
Abstract
We investigated how Australians and Hong Kong Chinese respondents describe individuals with lung cancer, examining the impact of culture and language on public discourse and stigma expression. A total of 303 participants (NAus = 176; NHK = 127) were recruited from a commercial panel provider to complete an online survey. Participants were presented with a vignette describing a hypothetical lung cancer patient and asked to provide their impressions through open-ended written responses. Content coding revealed seven main themes: Warmth, Competence, Morality, Bad luck, Poor health behaviors, Ordinary, and No judgments, with both similarities and differences in participants’ written expressions across cultures. The language Hong Kongers used to respond influenced response patterns, with English responses resembling Western norms of Australians. These findings demonstrate how both culture and the language a person uses influence how people express stigma. By understanding these cultural nuances public health strategies can better support people from diverse backgrounds.
Keywords
Lung cancer is the second most prevalent malignancy worldwide, with the highest mortality rates reported as of 2020 (World Health Organisation, 2022). Despite its prevalence and high mortality, lung cancer research remains substantially underfunded relative to other cancers (Kamath et al., 2019). Previous research conducted with Western populations suggests that lung cancer is more stigmatized than other types of cancer, mainly due to its perceived behavioral cause and primary risk factor—smoking (Else-Quest et al., 2009; Godward et al., 2022; Lebel et al., 2013; Marlow et al., 2015). Many studies on lung cancer stigma focus on individuals with the health condition, particularly internalized stigma (Hamann et al., 2014; Weiss et al., 2017). Extensive research has also examined enacted stigma, looking at how the general public expresses views toward individuals with lung cancer, and how such stigma can impact society by shaping societal attitudes, influencing public health campaigns, funding priorities, and other policy decisions (Hamann et al., 2018; Rigney et al., 2021). However, there has been limited exploration of this form of stigma in East Asian contexts. The studies that do consider the role of culture in lung cancer stigma suggest cultural variations that may be associated with people's beliefs, societal norms, and linguistic backgrounds, indicating that the formation of stigma is socioculturally specific (Liu et al., 2016, 2020, 2023; Scott et al., 2014). Given that language is a recognized channel for the transmission of stigma (Link & Phelan, 2001, 2006), we argue that examining how people talk about individuals with lung cancer in their respective languages is valuable. The use of language not only reflects but also shapes social attitudes and perceptions, helping researchers to better understand the nature of lung cancer stigma. Accordingly, we aimed to explore cultural and language differences in how lay people from the West (Australia) and the East (Hong Kong Special Administrative Region of China) perceive and communicate about individuals with lung cancer to uncover underlying stigmatizing attitudes and provide insights into how lung cancer stigma is perpetuated.
The public discourse surrounding lung cancer in Australia, as in many other Western countries, has been significantly influenced by decades of successful tobacco control campaigns and messaging. However, cultural norms around smoking and lung cancer stigma can vary widely across regions. While Australia has experienced a strong shift in social norms due to tobacco control efforts, this may not be the case in certain Western nations, where different historical, social, and political contexts may influence public perceptions of smoking and lung cancer. Through the denormalization of smoking, these campaigns in Australia reinforce the perception that lung cancer is essentially a self-inflicted disease, with smoking being a leading risk factor (Chapple et al., 2004; Evans-Polce et al., 2015). This can be explained by attribution theory (Heider, 1958). As Weiss et al. (2014) pointed out, individuals with lung cancer are often presumed to be partially responsible for their condition since it is seen as preventable. For instance, illnesses with biological causes, such as blindness and heart disease, are less likely to be stigmatized than those with behavioral causes, such as acquired immunodeficiency syndrome (AIDS) and obesity (Weiner et al., 1988). Furthermore, the legal availability of tobacco has shifted smoking from a legal concern to a moral one, emphasizing one's responsibility and self-efficacy in avoiding the behavior (Thompson et al., 2009). As a result, smoking is perceived not only as a poor health behavior stemming from personal choice but also as an indicator of one's social competence and morality (Occhipinti et al., 2018). While public health initiatives have been effective in reducing smoking prevalence, they have also contributed to stigma, by diminishing empathy for both smokers and lung cancer patients, regardless of their smoking status (Rankin et al., 2020).
Research on Chinese populations in the Chinese language, however, suggests that how people perceive and talk about lung cancer may depend on their cultural and language context (Liu et al., 2016, 2020, 2023). Given that smoking is socially acceptable in China, with cigarettes being exchanged as social currency through cigarette sharing and gifting (Wu et al., 2022), it has been suggested that the stigma associated with lung cancer may not necessarily be linked to smoking or anti-tobacco campaigns in China. Liu et al. (2020) found that the smoking status of Chinese lung cancer patients did not influence the stigma they experienced, and a qualitative study by Liu et al. (2023) found some Chinese lung cancer patients even disputed the link between smoking and their condition (e.g., “Is it because of smoking? My colleagues are also smokers, but they don’t [have] it”; p. 593), attributing their diagnosis to other factors, such as air pollution and bad luck. These findings align with previous research by Occhipinti et al. (2018), suggesting a cognitive dissonance perspective, where lung cancer patients may seek to weaken the perceived causal connection between smoking and their condition when faced with stigma.
Indeed, other factors beyond smoking have been identified as contributing to the stigma surrounding lung cancer in Eastern cultural contexts. Liu et al. (2016) noted a prevalent misconception among Chinese populations that lung cancer is “contagious” and “dirty.” This misconception is fueled by the common symptoms of lung cancer, namely cough and expectoration, which are often associated with infection and result in stigma (Liu et al., 2016). Moreover, Liu et al. (2020) also identified a high level of perceived blame and personal responsibility towards lung cancer patients in China. This perception arises because cancer is often seen as divine punishment for the misdeeds of patients in Chinese cultural contexts (Lee et al., 2013; Leung & Chan, 2015). This cultural belief contributes to a stigma similar to that surrounding mental illnesses, where life-threatening diseases are often linked to moral failings or personal wrongdoings (Bedi & Devins, 2016; Yang et al., 2007). Stigmatizing language, such as “karma” or “acts of fate” (mìng), which are perceived as impossible to alter, are commonly used to explain cancer in these contexts, leading to the “loss of face” (diūliăn) for patients and further exacerbating stigma (Goss et al., 2014; Liu et al., 2020). Thus, individuals without the health condition often attribute more blame and judgment to lung cancer patients whom they deemed as “deserving of their condition.” Overall, research to date suggests cultural variations in public perceptions and discourse on lung cancer across diverse contexts, particularly contrasting Chinese perspectives with Western views.
The Present Study
However, to date, there is limited research on lung cancer stigma in Asian cultures, and no direct comparisons between Eastern and Western cultures. Our study examined two regions: one representing the standard Western context from which much of the evidence on lung cancer stigma originates (Australia), and another reflecting a setting closer to East Asian cultural norms [Hong Kong Special Administrative Region of China (SAR)]. We sought to explore the cultural and linguistic nuances influencing the expression of lung cancer stigma between Australians and Hong Kongers. Understanding how stigma is communicated and perpetuated in different contexts is important, as it may impact health-related communication and potentially hinder support for patients in the forms of volunteerism, advocacy, and research funding (Weiss et al., 2014).
Both Australia and Hong Kong SAR have a remarkably low smoking prevalence of 10.1% and 9.5%, respectively (Australian Bureau of Statistics, 2022; Census and Statistics Department Hong Kong SAR, 2022). Tobacco smoking was introduced to Australia in the 1700s, with active promotion and advertising (Greenhalgh, 2019). However, restrictions began in the 1970s, following the U.S. Surgeon General's 1964 findings linking smoking to lung cancer (Vachani et al., 2017). Since then, public health efforts—such as tobacco taxes, smoking bans, and anti-smoking campaigns—have significantly shifted social norms, leading to smoking being increasingly viewed negatively in Australia, along with a marked decline in smoking prevalence (Riley et al., 2017). Similarly, Hong Kong SAR has maintained its low smoking rate over the years with a long history of anti-smoking initiatives, possibly influenced by its past as a British colony. These factors contribute to the strong social norms against smoking in Hong Kong SAR compared to mainland China. Therefore, by comparing lung cancer stigma between Australia and Hong Kong SAR, we can effectively control for smoking prevalence, and render more salient the cultural factors that may promote stigma.
Furthermore, the unique “trilingual and biliterate” language policy of Hong Kong SAR fosters the use of three languages: Cantonese (a dialect of Chinese), English, and Putonghua (Standard Chinese) in the territory (Wang, 2019), with Cantonese being the primary language for daily communication and English prevalent in formal contexts, such as government, legal, professional, educational, and business sectors (Bolton et al., 2020; Evans, 2011). Hence, we expected responses from Hong Kongers to be in either Cantonese or English. We argue that studying both the intercultural differences (Australia vs. Hong Kong SAR) and the intracultural variations within Hong Kong SAR, based on language choice (Cantonese vs. English), can provide a nuanced view of the impact of culture and language on health communication. This may help shed light on whether the differences are primarily cultural, linguistic, or a combination of both, contributing to a more comprehensive understanding of how these factors interact to shape people's perceptions and expressions about lung cancer.
In this study, we explored lung cancer stigma across cultures and languages by analyzing description of individuals with lung cancer through the lens of attribution theory, person perception theory, and the stereotype content model (SCM; Fiske et al., 2002), which is known for its generalisability and robustness (Grigoryev et al., 2019; Guan et al., 2010; Martinez et al., 2016; Yang et al., 2020). Person perception theory explores how people use mental processes to form impressions of others, while attribution theory, as part of person perception theory, examines how people interpret information about others and make causal inferences (Heider, 1958). For example, individuals with lung cancer may be perceived as irresponsible if their condition is attributed to controllable factors, such as unhealthy behaviors. The SCM, originally developed to explain intergroup perceptions, posits that people evaluate others based on two fundamental dimensions: warmth (one's perceived intentions) and competence (one's ability to act on intentions). Subsequently, the model also integrated a third dimension, morality, following the proposal for a three-dimensional framework (Leach et al., 2007). These dimensions place individuals or groups within a stereotype content space, which subsequently influences the emotions and motivations directed toward them (Thornton & Mitchell, 2018). Collectively, these theories provide a framework for understanding lung cancer stigma in the context of this study. Person perception theory emphasizes the formation of initial impressions, attribution theory addresses how people assign blame based on perceived controllability, and the SCM reveals how perceptions of warmth, competence, and morality shape the sentiments directed toward individuals with lung cancer.
Aim and Research Questions
We aimed to examine how Australians and Hong Kongers express lung cancer stigma through their written expressions of individuals with lung cancer, by addressing the following research questions:
How do Australians and Hong Kongers differ in their written expressions about individuals with lung cancer? How does language choice affect the written expressions of Hong Kongers about individuals with lung cancer?
Methods
Design
Data used were drawn from a larger cross-sectional project about stigmatization of different cancers. Ethics approval was granted by the Human Research Ethics Committee of the authors’ institutions. We adopted a qualitative approach to delve deeper into cultural and linguistic nuances, recognizing that qualitative data offer a more detailed understanding of how culture and language choice may shape people's ways of communicating about those with lung cancer and why their health-related narratives may vary. Since stigma is a complex social phenomenon, qualitative research is imperative to gain an in-depth, nuanced, and holistic understanding of participants’ responses (Stutterheim & Ratcliffe, 2021).
Participants
Data collection for the parent study occurred between October 2020 and July 2021. Participants were recruited from a commercial panel provider, with the requirement that they were (1) Australians or Hong Kongers, and (2) aged 18 years or older. Since this study focused on a cultural and linguistic comparison between Australians and Hong Kong Chinese, participants were excluded if they identified as Asian ethnicity in Australia or did not identify as Asian ethnicity in Hong Kong SAR. Our study focused on analyzing the open-ended responses from the larger survey study. Of the 924 recorded responses, 604 were related to melanoma or colorectal cancer and 17 were invalid responses. The final sample comprised 176 participants aged 19–86, Mage = 48.64 (SDage = 18.66) in the Australian group and 127 participants aged 21–68, Mage = 41.55 (SDage = 11.62) in the Hong Kongers group. See Table 1 for a summary of demographic information for participants.
Demographic Information of Participants (N = 303).
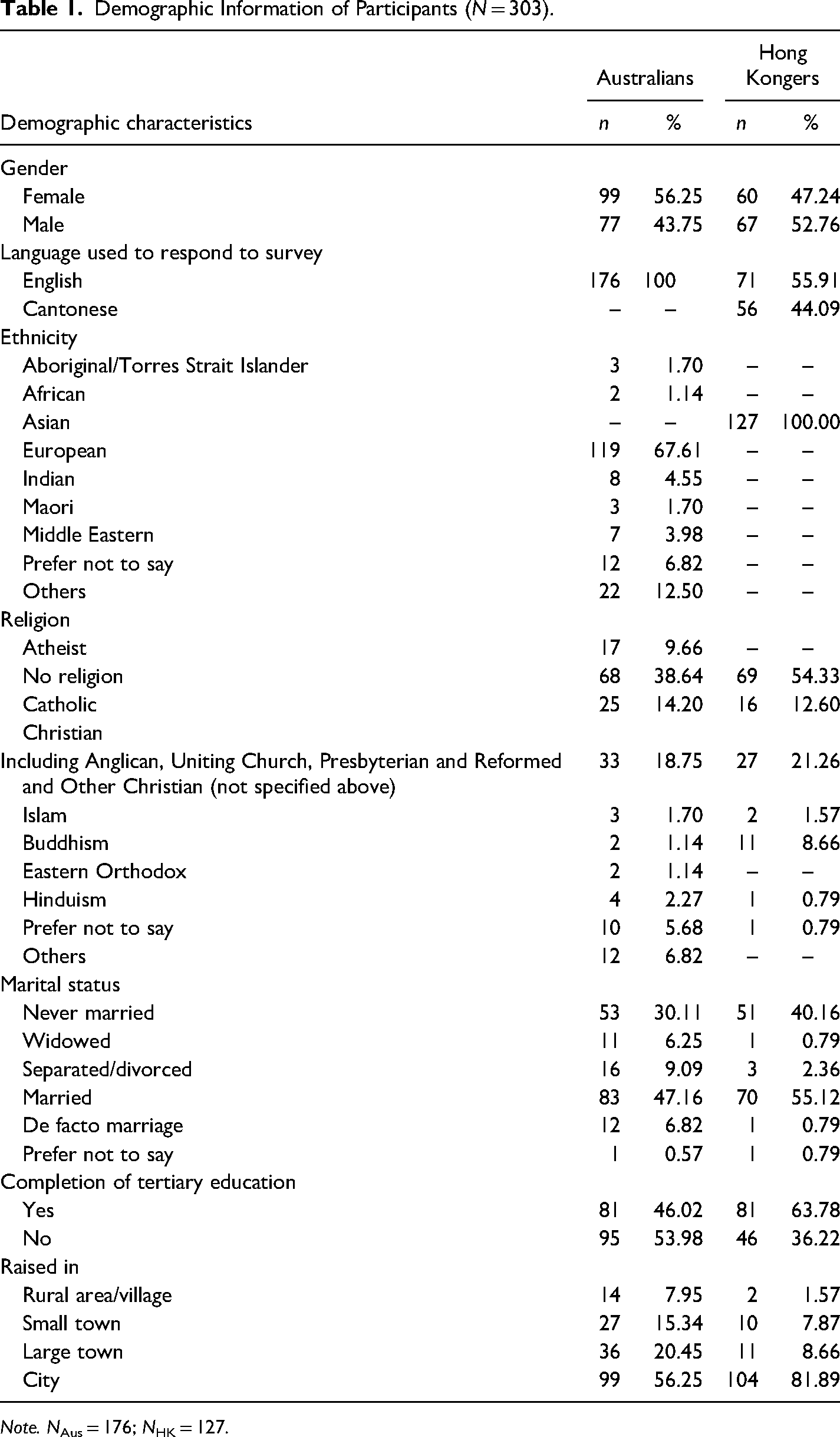
Note. NAus = 176; NHK = 127.
Procedure
After reviewing the participant information and consent form, participants were asked to complete an anonymous online survey hosted on LimeSurvey and were informed that completion of the questionnaire implied consent. First, participants were presented with a vignette describing a neutral hypothetical character named Sam (randomly assigned as either male or female), who displayed symptoms of lung cancer and had received a diagnosis (see supplementary material). The vignette was developed based on prior research on lung cancer stigma and was peer-checked by medical professionals to establish both content and expert validity (Occhipinti, 2022). In the parent study, participants were required to rate a range of structured measures about the attributes of Sam on a scale of 1 (not at all) to 7 (very much) prior to providing their open-ended responses (i.e., “Imagine Sam, the person you have just read about. Rate how likely you think that a person like him would be to possess each of the following attributes.”). Notably, these quantitative measurements may have primed subsequent open-ended responses. Finally, to elicit the culturally and linguistically shared expressions underlying lung cancer stigma, participants were asked to describe their impressions of Sam with an open-ended textual question (i.e., “For this question, we are interested in your open impressions. Based on the brief description of Sam provided, how do you imagine him as a person?”). The survey was translated and back-translated into Cantonese by two native speakers, allowing participants from Hong Kong SAR to respond in Cantonese or English. Participation was voluntary, and participants were free to withdraw at any time. Participants were offered a chance to win one of five $50 gift vouchers as an incentive.
Data Analysis
All responses written in Cantonese were translated by the first author, who is proficient in Cantonese. During the translation process, it was observed that participants from Hong Kong SAR tended to provide shorter or no comments when responding in English, whereas, in Cantonese, they often shared more detailed expressions of Sam. Data were analyzed in Google Sheets, using directed content analysis following Krippendorff's (2013) guidelines. First, the first author read through participants’ responses multiple times for familiarization, and identified all instances where participants described an impression they formed about Sam. Next, a coding scheme was developed, both inductively and deductively and informed by attribution theory, person perception theory and the SCM dimensions of warmth, competence, and morality (Fiske et al., 2002; Leach et al., 2007). The inductive coding enabled the identification of both additional themes not included in SCM, as well as a more detailed set of subthemes under the SCM dimensions. Some themes were valenced as positive, negative, or neutral (if applicable). Subsequently, each of the responses pertaining to participants’ expressions of Sam was content-coded. Since some participants provided extended descriptions of Sam, their responses were coded with multiple themes accordingly.
The first author continually refined the themes and subthemes as the analysis progressed, under the supervision of the second and third author. To maintain internal consistency, a second coder independently coded 20% of the data using the coding scheme, and any discrepancies were rectified through consensus discussion involving both coders. As a result, an inter-rater reliability of 0.94 was achieved using Cohen's kappa. The final themes and subthemes had consensus from all authors. Table 2 provides a description of the themes and subthemes. The presence and absence of each subtheme for every participant were then entered into IBM SPSS Statistics (version 27), and frequencies were calculated. Chi-square analyses were performed to test for significant differences in the frequencies of each subtheme across both settings. In cases where 20% of the expected counts were less than five, Fisher's exact tests were conducted instead. Lastly, the frequencies of each subtheme were calculated separately for participants from Hong Kong SAR who responded in English and Cantonese.
Coding Scheme for Participants’ Descriptions of Sam.
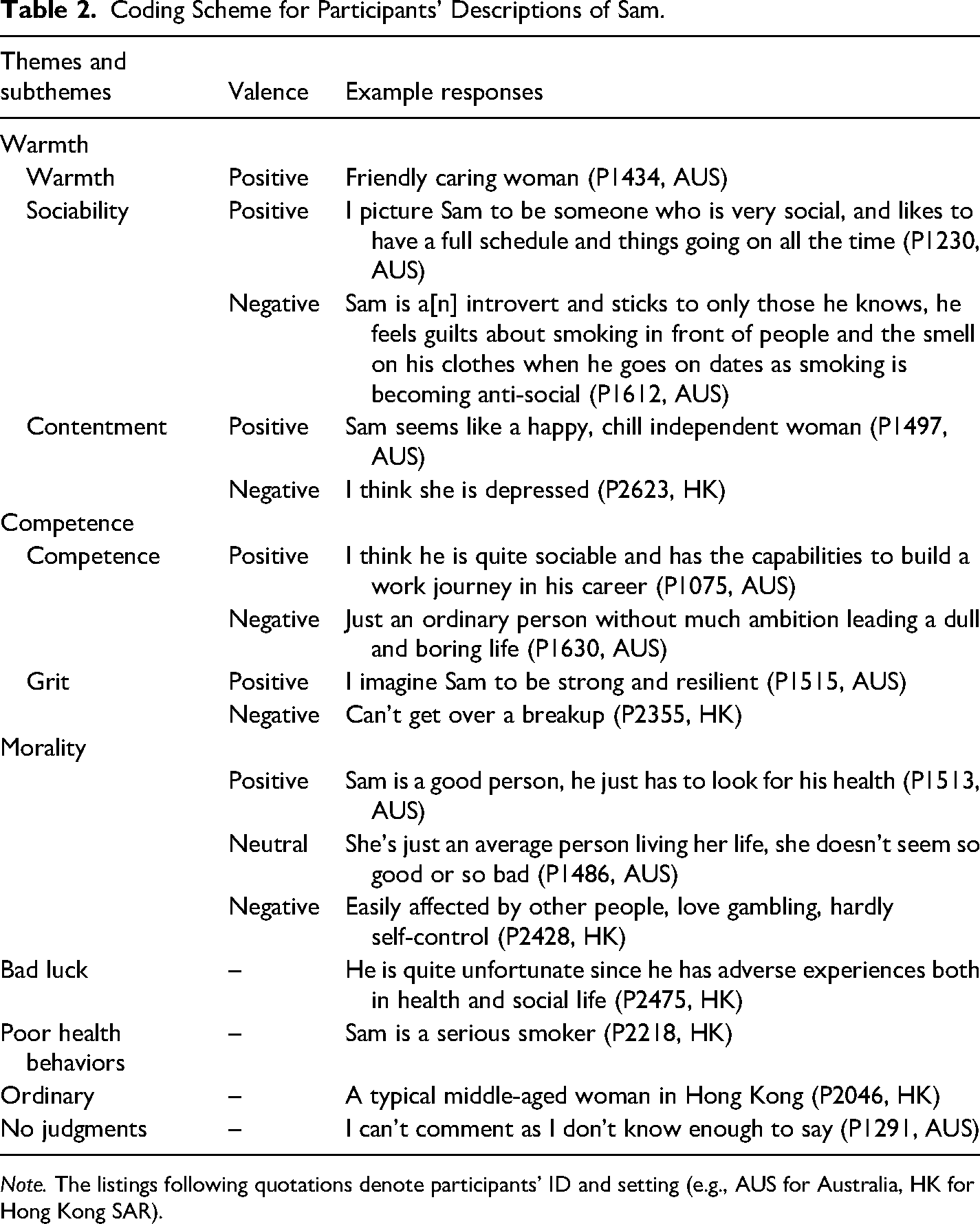
Note. The listings following quotations denote participants’ ID and setting (e.g., AUS for Australia, HK for Hong Kong SAR).
Results
A total of 303 participants provided open-ended responses about their open impressions of Sam. Ten subthemes were identified from these responses, with some being valenced as positive, negative, or neutral. These subthemes were then clustered and mapped onto the SCM, revealing seven main themes: Warmth, Competence, Morality, Bad luck, Poor health behaviors, Ordinary, and No judgments. However, the subthemes are reported individually in the following sections, to provide a detailed understanding of participants’ descriptions of Sam, including whether it was positive, neutral, or negative. The percentage of participants in Australia and the Hong Kong Special Administrative Region (SAR) mentioning each subtheme, along with their valence, was calculated and presented in Table 3. Table 3 also includes a breakdown of the percentage of participants mentioning each subtheme for Hong Kong SAR participants responding in English or Cantonese. Note, a chi-square test was also used to examine whether there was any significant difference across subthemes based on Sam's assigned gender in the vignette (either male or female). The analysis revealed that there were no significant differences in how participants perceived Sam based on the gender presented in the vignette.
Percentage of Participants in Australia and Hong Kong SAR Mentioning Each Theme and Subtheme.
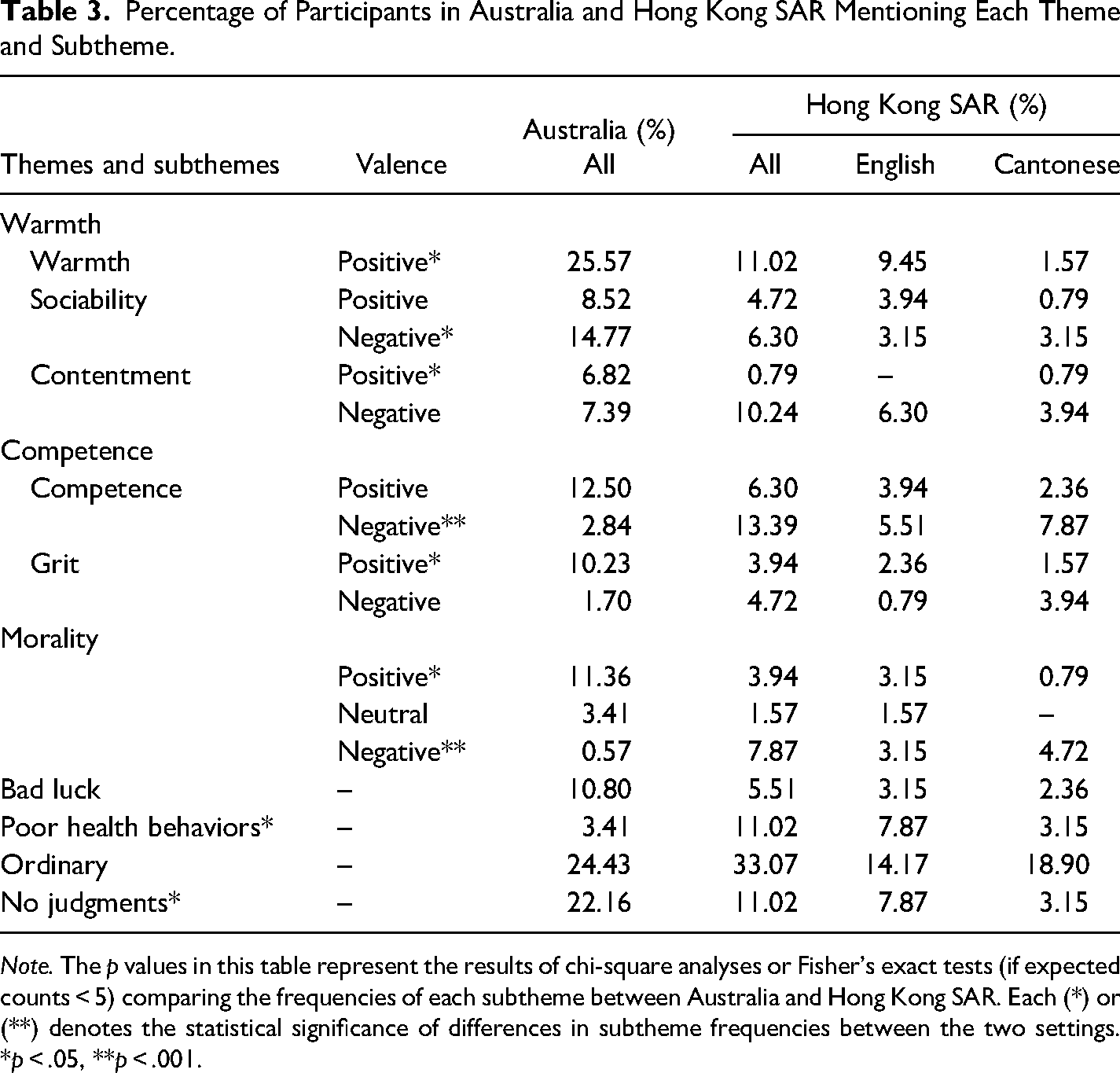
Note. The p values in this table represent the results of chi-square analyses or Fisher's exact tests (if expected counts < 5) comparing the frequencies of each subtheme between Australia and Hong Kong SAR. Each (*) or (**) denotes the statistical significance of differences in subtheme frequencies between the two settings. *p < .05, **p < .001.
Warmth
Warmth had three subthemes: Warmth, Sociability, and Contentment.
Warmth
All comments under warmth were positively valenced. Approximately 19% of participants described Sam as a warm person, demonstrating affection or kindness towards others. However, there were significant differences between cultures (p < .05), as positive warmth was mentioned more frequently by participants in Australia (25.57%) than participants in Hong Kong SAR (11.02%). Apart from being a “friendly and easy-going person” (P1606, AUS), Sam was mainly described as someone “nice and approachable” (P1532, AUS) by the participants. Specifically, one participant mentioned that Sam was an “everyday down-to-earth person” (P1301, AUS), and another participant stated Sam as someone who was “fun to be around” (P1366, AUS). In addition, some participants reported that they would like to be Sam's friend. For instance, one participant mentioned, “I think Sam is a good person and I’d be grateful to be her friend” (P1548, AUS). Responses included in this subtheme also highlighted the differences in language usage among participants from Hong Kong SAR, as positive warmth was more frequently mentioned in responses written in English (9.45%) compared to those in Cantonese (1.57%).
Sociability
Around 18% of participants brought up the sociability aspect of Sam in their responses, with some describing it positively, noting that Sam often engaged in social interactions and “enjoys going out with his friends” (P1534, AUS). Therefore, Sam was stated by many of these participants as someone who was “sociable, like[s] to interact with people” (P2524, HK) and “outgoing” (P2110, HK). However, some participants held different opinions, and their expressions about Sam's sociability were valenced negatively, as they primarily viewed Sam as an “introverted person who doesn’t have much social skills” (P1553, AUS). For example, one participant stated, “Sam is a quiet man who basically sticks to himself” (P1018, AUS). However, there were significant differences between cultures (p < .05), as negative sociability was mentioned more frequently by the participants in Australia (14.77%) than the participants in Hong Kong SAR (6.30%).
Contentment
Approximately 13% of participants discussed Sam's level of contentment in their responses, specifically referring to how enjoyable their lives appeared to be. However, there were significant differences between cultures (p < .05). Participants in Australia (6.82%) reported positive contentment more frequently than participants in Hong Kong SAR (0.79%). For instance, participants in Australia described Sam as someone who was “happy in himself” (P1604, AUS), “content with his routine” (P1074, AUS), and “living a comfortable, stable life” (P1043, AUS). Apart from positively valenced contentment, other participants also brought up negative contentment in terms of poor well-being. In this case, Sam was perceived as “having suffering[s]” (P1343, AUS) and “going through difficult times” (P1470, AUS). Specifically, some participants noted that Sam may be suffering from psychological issues, “I think she is depressed” (P2623, HK) or poor health, “[a] sick person” (P1575, AUS).
Competence
There were two subthemes categorized under the dimension of Competence: Competence and Grit.
Competence
Nearly 17% of participants included the attribute of competence in their responses, that is the ability or skill to be effective in work or life. For example, some described Sam as positively competent, to be “intelligent and hardworking” (P1109, AUS), as well as “skilled and capable as he has an impressive job that requires skills to complete” (P1538, AUS). A few other participants also commented on Sam's pay as an indicator of their competence level. For instance, one participant stated, “she could be anyone in a good paid job” (P1064, AUS). However, there were significant differences between cultures (p < .001), as participants in Hong Kong SAR (13.39%) mentioned more about negative competence than did participants in Australia (2.84%). For example, Sam was described as “someone who is not very self-disciplined” (P2552, HK), and that he “did not set himself a goal for his life” (P2039, HK). In addition to that, one participant stated that Sam was “not ambitious” (P2417, HK) because Sam was still employed as an administrative assistant at the age of 43. However, most of the participants from Hong Kong SAR who responded in English provided brief responses regarding this aspect, simply describing Sam as “not active” (P2359, HK) or as “a typical lower middle class man in Hong Kong” (P2037, HK). Those who responded in Cantonese, however, provided more lengthy and detailed descriptions of Sam's negative competence, such as “a person with no purpose in life, who only engages in entertainment activities such as playing mahjong and shopping during his spare time, without any further learning, and is relatively lazy” (P2494, HK).
Grit
Around 11% of participants stated the attribute of grit in their responses, alluding to the quality of determination in the face of challenges. However, there were significant differences between cultures (p < .05). Positive grit was mentioned more frequently by participants in Australia (10.23%) than participants in Hong Kong SAR (3.94%). For some, Sam was described as “brave” (P1357, AUS) and “with courage” (P1215, AUS). For others, Sam was described as “gritty” (P1502, AUS), “headstrong” (P1074, AUS), and “trying to live life as best as he can” (P2027, HK). In addition to the quality of determination, Sam was also stated by many as “optimistic” (P2097, HK) and “resilient” (P1515, AUS). For example, one participant described Sam as “a half glass full kind of guy who sees life in the lighter shade of light” (P1363, AUS). In contrast, some participants’ descriptions of Sam's grit were valenced negatively, as they imagined Sam as someone with “weak willpower” (P2366, HK) and “fragile on the inside” (P2358, HK). Responses included in this aspect also highlighted the differences in language usage among participants from Hong Kong SAR, as there were more lengthy and detailed descriptions of Sam's negative grit in responses written in Cantonese than those in English. One participant from Hong Kong SAR who responded in English simply described Sam as “weak” (P2559, HK), while another participant who responded in Cantonese provided a more detailed characterization, describing Sam as “someone who will run away from their problems, more negative, more pessimistic…” (P2127, HK).
Morality
Roughly 15% of participants addressed Sam's morality in their responses. However, there were significant differences between cultures (p < .05), with Australian participants (11.36%) discussing positive morality more frequently than participants from Hong Kong SAR (3.94%). Some of these participants stated that Sam was a “good man” (P2363, HK) or a “decent person” (P1112, AUS) guided by a moral compass. Specifically, one participant described Sam as “righteous” (P2530, HK), while another asserted that Sam was “respectful towards the community” (P1498, AUS). In addition, some participants believed that Sam was sincere and able to be relied on. For example, one participant mentioned, “she seems like a friendly, reliable person” (P1409, AUS), and another said, “sound[s] like a nice, genuine guy” (P2102, HK). Nevertheless, there were a few participants who offered neutral responses regarding Sam's morality. For instance, responses such as “Sam seems like an alright gal” (P1422, AUS), “he is an okay guy” (P1333, AUS) and “just like your everyday Aussie—no better and no worse” (P1371, AUS) were provided. There were significant differences between cultures (p < .001) in terms of negative morality, with participants in Hong Kong SAR (7.87%) reporting such expressions more frequently when compared to participants in Australia (0.57%). Among Hong Kong SAR participants, moral beliefs were that Sam was “easily influenced by others” (P2483, HK) and “addicted to gambling” (P2612, HK). There were also more lengthy and detailed descriptions of Sam's negative morality in responses written in Cantonese than those in English from the Hong Kong SAR participants in this category, mirroring the pattern observed with negative competence and negative grit. For example, most of these participants from Hong Kong SAR who responded in English simply described Sam as someone “bad” (P2192, HK), “not good” (P2206, HK) or a “player” (P2142, HK), providing short and concise responses. However, one participant who responded in Cantonese described Sam as “someone who loves to play mahjong at the mahjong school” (P2527, HK), while another commented that Sam appeared to be “someone who likes to play, and often go[es] to play cards…” (P2302, HK).
Bad Luck
Nearly 9% of participants believed that Sam was unfortunate and attributed their lung cancer to bad luck. Many participants who mentioned bad luck stated that Sam “seems to just be the victim of bad luck” (P1438, AUS) who has been “struck by an unfortunate and unlikely medical condition” (P1074, AUS). Specifically, one participant described Sam as “a middle-aged man who was doing alright, until his life came undone unfortunately due to his cancer diagnosis” (P1277, AUS). Some participants also claimed that Sam's diagnosis was unwarranted and that the onset of cancer was unexpected. One participant, for instance, described Sam as “an average girl with no pre-existing medical conditions but still got cancer” (P1293, AUS), while another remarked that Sam seemed to be “a very unlucky bastard [as] he did nothing to trigger cancer” (P1625, AUS).
Poor Health Behaviors
Approximately 7% of participants believed that Sam engaged in poor health behaviors and attributed their lung cancer to these behaviors. However, there were significant differences between cultures (p < .05), with Hong Kong SAR participants (11.02%) reporting poor health behaviors more frequently than participants from Australia (3.41%). Most of these participants assumed that “Sam is a serious smoker” (P2218, HK) and that they “should have quit [smoking] years ago and seen a doctor earlier” (P1211, AUS). In addition to smoking and delaying health-seeking behaviors, some participants pointed out how Sam was ignorant of their health. For instance, one participant mentioned, “he does not have a high awareness about his own health, because he should realise his after work activity is a poor activity. He probably smoked many second-hand smoke” (P2239, HK). Other participants highlighted Sam's “irregular lifestyle” (P2366, HK) and drinking behaviors, “Sam seems nice [but he] can’t bear the fact of the breakup and so [he] starts drinking” (P1429, AUS). As a result, these participants felt that Sam was “largely responsible for his plight” (P1358, AUS) and should be held accountable, as they have attributed Sam's lung cancer to poor health behaviors. Furthermore, descriptions related to Sam having poor health behaviors were also more frequently mentioned in English responses by Hong Kong SAR participants (7.87%) compared to those in Cantonese (3.15%). Of note, none of the Hong Kong SAR participants who responded in Cantonese under this theme mentioned that Sam might be a potential smoker, as most of them assumed that Sam was just “neglectful of their own body” (P2321, HK) and “do not know how to take care of themselves” (P2127, HK).
Ordinary
The most common expression among participants in both cultures (28.05%) was that Sam was an ordinary individual. This finding is unsurprising given that the vignette was designed to portray an ordinary person displaying symptoms of lung cancer and having received a diagnosis, providing further evidence to support the vignette's validity and effectiveness in eliciting participant responses. Examples of responses included “an ordinary Hong Konger” (P2349, HK) and “just an ordinary bloke” (P1185, AUS). Many of these participants described Sam as “someone who live[s] a normal life” (P2300, HK) with “nothing out of the ordinary” (P1409, AUS) and was “not much different than other ordinary people” (P2436, HK). Responses included in this theme also highlighted that Sam appeared to be a typical individual for their age. For instance, one participant mentioned, “I find Sam a normal person for his age showing attributes and habits of many like himself, except that he developed lung cancer” (P1603, AUS), while another stated, “I believe she is a typical person like many other similar aged females in Hong Kong” (P2049, HK).
No Judgments
Around 17% of participants expressed that they held no judgments towards Sam. However, there were significant differences between cultures (p < .05), with participants in Australia (22.16%) reporting having no judgments towards Sam more frequently than participants in Hong Kong SAR (11.02%). Many of these participants claimed that the information provided about Sam in the vignette was limited and that they “need to know more before coming to such a conclusion” (P1486, AUS). For instance, one participant mentioned, “the information provided tells me little of the person” (P1637, AUS). Other participants who were hesitant to express their opinions about Sam mostly commented that they “do not know” (P2340, HK) anything about Sam and were “unsure what to say” (P1391, AUS). In addition, some participants noted that they simply could not judge Sam. For example, one participant stated, “Sam could be an extremely good person, his decisions are his own, and no one has the right to judge anyone” (P1052, AUS). Similarly, another participant conveyed that it was not feasible for them to share their opinion, stating, “I’ve never met the bloke. How can I possibly express an opinion of this. To do so would be utter bullshit” (P1669, AUS). Notably, participants from Hong Kong SAR who responded in English (7.87%) reported having no judgments more frequently than those who responded in Cantonese (3.15%). In particular, most participants from Hong Kong SAR who responded in English also gave brief responses such as “no comment” (P2384, HK) and “not sure” (P2139, HK) under this theme.
Discussion
Through analyzing the open-ended responses regarding a vignette character named Sam, our study examined how the general public in Australia and Hong Kong SAR expressed their views about individuals with lung cancer. The results align broadly with prior literature, while also demonstrating the role of culture and language in shaping public discourse and stigma related to lung cancer across different contexts.
We found a number of similarities in how the general public describes cancer patients, suggesting that some impressions may be universal, while others are culture- or language-specific. For instance, consistent with past research, participants described people with lung cancer as warm but lacking in competence. Cancer patients are often viewed as deserving of kindness and empathy due to the significant health challenges they face (Cikara & Fiske, 2012; Fiske, 2018), but this is often accompanied by an assumption of low competence because they are seen as incapable of effectively managing their health and contributing to society (Badihian et al., 2017; Cho et al., 2012). In our study, most participants viewed Sam as having high warmth but low competence, highlighting a commonality in public discourse towards individuals with cancer. The observed similarities have also showcased the generalisability and robustness of the SCM and attribution theory across diverse cultural contexts.
Yet our findings also demonstrate significant differences in how Australians and Hong Kongers describe individuals with lung cancer through their written expressions. While both cultures expressed positive views on warmth, Australians tend to describe Sam as warmer compared to Hong Kongers. This accords with prior research which found that Westerners are usually high on both dimensions of warmth and competence, whereas Asians are often competent but cold, a stereotype derived from assumptions about their competitiveness (Cikara & Fiske, 2012; Hudson et al., 2019; Lin et al., 2005). Consistent with our initial expectations, participants from Hong Kong SAR were also more likely to describe Sam as lacking competence. For example, many of them attributed Sam's career progression to a lack of ambition and clear life goals because Chinese societies place a strong emphasis on career achievements (Le et al., 2020; Tsui et al., 2019). Hence, these cross-cultural variations underline the importance of considering cultural factors when studying health stigma.
Furthermore, our findings show that Hong Kongers were more inclined to make moral attributions about others compared to their Australian counterparts, consistent with previous research indicating that people from Eastern countries tend to do so more frequently than those from the West (Krendl & Freeman, 2019; Krendl & Pescosolido, 2020). Of note, we discovered that some of the Hong Kong SAR participants attributed Sam's lung cancer to karma resulting from violations of moral norms. As such, many of them commented on Sam as a player or someone who is heavily addicted to gambling. This aligns with past studies that found a traditional belief in Chinese culture that cancer is a form of punishment for patients’ moral failings or personal wrongdoings (Lee et al., 2013; Leung & Chan, 2015; Liu et al., 2020). In other words, Chinese people often interpret someone being diagnosed with cancer as being held accountable for their moral defects.
Contrary to our initial expectations, participants from Hong Kong SAR were more inclined to attribute Sam's lung cancer to poor health behaviors than their Australian counterparts. This lack of discussion among Australian participants is unexpected, given the prevalence of anti-tobacco campaigns and the denormalization of smoking in Western societies (Chapple et al., 2004; Evans-Polce et al., 2015). However, we observed that the automatic association of lung cancer with smoking was more common in the English responses among Hong Kong SAR participants, whose responses were similar to their Australian counterparts. By contrast, none of the Cantonese responses mentioned smoking; instead, most described Sam as having an irregular lifestyle and failing to take care of themselves. This is in accordance with previous research indicating that Chinese lung cancer patients are typically not stigmatized based on their smoking status (Liu et al., 2020, 2023), as their cancer was attributed to other factors instead. One potential explanation for this difference among the Hong Kongers’ responses is language priming effects. Several existing studies on Hong Kong Chinese-English bilinguals have shown that a given language can activate distinct cultural identities, knowledge, and shared meanings within an individual, influencing bilinguals to align their thoughts and responses with the cultural norms associated with the language used (Chen et al., 2014; Chen & Bond, 2007, 2010). Thus, our findings suggest that using the English language may have primed participants from Hong Kong SAR to think and express their impressions more similarly to Westerners, potentially leading to responses akin to those of Australians.
Participants from Australia were also more likely to report having no judgments towards Sam compared to the participants from Hong Kong SAR. Many Australians were hesitant to express their opinions about Sam, claiming that the information provided in the vignette was limited or stating that they had no right to judge. However, it is plausible that they hold internal stigmatizing beliefs about individuals with lung cancer but refrain from openly expressing them. This is in line with the findings of Occhipinti (2022), which highlight that Australians are less likely to admit to stigmatization, stating that others may stigmatize, but they themselves do not. This suggests that cultural norms may influence how judgments and stigma towards others are expressed.
Participants from Hong Kong SAR who responded in English similarly provided shorter responses, such as “no comment” (P2384, HK) or “not sure” (P2139, HK) under the no judgment theme. In contrast, those who responded in Cantonese were more open to providing direct and detailed descriptions about Sam. This is consistent with Lee et al. (2010), suggesting that English may prime an individualistic mindset and Chinese a collectivistic mindset, demonstrating how language choice may influence individuals within the same culture to express opinions differently. Hence, the use of English language might have activated cognitive schemas or cultural scripts associated with Western cultural norms, thereby potentially influencing these Hong Kong SAR participants to be less assertive and expressive in their judgments, resembling the pattern observed in their Australian counterparts.
Our study highlights differences in how lung cancer stigma manifests in different cultural and linguistic settings, stemming from distinct sources of stigma. The perceived nexus between lung cancer and smoking, commonly discussed in the Western literature on lung cancer stigma, was evident in the responses from Australians and Hong Kongers who chose to respond in English. However, our findings also support existing research on lung cancer stigma in Chinese cultural contexts, suggesting that stigma faced by lung cancer patients may also stem from perceptions of low morality, bad karma, and even low competence (Lee et al., 2013; Leung & Chan, 2015; Liu et al., 2020). These cultural variations not only exist between Australia and Hong Kong SAR but also within Hong Kong SAR itself, particularly influenced by participants’ choice of language in responding to the survey (Cantonese vs. English). This suggests that language choice may influence how stigma is expressed or transmitted in a particular context, although it is not the sole determinant of one's thoughts. Overall, our results shed light on the cultural nuances surrounding public discourse on lung cancer, indicating that the foundation of stigma lies within the language used by the general public to convey their impressions of individuals with lung cancer and that such expressions may serve as potent precursors for stigmatization. However, future research should delve deeper into this phenomenon to explore whether these stigmatizing perceptions and descriptions of individuals with lung cancer would translate into actual stigmatizing actions, such as prejudice or discrimination.
Our study had limitations. First, we assumed a homogeneous sample for Asian culture, focusing primarily on Hong Kong Chinese. However, recent cross-cultural research has emphasized the complex nature of cultural differences, cautioning against the oversimplification of East-West stereotypes (Alden et al., 2018; Pines et al., 2023). For example, a study by Pines et al. (2023) highlighted that individuals from Australia and the Philippines shared more similarities in healthcare decision-making. Likewise, individuals from the United States and Hong Kong SAR also displayed commonalities, contradicting previously held East-West stereotypes (Pines et al., 2023). Therefore, future research should include a wider range of Asian cultures, ethnicities, and regions, to enable a more comprehensive examination of lung cancer stigma across different Asian and non-Asian cultures, considering variations across multiple regions and countries, particularly in an era of increased global mobility.
Another limitation of this study is that we did not collect data on participants’ own experiences with cancer or smoking, which could serve as potential moderators in the expression of stigma. Given the impression formation task, it is plausible that individuals with personal experience or exposure to lung cancer or smoking may exhibit different perceptions compared to those without such experiences. Future research could explore how personal experiences influence the formation of stigma, providing deeper insights into the role of lived experiences in shaping perceptions toward individuals with lung cancer. In addition, how participants’ age might influence their perceptions of smoking and lung cancer is noteworthy. Given the evolving social norms against smoking over the past decades, older and younger generations may have had different exposures to smoking-related advertisements, anti-tobacco campaigns, and societal attitudes towards smokers (Greenhalgh, 2019; Riley et al., 2017; Vachani et al., 2017). Therefore, future research could explore how these generational differences influence views towards individuals with lung cancer.
Moreover, the open-ended survey responses we collected were also limited in terms of context and depth. Interviews with probing questions allow for greater flexibility and in-depth exploration of participants’ impressions about individuals with lung cancer. The shorter responses in English by participants from Hong Kong SAR may also reflect limited proficiency, but this is less likely given they were offered the choice to read and answer the survey in either language, with approximately 56% of them opting for English. Nevertheless, we need to better understand how language proficiency and choice may intersect and influence people's perceptions and stigma expressions. Future research could also consider assessing the frequency of stigmatizing labels (e.g., “smoker”) versus person-first language in the context of lung cancer stigma, to explore how different forms of language influence perceptions.
In conclusion, our study contributes to research on health stigma by underscoring the role of culture and language in shaping public discourse surrounding lung cancer. Our findings reveal both universal and culture- or language-specific impressions formed by the general public about individuals with lung cancer, highlighting the need for culturally and linguistically sensitive approaches to address the growing issue of lung cancer stigma globally. Understanding these nuances is vital for developing novel and effective public health strategies and anti-stigma interventions that address both the consequences (e.g., psychological distress and poorer quality of life) and the sources of lung cancer stigma (e.g., smoking and karma), particularly in Eastern Asian contexts where cultural beliefs and values are widely shared and firmly upheld. Such efforts can potentially remove barriers to timely medical help-seeking among the stigmatized populations, improving the outcomes for lung cancer patients from diverse cultural and linguistic backgrounds, with the long-term benefit of reducing the burden of cancer death.
Supplemental Material
sj-docx-1-jls-10.1177_0261927X251318879 - Supplemental material for Where There's Smoke, There's Stigma? Written Expressions About Individuals with Lung Cancer Reveal Cultural and Language Differences
Supplemental material, sj-docx-1-jls-10.1177_0261927X251318879 for Where There's Smoke, There's Stigma? Written Expressions About Individuals with Lung Cancer Reveal Cultural and Language Differences by Esther Ong Zhen Mei, Liz Jones and Stefano Occhipinti in Journal of Language and Social Psychology
Footnotes
Acknowledgments
We would like to thank all research assistants who made this work possible, especially Ivy Wu for translating the survey into Cantonese, and Amanda Au for her contribution in data coding.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Parts of this research were supported by a grant from the Griffith University (Health)/The Hong Kong Polytechnic University (Faculty Of Health and Social Sciences) Collaborative Research Grants Scheme to S. Occhipinti, L. Jones, B. M. Watson, and A. S. K. Chen and by a grant from The Faculty of Humanities Dean's Reserve, (P0043804) to S. Occhipinti.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.