairment. We used a mixed methods design, collecting quantitative data from two established measures (the Exercise Barriers and Benefits Scale and the International Physical Activity Questionnaire), and qualitative data from open-ended questions. We found that, during the initial stages of the lockdown, perceived barriers to exercise increased compared to pre-pandemic levels, driven by factors, such as the closure of exercise facilities and additional difficulties posed by social distancing. Interestingly, during the later stages of the UK Coronavirus-19 response, perceived barriers decreased to lower than pre-pandemic levels. Thematic analysis indicated that this may have been due to participants finding new online methods to exercise at home, in combination with the tentative reopening of facilities.
Introduction
Exercise is one of the most critical activities that humans can perform for their health and well-being. It is well documented that exercise is not only beneficial for physical health (Cotman & Berchtold, 2002; Ito, 2019; Ness et al., 2007) but it also has a vast number of psychological and social benefits (Penedo & Dahn, 2005; Raglin, 1990; Ruby et al., 2011). While many individuals struggle to exercise due to a variety of time, financial, and motivational reasons (Ebben & Brudzynski, 2008; Tappe et al., 1989), people with blindness and visual impairments have added barriers to exercise on top of those faced by the general population (Capella-McDonnall, 2007; Matoso & Portela, 2020). Prior research into exercise participation for populations with blindness and visually impairments suggests that some exhibit comorbidity with symptoms related to insufficient exercise, such as hypertension, obesity, and depression (Mann et al., 2014; Shields et al., 2012). Conversely, for groups with blindness and visually impairments, research has documented many examples in which exercise and sports can have positive effects. For example, in older adults with visual impairments, dance programmes have shown to improve not only aspects such as mobility, balance, and cardiovascular fitness, but also increased measures of cognitive flexibility and quality of life (Hackney et al., 2015; Hwang & Braun, 2015). In fact, the quality of life of national level athletes with visual impairments compared to matched controls was found to be higher in every aspect, including social functioning, perception of health, and physical functioning (Ilhan et al., 2021). Undoubtedly, access to exercise is incredibly important for health and well-being and, with the right support, people with blindness and visual impairments can participate in various forms of sport and exercise under normal circumstances.
However, the Coronavirus-19 pandemic has disrupted daily life for a high number of individuals across the globe, and in the United Kingdom, a national lockdown was implemented on 23 March 2020 under the Coronavirus Act 2020 (Coronavirus Act 2020, 2020). Under this act, the population was required to stay in their homes unless shopping for essential food or medicine, requiring medical attention, caring for a vulnerable person, travelling to a place of work (if essential), and finally, for one form of exercise per day. Similar measures were implemented in many other countries (Dunford et al., 2020). Research around the globe suggests that those with disabilities have been among the most severely affected by lockdowns and social distancing (Jalali et al., 2020; Mbazzi et al., 2020; Safta-Zecheria, 2020). The additional difficulties faced by people with visual impairments include additional transmission risk from navigating by touch and identifying food quality by smell (or closer visual inspection), being unable to change working routines to work from home (Suraweera et al., 2021), and reduced feelings of autonomy and independence (because of having to rely on other family members or online services for groceries). Furthermore, people with blindness and visual impairments reported how sporting hobbies decreased outside, but slightly increased inside the home (Gombas & Csakvari, 2021).
During the early stages of the UK lockdown, the government allowed and actively encouraged exercise (Coronavirus Act 2020, 2020). People who were typically low exercisers before the lockdown reported an increase in exercise participation during lockdown (Constandt et al., 2020). However, the same study also found that for those above the age of 55 years, people who previously were high exercisers before the pandemic and people who exercised with others reported a decrease in exercise participation. While the majority of a sampled population in the United Kingdom maintained normal levels of exercise during lockdown, groups more at risk for Coronavirus (including those with a disability) were associated with doing less physical activity than they did prior to the pandemic (Rogers et al., 2020). Many people with visual impairments require assistance with exercise, travel to exercise, or specialised coaching (Seham & Yeo, 2015; Skaggs & Hopper, 1996); hence, reduced access to this type of assistance dictated by the pandemic restrictions could have impacted access to exercise for those needing support.
This study aimed to understand how access to exercise was impacted by the Coronavirus-19 pandemic, comparing early lockdowns and late lockdowns to data collected prior to the commencement of the pandemic. Based on the limited evidence on the effects of the Coronavirus-19 restrictions and lockdown on individuals’ levels of exercise, we first hypothesised that there would be a difference in participation in, and perception of barriers to, exercise during lockdown compared to before the lockdown. We could not predict the direction of this change in participation and in perception of barriers, as on the one hand, working from home for many participants could have increased available time to exercise. On the other hand, a reduction in open exercise facilities (such as gyms and leisure centres) could have reduced exercise participation and be perceived as a great barrier to exercise (Constandt et al., 2020; Rogers et al., 2020). Our second hypothesis was that those living in less urban areas would have greater exercise participation than those in more urban areas as facilities had closed, and that open spaces and access to countryside may offer more opportunities to exercise with a reduced impact of the lockdown on these areas.
Methods
Participants
We recruited 61 people with blindness and visual impairments overall, 21 participants took part during the pre-lockdown period (7 females, 11 males, 3 did not answer; mean age in years = 39, range = 17–62 years). Furthermore, 22 participants took part during the early lockdown period (14 females, 10 males; mean age in years = 39, range = 17–70 years), and 18 participants took part during the late lockdown period (11 females, 6 males, 1 did not answer; mean age in years = 47, range = 18–68 years). See Appendix 1 for further participant details. All participants provided informed consent, and the study was approved by the University of Bath Psychology Research Ethics Committee (Ethics No. 19-088). We recruited participants through social media and word of mouth. As the questionnaires were anonymous, it is possible that some of the participants may have overlapped between groups.
Materials and measures
The International Physical Activity Questionnaire (IPAQ) was developed to monitor physical activity to a global standard (Craig et al., 2003) and has since become the most used measure of physical activity in academic literature (Van Poppel et al., 2010). The short version (IPAQ-SF) consists of nine items that cover activity at four different intensities (vigorous intensity, moderate intensity, walking, and sitting, respectively). The typical response format is to provide a 7-day recall of the number of minutes spent doing any of the four activity intensities. For example, ‘During the last 7 days, on how many days did you do vigorous physical activities, such as heavy lifting, digging, aerobics, or fast bicycling?’, followed by ‘How much time did you usually spend doing vigorous physical activities on one of those days?’. The IPAQ-SF is typically used to provide an estimate of Metabolic Equivalent of Task (MET), a measure of energy expenditure for a given activity. MET can be robustly calculated by multiplying the relative (to body weight) oxygen consumption of an activity by oxygen consumption while sitting. However, this method of calculating METs requires specialised equipment (such as Douglas Bags or VO2 gas analysers) and a great deal of time. The IPAQ-SF calculates an estimate of METs using only self-reported time spent exercising at different intensities and is far more feasible for establishing trends remotely or in large groups of people. To our knowledge, the IPAQ-SF has been used, but not validated with people with visual impairments (e.g., Barbosa et al., 2019; López-Sánchez et al., 2019).
The Exercise Benefits/Barriers Scale (EBBS) is a two-part psychometric measure (barriers and benefits) that can be used in isolation of one another (Sechrist et al., 1987). To maintain brevity, only the barriers section of the questionnaire was adopted for this study. The benefits of exercise are well documented, well reported, and we accept that most members of a Western demographic understand that exercise is beneficial to health and would unnecessarily extend the length of time required without making a commensurate contribution. The barriers section of the EBBS has been successfully applied to several demographics that often have reduced access to exercise, including the elderly (Fonseca Victor et al., 2012) and people with mobility impairments (Stroud et al., 2009; Thomson et al., 2016), but to our knowledge, has not been specifically validated for people with visual impairments. We also asked our participants other more flexible open-ended questions to probe both specific aspects of exercise during the pandemic and to understand the presence of exercise support networks under normal circumstances compared to disruption.
Procedure
The survey was hosted on the online platform Qualtrics (Qualtrics, Provo, UT) and was split into four main sections: the first pertained to demographic information (gender, age, level of impairment, onset of impairment, and residential location), the second and third sections contained the IPAQ-SF and EBBS questions, respectively, and the fourth section contained the open-ended questions (Table 1). Some of the questions had to be slightly adjusted from the initial pre-lockdown data to make sense or encapsulate exercise given the pandemic. For example, the first open-ended question was changed from ‘What sports do you regularly participate in?’ to ‘Before the virus, what sports did you regularly participate in?’. Another example of a slight wording change was for the introduction to the IPAQ-SF questions, asking the participant to reflect on their exercise specifically ‘on an average week during the coronavirus pandemic’, rather than purely an average week. We made these slight wording changes to ensure clarity and specificity of responses; the impact of the lockdown changed the definition of words, such as ‘typical’ and ‘average’. Pre-lockdown data were collected between 29 May 2019 and 10 March 2020. Early lockdown data were collected between 4 May 2020 and 1 July 2020. Late lockdown data were collected between 7 July 2020 and 22 February 2021.
Open-ended questions presented to participants at the end of the survey.
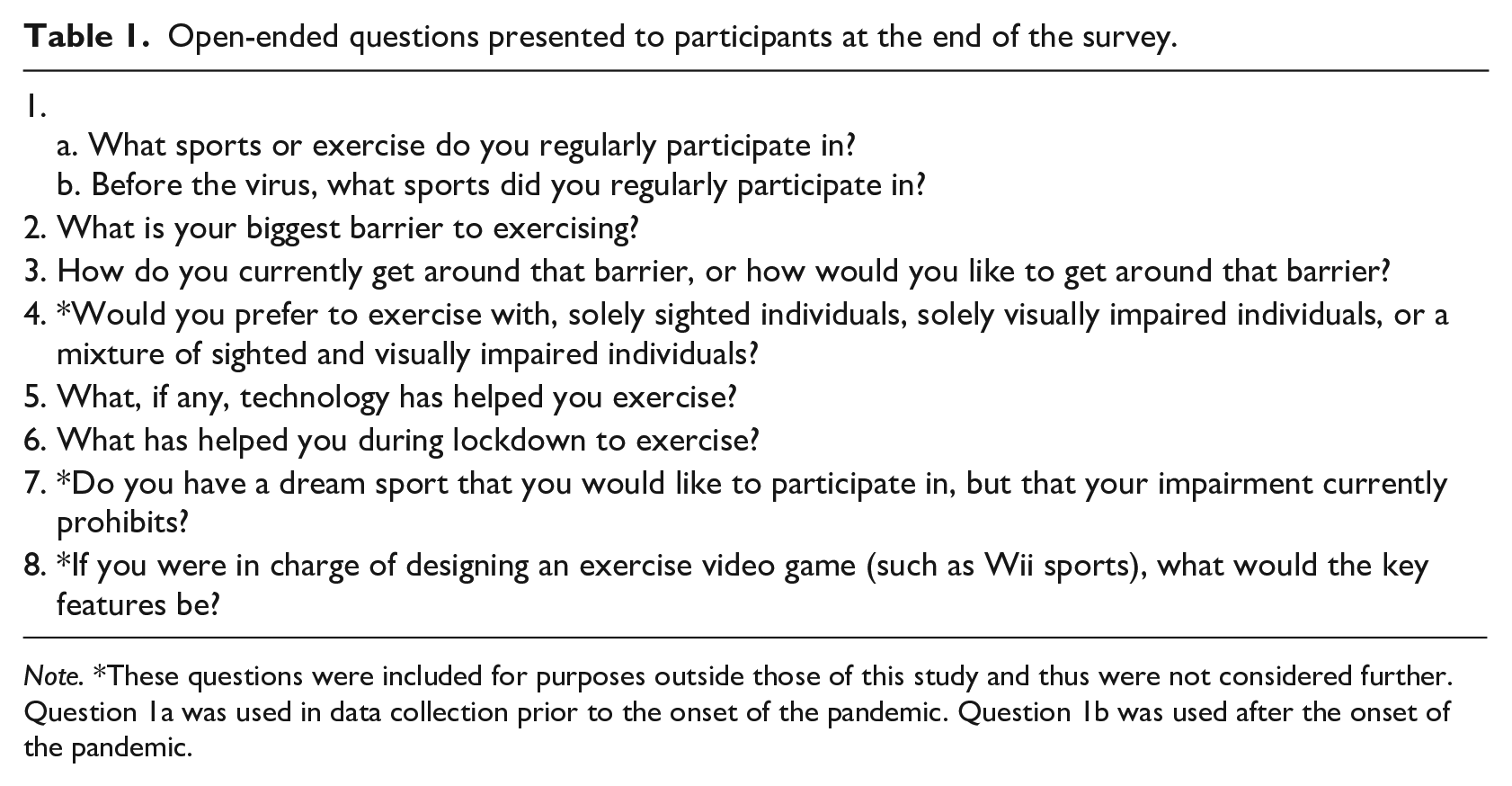
Note. *These questions were included for purposes outside those of this study and thus were not considered further. Question 1a was used in data collection prior to the onset of the pandemic. Question 1b was used after the onset of the pandemic.
Data analysis
Data were exported from Qualtrics into .csv files and processed in Microsoft Excel. Statistical analysis on the IPAQ-SF and EBBS results was conducted using the Pandas (version 1.2.1) and Pingouin (version 0.3.9) libraries for Python (version 3.8.5).
For the thematic analysis, we followed established practices based on common qualitative methods for psychology (Braun & Clarke, 2006). We used an inductive and deductive approach due to the specificity of the questions (the questions were open, but short and highly targeted) and reflected on the data from a critical realist perspective (generally taking each participant at their word) with aspects of constructionism (but also looking for deeper meaning or metaphor). The coding procedure entailed separating out the qualitative responses from the rest of the questionnaire into a separate word file. This document was then printed into a hard copy which was read through for immersion in the data, and then parsed a second time to generate initial codes and notes. Codes were refined; however, no large changes were needed as each participant’s response was concise and in answer to a specific question (i.e., as opposed to a longer open interview, in which a participant may make many complex and overlapping points which require untangling). Answers to the question, ‘What has helped you to exercise during lockdown?’, were not analysed due to too few responses, perhaps due to the similarity to the previous question, ‘What, if any, technology has helped you exercise?’.
In the case that a participant responded with ‘unsure’, the entry was treated as a missing value. One participant responded to the question, ‘During the last 7 days, how much time did you spend sitting on a weekday?’, with the response ‘40 hours’. Here, we assumed that the question had been misunderstood and divided the total hours by 7. In cases where the participant responded to the question, ‘During the last 7 days, how much time did you usually spend sitting on a weekday?’, with a variation of ‘the rest of the day’, responses were coded as 180 min. All outlying entries that recorded more than 180 min were truncated to 180 min, as per the IPAQ-SF recommendation (IPAQ Scoring Protocol – International Physical Activity Questionnaire, n.d.). A Python function was used to convert the IPAQ-SF results into estimated weekly METs (Boyle et al., 2021)
Results
The assumption of normality was violated for the EBBS pre-lockdown group (Shapiro–Wilk’s W = .888, p = .020), but not the early or late lockdown groups (Shapiro–Wilk’s W = .970, p = .717; Shapiro–Wilk’s W = .935, p = .234, respectively). The data were normally distributed for all residential location groups in the EBBS: a major city (Shapiro–Wilk’s W = .922, p = .237); a small city/large town (Shapiro–Wilk’s W = .954, p = .440); a town (Shapiro–Wilk’s W = .919, p = .183); and a rural area (Shapiro–Wilk’s W = .918, p = .267). For the IPAQ-SF, the data deviated significantly from a normal distribution for the pre-lockdown and early lockdown groups (Shapiro–Wilk’s W = .653, p < .001; Shapiro–Wilk’s W = .847, p = .003, respectively), but not the late lockdown group (Shapiro–Wilk’s W = .902, p = .062). All residential location groups in the IPAQ-SF failed to satisfy the assumption of normality: a major city (Shapiro–Wilk’s W = .746, p = .001); a small city/large town (Shapiro–Wilk’s W = .706, p < .001); a town (Shapiro–Wilk’s W = .840, p = .013); and a rural area (Shapiro–Wilk’s W = .759, p = .003). The Levene’s test demonstrated that there was homoscedasticity for lockdown stage in both the EBBS, F(2, 58) = .022, p = .978, and the IPAQ-SF, F(2, 58) = .619, p = .542, and the factor of residential location in both the EBBS, F(3, 57) = .516, p = .673, and the IPAQ-SF, F(3, 57) = .892, p = .451. Hence, for the EBBS data analyses, we used a between-subject analysis of variance (ANOVA) due to only one group deviating from normality and because ANOVAs are robust to deviation from a normal distribution (Schmider et al., 2010). For consistency, we also used an ANOVA for the IPAQ-SF, but since the deviations from normality were more severe, we also ran a non-parametric model to compare the results.
Two between-subject ANOVAs were conducted on the EBBS and the IPAQ-SF scores, respectively (see Table 2 for mean scores and standard deviations). The analysis included two between-subject factors, the lockdown stage (pre-lockdown, early lockdown, and late lockdown), and the area of residence (major city, small city/large town, town, and rural area). The results showed that for the EBBS scores, there was a significant effect of lockdown stage, F(2, 49) = 24.50, p < .001, η p 2 = .50, but not of residence location, F(3, 49) = .48, p = .696, η p 2 = .03. In addition, no significant interaction effect between these factors was found, F(6, 49) = 2.17, p = .062, η p 2 = .21. The results for the MET scores revealed no significant main effect of lockdown stage, F(2, 49) = .41, p = .666, η p 2 = .02, residence location, F(3, 49) = .79, p = .504, η p 2 = .05, or interaction between these factors, F(6, 49) = 1.64, p = .157, η p 2 = .17. A Kruskal–Wallis H test also aligned with the result of the ANOVA, indicating no significant difference in lockdown stage or residential location, H(2) = .495, p = .780; H(3) = 1.296, p = .730, respectively. As a significant difference of lockdown stage was found for the EBBS, post hoc corrected-for-multiple-comparisons Games-Howell t-tests were carried out on this factor, as it is more robust against varied group sample sizes and deviations from normality (Toothaker, 1993). Our participants reported that there were significantly more perceived barriers in early lockdown compared to pre-lockdown, t(40.2) = 2.47, p = .038, g = .74, significantly more perceived barriers in early lockdown compared to late lockdown, t(36.3) = 6.27, p = .001, g = 1.95, and significantly more perceived barriers in pre-lockdown compared to late lockdown, t(32.9) = 4.40, p = .001, g = 1.38.
Mean scores and standard deviation for the EBBS and MET as calculated by the IPAQ-SF.
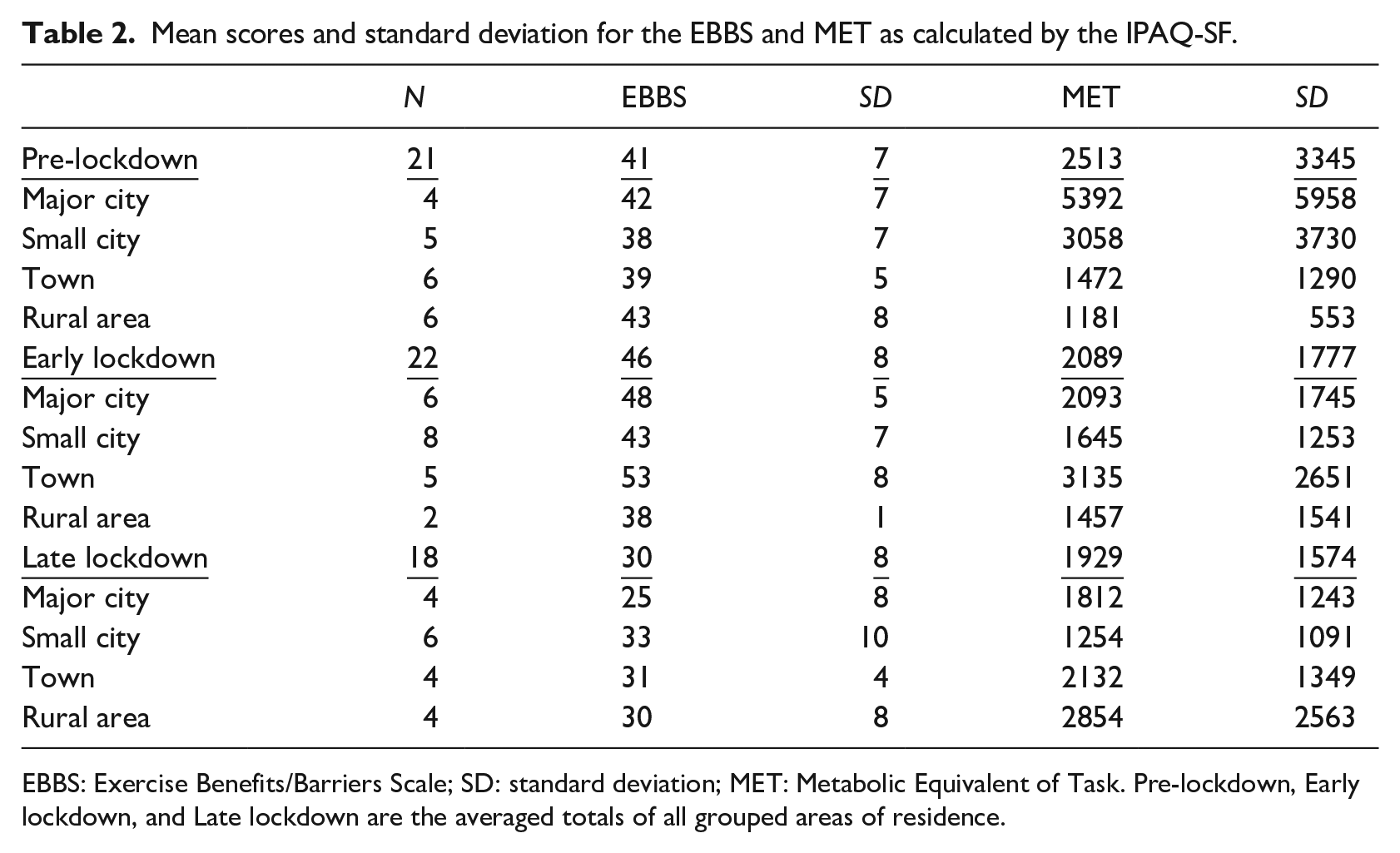
EBBS: Exercise Benefits/Barriers Scale; SD: standard deviation; MET: Metabolic Equivalent of Task. Pre-lockdown, Early lockdown, and Late lockdown are the averaged totals of all grouped areas of residence.
Responses to the questions ‘What sports or exercise do you regularly participate in? / Before the virus, what sports did you regularly participate in?’ were collated into a chart to give an overview of the most common sports and variety of sports in which our participants participate in (see Figure 1).
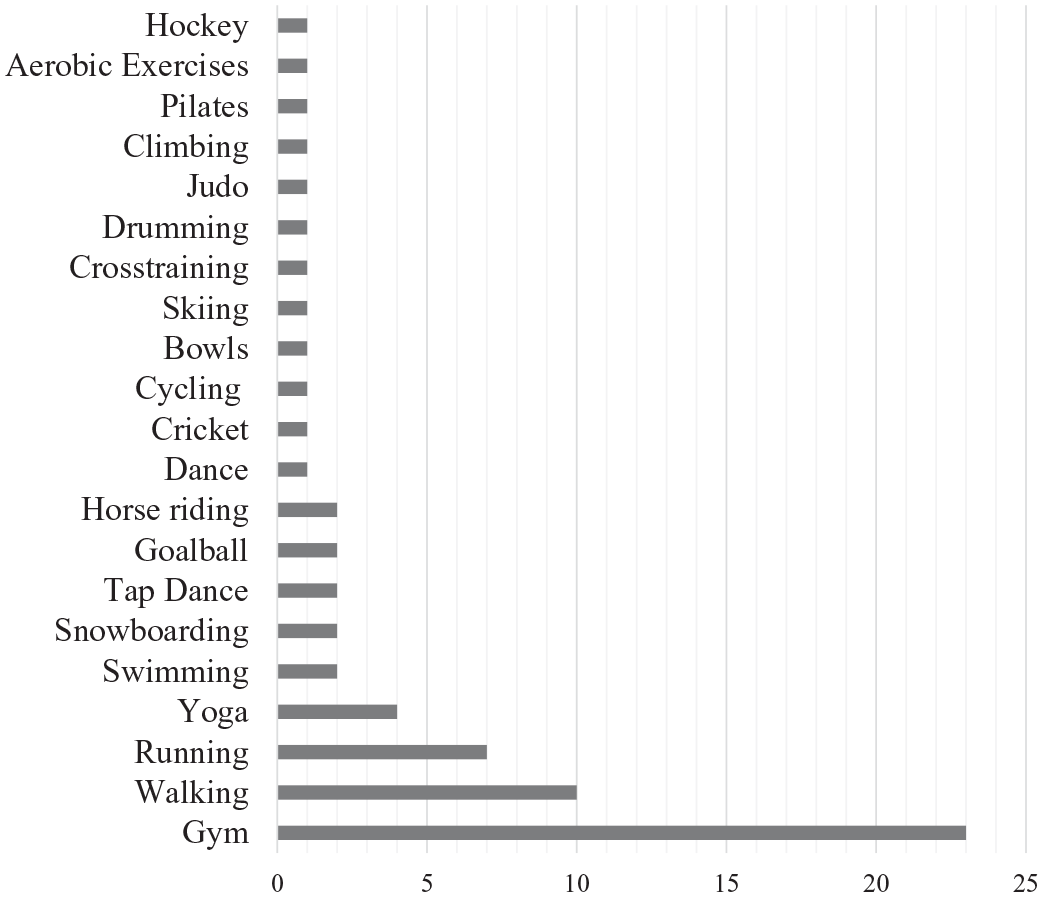
A chart demonstrating the count of sports and exercise activities regularly undertaken by our sample.
What is the biggest barrier to exercise?
Pre-lockdown
Prior to the pandemic, the most common barriers that were reported by the participants were themed as: lack of specific support, lack of motivation, inaccessible transport, and comorbidity. For one participant, many classes lack specific support for visual impairments: Finding people that will support someone with visual impairment. Increasing knowledge for support in class
This may exemplify that the participant was motivated to join a class, but classes often cannot provide adequate support for members with blindness or visual impairments. Another also echoed a similar sentiment on specific support: I am unable to operate gym equipment or see someone who is running a class
For one individual, exercising in a council run gym was not permitted without support: gyms run by the council don’t let me in without a carer and I don’t have one during the week as my husband works.
This response also hints at the role of family members in supporting exercise accessibility.
Lack of motivation was often reported as the major barrier to exercise participation: I cannot be bothered Getting in the mood after a day at work Lack of free time and personal motivation
Regarding inaccessible transport, one individual commented on the difficulties of transporting a bike to safe routes: once I’m on a proper route it’s easy for me to follow it but I am not safe to cycle on an ordinary road.
Another said it is difficult to find local activities, perhaps also alluding to lack of accessible transport: trying to find those activities I like to do, that caters for visually impaired people in my area.
Some participants commented on non-visual impairment-related health and well-being issues that prevented them from exercising, which we coded together under the theme of comorbidity. For example, two participants reported specific non-visual impairment-related barriers to exercise: [I have] an underactive thyroid. . . [and] chronic pain I have seriously injured my back and this is [a] major influence.
During lockdown
During the pandemic, the most reported barriers still included aspects of motivation, support, transport, and comorbidity, but more specifically centred around closed facilities (e.g., gyms and sport centres) and shielding/social distancing advice which affected existing support networks. For example: Because of my other illness I have to shield social distancing is difficult for some with little or no sight parents are shielding so walking is impossible without a guide.
Eight participants mentioned about how closed facilities (including gyms, community centres, exercise classes, and swimming pools) have presented barriers to exercise, and one goes further to say: exercise classes have gone online and I cannot see my iPad screen well enough to follow a class.
There were other prominent concerns over difficulties in social distancing as a person with visual impairments, and poor public understanding of visual impairments: Walking outdoors makes me feel more anxious now as I wish to stay safe. I do not look blind. I was told a number of times that I look like I am training my guide dog.
How do/would you overcome this barrier?
Pre-lockdown
Prior to the pandemic, the commonly mentioned methods for overcoming barriers were relying on friends and family for travel or exercise assistance, using gym equipment at work, travelling distance to get to places that can offer suitable support: I get around [the barrier] by travelling significant [distances] to cricket practice getting friends to take me where I want to go meeting friends at a time that suits them
During lockdown
These methods were no longer possible once social distancing was in place; for example, one person commented: Usually [I] use public transport but [I’m] avoiding at the moment due to risk.
Other participants mentioned that walking at home or with members of their households became a prominent method of exercising. Home gym equipment and online classes were also mentioned as ways to navigate the barriers posed by Coronavirus-19 to exercising: I purchased an exercise bike, which has helped me keep a level of fitness
In the later section of the lockdown after some facilities had reopened, a participant reports a method of exercise by: Home gym and going to a different [open] swimming pool further away.
What technology has helped with exercise during COVID-19?
The technology that participants reported to help with exercise was grouped into four categories (or themes). The two most prominent categories reported were themed as social technology and fitness trackers. Social technology included using Facebook, Zoom, YouTube, and Instagram to help increase exercise participation. Fitness trackers included FitBit and smart watches, using health data from smart phones and tablets and step counters. Other categories included navigation assistance (Google Maps, two-way radio, flashlight, and guide dog) and exercise equipment (treadmill, bike, and exercise bike). Two individuals both attributed the internet generally as a facilitatory technology, and four participants (out of all 40 participants who were asked the question) either did not answer or reported that there was no facilitatory technology that helped them exercise.
Discussion
This study aimed to explore the effect of the UK lockdown during the Coronavirus-19 pandemic on access to exercise for people with blindness and visual impairments. To do so, we adopted a mixed methods approach. First, using two questionnaires to quantitatively measure estimated weekly physical activity and perceived barriers to participation, respectively. Second, we created open-ended questions to gain insight into specific barriers to exercise participation and how these barriers were (or might be) overcome. The EBBS questionnaire found that perceived barriers were highest during the initial UK lockdown (data collected between May 2020 and July 2020) and lowest during the later parts of the UK lockdown (data collected between November 2020 and February 2021). Perceived barriers to participation prior to the pandemic were in the middle between early lockdown and late lockdown. There were no significant differences between estimated METs from the IPAQ-SF in either lockdown stage or residence location. The thematic analysis suggested that the UK lockdown initially added extra barriers to participation to several already existing barriers specific (e.g., lack of specialised support or equipment) and non-specific (e.g., motivation and time commitments) to disability.
Combining the open-ended questions with the results for the EBBS questionnaire, it would appear that prior to lockdown, people with blindness and visual impairments tended to perceive typical and impairment specific barriers to exercise, such as lack of motivation, transport issues, and lack of accessibility support as previously reported in other studies (Ebben & Brudzynski, 2008; Gombas & Csakvari, 2021; Tappe et al., 1989). The implementation of the UK national lockdown added a greater number of barriers to exercise to those already existing, such as not being able to socially distance, and no longer having access to previous support. However, as the lockdown evolved and progressed, some individuals began to use technological interventions, such as online classes and social media, to facilitate exercise at home. In the early lockdown, the EBBS score was at the highest compared to both other stages and based on open-ended feedback. This may have been primarily driven by the closure of exercise facilities as reported by many of our participants and by the increased difficulty to exercise outside due to lack of support and social distancing measures. Indoor fitness training, such as the gym, weights, and exercise classes, was the most reported type of exercise that participants regularly took part in, which were all closed in the United Kingdom in the early stages of the lockdown (Coronavirus Act 2020, 2020). Interestingly, according to the EBBS score, there were fewer perceived barriers in the late lockdown stage than prior to the Coronavirus-19 pandemic. This data collection time frame took place when facilities had reopened in the United Kingdom but with social distancing measures in place. This, plus the open-ended feedback we received, may indicate that the facilitatory technology developed for exercise at home during the height of the restrictions continued to be used alongside pre-pandemic exercise methods, thus increasing activity levels beyond pre-pandemic levels.
Our second hypothesis was that those living in highly built-up areas would have less access to exercise and more perceived barriers during lockdown rather than prior to lockdown. We did not find any significant differences for residential location on either EBBS score or estimated METs. A possible reason for this is that our sample size was not big enough to allow for a suitable number of participants in each area of residence category. This is perhaps a side effect of the unique possibility afforded to our study, in that our data collection spanned the societal change brought on by the pandemic, but limited opportunities to recruit the initially desired sample size. The extreme variation in IPAQ-SF scores also prevented the data from being conclusive. While others have reported successful uses of the IPAQ-SF for people with blindness or visual impairments (Matoso & Portela, 2020; Sadowska & Krzepota, 2015), the estimations of MET that the IPAQ-SF provides are not without fault. A systematic review found it to be a weak measure of total physical activity and to often overestimate the amount of physical activity compared to more objective measures (Lee et al., 2011). However, due to its wide use in the literature and the shortness of required response time, it is still perhaps the best estimate that can be obtained through remote questionnaire.
Our results offer further evidence that the pandemic severely affected those with visual impairments, complementing past research (Gombas & Csakvari, 2021; Mbazzi et al., 2020; Suraweera et al., 2021). Similarly, it may be possible to make the argument that those who regularly participated in exercise prior to Coronavirus-19 could not maintain exercise easily without the existing support systems on which they relied. As previously noted, people with blindness and visual impairments have reduced access to exercise (Capella-McDonnall, 2007; Matoso & Portela, 2020), and prior to lockdown, some of these factors included lack of disability-specific support, such as gyms and exercise classes being unable to cater to those with low or no vision. For individuals who did manage to exercise at gyms or classes, the closure of these places during the pandemic greatly hindered access and social distancing during outdoor exercise created further barriers.
Further research would be best directed towards identifying the best ways to make virtual exercise sessions more accessible. Some efforts have already been made in this direction, experimenting with tailored audio feedback through camera (Rector et al., 2013), multisensory interfaces (Morelli, Foley, & Folmer, 2010; Morelli, Foley, Columna, et al., 2010), and increasing enjoyment and motivation through ‘gamification’ of exercise (Barathi et al., 2018). The gamification of exercise, through platforms, such as Wii Sports or Xbox Kinect, has made a considerable impact on accessibility for people with injury or disability (Christine Higgins et al., 2010; Malone et al., 2016; Unibaso-Markaida et al., 2019). However, research is lacking on the inbuilt usability of these systems for those with visual impairments, and typically video games are designed for those with vision, unless specifically tailored otherwise (Gonçalves et al., 2021). We suggest that in the future, it could be beneficial to devote research attention to exploring methods to increase playability of online exercise games for users with blindness and visual impairments. In addition, validation of the IPAQ-SF and EBBS for people with blindness and visual impairments would strengthen the available tools for future investigations. Other more practical aspects of this study may be useful for designing more accessible exercise policies. For example, the participant who mentions that the local council run gym would not allow exercise without a carer points to a barrier that may be easily remedied with additional staff training and a more nuanced council policy on disability exercise.
Conclusion
The results of this mixed methods investigation suggest that, throughout the progression of the pandemic, access to exercise for people with blindness and visual impairments was initially severely impacted by the stay-at-home order. Thematic analysis offered further insights into the specific barriers to exercise participation. Suggesting that, the closure of gyms and facilities, and difficulties with social distancing as a person with blindness or visual impairments, combined with existing barriers, such as lack of motivation and lack of specialised support, to greatly hinder access to exercise in the early stages of the UK lockdown. However, in the later stages of the pandemic, we found that people established new methods to exercise at home and outdoors, which combined with their existing pre-pandemic methods once facilities began to reopen. This led to fewer perceived barriers to exercise compared to pre-pandemic levels. Overall, we maintain that for maximum exercise accessibility for people with blindness and visual impairments, offering specialised virtual exercise sessions may be beneficial, but that these cannot replace in-person sessions.
Footnotes
Appendix 1
Additional participant information, including gender, vision status (registered blind or registered partially sighted), age, and age of impairment onset.
Data accessibility
An anonymised version of the basic demographics, EBBS, and IPAQ-SF responses and the analysis script are currently available at: ![]() in a view-only format. On publication of the article, these data will be made publicly available. Responses to the open-ended questions have not been included in the repository, due to the disclosure of potentially identifiable or personal information.
in a view-only format. On publication of the article, these data will be made publicly available. Responses to the open-ended questions have not been included in the repository, due to the disclosure of potentially identifiable or personal information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.