
Abstract
Focused on colonial South India, this article presents and assesses detailed archival records of public health measures in response to plague outbreaks between 1900 and 1947. Starting in 1897 in the Madras Presidency, the colonial government strictly implemented anti-plague measures and introduced various health schemes and medical policies for plague prevention. However, despite partly vigorous government efforts, plague outbreaks could not be fully controlled. In the twentieth and twenty-first centuries, the plague remains among South Asia’s most feared epidemics, with an outbreak in Surat in 1994 causing major havoc. Neither indigenous knowledge nor Western medical systems provided fully effective remedies regarding causation, cure and prevention of plague epidemics. Since the article gained new relevance in light of current struggles faced by India’s public health system in handling the ongoing COVID-19 pandemic, some lessons from history emerge in the concluding discussion.
Introduction
The research for this article was originally conducted as an archive-based study of how plague epidemics were ravaging colonial South India to examine what measures were undertaken to control these outbreaks. However, this historical work received new relevance in light of the ongoing COVID-19 pandemic and its enormous challenges to India’s public health institutions. For the colonial period, the writings of David Arnold (1987, 1989, 1993) as masterpieces in the history of Indian medicine and public health focus mainly on smallpox as ‘a disease of exceptional significance in nineteenth-century India’ (Arnold, 1989: 45). His article on the Indian plague of 1896–1900 (Arnold, 1987) deals with an early phase of plague epidemics in Bombay, Calcutta and a few other parts of India, and does not even mention South India or the Madras Presidency.
Arnold (1987: 56) examines evidence of the plague in colonial India less as an epidemiological phenomenon and more as a commentary upon the developing relationship between indigenous elites, subaltern classes and the colonial state. During the early phase of this plague epidemic, apart from mounting mortality rates, the diseased body assumes specific medical, administrative and social significance. State efforts were directed towards its apprehension and control of victims’ movements, but this caused contention between indigenous and colonial perceptions, practices and concerns. In the early years of plague outbreaks, colonial hegemony and ambivalent responses, part resistance and part emulation, were prevalent among India’s subaltern classes (Arnold, 1987: 57). Then, as now in the current COVID-19 pandemic, dealing with the casualties and contact with infected bodies raise considerable concerns over pollution and spreading infections, yet some kind of official action that involves the general public becomes inevitable while devising control policies.
Throughout history, South Asia has been no stranger to sometimes massive epidemics (Arnold, 1993). Looking back briefly at earlier history, various epidemics affected the subcontinent from times immemorial, causing millions of deaths. Ancient medical texts on Ayurveda in Sanskrit, like the Charaka Samhita (Wujastyk, 2003) and Sushruta Samhita (Valiathan, 2007), contain references to epidemic diseases and their causation (Khan, 2013: 306; Ramana, 2002: 125). Navanitakam and Astanga Sangraham by Vagbhata also elaborated on medical practices and treatments of various diseases in India (Jaggi, 1981). During medieval times, various court chronicles, travellers’ accounts and biographies described epidemic diseases and their pernicious effects. Enayatullah Khan (2013: 306) refers to a bubonic plague outbreak with heavy tolls among soldiers, witnessed by Ibn Battuta at Bidar, during the time of Muhammad-Bin-Tuglaq (1324–51). Khan (2013: 307) also mentions an outbreak in Gujarat in 1574–75, with a daily average of 100 cart-loads of dead bodies taken out of Ahmadabad alone, to be buried in pits. Tuzuk-i-Jahangiri, an autobiography in Persian of Mughal Emperor Muhammad Jahangir (1569–1627) mentions a disease called ‘plague’ (Jaggi, 1981). He also reported that from 1616 to 1618, a great pestilence spread across the Parganas (sub-districts) of Punjab, Lahore, Sirhind Doab, Delhi, Agra, Ahmadabad, and Kashmir (Khan, 2013: 307). At this early stage, the aetiology of the plague was not fully understood regarding modes of transmission, causes, appropriate measures, confinement of human bodies, physical examination, isolation, hospitalisation and medication, but indigenous medical practitioners, Hindu vaids and Muslim hakims, treated these diseases (Arnold, 1987: 59–60).
Earlier societal and official ways of handling the victims of the disease tended to be brutal, with little concern for what is now called human rights. If one plague-infected person died in a house, all members of the household were isolated and even risked being carried off (Jaggi, 1981). It is known that sixteenth and seventeenth-century India witnessed numerous epidemic diseases, with devastating effects on the countryside. Like many colonial medical experts at the time, William Twining, Assistant Surgeon of the East India Company in Calcutta, argued that the harsh climate affected people’s health, holding environmental factors and lack of sanitation responsible for most tropical diseases (Jaggi, 1981: 1–10). By the nineteenth century, the increasing occurrence of communicable diseases gave much impetus to the ‘sanitary movement’ (Gupta, 2005). The history of the plague in the nineteenth and early twentieth-century India provides valuable insights into a period that witnessed the growth of tropical diseases, affecting millions of people. It was even claimed that no other modern Indian epidemic has caused as much social disorganisation as various forms of the plague (Mushtaq, 2009).
While the word ‘plague’ has medieval connotations in terms of ‘black death’, and one would hesitate to refer to ‘modern’ pandemics in the same terms, both the plague and COVID-19 are highly contagious, spreading rapidly over wide geographical spaces, helped by mass travel already in colonial times. Both infections, in many cases, destroy the victim’s immune system and since such epidemics potentially disrupt and ruin the life of millions of people, with vast local, regional and national economic and social consequences, this becomes a public health problem, requiring rapid action at various levels. This posed obvious challenges for the colonial state in India earlier and constitutes a mammoth task for current public health services. The generally advised preventive measures for both diseases are remarkably similar; too, like hand washing, social distancing or isolation and use of face coverings or masks. Provision of medication and various public health measures evidently involve different levels of public health services, and thus costs. In earlier times, very few infected people seem to have survived the plague and most patients would die on the second day of the attack (Nathan, 1898).
Anti-plague measures implemented by the colonial state pushed for adopting western medicines, including in due course antibiotics, which yielded some good results, as this article details by reference to archival records from South India. In the late nineteenth century, however, financial and political constraints discouraged the colonial state from greater medical intervention, since there was much initial public resistance especially towards vaccination, mainly due to social customs and religious sentiments (Arnold, 1987: 62–8).
After India’s independence in 1947, the government continued strictly implemented anti-plague measures, introducing various health schemes and medical policies for plague prevention. That such latent challenges are by no means extinct was shown when, in late 1994, outbreaks of both bubonic and pneumonic plague occurred in Surat (Madan, 1995). This led around 300,000 migrant workers to flee the city, rapidly spreading the infections over five states. Though the official death toll of less than 100 was minimal, and by late September 1994 the outbreak was under control, such evidence shows that an alert and capable public health system is an absolutely essential component in addressing such epidemics and containing them as efficiently as possible. Whether for colonial administrators and staff earlier, or current governments at various levels, the response to such major epidemics, therefore, cannot be official denial or non-action by public health authorities.
To examine the earlier responses to plague outbreaks in colonial South India, this article makes extensive use of archival records, which document earlier failures as well as achievements over many years in controlling plague outbreaks throughout South India. Such records and the evidence contained in them should not be discarded as irrelevant debris of history. All primary sources referred to in this article are collected from the Andhra Pradesh State Archives and Research Institute (APSARI) in Hyderabad and the Tamil Nadu State Archives (TNSA) in Chennai.
The article harvests archival evidence of the handling of plague epidemics in colonial South India, showing how such earlier challenges were addressed. Then, as now, non-action was not a viable option. After a brief section discussing the dissemination patterns of the plague in India, and especially in the Madras Presidency, the main body of the article examines in several parts the archival evidence of plague-related deaths between 1901 and up to 1951, providing much detail of how various plague epidemics were handled with varying success.
Transmission Patterns of the Plague
The plague was one of India’s most feared epidemics and it is well-documented that the colonial government made specific efforts to contain outbreaks, though it could never completely control it. As a result, India suffered terribly throughout the colonial period (Klein, 1998). The gravity of this disease in earlier times can be gauged from preserved official records. In 1894, more than one lakh people died from the plague and in 1896, the reported death toll in India due to the plague was 1.3 million people (Klein, 1998: 734–46).
There are three types of plague: bubonic, septicemic and pneumonic. The latter form of bacterial infection seems most similar to COVID-19, whose virus attacks the lymph nodes and lung tissue. The main symptoms of the plague are headache, high fever, body pains and intensely hot skin, with patients feeling as if their body is on fire, accompanied by cough with deep and oppressive breathing problems, considerable pains in the chest and joints and about the navel, delirium, great anxiety and thirst. Both pneumonic plague and COVID-19 involve infections that spread invisibly and rapidly via small droplets produced by coughing and sneezing. The pneumonic plague manifests as a severe lung infection, transmitted directly from person to person when the plague bacillus is coughed out of diseased lungs and droplets cause bacterial infection through breathing or oral contact. Since even touching contaminated items of clothing or bedding and infected surfaces pose risks, comprehensive sanitary measures would be required to avoid contamination of entire neighbourhoods.
In India, the more prevalent form of spreading the disease was the bubonic plague, caused by the bacillus Yersinia pestis, initially transmitted by the bite of the rat flea (Klein, 1998: 737). The fleas carried the plague bacilli, transmitted from local black rats as carriers, and ultimately transferred the plague to humans as alternate hosts (Hirst, 1953: 312, 388). The Indian Plague Commission believed that plague was an air-borne contagion transmitted from travellers to other humans. Rat fleas get attached to humans after abandoning rat carcasses for a new live host. A plague epizootic among rats sharply increases the number of flea attacks on people, since rats commonly nest in Indian huts and grain bins. Frequently, initial transmission was thus through contaminated food grains, due to black rats’ activities in grain stores. Since this meant that rodent control became an evident remedy, this would pose challenges in certain parts of India, where some people worship rats. Associated with Lord Ganesha, they would be even fed in temples, such as the Karni Maata temple in Rajasthan, as an internet search instantly brings up. However, the documentary evidence from Madras Presidency certainly confirms evidence of mass killings of rats in efforts to contain the spread of the plague.
According to a monthly health journal written in Telugu in Colonial Andhra, the Arogya Prakasika of 1925 (pp. 15–6), the recommended precautionary measures include not to preserve any foodgrains in the house. The Arogya Prakasika of 1929 (p. 15) advised keeping any remaining food materials near rat holes, and to use rat traps, called bone in Telugu. The presence of rodents was crucial for prolonging plague epidemics, as observed by Arogya Prakasika in 1925. One wonders, however, to what extent such health-related writing, published from Madras by its Chief Editors Dr U. Rama Rao and U. Krishna Rao, would have any local impact among villagers, and to what extent it influenced government policies.
A bubonic plague epidemic broke out in Bombay in 1896, imported through commercial relations by steamships coming from Hong Kong (Kumar, 1998: 195). The same then happened in Calcutta in 1897, spreading to large parts of India within five years. The plague challenged the prosperity of one of British India’s premier ports and administrative centres (Arnold, 1987: 60). The epidemic appeared often among merchants (banias), who were residing on port trust estates on land near the Bombay docks (Jaggi, 1981: 91). The slums of Calcutta and other ports provided ideal conditions for rapid spreading of infections (Kumar, 1998: 195). Klein (1998: 737) has argued that since Bombay as a major port of western India became the hub of a vast integrated logistics network, linking various commercial centres across India, the plague could spread widely. Then as now, migrant labourers carried the epidemic with them as railway passengers, literally from junction to junction, and from town to town within days (Klein, 1998: 737). Plague was also seen as a disease of darkness. Dirt and poor ventilation gave the bacillus its deadly impact (Klein, 1973: 652–7).
By 1899, the plague had appeared in many smaller towns and later extended into the countryside. Between 1896 and 1917, over 5.5 million people, according to a report in the Andhra Patrika of 1918, succumbed to the epidemic. Polu (2012) claims that from 1892 to 1940, over 10 million people succumbed to the plague in India. Klein (1998: 734–44) reported that from 1896 to 1920, the plague mortality was 1.87 million in Bombay Province and 100,000 in the Province of Madras. The Punjab had 2.64 million deaths, the United Provinces 2.35 million, and Bengal another million. Even Western medicine did initially not provide any effective remedies regarding its cure or prevention (Catanach, 1989: 149).
However, a Ukrainian microbiologist, Waldemar Haffkine (1860–930), globally recognised as the pioneer of developing vaccines against cholera and bubonic plague, successfully tried out his inventions in India. The introduction of Haffkine’s anti-plague inoculation in 1897–98 sparked off many rumours concerning its nature, purpose, and effects (Arnold, 1987: 72). Fear about hospitals and the practices of surgery, post-mortems and vaccination gave rise to widespread opposition to public health measures (Arnold, 1987: 75). Compulsory inoculation was advised, however, and doctors and administrators made good efforts to persuade local people to take up immunisation voluntarily (Arnold, 1987: 83). In due course, the colonial state received middle-class support and cooperation, as the higher and middle-class castes gradually overcame their doubts about western medicine and began to show greater acceptance of hospitals and inoculation during the early plague years (Arnold, 1987: 90).
Plague Mortality and Preventive Measures in the Madras Presidency
As noted, trading classes like Baniyas and Marwaris unwittingly contributed to plague transmissions. The Report of the Bombay Plague Committee for 1897–98 commented that Baniyas took the plague to the Deccan, where it became known as the ‘Marwadi Sickness’. They also carried it to parts of Khandesh, where it is called the ‘Baniya Disease’. Hindu traders, mostly from Gujarat, spread the disease to Karachi and Mandvi in Cutch (Arnold, 1993: 210). Various travelling communities and traders brought the plague to Southern India, particularly Madras, which had good commercial contacts with traders and business communities elsewhere and was also a major port city (Arnold, 1993: 210–1). In 1898, Hinganghat, Wardha and Nagpur in the Central Provinces were affected by a plague epidemic, which spread in August 1898 from Hubli and Bangalore to Guntakal junction in the Ananthapuram district of Madras Presidency. From there it moved further into Bellary, Salem and Kurnool districts and led to a plague attack throughout South India by December 1898. In his autobiography, Achanta Lakshmi Pati (1973: 53–4) recalled the history of this plague in Madras Presidency in 1898. He also detailed the implementation of vaccination systems for the prevention of epidemics in many parts of the country.
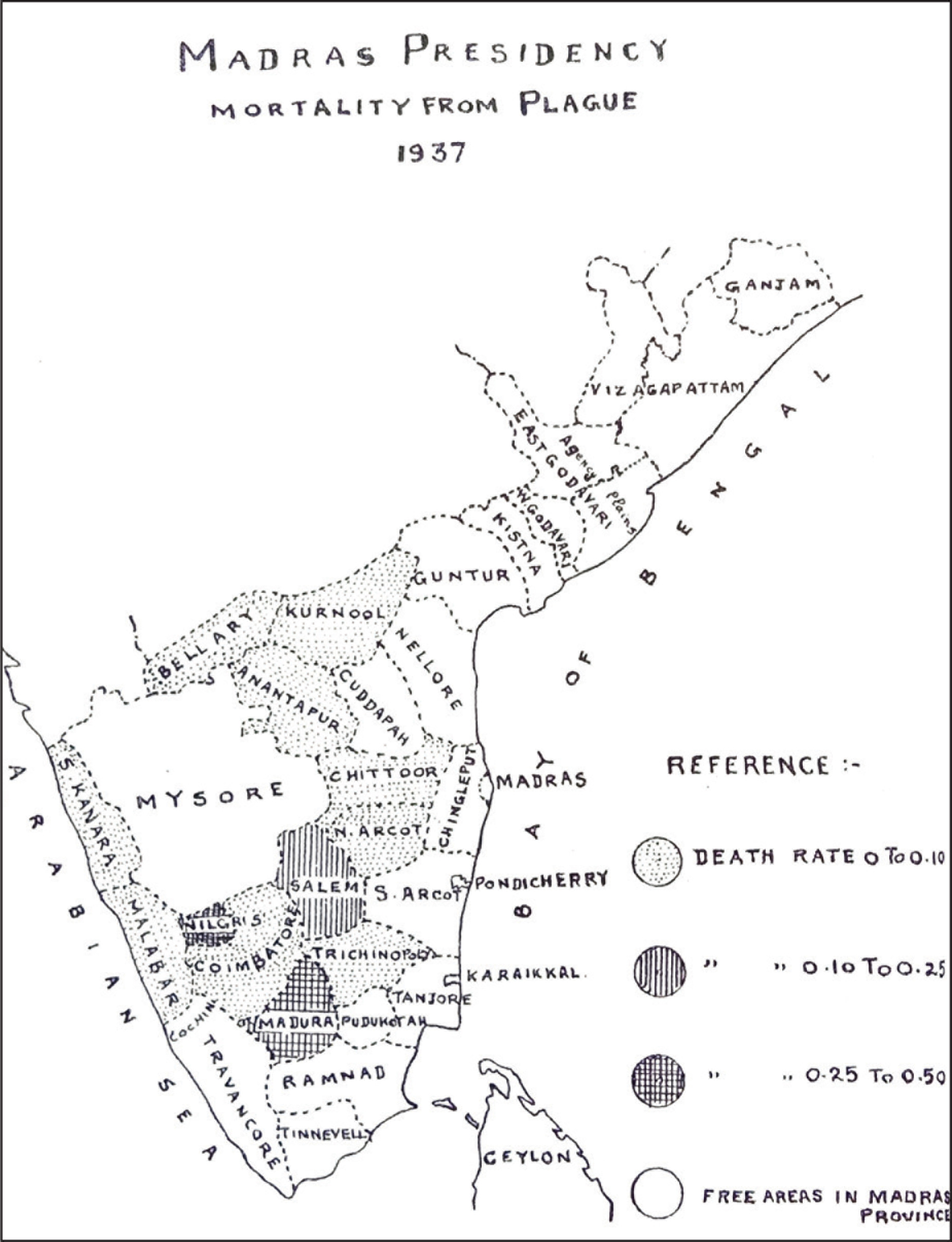
The plague was majorly responsible for the high mortality rate in India, particularly in the Madras Presidency. A map showing the districts of the Madras Presidency is taken from Madras (1939: 99).
Table 1 gives data on the plague mortality from 1900 to 1920 in the Madras Presidency. While these death figures vary, they are shockingly high in some years.
Table 1 shows no particular pattern of plague deaths recorded in the period between 1901–2 and 1920–1. In some years, there was somewhat lower mortality, without explanations. Tracing infected people posed major challenges. Since many victims sought to evade detection and maybe self-isolated or concealed themselves, they escaped the recorded data on mortality, so that the numbers of actual deaths are likely to have been higher than the official figures. The Report on deaths in 1903 discusses the situation in different areas, noting that the infected districts were Ananthapur, Bellary, Coimbatore, Kurnool, the Nilgiris, North Arcot, Salem, South Canara and also the Central districts of the Presidency. The government’s policy to combat the disease varied little from earlier approaches adopted on the plague’s first appearance in the Presidency (Sanitary Commissioner, 1903: 89). In 1904, at the all-India level, registered deaths were 1,143,993. Locally, the death rate was highest in Bellary, compared to the other nine districts affected. Specific problems arose in implementing local plague policies due to conflicts between local judges (munsifs) and sanitation coolies (Sanitary Commissioner, 1904).
Districts of the Madras Presidency
Plague Deaths in Madras Presidency Between 1901 and 1921
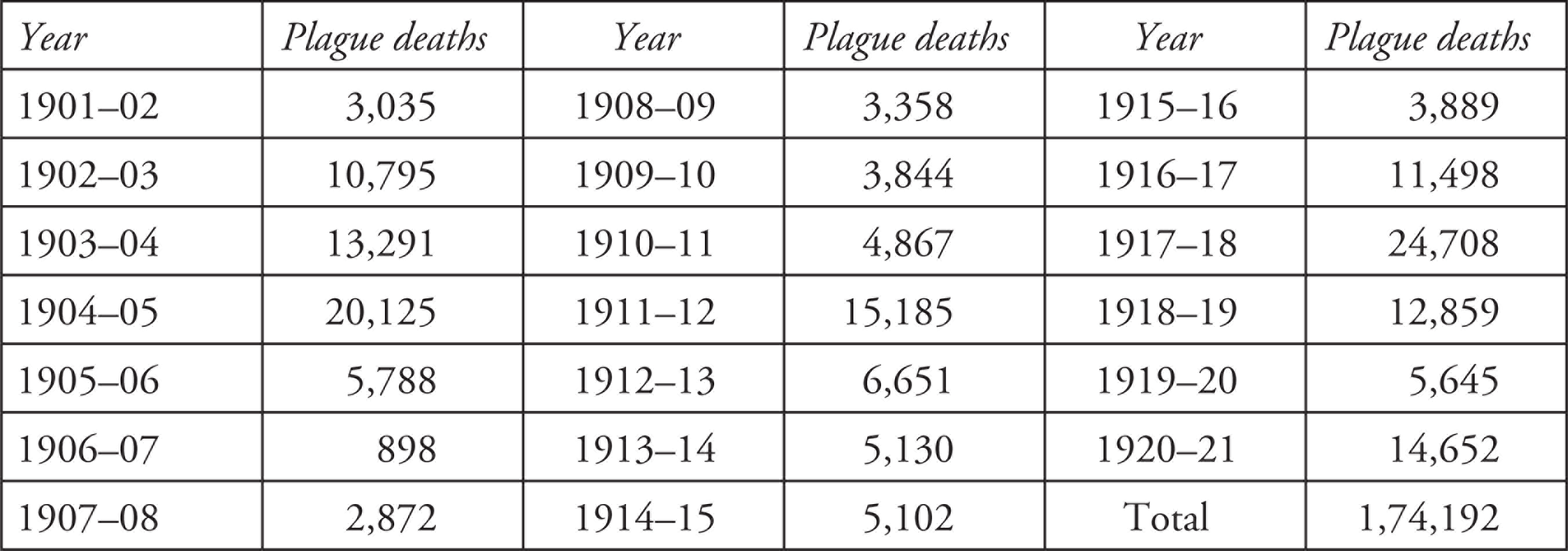
Source: The author (from various Reports on the Administration of Madras Presidency for the Years 1901 to 1921, mainly Report [1911, 1912, 1913, 1920, 1921, 1922]).
The 1898 plague outbreak in Madras Presidency was initially principally confined to districts bordering on Mysore, Hyderabad and the Bombay Presidency. Since the spread of the epidemic was thought to occur mainly through infection from travellers, a system of issuing passports was used to enforce surveillance of contacts. For instance, at the inspection station of Jalarpet, 120 plague-infected people were removed from trains (Sanitary Commissioner, 1901). Since the study of these cases indicated that the infection was brought from territories beyond the control of the Government of Madras, no material change was made in this surveillance policy (Sanitary Commissioner, 1902: 84). Notably, this looks like an early precursor of current containment policies in the COVID-19 pandemic, maybe even involving basic attempts to trace contacts.
By 1905–6, the colonial government incurred increased public expenditure for setting up some laboratories in different parts of the country. A Central Research Institute was created at Kasauli in Himachal Pradesh, though very few factories for producing vaccines and sera were established. There was little progress in research in these facilities (Kumar, 1998: 204), as the scientific community of India looked to the metropolis, where work on tropical diseases had been undertaken. Harrison (1994) has claimed that anti-plague drives facilitated medical research work in India. However, in the Madras Presidency, many government plans for more extensive laboratory networks remained on paper.
Between 1906 and 1910 less deaths were registered, connected to the fact that millions of rats were killed (Harrison, 1994: 157). Travel restrictions in the Presidency, including the necessity of a passport for travelling on certain routes, somewhat reduced transmission rates, according to the Madras Plague Proceedings of 1905 (Sanitary Commissioner, 1905). There was a slight increase in deaths in 1910 due to the decline of vaccinations. Even re-vaccinations failed, partly blamed on the abnormal summer heat, with 84 deaths recorded among persons who had been previously inoculated. Such failures of revaccination affected trust among Indians in the western medical systems (Report, 1911).
The 1911 Census of India blamed overcrowding, bad town planning, poor sanitary arrangements and ill-ventilated houses for the spread of the plague. While in many rural districts of Punjab and the United Provinces, high death rates were reported, in Madras Presidency, with 15,185 deaths in 1911 (Table 1), the disease remained prevalent throughout the year. It affected Bellary, Coimbatore, North Arcot and Salem, as well as municipal towns like Tirupattur, Coimbatore and Bellary (Report, 1912). A critical report of the Madras Drainage Committee (Report, 1913) argued that ineffective and incomplete drainage systems failed to dispose of solid excrement, while waste left for collection in the streets had become ‘poisonous dust’ that would increase plague infections. The functioning of public health officials was, however, often ineffective, as their powers and sanctioned funds were inadequate for improving sanitation in the Province (Report, 1913:15–9). The Second All India Sanitary Conference, held at Madras in 1912, reiterated in its report (Proceedings, 1913) that unhygienic conditions and poisoned foodgrain were mainly responsible for plague epidemics. The Conference repeated calls for improving water supplies and argued that inspection of foodgrain and supply of drugs could help control the plague (Proceedings, 1913: 290–6). Such calls and reality continued to diverge widely.
In 1914 and 1915, plague deaths decreased (Table 1), but mortalities remained high in Bellary and in municipal towns, with Tirupattur suffering the most (Sanitary Commissioner, 1914: 113). In 1917, the highest mortality in the first two decades of the twentieth century was recorded, with 24,708 deaths from 13 districts in the Madras Presidency (Table 1). The casualties were again highest in Bellary, followed by Anantapur, Coimbatore, Salem, and North Arcot. Again, even patients previously inoculated with anti-plague vaccine died from the severity of the epidemic. The impact of the First World War and the failure of western medical systems were seen as possible causes for the highest death tolls in 1917 (Klein, 1973: 642–5). The general health of the Presidency during the year was very unsatisfactory, attributed to two chief causes, the severe economic distress and consequent lowering of people’s resistance to infection and a widespread influenza (Report, 1920: 96–7; Sanitary Commissioner, 1917). During 1916 and 1917, Pandit Gopalacharyulu, an Ayurveda practitioner in the Presidency, started a public awareness campaign on plague, its mode of spreading and methods of protection. His advertisement in the Andhra Patrika of 18 February 1916 assured people not to fear plague since his organisation would provide good Ayurvedic treatment, as he supplied medicine, not only in India, but also in Burma and Ceylon. This was clearly a mixture of public service and business development.
The period from 1917 to 1921 again recorded higher death rates from the plague, except for 1919–20 (Table 1). During this period the conditions were unfavourable to agriculture and food grain prices increased. Food grain shortages necessitated imports from Burma and Bengal, leading to a marked rise of infections from contaminated imported grains (Report, 1921: 11, 92). The colonial government took further preventive measures to contain the plague during these years. The number of rats destroyed added up to 2,623,486 since the beginning of this operation in July 1898. Yet mortality was heaviest in 1921, with 14,652 deaths (Table 1), even though eight districts remained completely immune to the disease (Report, 1922: 92). Many plague victims were identified only near the end of their illness and were almost moribund when hospitalised. During 1921, telegraphic reports of first cases of plague were discontinued under Government Orders (G.O.) by the government (G.O. No. 330, Public Health (P.H.) 1 March 1922), while Ayurvedic doctors like Pandit Gopalacharyulu continued to advertise their services, as in Andhra Patrika of 7 January 1920. Overall, between 1871 and 1921, India experienced what Klein (1973) has described as the ‘woeful crescendo of death’. The death rate of 41.3 per thousand of the population in the 1880s rose to 48.6 per thousand in the decade of 1911–21 (Arnold, 1989: 199–200).
Developments in Plague Mortality from 1922 to 1942
Various later reports of the Director of Public Health in Madras show that while the plague mortality rate declined over time, and only 51 cases of plague were registered in 1945, plague outbreaks continued to cause concern throughout the 1940s. The most striking change in mortality patterns was the increase in cholera deaths and a decrease in plague-related deaths (Arnold, 1989). The statistical data of several reports characterised the period from 1920 to 1947 as ‘unhealthy’. In the 1920s, many people still resisted preventive measures concerning plague, so that Mysore, Bombay, Hyderabad and Bellary districts always faced difficulties in controlling outbreaks (Annual Report, 1924). While the government introduced a policy of destroying imported foodgrains contaminated with plague virus, this control system was not accompanied by paying government compensation to affected traders. Fearing loss of money as well as business, many traders did not cooperate, which then increased the spread of plague because infected foodgrains came into the market (Annual Report, 1924). Table 2 continues a varied picture over the two decades, though compared to Table 1 the casualty figures are generally much lower.
Plague Deaths Between 1922 and 1942
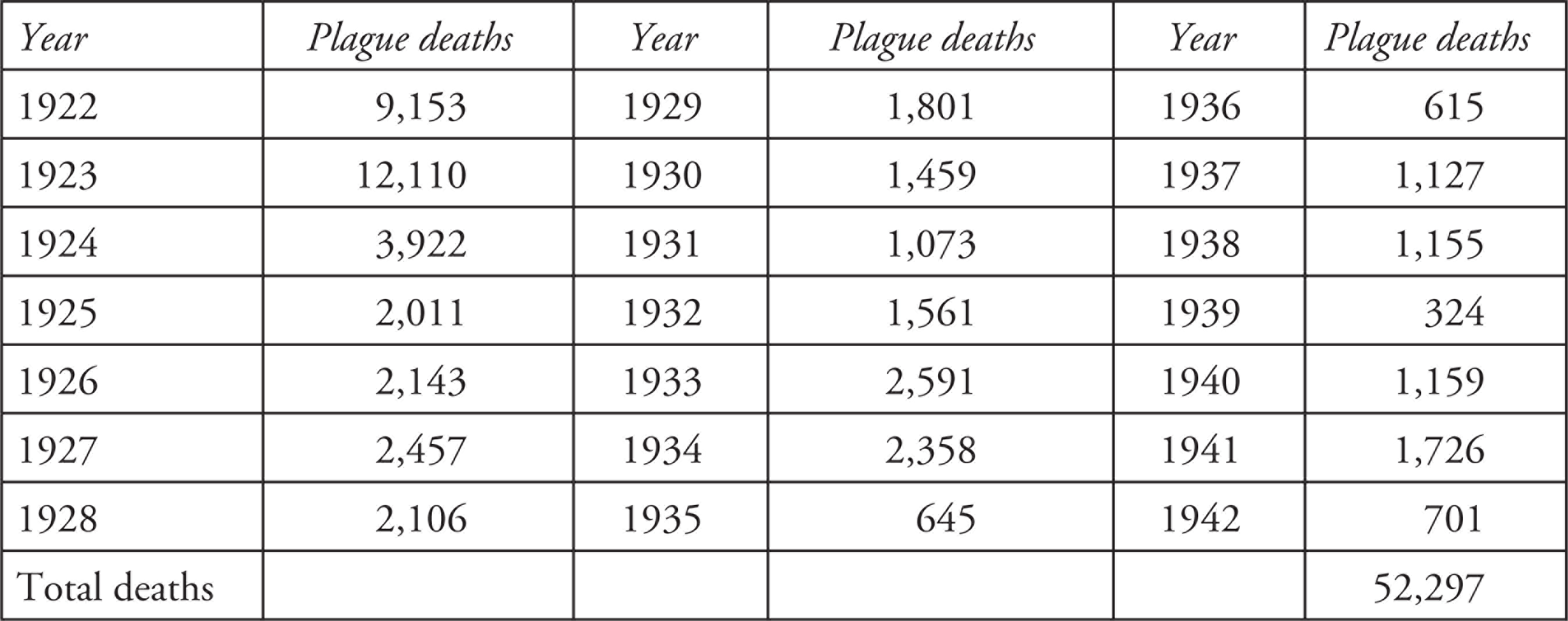
Sources: The author (from Annual Reports of the Director of Public Health and Annual Administrations Reports). For 1922 to 1924, Annual Report (1924: 17) and Annual Report (1925). For 1925–9, Report (1925, 1931) and Annual Report (1931a: 15). For 1930–42, the Annual Reports on the Administration of Madras Presidency for the Years 1930–42 were used (Annual Report, 1931a, 1932, 1936, 1937, 1939, 1942).
Table 2 shows that the total number of plague-related deaths in 1922 and 1923 were still high in the Presidency, but tailed off thereafter. In 1922, Coimbatore district emerged as one of the plague-spots in the Presidency, especially Pollachi, Udampet and Dharapuram taluks, and Pollachi and Dharapuram municipalities. From Dharapuram, the infection spread to Palni taluk in Madura district. In 1923–24, Salem district was considered the most dangerous part of the Presidency, with Salem town itself reporting 680 deaths (Annual Report, 1924: 176–82). Coimbatore and Periyakolam taluks were also seriously affected and the latter was responsible for over half of the total district’s mortality. District Health Officers confirmed that Madura, Sholavandan and Periyakolam were prone to plague outbreaks. Sixteen districts registered plague deaths, but 96 per cent of the total mortality occurred in Madura (4858), Coimbatore (3888), Salem (1818) and Bellary (1090) in 1923. In Ramnad district, plague cases were almost solely confined to the Nadar community of Aruppukottai. Tuticorin was also severely affected, as the infection was brought into the town from Madura.
During the latter half of 1923, the plague spread in a virulent form into Hyderabad. In the Presidency, fifteen rural towns recorded 529 deaths from plague as against 43 towns with 1,220 deaths in 1923. Towns with high death rates were Sholavandan, Kottur, Aruppukottai, and Kumbam. Twenty-two deaths from pneumonic plague occurred in Naduvattam in Ponnani taluk. The Cumbum valley and the Travancore hills are also mentioned as plague hotspots, because of cool and moist conditions, but also due to large grain centres that attracted rats and fleas. Grain trade routes are explicitly identified as disease-spreading centres by the Director of Public Health in Madras in 1923. The salaries of qualified plague inspectors and temporary sanitary inspectors were provided from provincial funds. The Public Health Board recommended that plague supervisors are not necessary. The government accepted this recommendation and directed that, with effect from 1 March 1923, this class of officers should not thereafter be employed, since qualified plague inspectors were appointed, at a monthly pay of ₹60/- (G.O. No. 232, P.H. of 8 February 1923). It is not possible to establish direct links, but plague infections continued in several parts of South India.
The breakdown of 3,922 deaths in 1924 (Table 2), one of the lowest figures on record in the Presidency for some time, shows that 14 districts and 21 municipalities were infected. Coimbatore, Madura and Salem districts were responsible for 83 per cent of all deaths in the Presidency and four municipalities (Periyakolam, Salem, Pollachi and Dharapuram) accounted for 74 per cent of all plague deaths in the entire municipal areas (G.O. No.1951, P.H. 21 September 1925). In Madura district, 20,516 persons were inoculated and a rat killing campaign was carried out in railway stations. Because of local people’s continued resistance to preventive measures and its exposure to infection from three sides, namely Mysore, Bombay and Hyderabad, Bellary district still presented difficult problems regarding plague control. Half-hearted rat trapping was never successful, as rats are cunning animals. It was claimed that much money and energy were wasted because it was erroneously believed that de-ratting can be left to sweepers and coolies. Construction of rat-roofs for all grain go downs in the Presidency’s main grain centres was not adopted due to financial constraints (Annual Report, 1924).
According to the Reports of Health Officers during 1925–29, Mysore state was the focus of infections, with deaths from plague increasing slightly from 2,044 in 1925 to 2,143 in 1926. Over 75 per cent of these deaths were registered in Bellary, Coimbatore and Salem districts. Another epidemic broke out in Ramnad district in late 1925 (Report, 1927: 183). Private practitioners or Sub-Assistant Surgeons were employed as plague Inspectors during such emergencies. Unfortunately, the government passed orders that such private practitioners will be paid only ₹60/- per month, a counter-productive measure causing staff shortages (G.O. No.1492, P.H. 20 July 1925). Instructions aimed at preventing the spread of plague outside the Presidency town of Madras were issued for a further year from 15 July 1925 (G.O. No.1421, P.H. 9 July 1925), but these anti-plague measures were again not carried out vigorously and negligible numbers of rats were destroyed. Rat-proofing of all grain and cotton warehouses was still not undertaken and danger spots of plague were not identified in time (Annual Report, 1925).
During these years, Mahatma Gandhi started the Sarvodaya movement with the aim of protecting village public health (Pati, 1973: 296). In view of the COVID-19 pandemic, an article originally published in Gandhi’s journal Indian Opinion on 16 January 1905 has now been reproduced (Gandhi, 2020). Intriguingly, this shows the Mahatma’s hands-on responses to a plague outbreak in South Africa, where he had become involved with 23 pneumonic plague victims of Indian origin, working in a gold mine outside Johannesburg (Kant & Bhargava, 2019: 28). While 21 of these men and a nurse appointed to care for them died, rigorous hygiene and luck helped Gandhi and his colleagues, including a brave doctor, William Godfrey, to survive. Concerned that the plague might be used to introduce new anti-Indian restrictions, Gandhi was fighting plague and prejudice. His basic advice related to cleanliness, use of disinfecting fluids and avoidance of lavish feasts. Importantly, he urged those who had come in contact with a plague patient not to conceal this, but rather to have their clothes and belongings decontaminated. This incident enhanced Gandhi’s faith in his hygiene strategies and also strengthened his scepticism regarding the efficacy of brandy as a medicine (Kant & Bhargava, 2019: 29).
In 1920s South India, prominent preventive measures including rat destruction, sun-disinfection of grain, use of cyanogas, calcium cyanide used as an effective rodenticide, and the cleaning of houses, drains, grain stores and railway stations were adopted in the Presidency (G.O. No. 1453, P.H. 30 August 1923). Plague regulations for areas beyond the presidency town of Madras were extended from time to time (G.O. No. 2329, P.H. 13 August 1942). The districts of Ganjam, East Godavari, Nellore, Bellary, Madura and Chenglepet had been free from plague due to effective relief measures, as outlined earlier, in the 1920s. But in 1927, they faced fresh infections, with Bellary and Madura recording more than 85 per cent of the total mortality. While six municipal towns recorded 181 deaths, seven rural towns registered 440 deaths in 1927. It was proposed to commence a rat-flea survey of the six or seven main infected places in the Presidency (Report, 1929: 167). Similarly, in 1928, Hindupur which had long been free of plague, suffered new infections, affecting a total of 12 municipalities during the year. In 1929, the epidemic was particularly severe in the districts of Bellary, Salem and Madura, with 160, 574 and 461 deaths respectively, accounting for nearly 92 per cent of the total mortality in the Presidency. Also in 1929, a pneumonic plague epidemic occurred in Lalaikkal, a hamlet of Hoogana Palli in Hosur taluk of Salem district. Within two weeks, 29 deaths occurred among a small population of 150. No other area in the Presidency reported this type of dangerous plague (Annual Report, 1931b: 166).
Standard preventive measures to combat the plague were inoculations and evacuation of infected areas. Sun disinfection of grains was carried out in several districts, 50,768 inoculations were performed, and rat trapping and baiting were an ongoing activity. The Indian Research Fund Association paid for investigations on a plague outbreak in the Cumbum valley in 1932, which caused a large death toll (Annual Report, 1932). That year, a conference involving the Directors of Public Health of Bombay, Mysore, Madras and the Assistant Director of the King Institute at Guindy near Madras, discussed strategies for coordinated efforts to combat the plague (Report, 1934: 157).
During the third quarter of 1932, the disease was conspicuously absent from Northern India, but its incidence rose in Bombay, Mysore, the Central Provinces, Burma and Madras, as reported in Parliament in London (India, 1985 [1932]). Plague epidemics continued to hit Bellary, Madura, Coimbatore and Salem in 1933 and 1934. After encouraging experiments in Cumbum Valley, fumigation by cyanogas was extended to rural Bellary, where death rates had remained particularly high (Report, 1935: 157). During 1934, pneumonic plague re-appeared in North Arcot and Chittor districts (Report, 1936: 170). Meanwhile, experiments were initiated by a certain Dr. Chitre to test immunity to plague in rats from different regions where the disease had occurred in epidemic form. An accurately measured test dose of ‘B-Pestis’ was used for this experiment. A batch of rats from Madras, highly susceptible to plague, was contrasted with a batch of rats resistant to plague from Bombay. This investigation showed that the percentage of deaths from plague in the inoculated rats displayed a general correspondence to the aggregate incidence of plague in the area from which the rats were obtained (Annual Report, 1936: 197).
In 1934, at all-India level reported plague cases rose to 103,271, the mortality rate increased in Hyderabad state, the United Provinces, Punjab and the Bombay Presidencies (India, 1985 [1935]). However, the entire Madras Presidency recorded only 645 plague deaths in 1935 (Table 2), the lowest figure since the plague’s advent in the Presidency 38 years earlier (Madras, 1938: 173–4). The disease was mostly confined to localities bordering the Mysore plateau and the Cumbum Valley. The significant decrease in mortality was clearly related to strict government methods of evacuation, inoculation, isolation, disinfection and rat destruction. A total of 84,243 anti-plague inoculations were performed and extensive cyanogas fumigation of rat burrows was carried out, with great success. Local bodies encouraged fumigation measures and sanctioned half the costs. As a result, 219,315 rat burrows and 6,374 cracks in mud walls in 31,927 houses in 27 localities were fumigated. 8,358 rats, 10,474 house mice and a fair number of other rodents, 17 snakes and 11 bats were caught during the cyanide fumigation (Annual Report, 1937: 16–7). Plague research was conducted at different places, but lack of consistency in government policy led to a revival of the epidemic in several areas of the Presidency. The 1,127 deaths in 1937 (Table 2) were spread over seven districts and eight municipalities. Madras, Salem and the Nilgiris accounted for 84 per cent of the total plague mortality. The Nilgiris, which had remained plague-free for 15 years, got re-infected in 1937 (Madras, 1939: 97–8).
The government scheme of originally experimental cyanogas fumigation was now extended to all plague-affected areas, with very satisfactory outcomes. A new scheme was sanctioned for a temporary hospital in the Cumbum Valley, experimenting with an anti-plague serum developed at the Haffkine Institute in Bombay (G.O. No. 2916 P.H, 16 August 1939). This yielded such good results that only one death was registered in Bellary district, synchronised with decreasing rat populations in five villages due to fumigation. Significantly, in areas where fumigation was not used, plague mortality continued. Worst affected was Hosur taluk in Salem, from where the infection spread to Krishnagiri and Dharmapuri taluks and the Cumbum Valley, with 35 villages reporting infections (Annual Report, 1939).
After the Government of Madras formally took up the ‘Fumigated with Cyanogas Scheme’ (Madras, 1941: 79–80), more villages were fumigated. Special attention was now paid to the bionomics of fleas and destruction of rats and fleas in thatched roofs. A further government scheme was sanctioned for treating plague victims in local hospitals. As a result, in 1939, the lowest ever mortality from plague since 1898 was recorded, with only 324 deaths (Table 2). A total of 277,921 inoculations were administered and further plague research was conducted at Cumbum Valley with grants from the Madura District Board, the Indian Research Fund Association and the Travancore government. Picketing stations were opened where plague-infected commodities and personal effects of passengers were now fumigated with cyanogas (Annual Report, 1942: 21–2). The government sanctioned ₹45,900/- for cyanogas fumigation in the infected areas (G.O. No. 1308, P.H. 27 March 1941), quite a large sum at that time.
Developments Between 1943 and 1951
Table 3 shows that plague mortality in the Madras Presidency continued to be fairly high until 1947, mainly due to socio-economic conditions of austerity during the Second World War. From 1940 to 1947 there was a revival of significant plague infections in various taluks. The eastern parts of Bellary district, which had been plague-free for about 23 years, suffered re-infection, causing about 70 per cent of the Presidency’s total mortality in 1941 (Table 2) and many more deaths in the following years.
Plague Deaths 1943–51

Source: The author (from Report [1955] for the 1943 data and Madras [1942, 1943 and 1946] for all other data).
During this most difficult period, which also saw the subcontinent’s Partition of 1947, there was a widespread lack of reliable water supply, protective vaccinations and environmental hygiene in the whole subcontinent. Plague mortality declined gradually, mainly due to intensive cyanogas fumigation of huts, houses, godowns and other commodities in numerous infected areas, and there were no new cases after such fumigations (Annual Report, 1946: 7–9), which again killed large numbers of rodents and some other animals. 300,000 plague inoculations were administered in Madras Presidency during this time and the government now ordered that all local boards and municipalities should insist on constructing rat-proof godowns as a condition precedent to granting licences for traders (Madras, 1946: 121–2). Observation stations were opened at the outskirts of infected localities, where all articles likely to harbour rats or rat-fleas were fumigated before they were allowed to be transported anywhere. Such surveillance certainly reduced plague outbreaks in the Presidency.
Overall thus, in colonial South India, starting in 1897 in Madras Presidency, albeit with many delays and tribulations, the government strictly implemented anti-plague measures and introduced various health schemes and control policies. In due course, major measures became the inspection of ships and trains as well as intending and actual passengers, subjecting suspected plague victims to detention and segregation. Plague regulations under the Epidemic Diseases Act of 1897 were strengthened by appointing plague inspectors, as well as daily and monthly plague reports sent by Collectors to the Director of Public Health. Control measures focused on removal of infected items, rat destruction especially at infected railway stations, and the systematic clearing of garbage to improve general cleanliness of dwellings and their surroundings. The establishment of separate plague hospitals, connected to the development of plague vaccines, mass inoculations, segregation of plague patients and evacuation procedures were important steps. Sun disinfection of contaminated food grains and clothing, frequent checking of grains and especially cyanogas fumigation became standard control measures. Permanent preventive measures by the colonial government also included control over the location of trades and industries which attract rats, construction of rat-proof and rat-free granaries (G.O. No. 1146, P.H., 10 July 1926: 2–21). Effective propaganda methods such as lectures, lantern slides, cinema shows, health-related songs, dramas and skits gave good results (G.O. No. 1130, 19 March 1939: 27–31). Consequently, the plague had almost disappeared in the whole of Madras state by 1953, with only nine attacks and six deaths from plague in that year, as against 23 attacks and 12 deaths recorded in 1952 (Madras, 1954).
India’s government later also introduced Dichlorodiphenyltrichloroethane (DDT) treatment, which replaced cyanogas, with good results. Recognising the public health needs, despite awareness that such treatment has poisonous side-effects, more efficient control policies were developed, and sufficient health staff was appointed (Madras, 1954: 43). Prophylactic treatment of endemic areas with DDT, which also worked well in malaria control, was adopted and the Epidemic Diseases Act of 1897, which continued to give officials special powers to enforce containment, was strictly implemented. It is gratifying to read the records of excellent progress achieved in plague control by the early 1950s (Report, 1955: 16–9).
Concluding Discussion
This article was originally conceived as an archive-based historical research to contribute to ongoing academic discourses about the tensions caused in local colonial scenarios of South India between modern western medical interventions and the resistance of colonial subjects to such interventions and control measures. Meanwhile, though, the almost unspeakable realisation that the ongoing COVID-19 pandemic looks rather like a new form of plague hit home, and has affected this concluding discussion.
Among several terrible epidemics that ravaged colonial Indian society in the first half of the twentieth century, the spread of various forms of the plague, also in South India, was promoted by certain social and environmental problems. Early reports from Madras Presidency about how the colonial state handled plague outbreaks, found in immensely rich regional archives, provide important illustrations of the vacillations and policy failures involved in control policies, before more effective processes and remedies were developed and applied. In due course, the colonial government made some pioneering efforts to introduce various health and medical policies, which yielded good results with lasting long-term effects, felt especially after the independence of India. The initially unfocused phase of anti-plague measures soon gave way to the colonial state’s push for adopting western medicines in efforts to reduce infections and mortality figures. The greater spread of hospitals and inoculation programmes, despite much initial resistance and distrust, later somewhat mitigated the ongoing local problems. Regarding plague prevention, western medicine gradually almost succeeded in elimination of the plague.
This article has clearly shown that when faced with dangerous epidemics like the plague, or indeed now COVID-19, denial or downplaying the risks posed by an aggressive epidemic cannot be a viable strategy either at the private or the public level. The detailed archival evidence of local struggles in colonial South India between about 1900 and 1947 to contain plague epidemics and outbreaks has documented the inescapable demands for a synergy of private responsible action, together with considerable, increasingly focused engagement by the public health sector, however rudimentary this may have been in colonial India. Given the known root causes of plague epidemics, measures had to include the mass killing of rats and other rodents to eliminate the sources of infections, including rat fleas. In late nineteenth century South India, however, not everyone pulled together to act, as it would now be called, in the wider public interest when it came to controlling plague outbreaks. The narrow interest of some entrepreneurs who continued to sell contaminated food grains was one stumbling block. The initial fears and distrust of uneducated local people about inoculation and especially segregation, caste barriers and the grave nature of plague itself, all helped the spread of sporadic plague epidemics and their periodic re-appearance over several decades.
In earlier times, despite partly vigorous government measures, plague outbreaks could not be fully controlled, however. More recently, too, outbreaks have flared up from time to time, as seen in 1994 in Surat (Madan, 1995). Outbreaks of dengue fever and chikungunya, which are not covered here, but should at least be mentioned, refer to different manifestations of highly dangerous and contagious diseases with similar symptoms as the plague. Presently, faced with the COVID-19 pandemic in India, common people, health authorities at various levels and the central state, now the largest democracy in the world, are again seen struggling to contain the disastrous spreading of a new type of infection that causes many deaths and has already brought massive social and economic turmoil.
The earlier experiences of handling such challenges, managed in pre-democratic times by a foreign colonial power, indicate that then, as now, some firm, focused action is absolutely essential, otherwise such dangerous epidemics will completely escalate out of control. Outbreaks of the plague may have been confined only to certain areas, yet often spread easily in the past. As this article has shown, after some initial complications, an increasingly firm grip over the plague was achieved. Currently, India does not have decades to work out how to handle the imminent challenges of COVID-19. As new research demonstrates (Kummitha, 2020), various methods of interventions into people’s freedom of movement are inevitable to contain the spread of such a pandemic. But control methods based on isolation are clearly insufficient by themselves, more so in crowded twenty-first century South Asia. The worrying similarities between plague outbreaks in colonial South India and the current pandemic suggest that to avoid further huge casualties, re-infections and further waves of the COVID-19 pandemic, everyone has to act responsibly, a tough private as well as public challenge, focused on local needs and measures. While it seems unwise to wait for, or rely on, state-driven control policies, a new sense of civic responsibility may become a new component of post-pandemic life, again not unfamiliar in light of what the people of the Madras Presidency—and their rulers at that time—began to learn in the early decades of the twentieth century.
Today, pandemics are not a brilliant chance to polish the profile of leader figures, rather they require hard work, in locally focused action, very much in the way the archival resources of early twentieth century Madras Presidency, as shown here, have documented. There needs to be responsible leadership at the centre, endorsing firm controls, where necessary. But at the crucial local and individual levels, which will of necessity be less well documented, if at all recorded for posterity, apart from good luck, finding an appropriate balance between alert monitoring, watchfulness and engaged commitment to prevent the spreading of pandemics, as Gandhi’s example shows, could make and mark the difference between becoming part of mortality statistics and survival.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.