
Abstract
Intensive Intervention Risk Management Service (IIRMS) is a time-limited enhanced level of input for those who are subject to probation service supervision and present with high risk and a likely personality disorder. In order to understand experiences of delivering or receiving this service and ways in which the service might address need or reduce risk, semi-structured interviews were conducted with all those providing the service (n = 10) and participants who had accessed the service (n = 9). Data were analysed using thematic analysis, first by group (provider or recipient) and then together. Themes concerning the ‘purpose of IIRMS’, ‘relational working’, ‘IIRMS experience’, ‘practical challenges’ and ‘outcomes’ were shared across the two participant perspectives whilst ‘engagement and change’ was unique to those accessing the service and ‘future directions’ to those providing the service. Addressing risk and promoting well-being requires an individual focus and flexibility and effective support and supervision for staff.
The Offender Personality Disorder Pathway (OPDP) is a programme jointly delivered by the HM Prison & Probation Service (HMPPS) and National Health Service (NHS) in England and Wales (Joseph and Benefield, 2012). The Pathway offers support to people on probation who meet specific risk criteria and are assessed as having personality difficulties. Input is also available in the form of consultation, supervision and training for probation practitioners (PPs) who supervise this group in the community. The aims of the Pathway are to improve public protection, to improve service users' psychological health and to train, develop and support a competent workforce (Joseph and Benefield, 2012; Skett et al., 2017). Intensive Intervention Risk Management Services (IIRMSs) form part of OPDP services and are available only to people on probation who are eligible for OPDP core services. IIRMS provision has its origins in models originally designed and piloted in London (Craissati and Campbell, 2018) and Liverpool (Baker et al., 2013) and is intended to provide additional input to individuals who need further support due to specific factors relating to their risk or psychological health (Craissati et al., 2021). IIRMS services differ in their regional implementation (informed in part by the availability of local resources and existing provision); however, all services are based on national IIRMS guidance (NHS and HMPPS, 2022). Whilst there are no published data on the average duration of IIRMS contact, the expectation is that these interventions are time limited.
Those accessing IIRMS services are a complex and high-risk group, as demonstrated through recall-to-prison rates. For example, in one study, approximately one third of those accessing IIRMS were recalled to prison (Craissati et al., 2021), rising to approximately 60% of service users accessing a specialist high-intensity and extended-duration IIRMS programme (Ryan et al., 2022). Direct comparisons with recall rates for other groups of people released from prison on licence is difficult because of the ways in which figures are calculated and reported (see Ministry of Justice, 2024, for data limitations). However, official data provide a proxy proportion of licence caseload recalled in June 2024 as 6.52% (Ministry of Justice, 2024). However, PPs have reported IIRMS as helpful when managing people on probation, with improvements reported in service users’ self-awareness, ability to create therapeutic relationships and reduction in anxiety and stress (Webster and Gardner, 2021). However, this study also found barriers to people on probation accessing IIRMS, including factors associated with the person on probation themselves (e.g. ‘instability’) and issues with available facilities (e.g. the non-therapeutic environment of probation offices). From the perspective of those accessing IIRMS, people on probation have reported that they experience IIRMS practitioners as compassionate and able to provide practical and emotional support (Ryan et al., 2019). This study also noted that participants reported having been able to form a more therapeutic relationship with IIRMS staff than had previously been experienced with staff from other services.
The delivery model of IIRMS differs by region with unique and specialist features based on local resources, services and expertise. In South Wales, IIRMS provides two tiers of provision on top of the Tier 1 ‘core’ OPDP provision, which delivers case consultation, formulation and limited joint working (OPDP Wales, 2024). Tier 2 focusses on relational work, skill development and psycho-education and is typically undertaken by transitional liaison nurses (TLNs) and personality disorder probation officers (PDPOs). Tier 3 provides specialist intervention for complex needs (e.g. risk and trauma) and is conducted by forensic and clinical psychologists.
Whilst at least one aspect of the Tier 1 service will be provided to most of those meeting OPDP inclusion criteria, fewer access Tier 2 services and a smaller number gain access to Tier 3. Within Tier 2, the TLN team work directly with service users in the period before and during the transition from prison to the community or approved premises (O’Meara et al., 2019). This involves providing a bespoke service led by individual needs and may include working directly with the individual, liaising with other services and supporting the service user to attend appointments or to register with local services (O’Meara et al., 2020). Tier 2 services can also include dialectical behaviour therapy skills support, mentalisation-based treatment introduction and psychoeducational intervention (OPDP Wales, 2024). Tier 3 work involves the delivery of specialist psychological interventions to the most complex cases or those who are at risk of destabilising (OPDP Wales, 2024). Currently, Tier 3 work prioritises trauma-focused intervention, risk management support for sexual violence and collaborative formulations (OPDP Wales, 2024).
Due to these differences in service design and delivery, this study sought to explore the experiences of IIRMS within South Wales to inform future service development and contribute to the literature on IIRMS. In the current study, we interviewed both IIRMS practitioners and people on probation who had accessed IIRMS in order to gain an understanding of IIRMS from the perspectives of those delivering and those receiving the service.
Method
This study was approved by the HMPPS National Research Committee (reference number 2023-095). The research process was informed by the British Psychological Society (BPS, 2021) Code of Human Research Ethics, and all participants were required to provide informed consent prior to participating in the research.
Participants
Staff delivering IIRMS
All staff members working within South Wales IIRMS between June and September 2023 were invited to participate, and all agreed to do so. The 10 staff participants (SPs) comprised four psychologists, four members of the TLN team (three nurses and one healthcare assistant) and two specialist OPDP PPs (PDPO), with eight female and two male participants across the sample. In order to protect anonymity and to reduce the likelihood of quotes being directly linked to individuals, no further demographic information is provided, and gender-neutral pseudonyms have been used where quotes are presented in the text.
People on probation accessing IIRMS
Staff members working with IIRMS between March and May 2024 were asked to identify current or past IIRMS service users who could be approached to participate in the research. Of the 16 service users identified, a review showed that three had been recalled to prison, one had disengaged from IIRMS, one was no longer under probation supervision, and one was deemed ‘too unstable’ to participate. Of the remaining 10, one person declined to participate, resulting in nine service users who were contacted and who subsequently consented to being interviewed for the research (five men, two women and two who identified as transgender men). Ages ranged from 24 to 49 (mean age of 39), with most participants (n = 8) recorded as being of White ethnicity (one participant's ethnicity was recorded as Black). Most participants (n = 8) had an index offence of violence, with one index offence recorded as a sexual offence. Three participants were accessing IIRMS at the time of the interviews; of those who had ‘finished’ their IIRMS involvement, the longest time between finishing IIRMS and conducting the interview was around 18 months.
Procedure
SPs were recruited via an email invite with reminder emails. Those who responded to the email were given an SP information sheet and consent information. Staff interviews took place in person at probation service and NHS offices in South Wales.
Participants who accessed IIRMS (PWAI) were identified through a staged process. IIRMS staff were approached by email to identify current or past IIRMS service users who might be willing to participate in the research. This group was screened to ensure that members were still in the community, subject to probation, able to give informed consent and contactable. This group was then informed of the study and provided with the IIRMS service user participant information sheet. To minimise demands and costs on the individual, all interviews were scheduled to take place in conjunction with an existing appointment the participant had at probation premises. Informed consent was collected prior to starting the interview, which included informing participants that they have the right not to participate in the study and to withdraw from the study (although no requests to withdraw were received), that their involvement (or not) in the study would have no impact on their probation status and that their responses would not be shared with their PP, except in cases where safeguarding concerns were identified. No such instances were identified. Service user interviews took place in person at six different probation service locations in South Wales.
Interviews were guided by one of two semi-structured interview schedules – one for SP and one for PWAI (available from the corresponding author on request). Whilst these covered broadly similar domains, questions were tailored to access the viewpoints of each participant group. Questions were open-ended and were designed to explore people's experience of IIRMS by considering various topics. For example, questions for people on probation included ‘Could you tell me a little bit about what your IIRMS sessions are like’ and ‘What, if any, benefits have you had from attending IIRMS sessions’, and questions for staff included ‘What, if anything, works well about IIRMS in your experience’ and ‘What, if any, changes have you seen in your client since starting IIRMS work with them’. The interview guides are available from the corresponding author on request. SP interviews lasted between 27 and 57 min (average of 44 min), and PWAI interviews lasted between 16 and 32 min (average of 23 min). All interviews were conducted by the first author and were recorded using Microsoft Teams in order to aid transcription. Participants were given a SP or PWAI debrief sheet at the end of the interview as appropriate. All interview transcripts were checked for accuracy and amended where necessary by the first author within 3 weeks of the interview taking place.
Data analysis
Transcripts of the interviews were analysed using thematic analysis as described by Braun and Clarke (2006). First, all SP interviews were individually coded before themes were identified and drawn together across SPs. Next, PWAI interviews were individually coded before themes were identified and drawn together. Finally, the thematic summary from each group (SP and PWAI) were pooled, which resulted in the identification of three theme types: those unique to the SP group, those unique to the PWAI group and those present for both SP and PWAI groups. Microsoft Excel, Word and Visio were used to aid data analysis and visualisation.
Results
Seven main themes emerged from the data – five themes shared by both participant groups, one theme that was apparent only in the SP data and one theme that was apparent only in the PWAI data. As can be seen in Figure 1, each main theme contained between two and four subthemes, and for the shared themes, most subthemes were present in both groups. Whilst there is no hierarchy of themes implied by the order of presentation, they are detailed below in an order which is consistent with a journey – starting with the general purpose, moving through what happens and how it is experienced and concluding with outcomes and future directions. This hopefully provides a flow between the themes which enhances readability and understanding.
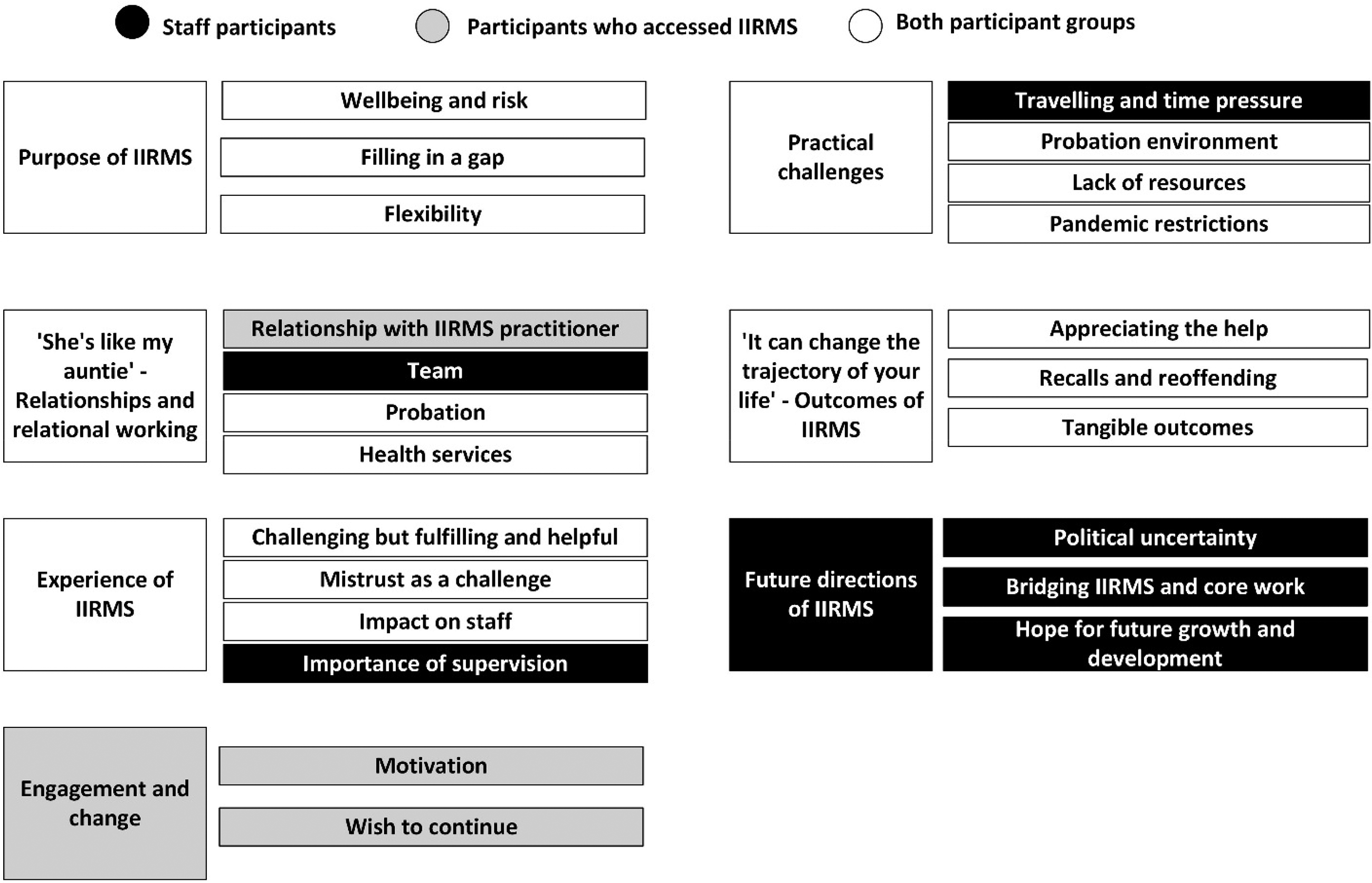
Shared and specific participant group themes and subthemes.
Throughout this section, quotes are used to evidence and enrich the theme descriptions, with pseudonyms used to maintain participant confidentiality.
Purpose of IIRMS
SPs and PWAIs identified two key functions of IIRMS, namely, [Risk management] goes hand in hand with well-being. Obviously. Because you’re dealing with the way that … how well I connect with others… my place in society…. (Bruce, PWAI) And I guess that if we enable people to be aware and manage their emotions better, then that will also have an impact on their risk. (Alex, SP) I've got ongoing mental health problems … and sometimes I need I need professional intervention. You know, … it's difficult to access. (Cliff, PWAI) I think the initial sense was to see what CMHT [Community Mental Health Team] could provide but then sort of like as soon as you start saying ‘but there's another service’ they back off and let other services take over. (Jay, PWAI) I think we're trying to fill some of the gaps that maybe can’t be filled by health or there isn't sufficient provision in HMPPS. (Jamie, SP) I was actually meant to have [other interventions] as part of my release plan … but that never happened, never happened. I was meant to be engaged with mental services through probation, didn't happen … my last probation officer said it was due to cutbacks and lack of money. (Cliff, PWAI) My sense is that what we're trying to do, and this this sounds a little bit awful when you say it out loud, but what we're trying to do is do the minimum possible to help people before we move on to trying to do the same with somebody else. Now if you tried to help someone to the extent that they had all of their trauma fixed, if you like, if that's even possible, you might be working with someone for two or three years. (Blake, SP) In other services I’ve worked with umm, you know you would discharge people if they weren’t engaging … but I think the IIRMS model recognises actually withdrawing services, it's kind of it's perpetuating some of those difficulties. … It's also very individually tailored each session and each IIRMS intervention. (Cameron, SP) But [IIRMS practitioner] has always said, like, if it doesn't work, we'll find something else. And I've never had that before. I've never had that sense of ‘we will do what you need’. (Jay, PWAI) That was the first session I think was like her trying to figure out what she needed to do with me. And then it was she built all the sessions around what like what she felt needed work … it was like aimed at my, what I needed help with, … and it might be different for a different person. (Matt, PWAI)
“She's like my auntie”: relationships and relational working
Both participant groups spoke about the importance of relationships within IIRMS and beyond. Relationships could be seen in layers – the inner most layer being the direct contact between the SP and PWAI whilst the outermost, the relationship between services. PWAIs talked about their [IIRMS practitioner] was very supportive … she’d try her best to help and whatever and I could ring her up … to talk to about what is going on. … Yeah, I think we have a good [relationship] yeah. Professional. (Drew, PWAI) After about the third session I felt like I’ve known [name of IIRMS practitioner] forever. She's like my auntie. I just talked to her and talked to her. Some of our sessions went on for like 2 h. (Matt, PWAI) Umm, she tells me off. But we’ve got that rapport over time. To me [IIRMS practitioner] is like an authority figure, maybe she doesn’t look at herself like that. She will tell me to get right back on the horse. So yeah, I think it's good. It's good for me to have that relationship. (Alan, PWAI)
SPs emphasised the importance of the second layer of relationships, other OPDP professionals. Staff enjoyed working as part of a I really like it that there feels like there's nothing to fight against for me in terms of people having very different views about things. I think recruitment to the pathway has been really good … I find the staff within the team really supportive, and you can sort of go to anyone of any discipline and any grade and talk to people about difficulties or successes or whatever it might be. (Blake, SP) The team is a wealth of kind of experience in terms of and different job roles as well … probation officers like PDPOs, psychologists, nursing. Like, I feel like it's a kind of range of knowledge in terms of support. (Ashley, SP)
Perhaps, inevitably, SPs spoke of working closely with other We work very closely with our probation um colleagues, which is very helpful because if we're struggling to engage someone in the community, we will usually sort of like tack on to the end of a probation appointment. (Taylor, SP) Sometimes people are on leave or long-term sick. And then you you're not able to get hold of the person so having to try and find out who else you can get hold of. … because we're not based in the team, we're kind of supposed to do outreach work in the sense … that can sometimes take more work to get hold of people. (Cameron, SP)
The final layer of relationships was those with professionals from [TLNs are] not seen as NHS nurses. … like within the mental health teams, they don't always recognize [TLNs] as NHS, so that can be a little bit of a challenge sometimes. (Ashley, SP) There's long waiting lists. Quite often, if we start [working] with people, they’re more reluctant to kind of take them on rather than more willing because they assume that they're getting some therapy somewhere. Certainly, the forensic risk aspect is often used as a … gatekeeping thing to other services, so they'll refuse to take them on because of the potential risk to others. [Max, SP]
Experience of IIRMS
IIRMS was experienced as They can help you a lot, they can. They help you, like they've helped me a lot. Like … they've done a lot, a lot for me. (Beth, PWAI) it has an immediate effect … the stress I felt inside myself, one day I felt like a certain way and then overnight that dissipates and I felt a different way. That's a massive thing. Even things like relationships now and connecting with people, um there's a whole new outlook… It touches on every part of you. There's an uplift in every area of your life. (Bruce, PWAI) one time I left and I don't know, like [many] years of tears just started streaming and they didn't stop all day… Yeah, yeah, there's sometimes it's hard and sometimes I just wanted to stop. Sometimes you’re just like, do I want to go through this again. (Alan, PWAI) It's an absolute gift of a job. Really, I can't sing its praises highly enough, and it's a tremendous opportunity for all of us that are involved with the team. (Alex, SP) I did get the sense [IIRMS practitioner] wants to do the job, you know what I mean. And she wants, she's not just going through the motions. She wants [IIRMS] to work for me. (Jay, PWAI)
The nature of the service user population accessing IIRMS was discussed with specific attention to She didn't trust mental health services either, so that was a big thing because of previous experience. So, to try and build that relationship at the CMHT took a lot of work with us doing joint work with them, with her. (Ashley, SP) [Service user's name] has had a lot of history of being let down by mental health services, so it quite badly damaged our relationship to the point where he was pretty sure he didn't want to work with me. (Taylor, SP) I struggled, you know, like speaking to people. I don't know why I find I find it hard. Yeah, but with [name of IIRMS practitioner], it is easy and I felt comfortable straight away. (Ron, PWAI) But, but you know, then I told her things like, yeah, maybe I haven't even told people you know who I've known forever, you know. So yeah, I did have a good trust in [name of IIRMS practitioner]. (Matt, PWAI)
However, SP also recognised that IIRMS work could have a had a We have to get used to as well disappointments. So, you can work extremely hard with someone, and they reoffend. And that can be difficult. Sometimes we have, due to the nature of the people being high risk, we have suicides and that can be tough when you work closely with someone and when they reoffend seriously, it's really hard. (Avery, SP) Sometimes when you feel a bit responsible or completely responsible for someone disengaging it makes you think really hard about whether I could have done that differently, but also you know to go a little bit easier on yourself is sort of like, you know, there were a whole host of other things going on in his life, which may also have contributed to that decision. (Blake, SP) Um some things that are more likely to kind of affect me than others, but yeah it is [hearing about trauma] it is very hard, especially if it's around often links to kind of sexual abuse. Obviously that that's very hard to kind of listen to. (Max, SP) I don't know if it's putting too much on [name of IIRMS practitioner] by doing this. (Alan, PWAI) I had a lot built up, you know [name of IIRMS practitioner] is probably there now with all of my stress on her shoulders. (Matt, PWAI)
For staff, the what the pathway do extremely well is supervision… We'll have a good chat about all the things that may be playing on my mind. Some of the stories I've heard and like [supervisor] will help sort of carry that burden with me. You know, I'll get a chance to discuss it. I'll get a chance to say ‘Oh God, it was awful. I've heard the worst thing ever last week and it's really stayed with me, I've really been thinking on it’ and then we'll talk it through and I think I don't think any of us could do this role without the supervision that we get to help us not suffer too badly from transferred trauma. (Taylor, SP) Because everyone is very busy, and I suppose a lot more reactive than I've experienced previously. There's often not supervision regularly on any of these issues either to kind of look through the content of anything that's been distressing or that may have impacted. (Max, SP)
Engagement and change
Engagement as a theme was unique to PWAIs who spoke of the need to be in the right headspace and to have That's the other important thing that I think has to be taking into account is somebody's motivation. … if somebody is not fully committed to engaging in this work and to be open and honest. Or they're just simply not in that space, you can't expect this work to help. (Bruce, PWAI) Back then [IIRMS practitioner] … was gonna … try and do some work over the phone. But I just wasn't in the right headspace as I was out drinking all the time. (Drew, PWAI)
The I am grateful because when I thought it was coming to an end, I thought it was just gonna stop. Just like you know, I think it's just the the way it continues a bit and it's like that long goodbye. It is there to try and help nip in the bud little things from one moment to another. (Alan, PWAI)
Practical challenges
Numerous practical challenges faced in delivering and accessing IIRMS were identified. SP noted the So, I was in [City 1] this morning, for example. I'm in [City 2] this afternoon … If we tell someone to turn up in a place that they haven't been to before or they're not familiar with, they won't turn up. So, we have to turn up in the place they're familiar with. So, I get that … [but] I've lost whatever that is 3 odd hours by travelling. (Blake, SP)
The Of course you know, you you’re still be watched, aren't you? So, you’re still under eyes. So, it can be quite daunting. (Emma, PWAI) probation offices, for a lot of people are quite challenging places to be. They can remind them of lots of things that they've done that they're not terribly proud of. Uh, they could also be incredibly chaotic. They can bump into people there that they don't necessarily wanna bump into, etcetera. So, the environment itself can be a barrier to some people. (Blake, SP) I don't like coming in. It's actually all right once you're in a room, it's fine. But I don't like the waiting room and stuff like that. It's the people in the waiting room, not the actual waiting room [laughs] Yeah. You just you don't know who people are … And being trans and gay as well. … It's just that environment doesn't feel that great. (Jay, PWAI)
Given the timing of the interviews, it is perhaps unsurprising that COVID-19 I don't think [face-to-face sessions] would have made a difference. … I think even if she came up however many times, I still don’t think it would have made a difference to where I was then. (Drew, PWAI)
“[It] can change the trajectory of your life”: outcomes of IIRMS
PWAIs spoke in general ways about I know at one point I didn’t think I was deserving of [IIRMS] because, I became, I was a victim and then I became a perpetrator and ended getting locked up… So yeah, so that makes a lot more sense now. Yeah, and I’m grateful for that that understanding because I didn't feel like I deserved it you know, but I'm grateful to have participated for what it's done for me. (Alan, PWAI) I always talk with people in supervision about the idea that you never know what you're prevented from happening. So, the support you're able to give to somebody might mean that either they don't commit an offense or they don't take drugs or they don't go out on an alcohol binge, but you'll never know because you're measuring something that didn't happen. (Blake, SP) But I think I would have gone back to jail if I hadn’t had [IIRMS]. (Alan, PWAI) something that I did notice about myself is when I received the help that was hitting the spot … there was no desire to offend. (Bruce, PWAI) He was telling me about how he was, you know, structuring his time differently and that he had daily routines that were helping him to keep grounded in away from different people and negative influences. (Morgan, SP) So, we've done the [specific psychometric measure] pre and post. He has achieved a reduction in every area of clinical symptoms that was present before, but [what's] more important [is] his self-report and he looks like a different person. He's taking care of his health. He's re-engaged in voluntary work. … And now he's started a relationship. He has got plans for future about paid employment and really important he's reduced his crack use to minimal. (Jamie, SP) before the trauma work, there was a slight noise at night I'd be so hypervigilant I wouldn’t be able to sleep. But now something wakes me up, it doesn't bother me and doesn't linger so much. It's it's woken me up, but I can settle down again and I can relax and go back to sleep. (Alan, PWAI) If you are emotionally ready [for IIRMS], you can deal with the biggest contributing factors that are destabilizing you … And that can make a massive shift and change the trajectory of your life and lead you to different things. (Bruce, PWAI) it's been very difficult to engage people. People have just been too chaotic or not really something that they want to do … I haven't really seen a great impact … I don't feel like I could say that's successful or that there's a lot of like … good news stories. (Max, SP) if I lost my temper or something, I wouldn't be thinking like oh I need to start breathing … I don't think it's stuff like that you could use in in the real world to be honest. … I don't think if you were in the pub you would just like lay down and start like counting to 10 and stuff like that. It could be a bit awkward. (Ron, PWAI)
Future directions of IIRMS
The direction of the service was a theme unique to the SPs in which they shared anxieties for the future and changes they would both want to and expect to see happening to IIRMS. Some participants expressed concerns about IIRMS because of Well obviously, we don't know anything for certain. We don't know what you know government and we are aware that obviously it is all kind of always under review. (Ashley, SP) I think a lot of that [the future of IIRMS] is a political question because all depends what government's in … I think there's always that little bit of insecurity with that as well. If a different government came in, they might go ‘Oh no, we don't want all these people in the community …’. (Avery, SP) Perhaps also for us to upskill the probation practitioners and, you know, to give them a few of the skills that that we've acquired so that perhaps they might be able to incorporate that and reflecting in their everyday practice. (Alex, SP) And I've seen people being referred through to IIRMS and … people have been stuck for ages … I do wonder whether we could equip PPs to do some of that work. (Morgan, SP) I can see it [IIRMS] growing and strengthening … it's like … a building going up …… foundations are in and the … bricks are … sort of heading up. I'd like to see … nice, bright, shiny building. It doesn't fall down. (Robin, SP) I would just like to see that [IIRMS] continue now to continue to grow and because I think … we keep consistently proving and showing the Commissioners that what we do is making a difference. I really do believe that, and I think the more we can show that we've made a difference and we are meeting a necessary need, hopefully the more we can keep expanding and the more we can keep offering the service to more people who need it. (Taylor, SP) What I really wanna do is set up a [specialist intervention] service within the pathway. …a couple of days a week … where a small team of us. … maybe four or five of us … could see four clients a day, each over 2 days. So, if there's four of you seeing, four clients [a day] are 16 people. That's 32 cases [in 2 days]. That's crazy numbers for a forensic service when currently we're able to see two people a week. (Blake, SP) Perhaps ideally … a separate sort of resource … enough of a resource to be flexible for the people that are hard to reach you, unable to engage in weekly therapy or maybe I know there's things like rolling groups or therapy groups that more people could access. … increasing some resources … specifically for people that need that lower level intervention just to help prepare them to do some of the more intensive work. (Cameron, SP)
Discussion
The seven themes derived through pooling the data from people on probation and staff delivering IIRMS provide important insights into the views about and experiences of the South Wales IIRMS service. The findings reveal the extensive overlap between the perspectives of staff and those accessing the service in relation to the service purpose, relational working, IIRMS experiences, challenges and outcomes. It also provides insights into perspectives specific to staff concerning service future directions and people accessing the service regarding engagement and change. Together, the findings provide details about key aspects of IIRMS service delivery, the challenges and possible outcomes.
The focus of IIRMS on reducing risk and increasing well-being is a formal part of the IIRMS specification (NHS and HMPPS, 2022) and indeed the OPD services as a whole (Joseph and Benefield, 2012). However, this study revealed that alongside this overarching aim, IIRMS is seen as a flexible and responsive service, potentially filling gaps in other services. Additionally, the importance of readiness and the relationship were regularly discussed in the interviews in terms of both service delivery and their relationship to change. These facets provide some information on ‘how’ the service is being delivered alongside ‘what’ is being delivered and warrant further description and research.
The experiences of IIRMS reported by participants align with those reported in previous IIRMS research. This includes the extent to which IIRMS is experienced as helpful (Webster and Gardner, 2021) whilst also recognising the potential impact on staff of working with trauma, abuse and harms. Hearing about traumatic experiences and offending behaviours is a common aspect of working within criminal justice settings (Ko and Memon, 2023). However, working with a client group who are high risk and have complex needs, many of whom may have a common origin in trauma and adversity (Ford et al., 2019, Skett et al., 2017), may intensify the scale and extent of the experiences being relayed to staff. Perhaps inevitably, staff recognised the importance of supervision to support the worker themselves and the integrity of their work (Davies, 2015). For example, supervision can provide a mechanism for maintaining boundaries and acknowledging and responding to the impact of work on well-being (Moore, 2012). More recently, the importance of staff supervision and organisational consultation when delivering trauma-informed practice and care has begun to be recognised (Davies and Jones, 2024). While there are multiple supervision arrangements in place in Wales OPDP which are detailed in the IIRMS Model document (OPDP Wales, 2024), two SPs considered their supervision to be insufficient. Further research could help shed light onto access to supervision alongside what is helpful and effective for supporting workers to undertake their roles.
Perhaps inevitably, staff recognised mistrust towards services by many people with whom they worked, although similar to Ryan et al. (2019), the current study found the relationship between PWAIs and their IIRMS practitioner to be supportive. Indeed, PWAIs in the current study spoke of their high motivation and engagement to work with the IIRMS practitioner. The role of motivation and the importance of trust for establishing an effective working relationship between people on probation and probation staff have long been recognised (e.g. McNeill and Weaver, 2010). Trust between people on probation and probation staff has been linked to rates of recidivism and within forensic mental health to engagement with treatment (Cartwright et al., 2022). Linked to this, PWAIs also emphasised how IIRMS is tailored to the individual, which has been recognised as important within both probation (McNeill and Weaver, 2010) and forensic mental health services (Cartwright et al., 2022).
Although some of the practical issues identified by SPs may be a consequence of the geographical area covered by the service, ideas such as upskilling other workers and reviewing how service delivery is provided were suggested to address these. However, the negative impact of conducting IIRMS sessions in the probation environment was identified as a practical challenge itself in both this and previous studies (Webster and Gardner, 2021). Whilst aspects of the IIRMS service such as the TLN team (e.g., O’Meara et al., 2019) are routinely delivered in other settings, extending this approach could be useful, especially where this might be seen as a way to foster access and engagement. This could include learning from the one-stop shop approach developed for women subject to probation, which provides a suite of services (including probation) outside the context of a probation office (Berry et al., 2014). However, besides the OPDP cohort focussed on in this study, careful consideration of the service setting could be useful for a wide range of other groups such as those who are vulnerable, those with neurodiversity and those with physical health problems.
Although individual experiences of IIRMS (both staff and PWAIs) were described in positive terms, formal outcome evaluation was seen as challenging. However, the individual focus of IIRMS provides opportunities for utilising a wider range of methods and approaches that may be more appropriate and informative. Indeed, participants identified domains of interest (e.g., self-care, establishment of routines, substance use and abstinence, appointment attendance, use of coping skills, engagement with family and prosocial use of time), all of which could be approached through individual goal setting (Davies et al., 2022) and individual outcome measurement (Davies, 2011). Further work should be undertaken to examine how routine outcome measurement, tailored as necessary, could be established within individual IIRMS work.
Staff described future service directions for IIRMS and ways in which the IIRMS service could further develop and grow (Skett et al., 2017). These included opportunities for connecting IIRMS work to other OPDP working. Despite this, some SPs voiced concerns about the influence government priorities may have on the nature and direction of IIRMS in the future. However, this may indicate a lack of familiarity with the joint 5-year strategy which outlines plans for OPDP delivery, including IIRMS, through to 2028 (NHS and HMPPS, 2023). It may be necessary to consider how such broader information and strategy is shared with practitioners in a timely and succinct way.
Limitations of the current study include the focus on a single IIRMS implementation area although the findings in this study appear to align with and extend learning derived from other IIRMS research. In addition, only service users who had either completed IIRMS or were accessing IIRMS at the time of the interview were included. As a result, the experience of those who do not complete IIRMS due to recall or disengagement should be a priority area for further IIRMS research given the link between treatment non-completion and recidivism/reconviction (McMurran and Theodosi, 2007). This should also include those who are sceptical about the impact IIRMS involvement has had on them. As with much qualitative research, there is the potential for selection bias in the convenience sampling approach adopted. Consequently, those PWAI who found IIRMS useful might have been more likely to be invited or to participate than those who had more negative views of IIRMS. Future research may wish to adopt a more general sampling strategy in which a random sample or all those who have received an IIRMS service are invited to participate. Other voices that future research should seek to capture include PPs, agencies also providing services to individuals who access IIRMS, service commissioners and family members of those who have accessed IIRMS. Finally, the researcher who conducted the interviews is employed as a research and evaluation officer by the Wales OPDP team. However, the emphasis for this role is to identify both what works and what does not work in order to inform service delivery. Supervision and a reflective diary were used to ‘test and challenge’ the interview schedule and the themes as they emerged, whilst participant quotes were used to embed the themes within the interview transcripts from the participants.
Conclusions
The findings presented here provide important information for practitioners and commissioners working with or referring to IIRMS. Overall, the flexibility and the trusting relationships formed within IIRMS between IIRMS practitioner and service user support engagement and a focus on well-being and risk. Whilst there are practical challenges in providing and evaluating the service, the service is seen as helpful and filling gaps in other services. Supervision for staff, especially for working with trauma, and the consequences of offending behaviour are important for the long-term sustainability of this workforce.