
Abstract
This article offers a cross-sectional exploration of the COVID-19 containment strategy in Kerala and highlights its initial effectiveness in the Kasaragod district, the first to record a second stage transmission in the state with a cluster of cases from 23 March 2020 onwards. Despite its underwhelming healthcare infrastructure, Kasaragod district managed to contain the transmission and record a 100 per cent recovery rate, indicating a promising model of infection control. However, the district subsequently succumbed to community-level transmission when another wave of positive cases of COVID-19 was detected among repatriated overseas citizens on 7 May 2020. The article explores the confluence of elements that allowed the initial successful recovery from a second stage transmission and then examines the factors that later led to community-level transmission. Given the close connections of Kerala to other parts of the world through migration, the article illustrates how precariously the local is now part of the global.
Background of the Study
After a cluster of COVID-19 cases was reported in China’s Wuhan city on 31 December 2019, the novel coronavirus started its lethal transmission across the globe, infecting millions and claiming the lives of hundreds of thousands. The absence of a vaccine made it necessary to fight the virus with locally, regionally and nationally available resources and medical procedures. The transmission of COVID-19 occurs in four phases, namely first appearance through travellers who test positive, then local spread, followed by community spread and finally, widespread outbreak of a pandemic (Upadhyay, 2020). Since the first occurrence of COVID-19 outside China in Thailand on 13 January 2020, even nations with effective healthcare systems and elaborate healthcare administration like the UK and the USA have quickly slipped from the stage of local spread to community transmission. Analysis of data from many countries shows extremely rapid escalation from the second stage of transmission to the third, often within weeks.
The present case study records how local control measures in Kasaragod district in Kerala, despite being one of the state’s most underdeveloped districts in terms of healthcare systems, were initially successful in flattening the infection control curve within weeks, recording a 100 per cent recovery rate with zero deaths on 10 May 2020, even after second stage transmission. The combination of rapid and effective measures employed in the district was hailed as a potential model for infection control, until a sudden large influx of citizens returning to Kerala from overseas and other states in India occurred from 7 May 2020 onwards (Government of Kerala, 2020; Rai, 2020). This overwhelmed the district, along with the entire state, which now succumbed to stage 3 community-level transmission. Subsequently, Kerala has been witnessing thousands of new cases per day, and the earlier successes of epidemic control were rapidly wiped out. Despite determined local efforts to control the rates of transmission, the connectedness of the district’s population with other parts of the world ultimately overwhelmed the healthcare system.
Across the globe, the transmission pattern of this particular pandemic implicates the interlinked nature of the global and the local through various forms of migration and travel as a major risk factor. There were, however, other elements that had a critical negative impact. As COVID-19 spread, Indian migrant labourers working in the Middle East were often deprived of medical care and sometimes even basic needs. Suffering job losses, pay cuts, risky crowded accommodations and poor treatment facilities during the pandemic (Amnesty International, 2020), many migrant labourers became desperate to return home. This precipitated a large-scale return migration to India, with Kerala receiving the highest number of repatriated citizens (Rai, 2020). Since Kerala has a population density of 859/sq. km, more than twice the national average, and has the highest number of emigrants in India (Rajan, 2014), local healthcare systems which could earlier effectively manage the low number of infections were now overwhelmed by this sudden large influx of citizens from overseas, which also forced the state to relax its containment and isolation strategies. This soon led to rising numbers of cases that were undiagnosed or discovered late. Through such carriers, the state then gradually slipped into the community-level transmission stage.
This predicament underlines how the global and the local are inextricably intertwined in ways other than the economy and shows that this connectedness of the global and the local necessitates more robust ethical benchmarks in situations of humanitarian and medical emergency. Better treatment, not only in the host nations but also within some parts of India itself, could have avoided panic among migrant labourers, resulting in lower returnee rates, which could have prevented local pandemic control measures in Kerala from being overwhelmed.
To explore the initial success of control measures and their subsequent collapse, the article first presents some insights into the nature of Kerala’s healthcare system in the wider context of the ‘Kerala model’ (Parayil, 2000). It then discusses the trajectory of healthcare responses in two sections, showing first what worked well in the initial flattening of the curve. The discussion then proceeds to examine what went wrong later, when Kerala succumbed to community transmission. The realisation that the local and the global are precariously linked through the prominence of migration in today’s interconnected world stands out in this context, containing some lessons for future reactions to outbreaks of pandemic proportions.
The Healthcare System in Kerala: Background Analysis
The South Indian state of Kerala has long been one of the best performers in India when it comes to healthcare, with indices at par with those of advanced economies, largely as a result of steady investment in education and healthcare infrastructure by various governments over time (Kutty, 2000; Madore et al., 2018). The state has repeatedly been recognised as leading the nation in terms of healthcare indices by NITI Aayog, the planning and policy think tank of India (Paliwal, 2019). Despite not being economically prosperous, Kerala has managed to provide Universal Health Coverage (UHC) for its people to a great extent, which is still ‘work in progress’ in many developed nations, though opposition to UHC is manifestly based on ‘crude and faulty economic reasoning’, as Amartya Sen (2015) has forcefully argued.
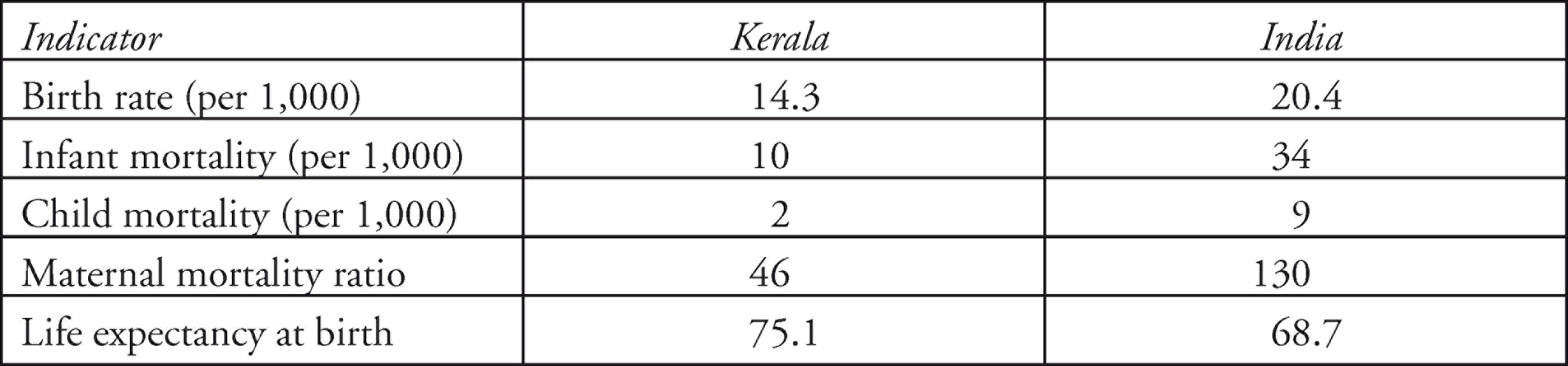
In Kerala, combining public and private sector engagement contributed to the sound overall standard of the state’s healthcare structure. High levels of education, especially among females, ensured that most people are aware of trends and developments in treatment. Unsurprisingly, there are 1.5 medical institutions per 10 sq. kilometres in Kerala, indicating investments in medical infrastructure, from both public and private sectors (Kutty, 2000). Mortality rates, too, one of the common indicators of health status, show Kerala’s health status at par with developed nations. The factors contributing to this strong position clearly relate to the growth of integrated medical systems in the public, private and cooperative sectors, combined with good health awareness of people as a result of educational advancements. According to statistics of the Kerala State Council for Science, Technology and Environment (ENVIS Centre Kerala, 2020), the health status of Kerala is a positive outlier among the states of India, as Table 1 indicates.
Major Health Indicators of Kerala in Comparison to India
In addition to this strong set of healthcare indicators, the state is also renowned for producing a skilled medical workforce through its network of at least 287 nursing institutions, along with support institutions for other medical professions. This medical workforce actually serves many parts of the world and has significantly contributed to outmigration of nurses from Kerala (Percot, 2006). More recent estimates show that 30 per cent of the nurses educated in Kerala work in the UK or the USA, 15 per cent in Australia and 12 per cent in the Middle East (WHO, 2017). This not only indicates that Kerala’s system of medical education meets the standards of developed nations, but it also shows, as this article argues, that deep awareness of activist healthcare interventions is one of the major reasons why the threat of the COVID-19 pandemic initially caused only minor damage at the local level in Kerala, even in the relatively disadvantaged district of Kasaragod.
Kasaragod is the northernmost border district of Kerala, with an area of 1,989 sq. km and a population of 1,302,600 according to the 2011 census. It is ranked 11th among the 14 districts of Kerala in Human Development Index with a score of 0.760, which is less than the state average of 0.773 (Government of Kerala, 2006). In this border district, infrastructure and services development have been slow, reflected in the healthcare sector as well. The district has just 209 hospitals in total, slightly more than the districts of Wayanad and Idukki, 2 districts with far less population. Also, these districts have more beds for treatment than Kasaragod (Government of Kerala, 2006). Notably, there was no functioning medical college in Kasaragod district, neither in the public or private sector, when COVID-19 infections began to spread. In fact, the district had been dependent on Mangalore city in the neighbouring state of Karnataka, which is a hub for healthcare services. To add to the local crisis of this border district, the state of Karnataka closed its borders with Kerala on 22 March 2020, citing fears over COVID-19 transmission through the borders (Cutinho, 2020). In short, as a negative outlier in terms of healthcare facilities in Kerala, Kasaragod now suffered even more because of its borderland position. And yet, it managed to handle the emerging crisis rather well.
Early Strategic Planning for COVID-19 Control in Kerala
The Ministry of Health of Kerala government anticipated the threat posed by the novel coronavirus well before any positive cases were identified in India, as many students from Kerala are studying in different parts of China, including Wuhan. Identifying the possibility of transmission through carriers travelling from China, the government opened a control room on 24 January 2020 in Thiruvananthapuram, the state capital, to closely monitor the emerging threat. This included making plans to quarantine people who travelled from the epicentre of the infection in China and to pool medical resources required to manage the situation in case of casualties (Rajan, 2020).
The first case of COVID-19 in India was reported from Thrissur in Kerala only 6 days later, on 30 January 2020, as anticipated by the state government (Reid, 2020; Unnithan, 2020). Soon two more positive cases were identified among students who had been infected in China before returning to Kerala. All three patients recovered and tested negative by 20 February 2020. The first episode of COVID-19 was thus successfully handled by the state, and the calamity warning, issued on 3 February after the initial identification of positive cases among 72 returnees from Wuhan, was withdrawn on 7 February (The Hindu, 2020a). However, the healthcare and administrative systems remained on high alert, and the control room and associated activities remained in operation.
When six new positive cases were reported in Kerala on 9 March 2020, this marked the second wave of positive cases to hit the state (Government of Kerala, 2020). Since then, the state authorities have been employing a combination of medical and social strategies, including aggressive testing and quarantine, to contain the spread of the virus. Since this second wave of cases began on 9 March 2020, Kerala has been experiencing a gradual rise in positive cases, mostly among individuals who returned from overseas. A considerable number of Keralites are working abroad, significantly contributing to the state’s economy and prosperity through their remittances. However, this gradual rise of positive cases diagnosed in Kerala also remained under control, until Kasaragod reported 80 positive cases within a short period of just 8 days, from 23 March to 30 March 2020, including 34 positive cases on 27 March 2020. This contributed to a sharp rise in the total number of cases across Kerala to 181 from just 61 active cases on 22 February 2020, suggesting the possibilities of an escalation to community-level transmission if unchecked, specifically in Kasaragod.
Flattening of the COVID-19 Curve After Second Stage Transmission
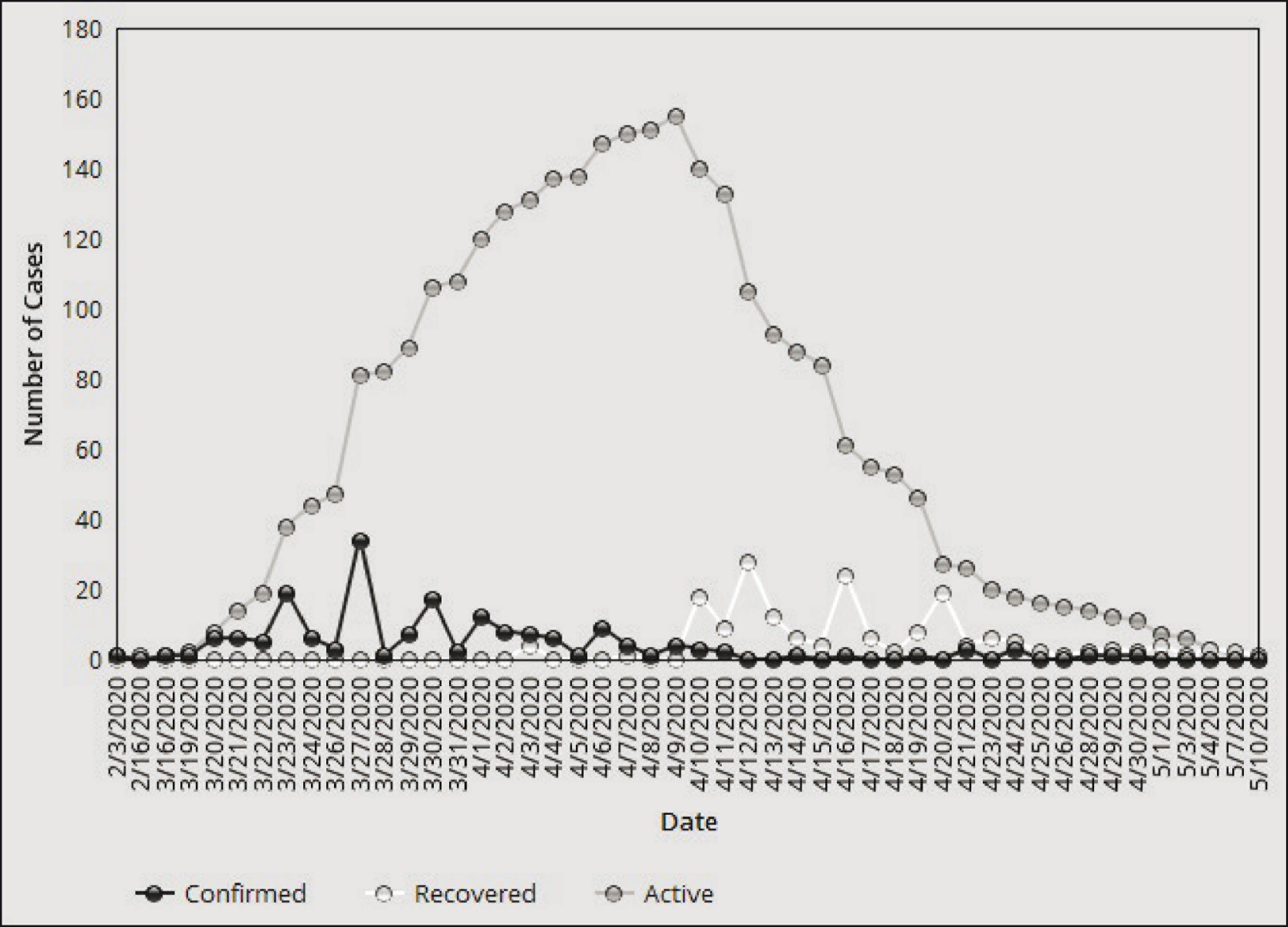
To reiterate, the cases reported in Kasaragod in the initial stages involved people returning from overseas. The district has a large number of people working abroad, contributing overall ₹511 million as annual remittance from abroad per year (Zachariah et al., 2003). Undiagnosed cases, mostly due to the absence of symptoms, led to a new pattern of transmission to people who had contact with carriers by late March, resulting in a cluster of cases in the district and the first recorded cases of local transmission in Kerala. However, the return of people from overseas was halted soon when international travel bans were imposed to prevent further transmissions. As a result, the COVID-19 curve was flattened in the district within weeks, as Figure 1 documents. Indeed, the district again recorded a 100 per cent recovery by 10 May. Being able to contain the transmission despite the progression of the infection to the local spread stage was commendable, especially since the district has one of the lowest-rated healthcare systems of Kerala.
Key Elements in the Kasaragod Model of Flattening the Curve
The successful initial containment of COVID-19 in the district was primarily due to a shrewd combination of social and medical efforts, facilitated by the state administration with the cooperation of various key stakeholders. Some of the factors contributing to this model further indicate the importance of local–global connectivities and the role of modern media.
First of all, practical lessons were learnt from the recent management of the Nipah virus. Kerala had encountered the deadly Nipah virus in May 2018, resulting in 17 deaths (ENVIS Centre Kerala, 2020; WHO, 2018), including that of a healthcare worker. In efforts to contain this virus, the state quarantined thousands of people and placed thousands more under observation in the districts of Malappuram and Kozhikode (Rejimon, 2018). The state even developed a virus protocol to handle infectious viruses, with the support of WHO, as reported by Varma (2020a). This protocol defined suspected cases, probable cases and confirmed cases. It also laid down strict guidelines for isolation of patients, quarantine of suspected cases, sample collection, sample transportation and use of personal protective equipment. These strategies of quarantining and observation were later used by the state to contain COVID-19 effectively. Remembering and using the Nipah protocol laid foundations for a successful transmission control system in COVID-19 infection outbreaks. Especially the practical lessons from the Nipah encounter and earlier emergencies in Kerala are reflected in actions taken by the state in managing COVID-19 cases and evolving a COVID-19 protocol based on the Nipah model (WHO, 2020).
The state government, right from the start, was aware of the danger of virus transmissions from overseas and employed control measures based on locating infected individuals, isolating them and aggressively testing all potential contacts. The government conducted symptom assessments in all airports of the state ever since the first COVID-19 cases were reported in January 2020. Individuals with symptoms were taken to hospitals, while those without symptoms were sent to home quarantine, supervised by a local healthcare facility. Cases identified as positive after being sent to home quarantine triggered a swift process, under which all people who were in contact with that person were necessarily quarantined and tested. In cases of people who were infected but were not put under home quarantine, a route map of the infected person was prepared with the assistance of mobile tower locations, and this was then published in open portals, including newspapers, without revealing personal identification details. Local people were asked to report in case they had come into contact with the infected person to investigate the possibility of local transmission. To ensure containment at the local level, the locations concerned were locked down immediately after diagnosing any transmission through contact. This rapid strategy paid off, but only while there was a manageable number of cases from overseas.
In this control process, dissemination of information through press briefings and live statistics was given much importance. Access to relevant information and being informed about the risky situation are key elements in avoiding panic among people and promoting hope and confidence in the community. Kerala excelled in this regard, maintaining a record of real-time data related to COVID-19 in the state through a dedicated website operated by the state government (WHO, 2020). Transparency in disseminating information and ensuring that it reaches the community was achieved through daily press briefings, right from the first day of identification of positive cases in the second wave until the curve flattened. These daily press briefings, by the female health minister or the state’s chief minister, provided updated statistics and instructed the community about the risks being faced. This dissemination of information was pivotal in giving a real-time picture to the people (Ramachandran, 2020).
The state also used a participatory approach to tackle the situation at the ground level. One of the key problems faced by developing nations in restraining COVID-19 from reaching the third-level community transmission stage has been the lack of effective mechanisms to trace cases, create awareness and ensure compliance at the grassroots level regarding social distancing. Despite limited resources, Kerala was able to excel in this aspect, too, again achieved through combining public and private sector efforts, coordinated by the state. Some of the key players in this regard were health workers, the state police force and volunteers from the community, as discussed below.
Accredited Social Health Activist (ASHA) workers are trained female community health activists selected from and working within the community. They act as an important bridge between the local community and the public health system, and India has around 900,000 ASHA workers spread across the country (Bisht & Menon, 2020). Kerala adopted a ground-level approach through a Rapid Response Team consisting of ASHA workers to closely monitor the situation in local communities. Kerala’s approximately 26,000 ASHA workers act as the government’s local vigilante mechanism, keeping a tab on people under home quarantine through house visits and also looking out for people entering the locality from other places. As members of the community, ASHA workers share interpersonal connections with local people, which the government put to highly efficient use at the grassroots level, treating such women as ‘foot soldiers’ in the battle against COVID-19, as Varma (2020b) put it. In addition to monitoring the situation and alerting the healthcare system, ASHA workers have been distributing protective equipment like masks and sanitisers, provided by local self-governance bodies, at doorstep level. This model has proved highly effective in the entire state, especially in Kasaragod.
The state also allocated one-third, that is, around 200,000 persons, of its official police force in COVID-19 containment operations, at considerable personal risk to such staff (Shan, 2020). Though the standard operating procedure (SOP) of the state police force did not have a protocol for pandemic response, the force was quick to devise a strategy. The primary responsibility of the police was to ensure lockdown of public spaces and prevention of gatherings. However, what made the services of the police force commendable in Kerala was that they rendered services other than law and order maintenance. The social network handles of the state police department, popular for fun-packed informative posts, have around 2.5 million followers across different online platforms. The police force used these platforms to educate local people on the intensity of the situation, procedures for social distancing, quarantine and the need for staying at home (Aiyappa, 2020). Also, along with the state’s firefighters, the police assisted needy persons with acquiring essential services like medicines. In Kasaragod, the police certainly acted as a decisive force in preventing community-level transmission by strictly enforcing lockdown measures, while remaining communicative.
Also, the volunteering efforts of community members contributed much to overcoming difficult situations. While non-co-ordinated volunteering by random individuals or organisations could do more damage than bringing benefits, through possible transmission by volunteers, to tackle this situation, the state government rolled out a plan to enlist more than 200,000 volunteers aged between 22 and 40 years through government channels. Respondents hailing from a specific region were deployed in their locality after being trained. The registration for volunteering was online, and these volunteers delivered food and other amenities to people quarantined in their homes. The volunteers were also deployed in other social awareness creation activities after training under the supervision of local administrative bodies (The Hindu, 2020b). These trained volunteers became a key force, helping the administrative system in reaching out to home-quarantined people who were short of resources, especially in places like Kasaragod, where many people were quarantined under lockdown after the identification of local transmission.
Co-ordinated Welfare Measures and Allocation of Resources
Effectiveness in administering a plan to contain the threats of a pandemic depends on administrative agility and people’s cooperation. No matter how stringent the laws, people will not co-operate with a lockdown situation or social distancing if they lack resources to satisfy their basic needs. Foreseeing this, and concerned to avoid panic, the state rolled out a set of additional welfare measures targeting vulnerable sections of society. To ensure that all people have access to basic needs such as food, the government distributed 15 kg of food grains to 8,114,000 households through the public distribution system (Krishnakumar, 2020). Besides, the government also implemented a large financial package of ₹20,000 crores for welfare measures, including health packages, subsidised meals, loan assistance and welfare pensions. The state, especially in view of ensuring the food and social security needs of migrant labourers, opened 4,503 relief camps, where labourers were provided food and recreational facilities, which also contributed to the containment of the pandemic (Nileena, 2020).
Despite limited financial means, Kerala was able to allocate resources efficiently, as seen in the early establishment of a control room, allocating a financial package, training volunteers and using ASHA workers as community-level monitors. As noted, the district of Kasaragod, where the first instance of local transmission in Kerala was identified, had no medical college when the first infections were detected. The state set up a modern COVID-19 treatment centre within 4 days in this district, a facility which is now entitled to be upgraded as a fully functional medical college (Philip, 2020). The state was constantly pooling medical resources like rapid test kits and protective equipment to ensure their availability (Varghese, 2020). Determined, cool-headed planning ensured success in allocating the available resources effectively, although Kerala is not the strongest among India’s states in terms of financial resources.
Reversal of the Infection Control Curve After Influx of Repatriated Citizens
As is evident from the cross-sectional analysis discussed above, initially, Kerala had a system of infection control that was performing well. However, once the initial curve was under control, the state faced a combination of factors that led to a reversal of the initial successes in infection control. The case is evident from Kasaragod, where a complete flattening of the curve was in place by 10 May 2020, but the infection then escalated to a community transmission in the following months. The key elements in the successful model of flattening the curve followed by the state were still in place, but a few newly introduced factors disturbed the equation. The new situation that led to the reversal of the infection control curve and caused the failure of the previously accepted model of infection control now needs to be examined.
As indicated, Kerala largely depends on foreign remittances from Keralites working mainly in the Middle East and Europe, who constitute a powerful economic and political section of society. Around 2.4 million Keralites in various countries contribute about 36.5 per cent of the state’s net domestic product through their remittances (Government of Kerala, 2016). With a lauded infection control model in operation, the state was believed to have the potential to facilitate repatriation of its citizens from the Middle East and Europe. Kerala was India’s first state to allow the first two flights of the repatriation mission from the Middle East, which landed on 7 May 2020 (Nidheesh, 2020). Though the state had made extensive preparations, including ultraviolet tunnels and disinfection of passenger luggage to contain potential transmissions, serious concerns remained over the potential threat of community transmission. The state expressed this concern regarding the potential dangers of large-scale repatriation to the central government (Nayak, 2020). However, as a state that gains large economic contributions from migrant labourers, Kerala faced huge pressures to accept its returning citizens. Recent research shows that migrant labourers across the globe suffered terrible uncertainties regarding the health measures available in their place of work (Ullah et al., 2020). Hence, despite concerns over potential dangers, the state accepted the largest number of returnees from abroad (Rai, 2020).
Though screening tests were mandated and quarantine was advised for all, many returnees developed symptoms only at a later stage. This significantly affected local infection control efforts. The initial cases reported after 10 May 2020 were all expatriates, but gradually, the clusters of infected persons expanded to people who came into contact with these expatriates, and, later on, this escalated to community transmission. By 30 June 2020, there were 4,189 recorded cases and 23 deaths (WHO, 2020), but since then, the situation has become much worse.
Still, Kerala’s approach could be considered much more effective than we see in many other Indian states. As reported by the New York Times, the number of positive cases per 100,000 people in Kerala was as low as 297 on 11 September 2020, leaving Kerala in 20th rank in India in the number of cases per million. Despite conducting many more tests per million people than the national average (The Wire, 2020), the relatively low infection numbers in Kerala reflect the effectiveness of the state’s model, even in an escalated situation. If there had not been such large numbers of returning expatriates, the situation would have been much better. This observation, too, confirms that the effectiveness of transmission control in Kerala is fatally interlinked with parallel efforts of infection control in the Middle East and Europe, which were less effective than local processes in Kerala. These connections further point to global impacts on local developments, ruining in this case the earlier achievements of infection control in Kerala, and in the district of Kasaragod. Such precarious linkages not only involve migration but also evidently concern economic factors.
The Choice Between Potential Transmission and Economic Slowdown
Economic slowdown due to the COVID-19 pandemic has become a major concern for nations across the globe. Many of India’s states, including Kerala, rolled out welfare measures for citizens to deal with loss of income and consequent lack of even basic provisions. However, a long-term shutting down of economic activities would not be a feasible option for the Indian state as revenues, including remittances, are rapidly beginning to decrease. The state thus had to gradually open the economy for business. These relaxations in the opening of multiple business outlets like small shops, and relaxation in transport first started happening in May, after the large-scale repatriation had occurred (The New Indian Express, 2020a). The state was quick to realise that the number of cases would rise due to the return of people from outside the state, paired with relaxations given to the business sector (The New Indian Express, 2020b). By the time the state fully grasped that the new surge in cases was mostly due to these relaxations, paired with the influx of expatriates, the transmission rate was already rising; for example, Kasaragod has an emigrant rate of 36 per 100 households (Government of Kerala, 2016), and many local people returned from abroad since 7 May 2020. This would soon become a major cause for rising curves of infections.
Conclusions: What the World Could Learn from Kasaragod and Kerala
The initial successes in flattening the COVID-19 curve and later escalation to community transmission in Kasaragod provide useful insights about pandemic management for other parts of the world (WHO, 2020). Initially, Kerala successfully managed the threat posed by COVID-19 infections, yet only until the large influx of repatriates started. Earlier, as this article has shown, a combination of private–public initiatives allowed effective pairing of limited, but functional medical resources with social elements to contain the threat of infections. The grassroots-level work of ASHA workers, the police force and volunteers played equally important roles and avoided severe strains on local medical facilities. The limitations in the state’s healthcare infrastructure were skilfully overcome by blending the available resources with social capital. This combination of social and medical elements along with the use of social capital and participatory approaches could be a model for other nations, especially in the Global South.
This lauded model, however, relying on earlier disaster management experience, could not cope with the large later influx of repatriating workers, which was caused by a set of different economic and sociopolitical factors. Above all, this highlights the fact that locally focused efforts of initial screening and controlling an escalation of infections can have significant implications on the efforts of other localities, regions and countries as well. However, ultimately, the success of a nation’s efforts to control a pandemic depends partly also on the success, or failure, as the case may be, of infection control elsewhere on the globe, as is clearly shown by the recent experience of Kerala. The global spread of its huge labour workforce meant that success in control of epidemics, at the local level, remains fragile in the long term, unless other parts of the world, connected more than ever, are willing and able to implement similarly effective local control measures. The lesson here, clearly, relates to the need for a better understanding and operation of global burden sharing in exceptional situations, such as health emergencies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.