
Abstract
Many financial assistance programmes that target low-income individuals use income thresholds to determine eligibility. Eligibility serves as a critical interface between service applicants and providers, yet eligibility remains undertheorised in the policy literature. Drawing on interviews I conducted with both breast cancer survivors and providers of a range of health-related services, I focus on how organisations make income relevant for access to their services. This making-relevant-for-access is what I conceptualise as ‘doing’ eligibility. Eligibility is thus not a pre-existing status; it emerges through organisational practices. And when these practices change, who becomes eligible changes as well. I explore how different organisations ‘do’ eligibility through income thresholds. Focusing on processes for determining eligibility, rather than categories of eligible individuals, provides new insights into how disparities may be produced and reproduced through seemingly objective work practices such as the calculation of income thresholds.
Introduction
US health policy focuses primarily on insurance as a mechanism to enable healthcare access. This focus is evident in laws such as the Patient Protection and Affordable Care Act (ACA) and HealthyPeople priorities to improve the nation's health (HealthyPeople 2030, n.d.; Institute of Medicine, 2001). Insurance does play a significant role in facilitating access. Americans without health insurance are less likely to access health and preventive care, more likely to delay or forgo needed care, and to experience poor health outcomes and higher mortality (Institute of Medicine, 2002; Tolbert et al., 2024; Woolhandler and Himmelstein, 2017). But even individuals with insurance sometimes lack access to care because they do not have enough money to cover copayments, fill prescriptions, or pay for transportation to get to healthcare appointments (Raudenbush, 2020). This is especially true for individuals at the lower end of the socioeconomic spectrum.
The policy linkage between insurance and access clouds understanding how access is affected by household income. Income, separate from insurance, is usually absent from US health policy discussions, yet unmistakably present for Americans who struggle with both access to and affordability of care. A landmark study on cancer disparities found that poverty contributed to decreased survival, in part through decreased access to healthcare (Freeman, 1989). Low-income individuals are more likely to experience financial burdens during cancer treatment (Smith et al., 2019) and long-term financial consequences after treatment (Shih et al., 2022), including higher likelihood of debt or bankruptcy (Banegas et al., 2016).
In my research, the guiding question was how women with breast cancer obtain access to health and supportive care services. But in focusing on access, I became aware that access is not something (like insurance) that one either does or does not have; instead, access is something one achieves, often with effort. I argue that access occurs through eligibility enactments, or doing eligibility. Insurance can be seen as one way of doing eligibility; other eligibility enactments rely on income thresholds, or means testing. This article focuses on the nexus of income, eligibility, and access based on qualitative data. I begin with a story from my research that illustrates this nexus.
Bella,
1
a Spanish-speaking immigrant, was working as a housecleaner when she was diagnosed with breast cancer. She had no health insurance, but qualified for free breast cancer diagnostic services through a government programme based on her income. After her diagnosis, she was told to apply for Medi-Cal, California's version of Medicaid that provides low-cost or no-cost health coverage to low-income residents. Medi-Cal designates multiple means-tested programmes that each calculate eligibility differently based on household income, personal assets, age, disability, and the presence or absence of children. Bella explained,
2
I go to Medi-Cal and we go to apply, and my husband brings his taxes, all his information, and they say that he earns too much and that we don’t qualify…. And what they would say was so frustrating to me. They would say that if I had children from…another man, or if my husband had children from another woman, then I would qualify.
Bella was perplexed why her income was low enough to qualify for free diagnostic services, but not low enough for Medi-Cal to cover her treatment. She was also dismayed by the suggestion that she (or her husband) might have extramarital children. This insinuation failed to explain how the number of children was relevant for Medi-Cal (the allowable income threshold increases with family size, so Bella's income might have qualified if she had more children). Trying to access cancer treatment, she and her husband ‘battled a lot with Medi-Cal’.
We might perceive that Bella's difficulties accessing treatment resulted from lack of health insurance – a problem that the 2010 passage of the ACA attempted to rectify. Prior to the ACA, commercial insurance companies could decline coverage of individuals with pre-existing conditions such as cancer (Claxton et al., 2016), making someone like Bella virtually uninsurable. Pre-ACA, Medicaid primarily provided coverage to individuals with disabilities, pregnant women, older adults, and low-income families with children under age 18. The ACA expanded Medicaid coverage (in states that adopted the expansion, including California) to adults ages 19–64 with incomes at or below 138% of the federal poverty level regardless of whether they had children. In 2002, California also implemented a special Medi-Cal programme to cover breast and/or cervical cancer treatment (Department of Health Care Services, n.d.). Bella's diagnosis in 2000 predated these policy changes.
Bella's story illustrates the pivotal role of income for access to cancer treatment. She was able to obtain a Medi-Cal plan, but not one that covered all treatment expenses. Since her monthly income exceeded the Medi-Cal income threshold, she ended up with a share of cost plan. Her monthly ‘spend down’ amount of $1500 represented the difference between her income and the Medi-Cal limit (California HealthCare Foundation, 2010). Every month she had to pay the first $1500 of her treatment costs before Medi-Cal covered the remainder.
After Bella's third chemotherapy, she explained, ‘they suspended the treatment because we couldn’t – [she broke off into long silence]. We had to get the money. By that time, it was $4500 to be able to continue with the treatment’. Had Bella's income been slightly lower, she would have qualified for a no-cost Medi-Cal plan and paid nothing for her treatment. Had her income been slightly higher, she would not have qualified for Medi-Cal coverage and likely incurred significantly more debt. For Bella, getting Medi-Cal meant she could get treated – but not that she could afford her treatment. In fact, her public health insurance put her at significant financial risk, resulting in delays and possibly affecting her poor treatment outcome; three years later, her cancer metastasised to her bones and lung.
The policy emphasis on insurance-as-access obscures the fact that insurance is not always sufficient for access to healthcare, and often irrelevant for access to many other services needed by women during and after breast cancer treatment. Similar to Bella, many Americans need financial assistance to get through cancer treatment – not only to cover out-of-pocket copayments or deductibles, but also basic expenses of daily living such as food, gas, utilities, and rent. Foundations and nonprofits, often community-based, provide financial support either directly as cash assistance, or indirectly through no-cost provision of wigs, breast prostheses, transportation, and other services. The amounts of financial assistance are generally quite modest, especially compared with the high out-of-pocket expenses associated with cancer treatment; assistance ranges from $25 to several thousand dollars.
Many financial assistance programmes that target individuals at the lower end of the socioeconomic spectrum rely on income thresholds to determine eligibility. Drawing on interviews I conducted with service recipients and seekers as well as service providers, I focus on the organisational practices that make income relevant for access. This making-relevant-for-access is what I conceptualise as ‘doing’ eligibility.
I first outline some common assumptions about eligibility in the literature on access to healthcare and social services. I then explore empirically how different organisations ‘do’ eligibility using income thresholds, and discuss the equity implications of different eligibility enactments. I conclude by contextualising my approach in relation to street-level bureaucracy and administrative burdens, two other approaches to policy implementation and its equity consequences.
Methodology
This analysis is part of a larger study that maps women's access to breast cancer and supportive care services in a medically underserved region in Southern California (Lefkowitz, 2022). This region encompasses two counties with a population of over 4.6 million. Slightly more than half the population is Hispanic/Latinx, 42% speak a language other than English (predominantly Spanish), and the poverty rate is significantly higher compared to both California and the US. 3 (Brady et al., 2021: 2–3). Since many provider networks, insurance plans, and nonprofit services cover both counties, I analyze the counties as a single entity.
I conducted in-depth semi-structured interviews from 2011 to 2017 with adult women diagnosed with any stage of breast cancer, who spoke English or Spanish, and resided in the study region; Bella (discussed above) and Grace (discussed below) were among the participants. A trained healthcare interpreter accompanied me for Spanish-language interviews. I also conducted interviews from 2016 to 2017 with adult men or women who worked or volunteered for organisations that provided survivorship services. Under organisations, I included formal entities (e.g., healthcare facilities and nonprofit agencies) as well as informal organisations (e.g., support groups). I defined survivorship services to mean services provided directly to breast cancer survivors, whether in person, online, or by telephone.
My selection of participants was guided by concepts that emerged from the data rather than established in advance of data collection (Charmaz, 1990; Chun Tie et al., 2019). I sought to encompass as wide a range of experiences as possible to understand the dimensions of survivorship service delivery from the perspectives of both providers and recipients. Data collection and analysis proceeded together such that emerging analytic insights informed further data collection.
Altogether my research sample comprised 84 service providers and 82 breast cancer survivors. About half the survivors identified as Hispanic/Latina, African American, or mixed race; close to one third were uninsured or Medi-Cal recipients and therefore low income. To protect the privacy of research participants, each interview was assigned a unique alphanumeric code; survivors were also assigned a first-name pseudonym. When citing interview transcripts, I reference only the survivor pseudonym or the service provider's role (e.g., oncology nurse).
All interviews were audio-recorded. I wrote extensive notes during the interviews that helped me make sense of what was said, captured my responses to the interaction, and suggested further follow-up. I used these notes for writing memos to expand on my emerging insights (Charmaz, 2006). I created detailed transcriptions from the audio-recordings, then imported the transcriptions into ATLAS.ti for coding. Following the practices of other qualitative researchers (Corbin and Strauss, 2008; Glaser and Strauss, 1967), I began with a line-by-line reading of my transcripts, using inductive categories to describe my data. Through iterative coding, these categories became more clearly defined and increasingly theoretical. I began to understand eligibility as more than a binary relationship between individuals who are eligible and those who are not.
The university's Institutional Review Board approved all study procedures. Consent for data collection allowed the author to retain data for subsequent analyses.
Conceptualising eligibility
Eligibility serves as a critical interface between service seekers and service providers. In the literature on access to healthcare and social services, eligibility has been largely overlooked, or assumed as a given, and therefore undertheorised. Differences in how eligibility is enacted, or ‘done’, have consequences for individuals seeking services, for organisations providing services, and for policies aimed at eliminating disparities. How we conceptualise eligibility therefore matters.
There are several common assumptions about eligibility. First, eligibility is often conceptualised as criteria that determine who can obtain services. These criteria are used to assign people to the categories of eligible or ineligible. This conceptualisation suggests a clear differentiation between those who are eligible and those who are not, with non-overlapping membership. For example, the ACA specifies several income thresholds for financial assistance to make health insurance more affordable for low-income Americans: those with incomes up to 250% of the federal poverty level (FPL) 4 are deemed ‘fully eligible’ (eligible for both premium and cost-sharing assistance); those with incomes of 251–400% FPL are ‘partially eligible’ (eligible for premium assistance only); and those with incomes over 400% FPL are ineligible (Fung et al., 2017: 24). These three categories are presumed to be non-overlapping since an individual cannot have income that is simultaneously above and below 250% FPL.
Yet the assumption of a clear-cut distinction ‘conflates the simplicity of the category with the subtlety and complexity of the phenomenon categorized’ (Suchman, 1994: 185). Categorisation often simplifies complex phenomena into dichotomous groups (Stroumsa et al., 2019: 1886), such as eligible or ineligible, creating cleanliness and order out of mess and chaos (Mol and Law, 2002). In practice, mutually exclusive category assignments may not be possible (Bowker and Star, 2000), as I demonstrate in the next section.
A second assumption about eligibility is that category assignments describe the people who are categorised, not the act of categorising. Individuals are eligible for benefits or services because of who they are, based on personal attributes such as income, age, insurance, or immigration status. And they are eligible regardless of whether they actually enrol in programmes, receive the services to which they are entitled, or act based on their eligible status. This suggests eligibility as something that inheres in individuals, independent of their actions – or the actions of service providers.
To assume eligibility as an inherent characteristic of people shifts our gaze away from the process of assigning eligibility categories. Even when it appears straightforward, assigning categories is often socially, politically, or ethically charged (Bowker and Star, 2000). The categorical judgments that determine what ‘counts’ as an eligible case can be ‘difficult and controversial’ (Martin and Lynch, 2009: 243). Within an organisational context, these judgments make the resulting categories relevant for whatever actions the organisation may take (Caswell et al., 2010: 389). Categorisation practices ‘profoundly shape the way in which we think and act on social policy issues’ (Caswell et al., 2010: 385); they are thus consequential for individuals targeted by those policies.
Rather than thinking about eligibility in terms of who is eligible, I focus on how eligibility gets done. I follow Mol's (2002) use of the term enactment to refer to the way things come into existence through specific practices. Eligibility emerges through the practices of service delivery systems that make attributes such as income relevant for access. Most often, income becomes relevant for access in terms of income thresholds. Different enactments of eligibility have appreciable consequences for who gains access to services and benefits.
‘Doing’ income thresholds
Many programmes targeting low-income individuals use income thresholds to determine eligibility. Assessing income thresholds is how these programmes ‘do’ eligibility. The amount of the threshold varies by programme. For example, for Medicaid, the income threshold is 138% FPL; for the Supplemental Nutrition Assistance Program, the threshold is 130% FPL. Within the same programme, the threshold amount may vary from state to state, adding to the complexity of access to the US safety net. In the following discussion, the specific threshold amount is not in question. I focus instead on how different organisations do income thresholds to enact eligibility.
We generally think of income thresholds as straightforward numerical cutoffs: everyone with income below a predetermined threshold is eligible, everyone above the threshold is ineligible. Grace articulated this view when describing how she gained access to the Breast and Cervical Cancer Treatment Program (BCCTP), a special Medicaid programme: ‘And I just made the money cap. I mean within fifty dollars. I just fell under their radar to be qualified’. With her BCCTP coverage, as she explained, ‘I paid no copays. I paid for nothing’.
Similar to Bella discussed above, Grace was uninsured at the time of her breast cancer diagnosis. But unlike Bella, her income was low enough to qualify for the BCCTP (under 200% FPL). Falling just under the income threshold was highly consequential, both for Grace's ability to obtain cancer treatment and for not incurring debt in doing so. If her income had been just one dollar over the income threshold, she would not have been covered. Average costs for Grace's stage III cancer (as allowed by a commercial insurance company) amounted to $129,387 (Blumen et al., 2016: 28).
This is an example of a benefits cliff, where just a single dollar more or less can mean the difference between having or losing a benefit, and lead to significant financial consequences. But income thresholds are not simple numerical cutoffs. Similar to other classification schemes, they hide ‘the messier version of what is inside’ (Star and Bowker, 2007: 273). Federal, state and local programmes that use poverty guidelines in eligibility determinations ‘may define income in different ways’ (ASPE, n.d.-a). For example, ‘some agencies compare before-tax income to the poverty guidelines, while other agencies compare after-tax income. Likewise, eligibility can be dependent on gross income, net income, or some other measure of income’ (ASPE, n.d.-a). And programmes that use income thresholds also require different kinds of documentation to substantiate income claims.
In my interview data, I found considerable variation in how organisations enacted eligibility using income thresholds. I discuss several examples and then consider the implications of different eligibility enactments for health equity.
Doing income thresholds as income minus expenses
When income thresholds are used to determine programme eligibility, financial documents must be produced to verify individual or household income. One commonly requested document is the tax return. Not everyone files a tax return. More importantly, the tax return may not reveal a cancer patient's true financial predicament. In part, this is due to the temporal nature of the document: the tax return reflects income for the last calendar year, a period that generally precedes the cancer diagnosis. During cancer treatment, families often experience a loss of income if one or more wage earners takes time off for treatment or caregiving.
The president of a nonprofit financial assistance foundation for cancer patients explained that her foundation uses 400% FPL as its income threshold, but ‘the federal poverty level is only a guideline and doesn’t really truly assess the economic disadvantage of each person and/or their family’. For example, the FPL does not take into account significant differences in the cost of living across states, or between rural and urban settings (Fass, 2009: 2). Similarly, the FPL does not account for the increased out-of-pocket expenses that accompany a cancer diagnosis. As the nonprofit's president explained, ‘Even though on paper it appears that they are, you know, middle income or above middle income’, if you figure out a family's expenses after one member has been diagnosed with cancer, you might realise ‘that they are literally just making it every week’.
The foundation takes into account a family's newly incurred medical expenses in addition to the amount of income on its tax return. This strategy may present quite a different picture of the family's income compared to the previous year's tax return. In this way, a family might be deemed eligible for financial assistance by the foundation, but not by agencies that assess eligibility solely based on the tax return.
Similarly, ‘We’re looking at the entire disease process, what is it going to take you…to be cancer-free’, the outreach director of a charity transportation service explained. ‘[I]t's not a snapshot, it's not what your bank account has in it now’. In determining eligibility, his organisation considers that a cancer patient might not be able to show up for work, might have high medication costs, or ‘their copayments might have to equal 12 grand before insurance actually starts to pay. So, you know, it's, it's all of those factors that come into play’.
In these eligibility enactments, income is understood to mean more than the number that appears on a pay stub or last year's tax return. Another organisation, in contrast, provides assistance to ‘those that fall within the 300% FPL guidelines’ based on ‘appropriate documentation’, specified as ‘two years of tax returns’ and ‘bank accounts’. Enacting eligibility as income-minus-expenses presents quite a different picture of a family's level of income.
Doing income thresholds as negative net income
The director of Breast Cancer Helpers,
5
a nonprofit that provides financial assistance to breast cancer patients, described her agency's typical client as someone whose ‘income and expense ratio every month put them in the red significantly’. Someone for whom money was tight, but ‘maybe they’re still $200 ahead every month, you know, that's not somebody who's going to be eligible for us’. As she explained: We’re really looking at, you know, a shortfall in income and expenses and the lack of resources to address that shortfall. So, if somebody comes to us and…they were making $10,000 a month prior to breast cancer treatment and $8000 now, that might be somebody who really does have the financial means or equity in their home or something like that to be able to make up that shortfall.
Income threshold, as enacted by Breast Cancer Helpers, is therefore not a specific number or percentage of FPL. Rather, it is a comparison between income and expenses that results in a negative number. And it is not only the income shortfall that is considered, but also the lack of resources such as savings, home equity, or other liquid assets.
Breast Cancer Helpers’ director also emphasised the importance of making sure ‘that breast cancer is what's impacting their financial change’, and not a chronic problem with spending that exceeds household income. In determining eligibility, this nonprofit assesses applicants’ household income and expenses both before the cancer diagnosis, and at the time they make the request for financial assistance.
The director of Cancer Caregiving, another nonprofit, explained the rationale for excluding applicants with long-term financial difficulties: [I]f they’re in financial straits because of cancer…our grant is probably going to be enough for them ‘cause…it’ll help them get through [cancer] and get them back to where they were. But if they were in trouble before [cancer], we want to make sure that we’re kind of moving them in a direction to have a longer-term solution and not just, you know, here's a band-aid but it's not really gonna fix anything.
This emphasis on addressing budget shortfalls due specifically to cancer treatment also means that generally no assistance is available once treatment ends, regardless of whether individuals still experience financial hardship. Overall, cancer survivors have significantly higher out-of-pocket healthcare costs compared to individuals without a cancer history, especially those who are low income (Guy et al., 2015). Yet as Leana experienced when she sought financial support after completing chemotherapy and radiation, ‘Some type of programme…needs to help people after their treatments, getting themselves back on their feet…. Every time I called, “oh sorry, we only help….” [I]t's disappointing’.
The director of the breast cancer nonprofit We Care similarly highlighted that the financial assistance her organisation provides is not designed as long-term support. ‘I mean we’re not in a position to help people out in, in a big way long term. And that's really not my goal’, the director explained. ‘My goal is to be able to help them get through [treatment]’.
Negative net income is thus not a simple calculation of income above or below a specific cutoff, but a more complex assessment of income and expenses, before and after the cancer diagnosis, and in relation to the availability of other resources. Enacting eligibility as negative net income requires documentation other than the tax return. For example, Cancer Caregiving requires its applicants to provide a budget along with copies of bills and income statements. The amount of financial assistance is determined by the gap between income and expenses in the submitted budget. The director of Cancer Caregiving explained: ‘We match up copies of the bills…and then we take a look at what the difference is between the income and the out-go…. So, we try to make that difference up for them’.
When eligibility is enacted as negative net income, it is the size of the gap between income and expenses that is significant, not the total amount of income (or total income minus expenses). Individuals with higher incomes may have a large gap if they have proportionately high medical expenses. By examining a hypothetical example, we can see that different individuals become eligible, or ineligible, depending on how income threshold is enacted.
Suppose three individuals each live in a single-person household. One has a monthly income of $800 and $1200 of monthly expenses; the second, a monthly income of $3200 and the same $1200 of monthly expenses; and the third, the same monthly income of $3200 but $3600 of monthly expenses. Table 1 illustrates eligibility for these three individuals using (1) income cutoff ≤ 200% FPL, (2) income minus expenses ≤ 200% FPL, and (3) negative net income.
Eligibility enacted in three different ways using income thresholds.
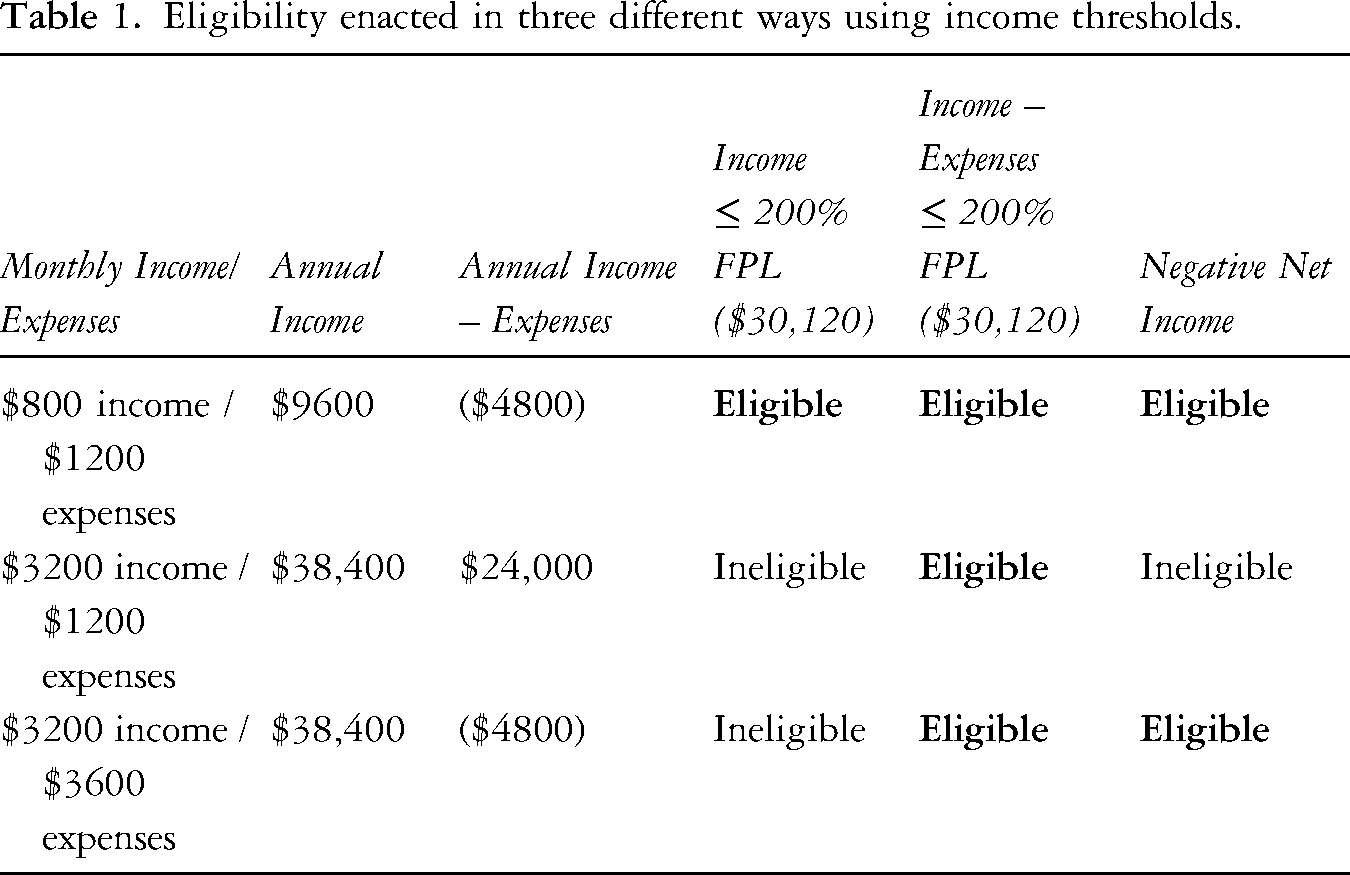
The 200% FPL threshold used in these examples is a common measure of ‘low income’ in the US (Macartney and Ghertner, 2023). As one nonprofit director explained, ‘that number is so critical because that's the number that renders [people] eligible for other types of federal support’. Adjusted for inflation, the dollar amount of the FPL changes every year. In 2024, 200% FPL corresponded to $30,120 for a single-person household. 6
The individual with a monthly income of $800 is eligible using all three enactments. The two individuals with a monthly income of $3200 are each eligible using one or two of the enactments, but not all three. For the individual with $3200 monthly income and $1200 monthly expenses, subtracting expenses from income results in a monthly income of $2000 ($24,000 annually). This net income is well under 200% FPL, and therefore constitutes eligibility using the income minus expenses ≤ 200% FPL. Since $3200 income minus $1200 expenses results in a positive number, this individual is not eligible using negative net income. The individual earning $3200 monthly with $3600 monthly expenses is eligible using both income minus expenses ≤ 200% FPL and negative net income.
These three different ways of doing income thresholds demonstrate that some individuals could be both eligible and ineligible for financial assistance, depending on how a programme calculates income, assets, and financial need. By focusing on what organisations do when they enact eligibility, we can see that multiple enactments are possible, even when income threshold is the criterion for eligibility. Therefore, eligibility cannot be understood as a way of categorising non-overlapping groups based on income, since income is not a fixed and stable amount. What is considered income for purposes of doing income thresholds depends on the organisational practices that make income—or income minus expenses, or any other income calculation—relevant for eligibility.
The above examples demonstrate that doing income threshold as income minus expenses ≤ 200% FPL enables the largest number of individuals to become eligible (all three of the hypothetical examples), while doing income threshold as income ≤200% FPL allows the smallest number of individuals to become eligible (one of the hypothetical examples). In stating this, I do not mean to imply that income minus expenses is the best, or most inclusive, form of eligibility enactment using income thresholds. Rather, I wish to point out that different practices matter for which individuals, and how many individuals, will be deemed eligible and thereby enabled to access financial assistance or other means-tested services.
Eligibility as policy
Doing income thresholds is a ubiquitous practice among US financial assistance programmes, whether administered by a government agency or nonprofit organisation. I discussed three distinct enactments above, although there are other potential variations of doing income thresholds (such as income plus assets, income plus required participation in another social service programme, and so on). My purpose in differentiating among three enactments is first, to demonstrate that seemingly similar enactments can create very different populations of eligible individuals; and second, to highlight the potential for eligibility enactments as policy.
From an organisational perspective, eligibility enactments are necessary to balance the ability to provide financial assistance (based on available funding) with demand for that assistance. While ‘covering whoever is eligible’ may be an unobtainable policy goal (Lei, 2014), US means-tested programmes vary widely in participation rates, defined as the percentage of the total ‘eligible’ population that actually receives programme benefits. In 2018, for example, participation rates ranged from 78% for the Earned Income Tax Credit to 15% for subsidised child care (Macartney and Ghertner, 2021: 2). Programme participation rates also vary significantly over time, and by state. Critics of income-based eligibility argue that means testing misses a large number of people with genuine need for support. ‘Either they don't know about [benefits], they don't realise they are eligible for them, or perhaps, particularly important, they are reluctant to claim them’ (Beresford, 2013). These challenges of accessing public benefits can undermine policy goals and exacerbate existing inequalities (Herd et al., 2023).
US policy research has focused primarily on two approaches to the conundrum of eligibility and its consequences for equity. One approach, developed from Lipsky's (1969, 1978, 1980[2010]) research on the administrative practices of street-level bureaucrats, focuses on the pressures experienced by frontline workers when interacting with service applicants. The other approach, developed by Herd, Moynihan and their colleagues (Christensen et al., 2020; Herd et al., 2013, 2023; Herd and Moynihan, 2018; Moynihan et al., 2016), focuses on the administrative burdens experienced by individuals when interacting with state and other agencies. These two approaches view eligibility from different vantage points, and lead in divergent policy directions. Both differ from my own conceptualisation of eligibility and its policy usefulness.
Lipsky's analysis of street-level bureaucrats, the frontline workers that interact directly with the public (1980[2010]: 3), emphasised the role of discretion. ‘While eligibility for public service benefits often may seem cut-and-dried’, he argued, ‘discretion must be used in determining eligibility for the presenting situation’ (1980[2010]: 60). In his view, eligibility is ‘the process of reducing a person to his or her qualifications for bureaucratic intervention’ (1980[2010]: 105). Turning individuals into clients requires developing an appropriate set of categories, assigning the categories to people, and then treating people in terms of those categories. Discretion enters this process because predetermined categories of action cannot anticipate every possible client scenario; policies may also be ambiguous or contradictory when applied to a specific case, and therefore require some degree of interpretation or judgment (Rowe, 2025).
Through the exercise of discretion in assigning eligibility to some would-be clients and not to others, Lipsky considered street-level bureaucrats to be making policy (Lipsky, 1978, 1980[2010]). Policy, according to this view, is not what is enacted in laws, but rather how laws get implemented through frontline workers’ case-by-case decision-making. Although Lipsky emphasised that categorisation is indispensable to bureaucratic decision-making, he acknowledged that racial and class biases can influence category assignments, especially in interactions with low-income and minority clients who are the most dependent on government services and financial assistance (Lipsky, 1969).
The administrative burden literature similarly foregrounds service encounters of those disadvantaged through low income, poor health, or cognitive decline (Christensen et al., 2020), but focuses on how these encounters are experienced by service seekers, not service providers. Administrative burden is defined as individuals’ ‘experiences of costs’ (Christensen et al., 2020) or ‘frictions’ (Herd et al., 2023) in service encounters. For example, an agency may require that everyone complete a form to gain access. Some individuals may experience this requirement as more burdensome than others. Additionally, some individuals may encounter more frequent burdens because they seek access to means-tested programmes with complex and time-consuming eligibility procedures.
Administrative burdens, termed ‘policymaking by other means’ (Herd and Moynihan, 2018; Moynihan et al., 2016), can effectively limit individuals from accessing benefits, even if they are legally entitled, or otherwise eligible, to receive those benefits (Moynihan et al., 2016). This explains variations in take-up rates across safety net programmes: more burdensome programmes have lower take-up rates than those that place fewer burdens on individuals. It also suggests opportunities to remedy poor take-up by redesigning enrolment and eligibility procedures. For example, Medicaid take-up in Wisconsin increased when administrative burdens were shifted from individuals to the state through auto-enrolment, simplification of forms, and state verification of eligibility information (Herd et al., 2013). Similarly, analysis of longitudinal data found that simplifying enrolment procedures improved Medicaid take-up across all 50 states. Notably, increased take-up through ‘administrative easing’ was independent of ACA changes in Medicaid income thresholds (Fox et al., 2020).
My analysis of eligibility enactments through income thresholds partially overlaps with theories of street-level bureaucrats and administrative burdens. I share an understanding that what agencies and frontline workers do is decisive for who can access benefits. However, both these theories assume eligibility as a status that pertains to some individuals, and not to others. For analysts of street-level bureaucrats, the concern is how to ensure that ‘potentially eligible’ individuals can access benefits (Brodkin et al., 2005). For analysts of administrative burdens, reducing or shifting burdens may enable more ‘already-eligible’ individuals to enrol in programmes and receive benefits.
In contrast, I emphasise doing eligibility rather than being eligible. The two are clearly interconnected: how eligibility is done determines who becomes eligible. The important distinction in my conceptualisation of eligibility is that individuals become eligible, rather than potentially or already are eligible. Eligibility is thus not a pre-existing status; it emerges through organisational practices. And when these practices change, who becomes eligible changes as well.
We could envision eligibility as a doorway that enables, or impedes, passage into services. Latour (1994) wrote about problems with door openings and closings. Passage through the door depends not only on whether it is open or shut – in other words, whether one fits or does not fit into a category of eligibility – but rather how the door is (metaphorically) held open or closed as someone approaches, and whether people carrying packages (again metaphorically) are facilitated or hindered in trying to pass through. Different eligibility enactments may not necessarily make it possible for more people to pass through, but perhaps different kinds of people.
Income thresholds serve as one form of ‘gatekeeping’ mechanism to control access to services. Gatekeeping mechanisms not only determine who gets access, but also how the gatekeeping process is perceived. Bella's exclusion from Medi-Cal coverage remained incomprehensible. She did not understand why her income was low enough to qualify for one programme, but too high for another; neither did she understand her rights to appeal her Medi-Cal denial. As Lipsky (1984) pointed out, most administrative organisations have processes for appealing gatekeeper decisions although appeal opportunities are not well known to service applicants. This not only discourages applicants’ participation in ‘fair hearings’ (Lipsky, 1984: 15), but also hides decision-making procedures from view. Organisational gatekeeping mechanisms are generally not open to challenge through judicial processes (Rummery and Glendinning, 1999: 346). Nevertheless, individuals may feel denials are more reasonable if they understand the basis for decision-making.
There will always be some level of injustice at the income threshold, wherever that threshold lies. For Grace, being just under the threshold meant she had access to cancer treatment with no out-of-pocket costs; Bella, just over the threshold, incurred significant debt. If the threshold were set higher, Bella's income might have fallen below it. But there would always be someone else whose income was just over the threshold. I suggest it is not the threshold per se that matters for equity, but rather how the threshold is determined.
Addressing eligibility as process, rather than population subgroup, enables different organisational practices to emerge. Examples of such practices include using net income instead of gross income, or shifting the timing of when income is assessed for programme eligibility. Bella's income might have fallen under the threshold for Medi-Cal if it had been assessed after she started treatment, and not before. Since she was unable to work during her treatment, she not only lost income but also incurred high out-of-pocket expenses. This is precisely the rationale for thresholds based on income minus expenses or negative net income, as sometimes used by nonprofits. The more common strategy is simply to raise threshold levels, for example, the increased Medicaid threshold under the ACA. But raising thresholds does not change how income is calculated to account for precipitous income loss during serious illness, especially for those already economically vulnerable.
Changes in organisational practices affect both equitable service provision and resource limitations. Organisational practices can, and should, be evaluated for how well they achieve this balance. For example, requiring more detailed income and expense documentation may identify, and make eligible, a broader range of individuals with financial need. But it also creates administrative burdens, both for service applicants and for the organisational workers who process those applications. It takes applicants longer to gather the required documents, but also takes organisations longer to review and evaluate those documents. With fixed staffing resources, either fewer applicants will be processed or applications will be given less scrutiny.
Theory on street-level bureaucrats helps explain how eligibility is enacted within a context of limited resources, but does not address how to improve equity in service provision. Theory on administrative burdens suggests mechanisms to increase programme take-up and thus improve equity, but does not address what happens when take-up exceeds available resources. Eligibility enactments serve as the fulcrum between organisations and applicants, between resource availability and demand. As an antidote to ‘policy by other means’, focusing on organisational practices opens up a new arena for intentional policymaking.
Conclusion
Understanding how processes of service delivery actually work is as important as identifying who the intended policy beneficiaries should be. While disparities research encourages ever-narrowing definitions of subpopulations to target policy interventions more effectively, I focus instead on service delivery processes and how these processes make personal attributes such as income relevant for access. Shifting the analytic focus from categories (of individuals) to processes (what individuals are doing) has implications for how we think about disparities.
From an individual perspective, eligibility requirements are often perceived as onerous gatekeepers that prevent certain categories of individuals from accessing services. Re-conceptualising eligibility as enacted through practices enables us to examine the extent to which particular enactments contribute – wittingly or unwittingly – to furthering equity or to entrenching disparities. Disparities, according to this way of thinking, describe how individuals become disadvantaged through eligibility enactments, and not a category of disadvantaged individual per se.
From an organisational perspective, this suggests some service exclusions that result in disparities may be remedied through tinkering with eligibility procedures. Redefining disparities in terms of processes, rather than categories of individuals, provides new insights into how disparities may be produced and reproduced through ordinary work practices such as intake procedures or calculations of income thresholds. Identifying these practices can facilitate interventions to enhance equity in cancer survivorship care as well as many other forms of healthcare and social service delivery.
Footnotes
Acknowledgements
Data collection and analysis were conducted at the University of California, Irvine with additional data analysis at the University of California, Riverside. I thank Mary Devereaux, Martha Feldman, Kaaryn Gustafson, and Mike Rowe for their thoughtful comments on previous drafts; Miriam Bender, Martha Feldman, Olga Petrovskaya, and Mike Rowe for the ongoing conversations that deeply inform my thinking; and all the interview participants who generously shared their experiences.
Funding
This research was supported by the National Cancer Institute of the National Institutes of Health under Award #F31CA192478. The content is solely the author's responsibility and does not necessarily represent the official views of the National Institutes of Health.
Notes
Author biography
Address: School of Public Policy, University of California, 4133 INTS, 900 University Avenue, Riverside, CA 92521, USA
Email: