
Abstract
Local communities within oil producing countries in Africa often face formidable environmental challenges that generate conflicts and concerns around exploitation, environmental impact, and health risks. A key feature of these concerns has been the paucity of effective risk communication mechanisms and the impact this has on the public understanding of risk. Risk communication has been identified as a significant factor in explaining why the health consequences of environmental degradation remain unabated in oil producing communities. This paper evaluates health risk communication in the oil rich Niger Delta region of Nigeria. The study is based on 69 interviews conducted in the Niger Delta region. The paper argues that the health of the local population is being impaired by risk incidences relating to oil and gas exploration activities, the effects of which are amplified by inadequate communication of health risks to the public. The study argues for and suggests ways in which health risk communication processes can be improved in the Niger Delta. A multi-dimensional framework for public health risk communication is developed as a means of advancing understanding, practice, and policy.
Introduction
… societies at risk will often neither have the resources to deal with a major pollution incident or accident, nor can they afford the costs of the chronic health impacts associated with polluting processes. (Aroh et al., 2010: 246)
This situation is particularly acute in sub-Saharan Africa where there have been recent discoveries of oil and gas reserves in countries such as Ghana, Kenya, Uganda, Tanzania, and Mozambique (McDonald, 2012; Vasquez, 2013). The result is that many of the poor, often uneducated locals in these oil communities find themselves having to manage and cope with complex environmental and health issues for which they are not equipped. Invariably, they lack the skills, information, and capital needed to mount an effective challenge to the powerful interests that lie behind local resource exploitation. The lack of effective mechanisms for health risk communication in these societies has been blamed for the high numbers of causalities and increasing deaths (O'Rourke and Connolly, 2003) and for escalating social conflict (Stern, 1991). While it has been suggested that a health risk communication approach that is context specific is important in addressing such health challenges (Plough and Krimsky, 1987), existing approaches are often inadequate within the African context because the dynamics between powerful interests and trust affect the tenor of the interaction between local communities and the various authorities. Added to this is the need to communicate with substantial numbers of people (if not an entire population) in a tailored way.
The oil rich Niger Delta region of Nigeria provides a highly relevant context in which to explore health risk communication. There have, however, been very few such studies and so the use of risk communication as a potential mitigation strategy is an area that needs further attention. Dodoo and Hugman (2012) identified several factors impeding effective risk communication in sub-Saharan Africa including limited ability to collect useful data, few credible and reliable scientific assessment practices, and few robust risk management and public communication strategies. When considering the role of the media in such situations, Edafienene (2012) found that the media had little or no influence on risk-related policy decisions in the Niger Delta. Work by Aroh et al. (2010) assessed oil spill incidents and pipeline vandalism in Nigeria between 1970 and 2006 and examined the potential danger posed by such activities to public health. However, none of these studies considered whether effective public health risk communication had taken place and they largely neglected the structures and the processes through which risk communication occurs. As such, it is the relationship between the demands associated with risk communication and the needs of local communities that are the main focus of this paper. The paper aims to: (i) explore the extent to which risk is effectively communicated in the Niger delta region; and (ii) design a risk communication framework that considers both the structure and process of risk communication.
The concept of risk and risk communication
The construct of risk and the associated processes of risk assessment and risk analysis have proved to be a subject of considerable debate within the academic community and across various communities of practice (Fischbacher-Smith et al., 2010; Gratt, 1987; Herkert, 1991; Rogers, 2000). Within the context of this paper, risk is understood as the likelihood of negative or undesirable events or outcomes occurring (Renn and Roco, 2006) where something of human value (especially human life) is at stake (Jaeger et al., 2013) either in the short or the long term. There are several considerations that are important within the context of this paper. Firstly, risk assessment is shrouded in uncertainty, which creates additional demands on an already complex risk communication process, especially in terms of expressing uncertainty to different audiences (Fischbacher-Smith et al., 2010). Secondly, where something of value is at risk, an emotive dimension infuses all communication processes. Thirdly, many risk assessments are socially constructed and the calculation of risk (as both probability and consequence) does not have strong predictive validity. Fourthly, the absence of formally calculated risk due to the uncertainty noted above is not proof of safety. Finally, there are costs and benefits associated with most forms of risk (Zerbe, 2008) and these accrue in different ways to different segments of society. Importantly, the benefits accrued from investments and commercial activities, for example are often experienced by parties who are not exposed to the negative aspects of risk. Distributive inequalities arise in these situations that complicate matters further. Risk communication is therefore a complex process that involves unequal stakeholder interests, emotive topics, and technical issues that may require scientific expertise in order for them to be appreciated in full.
Traditionally, risk communication has been conceptualised as information transfer from expert to non-expert – often termed the ‘deficit model’ (Wright and Nerlich, 2006). This approach is based on the premise that the public simply do not have all of the facts or the skills needed to understand risk. It is also assumed that they are largely ignorant of the facts, passive in terms of knowledge generation, and thus need to be educated. In practice, however, communication is often quite different, characterised by public groups who often have a nuanced ability to deal with issues of risk (Irwin and Wynne, 2003). Moreover, there has been a growing recognition that risk communication is an interactive, two-way process between the communicator(s) and the recipients of the message (Grönroos, 2004; Shannon, 1961) and one that is potentially enhanced by advancements in technology. The ‘two-way communication model’ (Shannon, 1961) recognises that feedback is essential for effective communication and many of the current working definitions of risk communication have adopted this interactive model. Löfstedt (2008), for example, defines risk communication as the exchange of information about health risks caused by environmental, industrial, or agricultural processes, policies, or products, linking individuals, groups and institutions. As such, the need for dialogue between communicators and stakeholders has been identified as a prerequisite for any successful risk management (Palenchar et al., 2005). In particular, the language used to communicate both the risk and the uncertainty that surrounds it, is important to the risk acceptability process (Irwin, 2006).
One of the challenges in communicating health risks to the public is the need to communicate with large numbers of people within diverse groups (Bennett et al., 2010) using language that is relevant to all the different end users of the information. Bernstein referred to the codes used in communication as ‘elaborated code’ to refer to the language of middle class educators, and ‘restricted code’ referring to the language of children from the lower working classes (Bernstein, 1964). He argued that this imbalance in the codes used to structure communication led to the disadvantaging of certain classes of children who could not access the meaning embodied within the elaborated code. Within risk communication, ‘elaborated code’ can be used as a shorthand for the language of experts, and ‘restricted code’ to the language of non-experts groups (Elliott and Smith, 2006; Smith, 1990). Within this context, the efficiency of risk communication could be severely compromised when it is carried out using a code that the receptor group has little knowledge of, or access to, or where they are unable to decode the uncertainty that might be inherent in the calculation of the risks themselves. The oil and gas producing Niger Delta region of Nigeria offers an opportunity to consider how risk can be communicated to the local population and where powerful stakeholders can mask the uncertainty inherent in risk analysis and distort the processes around risk acceptability. Moreover, the region is ethnically varied and has a predominantly poor population (Odoemene, 2011) that has been exposed to risks related to oil and gas exploration and production, and is typically unable to mount a challenge to the technical expertise provided by the oil companies or to muster the political power necessary to challenge government and its agencies. The remainder of the paper considers the nature of the environmental problems within the region and uses this as a vehicle to consider the nature and effectiveness of the risk communication process.
Study area: The Niger Delta and the nature of environmental and health challenges
The Niger Delta consists of nine states (Figure 1) with over 37 million inhabitants who constitute 22% of Nigeria’s population (National Population Commission, 2006). Within these are over 1500 communities who act as hosts to the oil industry (Forest and Sousa, 2006). The region largely consists of rural communities, but includes some important Nigerian towns such as Port Harcourt, Warri, and Asaba. The inhabitants in the region generally live below the poverty line and rely on fishing and agriculture to survive (United Nations Development Programme, 2006).
Nigeria, Niger Delta Region.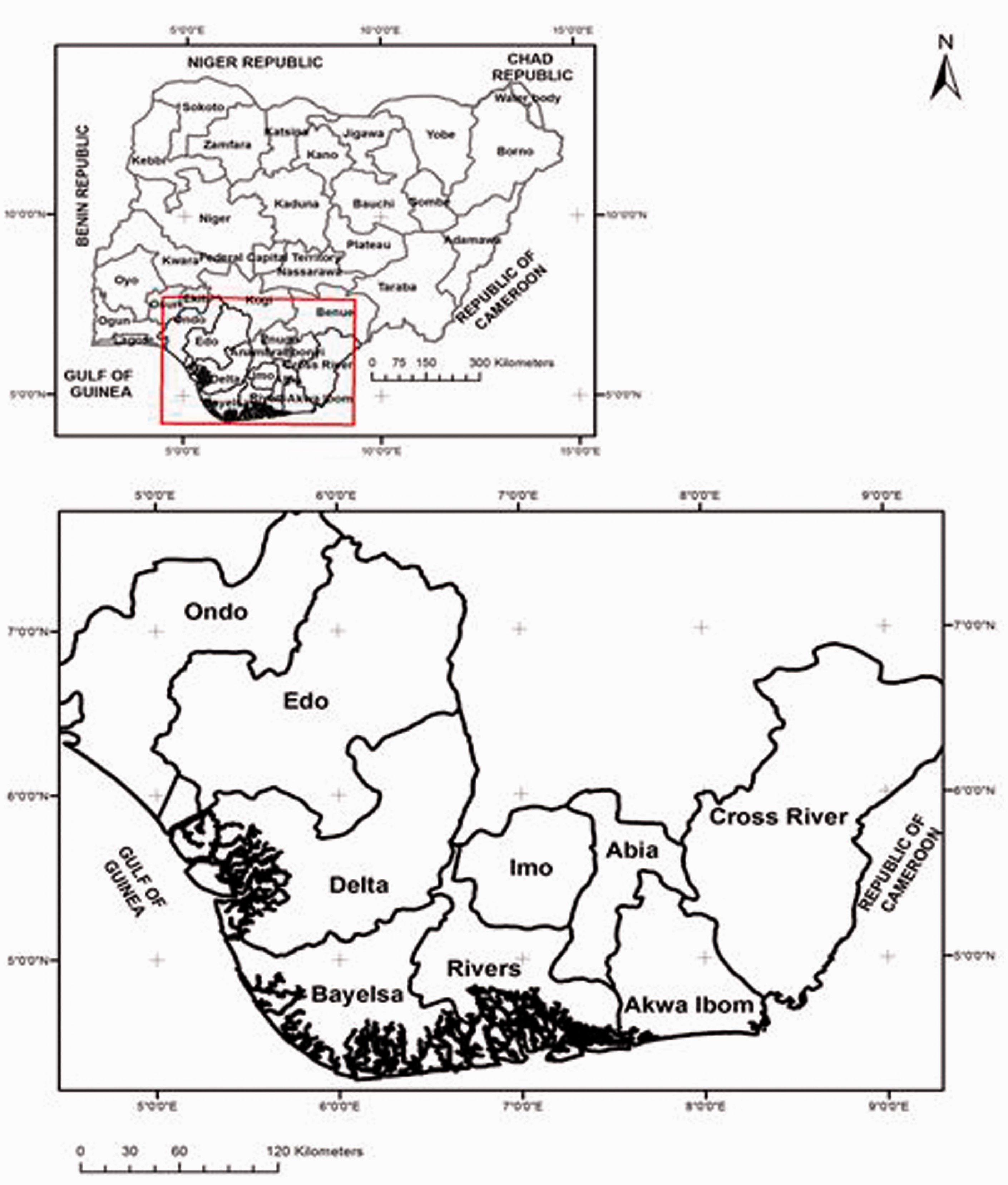
The Niger Delta region is home to the oil wealth that has made Nigeria the largest producer of petroleum in Africa and the sixth largest oil producer in the world (Watts, 2004). In the Niger delta, oil spills are a common occurrence and have been linked to corrosion of pipelines, poor maintenance of infrastructure, spills or leaks during processing at refineries, human error, and intentional acts of vandalism or oil theft (Amnesty International, 2009). The United Nations Development Programme (2006) estimates that between 1976 and 2001 there were approximately 6800 spills totalling 3,000,000 barrels of oil. Likewise, it was reported that there were 253 oil spills in 2006, 588 oil spills in 2007, and 419 cases in the first six months of 2008 (Yakubu, 2008). According to data from the Shell Petroleum Development Company (2014), around 324,000 barrels of crude oil in about 1500 incidences were spilled from its facilities between 2007 and 2013 (Figure 2). Shell reports that of the total volume of oil spilled from SPDC facilities in 2013, about 75% is due to sabotage/theft, and 15% due to operational spills resulting from corrosion, equipment failure, or human error. However, Amnesty International has challenged Shell, accusing the company of misrepresenting oil spill data and misleading the public (Amnesty International, 2013).
Number and incidences of oil spill in the Niger Delta (2007–2013).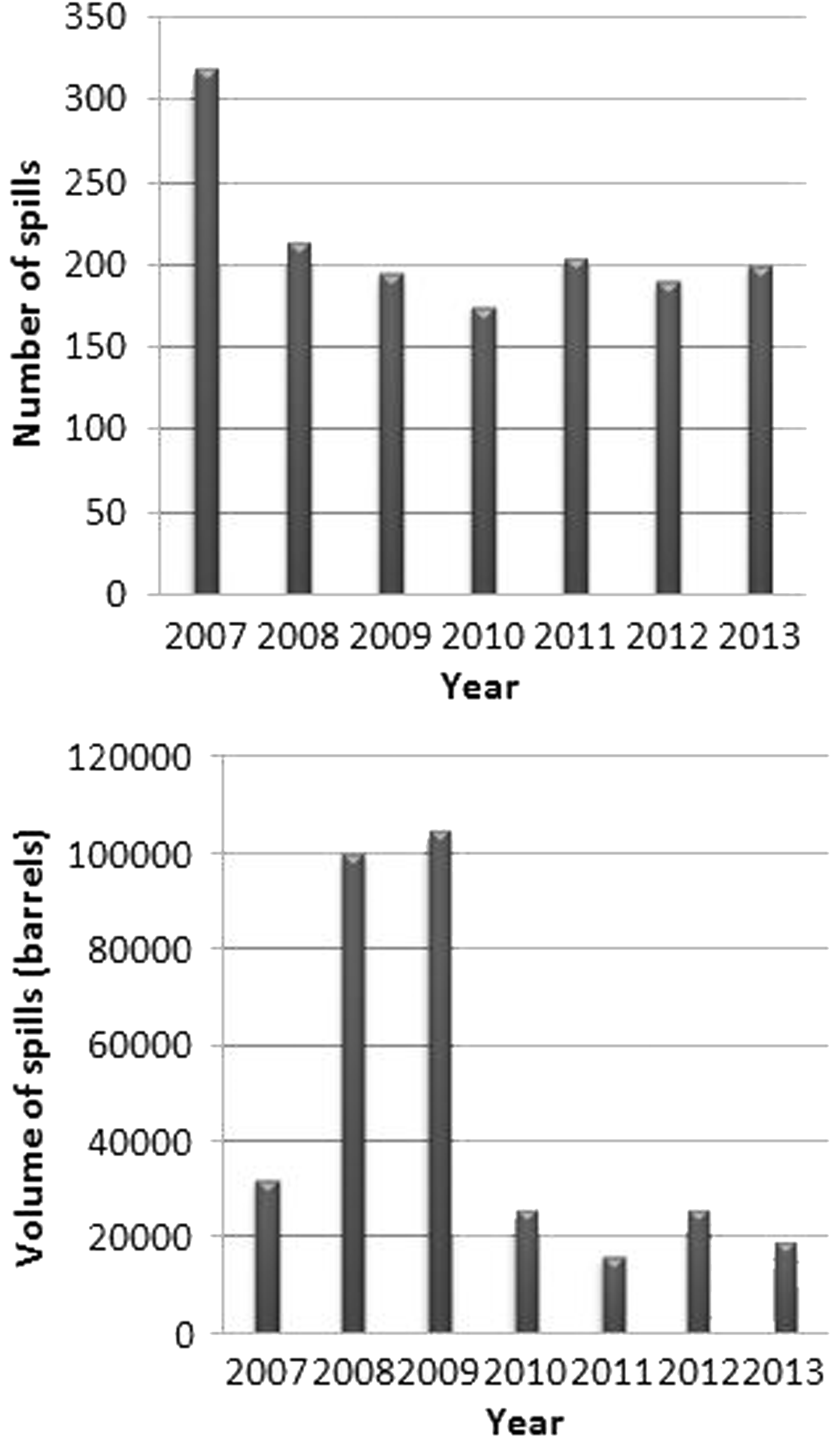
Health implications of oil spills in the Niger Delta
Frequent and collectively substantial spills have amplified the health challenges faced in the region. In 2011, a United Nations Environmental Programme (UNEP) report revealed that drinking water in Ogoniland was found to contain a known carcinogen at levels 900 times above World Health Organization guidelines (United Nations Environment Programme, 2011). In another study, it was found that oil spills reduce the ascorbic acid content of vegetables by as much as 36% and the crude protein content of cassava by 40%, which results in a 24% increase in the prevalence of childhood malnutrition in the region (Ordinioha and Brisibe, 2013). In the same study, it was found that animals that come in contact with crude oil could be hemotoxic (destroying red blood cells) and hepatotoxic (destroying the liver), and could suffer infertility and cancer. Figure 3 for example, shows a polluted fishing lake with oil crude that could be detrimental to human health when consumed.
Polluted fishing Lake in Oporoma community.
Gas flaring is another major source of environmental degradation resulting from oil exploration activities with serious health risk implications (Dung et al., 2008). Flaring of natural gas from oil stations as a by-product of crude oil production has been a normal occurrence in Niger Delta (Opukri and Ibaba, 2008). It has been suggested that more gas is flared in the Niger Delta than anywhere else in the world (Friends of the Earth International, 2004). Data from two flow stations (Kolo Creek and Obama) show that on average approximately 800,000 m3/day of gas is flared (Ishisone, 2004). Gas flares increase the risk of disease, food insecurity, and weather damage (Werner et al., 2015). Emissions from combustion of associated gas (AG) contain toxins, such as benzene, nitrogen oxides, dioxins, hydrogen sulphide, xylene, and toluene (Edafienene, 2012). Oil spills and gas flares contaminate surface water, ground water, air, and crops with hydrocarbons and these can easily accumulate in aquatic organisms and food crops on which the locals depend (Nriagu, 2011). Respiratory problems such as asthma and bronchitis, lung disease, heart attack, miscarriage, and skin disease are just some of the reported cases becoming prevalent as a result of exposure to heat from oil exploration-related activities (Ovuakporaye et al., 2012). However, the extent to which other confounding variables (e.g. economic instability and a lack of understanding of the exposure to risk) have contributed to these health problems requires further investigation.
The federal and state governments have the legislative mandate of communicating such health risks to local people. The responsibility for health risk communication is fragmented and can fall to at least three government agencies: the Federal Ministry of Health has the overall responsibility to strengthen the national health system; the National Emergency Management Agency (NEMA) is responsible for coordinating resources towards efficient and effective disaster prevention, preparation, mitigation and response in Nigeria; and the National Orientation Agency has as one of its duties offering liaison services with agencies and local government to promote smooth, rapid and efficient communication.
Methodological approach
The study was based on 69 semi-structured interviews conducted with respondents drawn from three communities Oporoma (OPO), Odi (ODI), and Yenagoa (YEN) in the Niger Delta. The communities were purposively selected because they are oil-producing communities that have experienced health risks due to activities of the oil industry. These three settlements are similar in terms of population (YEN – 17,112, OPO – 20,822, and Odi – 23,020), but are dissimilar in that while OPO and ODI are riverine communities, YEN is predominantly dominated by freshwater swamp forests and has relatively higher land. Face-to-face interviews took place between June 2010 and November 2010. Twenty-three households were randomly selected in each community, and the household head interviewed. The selection of 23 households from each community is not because these communities are of equal geographical size or population but so the data itself could have equal weight on the analysis/interpretation. The number (23) selected in each community is well within the range of 12–60 recommended by Patricia and Peter Adler in (Baker and Edwards, 2012). The interviews explored two broad areas: (1) the demographic and socio-economic characteristics of respondents; and (2) their knowledge of risk and their perception of and engagement with health risk communications. The latter were examined through discussions of incidents that had occurred within that community, and consideration of the communications received before and after risk incidences. Respondents in one of the three communities were asked further questions on a recent oil spill. An interview was also conducted with one government official. Unfortunately, it was not possible to interview respondents from the oil companies because of their reluctance to participate.
Data analysis
With total recourse to ethical considerations addressing issues of privacy and confidentiality, informed consent, and harm to participants (Hay, 2010), interviews were audio recorded and then transcribed into written form for closer analysis. In this study, visual information (such as facial expression, gesture or body orientation) was not deemed an important aspect of data analysis. Digitally recorded data were transcribed and verbatim quotations were used where it is possible to understand the English language used. Paraphrases in brackets were used where it is difficult to understand the Pidgin (popular local language). Two of the authors are fluent in both the English and Pidgin languages and were able to verify the translation to avoid distortion as Thornbury (2006) suggests. Features of talk such as emphasis, speed, tone of voice, timing, and pauses can be crucial for interpreting data (Bailey, 2008) and were noted during the transcriptions. Transcripts were read through coded and emerging ‘themes’ identified and discussed in the results and discussion session. Data collected were analysed using thematic analysis (Bryman, 2015).
Results and discussion
In response to the question ‘what is/are the greatest concerns for your health?’, all sixty-nine respondents pointed to the oil-related environmental hazards in the delta. This appears to be the main source of health concern in the region and all of the respondents were able to mention at least one health effect of oil spill or gas flaring (such as difficulty breathing, heartburn, eye pain, headaches, and skin conditions). Some respondents were also concerned with the swampy land which allows the impact of the oil spill to spread more quickly through the community. Air pollution and contamination of water sources were identified as posing the greatest health risk due to effects on everyday water supplies, agricultural produce and aquatic species that the local population directly consume and use as a source of income. This finding is synonymous with studies that claim that oil spills and gas flares contaminate surface water, ground water and air with adverse health implications and that damage to the livelihood of the locals (Nriagu, 2011; Obiajunwa et al., 2002; Ovuakporaye et al., 2012).
Level of risk communication
The respondents were asked if they had received any communication relating to environmental degradation such as an oil spill or gas flare. Only 13 (19%) of respondents had received any form of communication. Notably no communications were received from government or corporate organisations. Rather, information came from relatives, neighbours and friends. This underscores the role of social relations in risk communication and the importance of informal, sometimes hidden, channels in the supply of risk information (Fischbacher-Smith and Fischbacher-Smith, 2014). These 13 respondents were asked to rate the level of risk communication they received before and after the risk incidence and the usefulness of the information in mitigating health risk. Interestingly, all the respondents rated risk communication both before and after as low or very low such that it was insufficient to rely upon when taking risk-mitigating actions. One of the respondents said: No, nobody told us when something like this will happen, anytime it happens we just see it and if we are lucky we have someone (member of the community) to alert us. (OPO – 1)
He went further to say that If we get good information, at least we can do something (act), but as the situation is, we don’t get any information … so how can we act when the problem has already happened.
Although most of the information had not come from professional risk communicators, the content of the information was deemed relevant to the circumstances faced, but not practical enough in terms of suggesting what response the population at risk could make. For instance, 1 of the 13 respondents who received information from an in-law said He just told me not to drink the water that it will cause cancer, but since I don’t know where else I will get water from, all we did was just to boil the water and drink. (OPO –2)
Some of the precautionary measures such as boiling water and thoroughly washing vegetables before eating are already entrenched in the day-to-day practices of people in the local areas around the oil and petrochemical installations. Almost 90% of those interviewed stated that they always boil their drinking water and wash their vegetables because of fear of possible contamination from oil and gas activities.
The study also examined the nature of risk communication between those in charge of managing the risk and the local community leaders following an oil spill incident. The incident considered was the early 2009 crude oil leak from a pipeline of one of the major oil companies into the OPO community and pristine Boupere Lake farmlands, with subsequent contamination of other sources of water. Following this incident, there were reported cases of health problems across the community. The people (communities) around here simply do not have the capacity to manage these things (pollution), they take water from other part of the lake because the oil is not visible and when they drink it they fall sick … our (community leadership) advice is for them not to even use the water for bathing until the company or government do something. (OPO – 3) It (pollution of Boupere Lake) was a major problem to our community … they affect our rivers and fish … we could not fish nor collect water. (OPO – 5)
It was confirmed that none of the residents received any prior information warning them of health hazards relating to oil spills. The community often became aware only when oil became visible and had already contaminated the surrounding environment. As the community leader, I have not seen anyone in my community since the incident occurred. No NNPC official, no AGIP official has visited us … They have destroyed our land, water, palm trees and streams. We are rural dwellers but here, the people have not taken the laws into their hands. (OPO – 3)
Despite representation from the community development council to inform the oil companies operating in the region about the spill, no immediate attention to avoid or stop further leakage was taken. According to a local youth: The oil company refrained from immediate action and legally maintained the position that the leak was a result of sabotage by local youths. After months of finger pointing as to the real cause of the spill AGIP contracted a local company for cleaning up of Boupere. (OPO – 4)
Neither was any advice given to the community on how to handle possible health risks. Some respondents claimed to have informed the Ministry of Environment but nothing was done either to stop the leak or to educate the population on the possible health risks they were exposed to. Some studies have, however, claimed that efforts to contain the spill are sometimes deliberately undermined or sabotaged by locals in some communities for many complex reasons including oil theft (Anifowose et al., 2012; Fabiyi, 2008).
Challenges and barriers to risk communication in the Niger Delta
The study also explored the barriers to, and opportunities for, risk communication from the perspectives of the local community, non-governmental organizations (NGO) and government. For example, NGOs (including faith-based organizations in this region) play an active role in informing and providing support to the local population (Ikelegbe, 2005). The study found that complacency, high levels of illiteracy, multi-ethnic diversity, limited access to main and social media (especially in rural areas), a lack of alternatives (such as economic activities, water, food, scarcity of land), emotional attachment to place, limited access to experts who were perceived to be neutral, and lack of trust between locals and government officials were some of the main barriers to risk communication in the Niger Delta. These findings are similar to the study by Dodoo and Hugman (2012) who asserted that there is limited capacity for credible and reliable scientific assessment and public communication strategies in sub-Saharan Africa. In part, this reflects the relatively low levels of scientific literacy in the region and the power gradients that exist between local communities and the corporate–government nexus. These imbalances generate the potential for exploitation by constraining effective risk communication and thus increase the degree to which the locals are susceptible to health risks relating to oil exploration activities.
One of the respondents from ODI community reported the frequency of oil exploration-related risk incidences such that they have simply stopped worrying about the health implications – most ‘residents are now accustomed to the problem’ (ODI – 2) he says, thereby suggesting that the people might have accepted that they must live with the risk and are powerless to effect change. It may also mean that they have developed a degree of complacency (a coping strategy) towards possible health risks, and the limited, or near absence of communication between the local people and health risk experts, has the potential to entrench such behaviour further. Some respondents suggested that a possible solution is for them to relocate far away from gas flare and spill plagued communities. However, the widespread land scarcity in the region and the high prices of land where it is available limit this option. Pervasive poverty in the region has also reduced the ability of the locals to take alternative actions even when the implications of their action or inaction are known. When we (himself and his household) drink the water, we are afraid of the possible trouble (implication)) it will bring to us, but I have no choice, even we cannot trust the water from the vendors and government don’t supply us with water. (ODI – 2)
This situation is confirmed by Audrey Gaughran, a Director at Amnesty International, who stated that: People have been drinking water without having the scientific facts before them – the report (No progress report) found some people thought the water was likely to be contaminated but had no choice, others just didn’t know it was contaminated because no one has ever told them. (Clark, 2014)
Narratives around (dis)trust.
There is, as a consequence, a tendency for the locals to view any message from the government and corporate organisations with suspicion, and this mistrust is prevalent amongst the key community stakeholders in the region. However, mistrust is also a two-way process. The government official interviewed suggested when questioned about one of the incidents that he was always willing to go to the communities and educate the locals but feared for his safety thinking he might even have been kidnapped. Even where it was possible for the government official to educate the locals, he may not have had the requisite skills required to communicate scientific information with a less educated and ethnically diverse population in a way that would minimise distortion. In Bayelsa state alone, there are five linguistic groups speaking over 40 different dialects (Alogoa, 1999). It was not surprising therefore, when the official stated that ‘even if you tell them, they don’t understand’.
From the interviews it was clear that the health of the local people was being impaired by a combination of oil spills and gas flaring that led to localised contamination of air, land and water resources by hydrocarbons. However, little was being done to educate or communicate with the public about the health implications of oil exploration activities either prior to or following an incident. There is therefore a need for improvements to health risk communication in the Niger Delta and so in the next section, the paper explores how that might be achieved.
Opportunities for effective health risk communication in the Niger Delta
There are a number of opportunities to improve public health risk communication in the Niger Delta. Chief among these is the opportunity for local people, oil company representatives and government officials to engage in a more open and transparent process of information sharing. While local people already rely on their social networks (such as families, friends and religious organisations) to share information about risk, these networks can also serve to reinforce misconceptions and misunderstandings around the nature of the possible threats. Social networks are highly important in the African context (Teye, 2013). According to respondent OPO 3 (cited above), community leadership does provide information where available. For example, in the recent Ebola epidemic outbreak in West Africa, village meetings in rural areas were organised to share risk information related to health with input from medical experts and those who had survived the virus (Boisvert, 2014). Those present at the meeting including community leaders then conveyed the information to extended members of the community, family members and friends who were not present. It is often the case that these villagers are familiar with the people who share such information and they are therefore more likely to trust the information source. There was also the involvement of social institutions (Adebowale, 2014; Gilbert, 2014; Niyi, 2014) where mosque and church leaders were involved in communicating the risk (Adogame, 2007; Ilo and Adeyemi, 2010).
The upsurge in use of mobile telephone technology and electronic social media represents a further opportunity to enhance the potency of these forms of social networks in risk communication (Veil et al., 2011). Increasing numbers of rural Nigerians are taking advantage of the global system of mobile communications (Baro and Endouware, 2013) which suggests that there is considerable potential to use social media as a platform for risk communication (Filou, 2013). Social media supports public access to relevant risk information and increases the likelihood of public interaction with organisations (or those in charge of managing risk). Communication can also be tailored to individual needs (Moorhead et al., 2013) and, as such, risk communicators in the Niger delta could also take advantage of the speed and reduced cost of social media platforms and accommodate the problems associated with elaborated and restricted code by tailoring messages appropriately to various key audiences.
A way forward – A public health risk communication framework in an African context
What is pertinent in determining the most appropriate forms of risk communication is the need to utilise multiple avenues and means of communicating risk in diverse, multi-cultural communities like the Niger Delta. Here, we propose a three-dimensional risk communication framework. At Micro, Meso and Macro levels (see Figure 4) communication must be carried out in a way that reaches the wider public, yet has local relevance for those at risk. Macro, Meso and Micro are levels that need to be applied in light of the nature of the hazard/problem, the size of the population at risk and the transferability or spread of the problem/source. For example, in the case of Ebola virus outbreak, what began as local can quickly become inter-continental such that the Macro level is in fact a global level of analysis and action. In contrast, an HIV-infected healthcare worker, though carrying an infectious disease, may have had only local impact such that macro level in that case is regional or possibly national depending on the degree of delegated authority within the country in question. The ‘governance’ of any incident will be a function of the legislation and organisational arrangements in place within a particular country or region. Consequently, there are multiple levels at which issues need to be considered, understood and managed and the risk communications need to be adapted accordingly. This is therefore no template, but rather a framework that could be applied in light of the circumstances at play.
Multi-dimensional public health risk communication framework.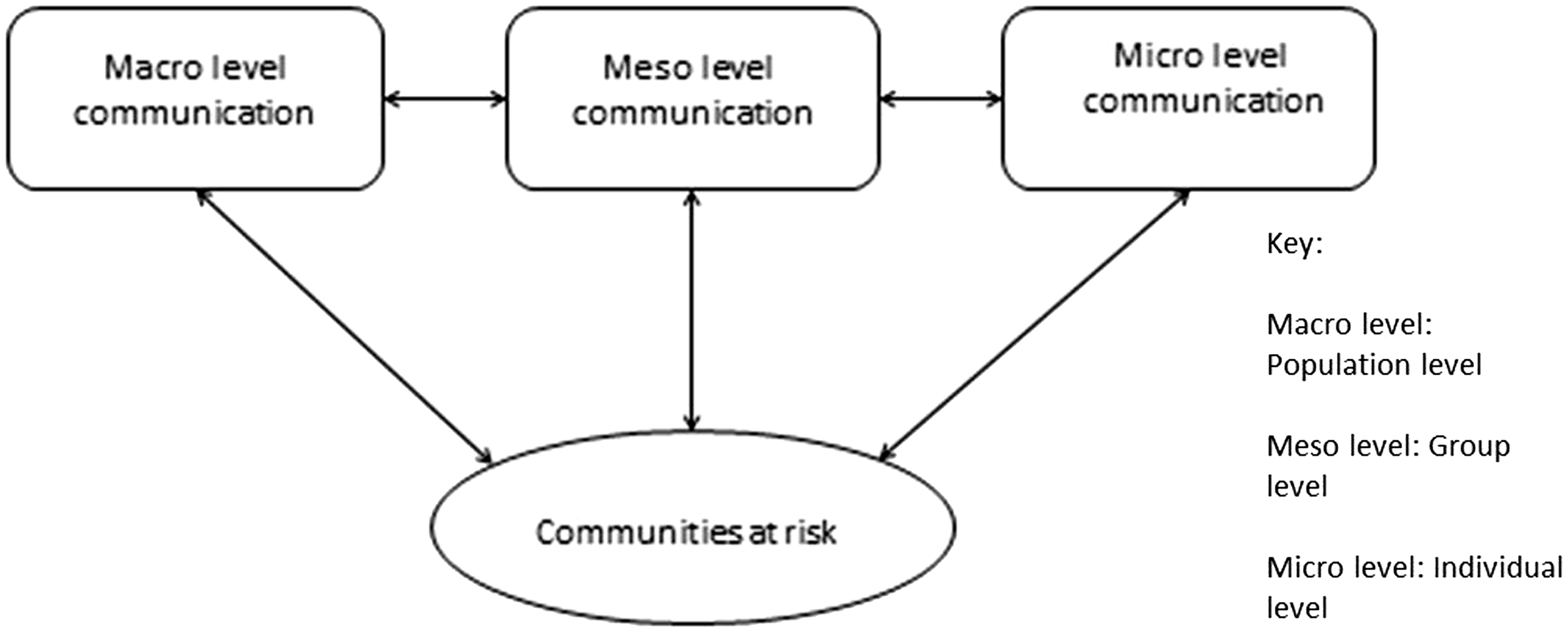
Within the context of this Niger Delta study, Macro communication is at the national level where communication is the responsibility of national designated agencies. The study found that while macro level communication was almost non-existent, the other two (Meso and Micro) were present with the micro level communication being the most prevalent and influential. There is therefore scope for a multi-dimensional public health risk communication space in communities such as the Niger Delta that allows concurrent risk messaging to the entire public and more tailored messaging to groups or individuals within the public, as well as the type of two-way communication reflected in contemporary risk communication in other cultural settings.
The macro level communication is one targeted at the entire population where risk information comes from national (or multi-national) designated bodies or organisations, and where the information is decontextualized to suit a broader public audience. Key priorities here are issues of broader interest with the aim of mitigating risk at society level and the need to have shared and common understandings of the risk faced, and the associated costs and benefits. The existence of different stakeholder groups means that different subjective interpretations are likely to be brought to bear on risk and close coordination and consultation is therefore required. Of importance is the need for the public to understand the inevitable tradeoffs and compromise in minimizing the risk in order to reduce the chances of conflict and grievance.
The meso level communication is closer to the source of risk, e.g. regional or local and where risk information in contextualised within its local context. Stakeholders at this level may be local policy makers, regional activist groups, support groups, agents (e.g. insurers) within the communities at risk. As this level, stakeholders often have different information requirements that will need to be satisfied and multiple and tailored risk messages will need to be designed accordingly. The challenge that then arises is that in framing risk messages specifically for different audiences, the original message can become distorted, thereby amplifying or attenuating certain aspects of risk (Renn, 1991). At this level, the use of local language and keen attention to local values and practices are required. This offers the potential to incorporate intrinsic values and local identity into risk messaging. The use of localised method and language in the Niger Delta, for example, brings with it an added advantage of allowing communication to take place in the diverse languages and dialects of the regions through involving town criers and other similar agents in the process.
The micro level communication may involve an individual communicating with the wider public (e.g. an influential community leader), one to one communication between people within a community such as doctor–patient communication, or one to one communication with representatives of support groups. At the micro level, informal communication may also occur, for example, between a parent and child or between adults in informal settings. It is important to note that one to one communication may also occur at the initial two levels e.g. a worried individual calling a national designated centre for specific information in an emergency for information. Emotive elements are at their strongest here, as the reality of the risk is felt very keenly indeed. The risk communicator at this level requires communication skills and local knowledge in dealing with the delivery of information and any potential aftermath.
While the community at risk is often the general public, there are different groups and individuals with different information needs and interest. Considering the lack of trust especially between the national designated agencies who are operating often at the Macro or Meso levels (typically owning the technically verified information) and other bodies at micro levels, we stress the importance of an integrated approach to communications across these three levels of risk communication to ensure clarity and consistency of message, to minimise amplification and distortion and to ensure an on-going dialogue between stakeholders that further informs communications. Moreover, communication is not one-way (from experts to the public), but multi-way and multi-level.
The means/medium by which risk is communicated is also crucial and utilising formal and informal channels (known and trusted mediums) could provide added advantages (Powell, 1991). Formal and information channels of communication can be supported by diverse means (see Figure 5) including (1) technology enhanced means, (2) traditional means (e.g. local, culturally specific custom and practice), (3) social institutions and networks and (4) professional avenues.
Different methods of communicating risk.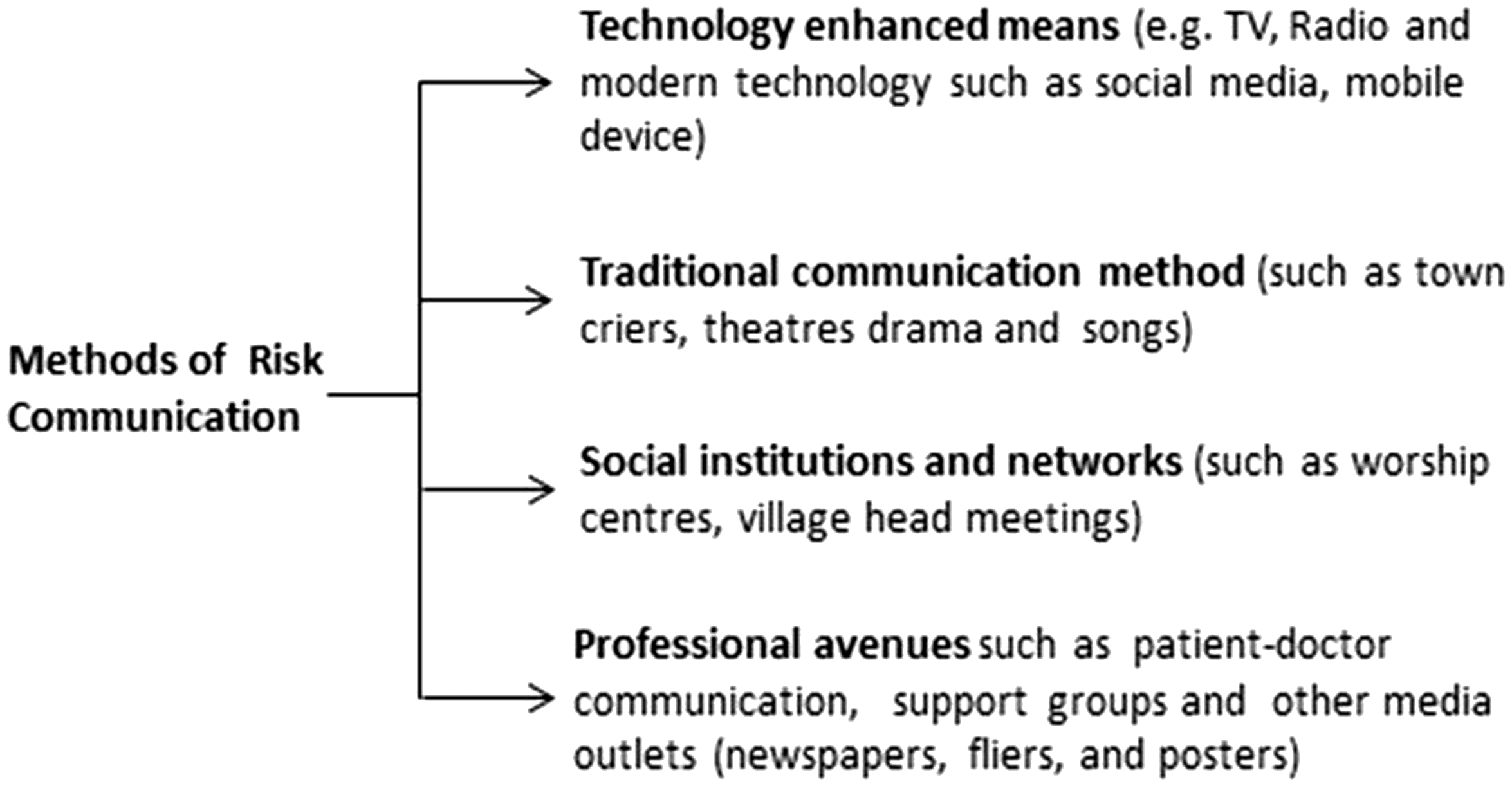
One of the strengths of this proposed framework is that it allows the coupling of formal and informal channels of communication, which in turn enables the wider public to access to information at all levels. The framework also presents a platform that creates a balance between communication from a trusted source and an expert source. This is particularly important where there is distrust amongst stakeholders or negative state–society relations that may create problems for effective risk communication. Existing literature on trust has highlighted the importance of trust in risk communication (Lundgren and McMakin, 2013) and it is generally accepted that risk information from a trusted source contributes directly to the way that individuals perceive and respond to such information (Frewer et al., 2003; Mayer et al., 1995). It is, however, a complex literature with debates about the relative importance of trust versus credibility which, although related, are not the same (Trettin and Musham, 2000), and the competing stakeholder interests arising from individual concerns versus the greater good (Leiss, 1995). These and other debates about trust building, regulatory environments and ensuring citizen representation to create inter-personal and inter-agency trust are beyond the scope of this paper and this study, but represent an area for future study in this particular Niger Delta research.
Conclusions and implications of the study
The near absence of formalised risk communication in the Niger Delta would appear to be an issue of some concern, especially if improvements to public health risk are to be made and conflict with the oil companies reduced. One of the biggest challenges concerns public confusion over what actions to take, especially in an emergency. Speed of communication and the availability of risk information are particularly important in terms of relocation or how to respond during periods when local water or food sources may be contaminated. The proposed multi-dimensional public health risk communication strategy has the potential to address some of these challenges by providing consistent and timely information that reaches a large public audience, and simultaneously provides information in its local context to those who need to take mitigating actions. The range of media also facilitates multi-way communications moving away from the traditional deficit model. This way, many health effects in the Niger Delta and similar communities may be reduced or even prevented.
There is a further opportunity to lessen the burden on the social health infrastructure. If citizens are provided with adequate and timely risk-based information about a particular hazard, they can then make choices about risk exposure. Similarly, there is a potential effect on economic welfare given ill health becomes an economic burden to families and communities. Improvements in economic welfare and social development may then in turn become a means of addressing the problematic trend of oil theft, sabotage, bunkering, illegality, kidnapping and conflict that has ravaged such communities.
While our framework addresses the integration across multiple levels and the combination of expert and local sources and elaborated and restricted code, it also highlights the complexity of the network of communications at play within health risk communication situations. We have not addressed in any detail the trust-related dynamics of unequal stakeholders and the varying incentives for change; rather, we have assumed a moral imperative for dialogue and pointed to broad economic and social benefits to the community at risk. Further research in the region and further development of the framework should be directed in these two areas so as to further develop the theoretical and policy perspectives offered here.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Some of the data presented in this article was collected by the fourth author during his PhD which was funded by Commonwealth Scholarship Commission in the UK.