
Abstract
In 2017, Donald Trump signed the Protecting Life in Global Health Assistance (PLGHA), thereby reinstating the Global Gag Rule. The policy restricted all United States foreign funding from abortion-related activities. Little research reports the responses of recipients of this bilateral assistance. The study documents the South African government's responses to the PLGHA. We accessed Hansard parliamentary debates, interviewed four parliamentarians alongside one government official, and reviewed a USAID-funded initiative developed while the policy was in effect. We analysed the data using interpretive content analysis through a global social policy and gendered coloniality lens. Our research documents silence, ignorance, avoidance, and possible over-interpretation of the PLGHA within the South African government. The colonialist politics of global redistribution created the grounds for gendered regulation, resulting in a fundamental undermining of reproductive rights. Ironically, the solution – advocacy and parliamentarian briefing regarding sexual and reproductive issues – is generally led by civil society, the bodies weakened by the PLGHA.
Background
On 23 January 2017, former United States President Donald Trump signed a presidential memorandum called Protecting Life in Global Health Assistance (PLGHA). The PLGHA reinstated the Mexico City Policy (also known as the Global Gag Rule (GGR)), which was first instituted in 1984 during Ronald Reagan's term (Van der Meulen Rodgers, 2018). Since its inception, the GGR has been rescinded by Democrat presidents (most recently by President Biden) and re-instituted by Republican presidents. The PLGHA prohibited foreign NGOs that receive US global health assistance funds from providing, advocating for, counselling on, or referring for abortion services as a method of family planning. The policy also expanded on previous versions to include all US Global Health (e.g., HIV/AIDS, Tuberculosis), Department of Health and Human Services, and Department of Defense funding, increasing its coverage from approximately $575 million to approximately $9.1 billion (Change, 2021). While the Helms Amendment, passed in 1973, states that no foreign assistance funds may be used for the performance of abortion for family planning or to motivate any person to practice abortions, the PLGHA also banned non-governmental organisations (NGOs) who received US government funds from using their own funds for any of the activities covered in the PLGHA (providing, advocating for, counselling on, or referring for abortion services as a method of family planning) (Van der Meulen Rodgers, 2018).
The various iterations of the GGR are entrenched in US politics, particularly domestic struggles between Republicans and Democrats (Crane and Dusenberry, 2004). These political battles spill over into the politics of US aid beneficiary countries. Through the restrictions placed on the use of funds, global health assistance is transformed from a positive means for change to an intrusive donor/recipient relation. Hence, scholars have dubbed the policy as imperialist, a form of neo-colonialism (Lane et al., 2021), or 'America's deadly export' (Filipovic, 2017).
The reinstatement of the GGR by Republican presidents has been linked to surges in complications from backstreet abortions, increases in abortion rates and maternal mortality, weakened HIV interventions, health facility closures, and reductions and/or stockouts in sexual and reproductive health commodities (Bingenheimer and Skuster, 2017; Mavodza et al., 2019; Schaaf et al., 2019). A study from Nepal, which has liberal laws similar to South Africa's, illustrated how the PLGHA slowed or reversed the progress made by NGOs working collaboratively with their Ministry of Health (Tamang et al., 2020).
Given the political and health systems implications of the PLGHA, the question arises as to how the governments of recipient countries have responded. Research in Nepal (Puri et al., 2020) reported a lack of discussion in Parliament despite concern about the policy's effects by the two parliamentarians interviewed. In Malawi, inaction in terms of decriminalising abortion through the enactment of the Termination of Pregnancy Bill was reportedly fuelled by fears of US government funding loss (Centre for Health and Gender Equity, 2020). Similarly, in Zimbabwe, the US government's policies were reportedly used to excuse the Zimbabwean government's failure to update its abortion legislation (FosFeminista, 2022). Indirect effects of previous versions of the GGR on governments’ responses include the inability of NGOs to collate evidence-based data on abortion, which can inform policy- and law-makers (Seevers, 2006).
In this study, we use South Africa as a case study of recipient countries’ government responses to PLGHA. We review debates about the PLGHA in Parliament, insights from parliamentarians and a government employee, and a government initiative funded by US Agency for International Development (USAID). As such, we view debates and views from the legislative branch of government, and present evidence from an initiative of the executive branch of government.
South Africa provides a pertinent case study because the United States Government (USG), through USAID and the President's Emergency Plan for AIDS Relief (PEPFAR), contributes significant funds to family planning and HIV programmes (Singh and Karim, 2017). Indeed, in 2020, prior to the PLGHA being rescinded by Biden, South Africa received $466.7M in US government aid, $462.7M of which was from PEPFAR (US Foreign Assistance, 2022). An interrogation of the South African government's response is also important since the PLGHA contradicts the country's legislation.
In South Africa's transformation from apartheid to post-apartheid, equitable health access was key to redressing the gross race-based violations of apartheid. This was achieved, inter alia, through entrenching health access as a Constitutional right and enacting various pieces of legislation to realise this access (Eyles et al., 2015). Encompassed broadly within this drive for access was legislative change around abortions through the enactment of the Choice in Termination of Pregnancy Act (Act no.92 of 1996 – henceforth CTOP Act) (Republic of South Africa, 1996). The CTOP Act permits abortion on request, including from minors, within the first 12 weeks of gestation and subsequently under various conditions, including socio-economic grounds. An important element of the legislation is that medical practitioners must inform women of their rights under the CTOP Act should they request a termination of pregnancy. This means that health service providers employed by NGOs accepting the conditionalities of PLGHA would, strictly speaking, be breaking the law should they not provide such information. The PLGHA did stipulate that healthcare providers have an 'affirmative duty' under local law to provide counselling and referral for abortion, meaning that compliance would not be seen as a violation of the policy. Despite this, a general lack of knowledge or misunderstandings of the PLGHA led to many NGOs and providers being unaware of this exception (Du Plessis et al., 2019).
While the CTOP Act is heralded as an exemplary piece of legislative reform, challenges remain. As outlined in a review (Macleod et al., 2016), many women do not receive the abortion care they request, there are frequent delays in the delivery of services and long queues at facilities, a minority of trained health service providers actually provide the service, services in functioning facilities are fragmented, and many health service providers and facility managers cite personal objections to abortion on the grounds of conscience. NGOs have often filled the service gaps, including information dissemination, training of providers, and advocacy (Du Plessis et al., 2020).
Methods
Theoretical framework
The US is the world's largest source of global health financing and the widest implementer of global health programmes (Singh and Karim, 2017). The dynamics of such global interchanges have been taken up within global social policy debates. Deacon (2005) conceptualizes global social policy as global redistribution, regulation, and rights. Global redistribution refers to social transfer, often through funding mechanisms (in this case, US government funding to health and other programmes in South Africa). This is linked to global social regulation, which, on the positive side, is provided by agreed-upon compacts and standards, but which may also be tied to globalized (e.g., neocolonialist) power relations. Global social policy should support global social rights – in particular, the advancement of the UN agenda of social rights – but can also be used to undermine them.
In this paper, we weave the triangulation of redistribution, regulation and rights into our analysis using an added lens of the gendered coloniality of power. 'Coloniality' refers to an overarching framework that continues to reflect current power relations between the global North and South, as well as the diverse relationships within the various geographies of the global South and North (Maldonado-Torres, 2007). Put differently by Ndlovu-Gatsheni (2013: 8), the coloniality of power refers to 'continuities of colonial mentalities, psychologies and worldview into the so-called ‘postcolonial era’ and highlights the social hierarchical relationships of exploitation and domination'.
Coloniality is deeply interwoven by gendered power relations. For decolonial feminists, gender is a mechanism of (neo)colonial domination over ‘non-western’ racialized bodies (Mendoza, 2015). Understanding gendered coloniality, according to Lugones (2010: 746), is 'to enact a critique of racialised, colonial, and capitalist heterosexualist gender oppression'. Such critique serves to deconstruct colonialized and patriarchal power/knowledge nexuses between the global South and the global North, as well as within these broad regions (Du Plessis et al., 2020).
Sampling
The aim of this study was to document South African parliamentary and government responses to Trump's PLGHA. To do this, we accessed information from three sources: (1) Hansard records of parliamentary debates; (2) Interviews with four parliamentarians and one National Department of Health (NDoH) employee; and (3) A government initiative on comprehensive sexuality education (CSE).
For Part 1, Hansard records were searched from 9 February 2017, the first parliamentary sitting after the PLGHA was instituted, to 8 June 2022, the latest available Hansard report at the time of write-up. Purposive sampling was used to sample the parliamentarians for Part 2. Characteristics included that participants be (1) members of Parliament, (2) work in the areas of health or gender, and (3) represent major parties. Four interviews were conducted: two with members of the Democratic Alliance (DA), the official opposition, and one each from the Economic Freedom Fighters (EFF) and the African Christian Democratic Party (ACDP).
Despite many attempts, we were unable to conduct an interview directly with any member of Parliament representing the ruling party, the African National Congress (ANC). We were referred by members to each other and eventually to a high-ranking government official in the National Department of Health (NDoH) who works in close proximity with parliamentarians on abortion. We include this interview in the study and comment on the significance of this referral in the analysis.
The ANC, DA and EFF are, in that order, the three largest parties in South Africa. The ANC is a social-democratic party and holds the majority of seats in Parliament. The DA is the official opposition and is a centrist, liberal party. The EFF is a leftist, pan-Africanist party. The ACDP, a socially conservative Christian party, is the fifth largest in Parliament. We decided to interview an ACDP representative because, of all the parties, they have actively challenged existing abortion laws. No other party opposes the CTOP Act.
In the third part, we outline evidence of the South African government possibly conceding to the demands of the PLGHA. In 2015, the South African government launched its Adolescent Sexual and Reproductive Health and Rights Strategy Framework 2014–2019 (Department of Social Development, 2014). We home in on Priority 2 of this framework – Developing Innovative Approaches to Comprehensive SRHR Information, Education and Counselling for Adolescents, in particular the contents of the Scripted Lesson Plans that were devised as part of this. We were alerted to this project through research we previously conducted on the impact of the PLGHA on NGOs (Masuko et al., 2020).
Data collection and analysis
We used the following keywords to access data in Hansard: abortion, termination of pregnancy, Choice on Termination of Pregnancy Act, CTOP Act, Global Gag Rule, GGR, Protecting Life in Global Health Assistance, PLGHA, Mexico City Policy, maternal health, maternity, pregnancy, reproduction, reproductive health. Using a simple frequency count, we collated the number of sittings and the number of times these words appeared. We anticipated conducting a content analysis on the text that mentioned the GGR, Mexico City Policy or PLGHA, but as none was found, this was not necessary.
The interview data consist of five semi-structured interviews conducted virtually or telephonically by the first author from August 2020, when the PLGHA was in full force and its effects had already been felt, to October 2021, a few months after PLGHA was rescinded by Biden. Interview questions centred on their knowledge of the PLGHA, their memory of parliamentary discussions on the matter, their reactions to the PLGHA, and their understanding of government responsibility regarding the PLGHA. All interviews were recorded and transcribed verbatim by the first author.
For the Scripted Lesson Plans component, we draw on some information from the above interviews, an interview conducted previously by our unit in an assessment of the impact of the PLGHA on the NGO sector in South Africa (Masuko et al., 2020), and an analysis of the Scripted Lesson Plans that were developed in the course of the implementation of the Strategy Framework mentioned above.
These data (for Parts 2 and 3) were analysed using interpretive content analysis. Interpretive content analysis focuses on both manifest content – characteristics that are readily identifiable in the data – and latent content – characteristics that are not overtly evident but are implicit or implied across the data (Drisko and Maschi, 2016). The aim of interpretive content analysis is to be both systematic and transparent in the tradition of content analyses yet draw on a more qualitative ontology. The initial codebook was drafted by the first author. The data were collaboratively coded by the authors of the article during a series of workshops.
Ethical issues/statement
Ethics clearance was received through the Rhodes University Ethics Standards Committee (under ethics clearance approval number: 2020-1604-3603. Parliamentarians’ contact details, specifically those within the Health, Women, Youth and Persons with Disabilities and Social Development committees, were sourced through the South African Parliament's website. A letter was then sent to the relevant member's personal assistant or directly to them if their details were listed on the website. Full information about the study, what participation would entail, as well as the benefits of partaking, were included in the letter. Given the public nature of Parliament, it is not possible to hide the participants’ identities completely. We, nevertheless, use pseudonyms to protect participants to the extent that this is possible. Interviewees were provided with a document describing the PLGHA policy (Rios, 2019).
Findings
Hansard
Table 1 outlines the number of times the various keywords searched for were mentioned in Parliament between 9 February 2017 and 8 June 2022. Remarkably, the PLGHA, the GGR (or equivalent) is mentioned only once in the entire period. In contrast, abortion or termination of pregnancy is mentioned 198 times, the CTOP Act 18 times, maternal health or maternity 148 times, pregnancy 471 times, and reproductive health or reproduction 107 times. This demonstrates a parliament interested in debating reproductive health issues. Thus, the lack of mention of the PLGHA cannot be put down to a lack of interest in reproductive health issues in Parliament.
Mentions of GGR or the equivalent compared to other reproductive health issues in Hansard 9 February 2017–8 June 2022.
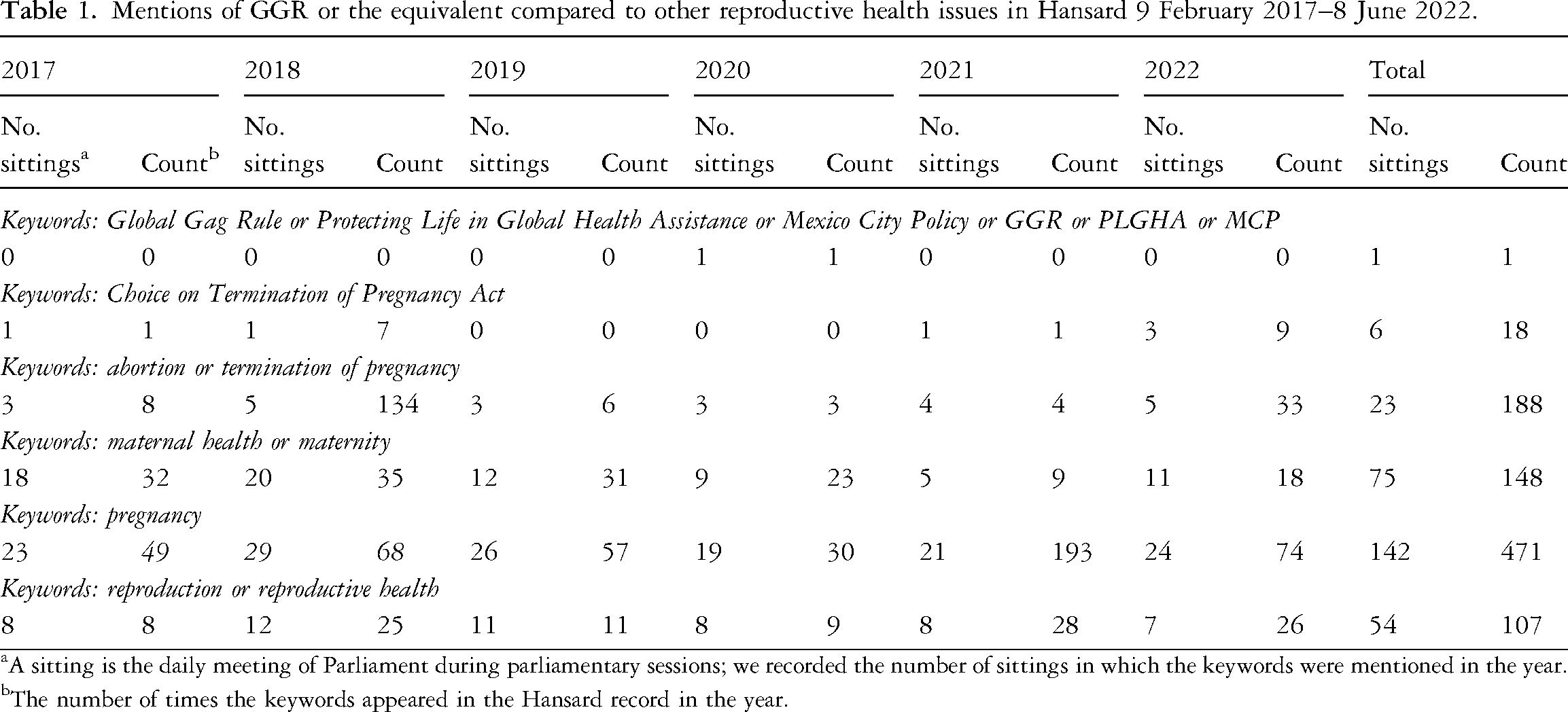
A sitting is the daily meeting of Parliament during parliamentary sessions; we recorded the number of sittings in which the keywords were mentioned in the year.
The number of times the keywords appeared in the Hansard record in the year.
The only brief mention of the PLGHA was on 10 November 2020 by a member following our interview. In other words, the interview alerted them to the issue, which they then raised in Parliament. The member moved to have the PLGHA and its implications debated in Parliament. Until the last publicised sitting at the time of writing (June 2022), the debate mentioned had not occurred. There is, thus, silence in the legislative arm of government concerning the effects of the PLGHA.
Parliamentary (or proxy) interviews
As noted in the method section, we were unable to access a member of the ANC to interview. We were not denied an interview outright. Instead, the members we approached referred us to each other and, after repeated requests for an interview, to a senior official in the NDoH. We interpret this in two ways. Firstly, it demonstrates a blurring of lines between state and party, a concern raised repeatedly in the media (Hoffman, 2021). Secondly, the responses we received gave us a sense that members were avoiding the issue, which was potentially politically sensitive.
Knowledge of the PLGHA
Parliamentarians were asked where they heard about the PLGHA, and what they know about it. Three of the participants were completely ignorant of the PLGHA before the interview was scheduled (e.g., 'I had no idea' (Ludidi, DA); 'I’m not so sure about that policy' (Khanyile, NDoH)). Possibly feeling judged, Zoë (ACDP) explained her ignorance through an appeal to being busy ('If you serve on a number of portfolios, you need to prioritise your time and attention to very specific things' (Zoë, ACDP).
Receiving the invitation to participate in the interview resulted in participants engaging with material regarding the PLGHA.
[T]his conversation started with you, you know, forced me to pay attention … then, of course, you brought it into soft focus when you asked for an interview. (Zoë, ACDP)
I mean, what I read recently, before our interview, was the document that you sent. (Ludidi, DA).
Other than the information sent to the participants by the interviewer, one participant (Khanyile, NDoH) vaguely mentioned 'the media and in some NGO meeting platform' civil society.
Changa (EFF) was the only interviewee who had direct knowledge of the PLGHA prior to the interview.
I can’t note when exactly I got to know about it [PLGHA signed by Trump] … Probably immediately … a more direct confrontation happened when I worked with [NGO] in 2018 … besides it just being a social media issue and social media outrage. (Changa, EFF)
Unlike the participants above, Changa's knowledge came from the media and experiences during previous employment at an NGO. Of concern, thus, is that none mentioned political briefings or serious engagement with the policy or with research concerning PLGHA's impact. While it is easy to lay blame on individual participants for their ignorance (something that Zoë anticipated with her response around being busy), of real concern is the lack of systemic engagement with the legislative arm of government concerning the provisions and implications of the PLGHA. This meant that these members were unaware of how the politics of redistribution were being used by the centre (the US) to regulate not only the actions of grant recipients but also pregnant people's right to bodily integrity.
Reactions to the PLGHA
In introducing ourselves to the participants, we sent them a copy of a report on the effects of the PLGHA on NGOs in four countries – Kenya, Nigeria, South Africa and Nepal (Rios, 2019). As such, where they did not previously know about the PLGHA, they now had some background.
As would be expected from parliamentarians from different parties, there was a range of reactions to the PLGHA. What is of interest here, however, is how each participant spoke to the politics of regulation in their responses. It [PLGHA]limits choice of a woman's body, and at the end of the day, we can’t allow politics to come in between lifesaving services and measures. And a woman and her right to access of information and her right to access to good quality healthcare. And what these policies and these politicians do, especially when you’re in a room full of men, and they try and control our choices and our bodies. This is the sort of policies that we have, and the symptom is that women are dying. (Jacobs, DA).
It was just an issue of really marginalizing and othering African countries and othering poorer Third World countries. And cementing the US supremacy … It's classism, it's racism and it's xenophobia, right? And it's misogyny. (Changa, EFF)
This policy is actually affecting the poor of the poorest … because sometimes those who do have money, you know, they can access some services in a private sector, because they do have money, they have got medical aid and all of that. And then, as anyone, if they want any information, they can go to that private sector. (Khanyile, NDoH)
These responses are, to a great extent, in line with the individuals’ party politics. The DA parliamentarian's liberalism is on show, with the language of rights and choice. The EFF is a self-styled anti-capitalist and anti-imperialist movement, which explains their focus on global power dynamics. The health department employee, on the other hand, is less concerned with political rhetoric and more focused on the practical implications of the policy on the ground.
Using the language of rights, choice, and access, Jacobs (DA) stressed how gendered dynamics can result in negative consequences for women, including death. Changa (EFF) was more focused on the issue of US imperialism but also referred to intersectional power relations along the lines of race, class, nationality, and gender. Khanyile (NDoH) was concerned with the practical effects of the policy that will disadvantage people already marginalized by poverty. Thus, despite their party-line differences, each referred to how, in this instance, the politics of global redistribution (USA global health assistance) is deeply intertwined with an intersectional politics of regulation that feeds off and is embedded in gendered coloniality.
Zoë (ACDP), however, constructed the policy as liberating a constrained voice, which she identifies as pro-life.
And in this case, from what I read about the policy, it is about protecting the rights of the unborn or the sanctity of life …. The policy rather, you know, enraged to the left [rather] than to the right. You know, first of all, don’t you believe in the sanctity of life? [These ideas] are not featured on television programmes and they certainly don’t get platforms to shout from the roof-top their views. It's a suppressed voice I think, and it has been suppressed. (Zoë, ACDP)
Zoë (ACDP) declared herself upfront as pro-life. The ACDP, as a party, is anti-abortion and has drawn on various popular anti-abortion tactics to persuade its audience, including moralising abortion. In line with this position, Zoë argued that the pro-life voice is 'suppressed' in South Africa, which the PLGHA helps to relieve. The regulation, thus, that the PLGHA redistribution enables, according to Zoë, is the freeing of an internally (to South Africa) suppressed pro-life voice.
There was also a general frustration with making an enemy of the US funding system, knowing how dependent organisations are on it.
And I remember there was a lot of pushback, but even the pushback had to be silenced because now we are depending on these people to fund our programmes. (Changa, EFF)
I have always kind of understood that foreign aid obviously has conditionalities attached to it, so no country can just give aid to another country without attaching conditions. But I’ve always understood that as a country, particularly in South Africa, that we would always reject conditions which would be in contravention to what is protected within our Constitution. … And of course, we don’t have infinite resources, so there is that; there is a balance between accepting money that comes with conditions that are regressive, but also versus needing the money itself because NGOs also do various amounts of work that benefits South Africans. (Ludidi, DA)
It creates contestation between the collaboration of NGOs, and also distrust between the collaboration of NGOs. So, now how do we collaborate effectively to save people's lives if we can’t even have a conversation about it? (Jacobs, DA)
Speaking from their experience as a former employee of an NGO, Changa (EFF) noted how the dynamic that enables those involved in redistribution to enforce particular regulations inevitably leads to silence amongst recipients when the stipulations counter their autonomy. The DA parliamentarians also identify this tendency towards silence and the frustration of this catch-22 situation in which Global South countries find themselves. Ludidi (DA) suggested that South Africa is a strong Global South state that can push back against foreign conditionalities but then noted how resource poverty sets the scene for redistribution to be linked to regulatory silence. Jacobs homes in on the tensions created between NGOs that accepted and those that refused USG money. These tensions led, they rightly point out, to strained or no conversation between NGOs. Instead of dissension being focused on undermining or contesting the gendered coloniality of the PLGHA and its stipulations, dissension is turned inwards, undermining the very organisations foreign aid is meant to support.
Parliamentary engagement
Participants were asked about Parliament's engagement with the PLGHA.
No, there was no discussion, but it was brought up as part of a debate … not as debating as a whole in the house, but as part of a statement. So that's the only mention of it in a statement. (Zoë, ACDP)
The past year has been really in the space filled with discussions in Parliament around the national health insurance … So, that is my concern, that at the moment, the conversation [in Parliament] is around universal healthcare. (Ludidi, DA)
Our participants confirmed our Hansard findings, viz., that there has been no direct discussion of the PLGHA in Parliament. Ludidi (DA), who was interviewed when the PLGHA was still in place, provided a reason for the lack of discussion: they suggest that this may be because parliamentary time has been dominated by the National Health Insurance (NHI) bill.
There was some discussion about what bringing the PLGHA up in Parliament would mean. For Jacobs (DA), they could anticipate divergent views, with the consequence being that a conservative agenda is given floor space.
I could imagine that it [PLGHA] would limit the amount of debate and I can imagine that it would embolden those conservative parliamentarians that we have in South Africa … and I would hope that there are parliamentarians in our National Assembly that will stand up against such policies, especially given that South Africa is a constitutional democracy. (Jacobs, DA)
In line with this, Zoë (ACDP), a conservative parliamentarian, argued that they would push for the debate to cohere around the moral status of abortion.
Interviewer: Do you think it is an issue that should be discussed in Parliament?/ It depends on what basis. Yeah. You know, on what basis are we going to, because in the end it's actually about abortion services … and I think we shouldn’t hide the fact that it is about ideology; it is about how you view life, and whether you view the life of the unborn to be as precious as the life of the mother carrying the child. (Zoë, ACDP)
Obviously, in parliamentary debates, differences of opinion are to be expected. Jacobs argues that debate about the PLGHA may be used by conservative parliamentarians to bolster their anti-abortion position, which Zoë's response appears to support. While this is a possibility, what these extracts highlight is that parliamentarians of parties that are not actively against the constitutional right to abortion may be wary of the consequences of opening a debate on abortion. This fear bolsters the politics of regulation in which silence is imposed externally but also enacted (from fear) internally.
Government responsibilities and the PLGHA
Participants were asked to reflect on the government's role and responsibilities in reacting to or countering the impact of the PLGHA. They spoke about the lack of South African funding and inefficiencies in the system.
We as the DA, what we need to be doing is ensuring that more funding comes from the South African government so that our organisations are not necessarily dependent on foreign aid that comes with so many of the conditions … [But] We don’t don’t have the financial resources. In fact, we have financial mismanagement, and so money goes where it's not supposed to go. (Jacobs, DA)
You know as government, we can’t, we can’t do it alone. We need partners. Yeah, to support us, so that partners, also, they are our soldiers at the implementation phase. (Khanyile, NDoH)
These parliamentarians confess that financial and human resource constraints underpin the government's reliance on external funding and partners. While this positive rhetoric about the need for internal funding and partners is useful, it is interesting to note that none of the parliamentarians recognised their own silence in Parliament or ignorance of the policy as a contributing factor.
The important role that NGOs and civil society, in general, play in the democratic process was noted, and there was a fear of the outcome of a weakened civil society by the main opposition parties.
My big concern in South Africa is that the [Global] Gag Rule can hamper advocacy, and that is a big problem because if we hamper advocacy in that sense, then we are not going to have organisations that are pushing government to do better, to do more, holding government accountable. (Ludidi, DA)
I think it's exactly what it's called – it gags us. It makes it impossible for those who are arguing for pro-choice to be able to speak about it and advocate for it. (Jacobs, DA)
Because now, we have very close links with NGOs, who then give us information on what's happening, who assist us with oversight. And all those things are now all of a sudden, the one, one of the most important aspects of ensuring the sex, sexual [and] reproductive health rights are a reality is suddenly taken away overnight. (Changa, EFF)
South African NGOs play a vital role not only in service delivery but also in advocacy and accountability campaigns. For example, as Changa (EFF) went on to describe, the Treatment Action Campaign forced the government through court action to roll out anti-retroviral medication for people living with HIV. The regulations specified in the PLGHA effectively silence or gag NGOs accepting the funding and bootstrap those who refuse to sign, with knock on effects in terms of the defense of pregnant people's rights to bodily integrity and to access abortion in line with the country's legislation.
Despite the negativity regarding government accountability, the two DA members mentioned the Constitution repeatedly to emphasise its importance in countering negative politicking.
Yeah, the rights of the individual and with the right of the individual means the right to the autonomy of my body. And it's enshrined in the Constitution, so I can’t imagine that any other right-conservative political party can influence South African politics. I mean, we are so progressive when it comes to things like this. And we cannot go, we can’t take two steps back just to be liked by a world power. We need to stick to core values and our principles and keep pushing forward. (Jacobs, DA)
And that is one of the things that is beautiful about the South African Constitution. Because at any given time, whoever is contesting an election, nobody is saying 'We are contesting elections and if we win, we will make sure that abortions are clamped down on or make sure that we will never afford sex workers’ real work status'. So, there are certain unalienable rights that are contained within the Constitution. (Ludidi, DA)
The Constitution is held up here as a document that serves to hold South African politics together and to withstand outside influence. These members talk to the ideal of the progressive rights-based South African Constitution trumping the politics of redistribution and regulation. Ironically, of course, such a situation cannot arise unless there is basic knowledge of the conditionalities of foreign aid and debates thereof within the legislative arm of government.
Government initiatives: The case of the scripted lesson plans
A key element of the PLGHA was that the restrictions did not apply to US global health assistance funds provided to recipient governments. Nevertheless, pressure may have been exerted on recipient governments to comply, or there may be a confluence of interests between some in government and the specifications of the PLGHA. This seems to be the case with the national Scripted Lesson Plans for Comprehensive Sexuality Education released in late 2019 (for more information, see https://www.gov.za/speeches/scripted-lesson-plans-13-nov-2019-0000). The lesson plans – which were funded by USAID and drafted by a task force of individuals from various sectors involved in adolescent sexual and reproductive health (including the Department of Basic Education) – were developed with the idea of giving more guidance to teachers on teaching comprehensive sexuality education within the Life Orientation curriculum.
The following is a quote from a participant in previous research conducted by our unit on the effects of the PLGHA in South Africa (Rios, 2019).
The scripted lesson plans are now out. We did a very careful search through all of the scripted lesson plans – both the learner manuals and the teacher manuals – to see how abortion is dealt with in these. And what you land up with is abortion – yes – is mentioned, but very much in passing. It's never dealt with substantively on its own. So, there is no information of the CTOP Act and of people's rights under the CTOP Act. There's no information around, for example, avoiding illegal abortions and unsafe abortions, what would be expected if you were to go for an abortion, where you would go and what the process is. I appreciate that some teachers may find it a bit of a difficult topic to tackle, but nevertheless, it is the law. And so, with that in mind, I think it's a complete disservice to learners to not give them even just the factual information. (Director, SRHR unit)
The participant bemoans the fact that learners’ rights to information about legal stipulations regarding reproductive health are undermined through the CTOP Act not being provided adequate coverage in the Scripted Lesson Plans. The lack is confirmed in an analysis of the contents of the Scripted Lesson Plans by the NGO, Section 27 (Julia Chaskalson, personal communication, 10 August 2022). They found that abortion was not dealt with at any of the grade levels for which the Scripted Lesson Plans were developed. Abortion is mentioned only in the context of asserting that emergency contraception is not abortion. Given the fact that the CTOP Act enables minors to make autonomous decisions concerning the outcome of a pregnancy, depriving learners of their rights to basic information on their reproductive rights is a gender injustice. This silence will only exacerbate already low levels of knowledge amongst the youth concerning abortion (Macleod et al., 2014).
The participant goes on to posit a reason for this lack.
Now, of course, what do we see? These scripted lesson plans are funded by USAID, it's stated very clearly. But was this the USAID insisting that abortion doesn’t appear if they are going to provide the funding? Or was there simply a confluence of ideologies, I suppose, between the USAID and the Department of Basic Education? I don’t know. Because obviously PLGHA is not supposed to apply to governments. And what is worse is that we asked repeatedly in the Adolescent Sexual and Reproductive Health and Rights Strategy Framework workshops – that's a long name – we asked repeatedly when the Department of Basic Education spoke of drafting of these lesson plans whether information on abortion and the stipulations of the CTOP Act would appear. They simply would not answer, which made us suspicious about whether any proper information would appear, and, well, we were proven right. (Director, SRHR unit)
Here the Director raised a similar concern to the one expressed above: the silencing effect of global redistribution where funding clashes with a country's democratic laws. Government accountability – in the form of answering questions regarding actions – shifts from within country spaces (such as the workshops referred to by the Director) to answering to global funders.
Discussion
The impact of the PLGHA on NGOs has been well documented, with many who refused such aid having to retrench staff or close down, and those accepting aid having to re-write materials and re-orient interventions in line with the PLGHA regulations (Du Plessis et al., 2019; Rios, 2019). This paper highlights how conditionalities attached to foreign funding can have negative effects not only on NGOs and people's health and well-being, as highlighted in the introduction, but also on the recipient country's democratic processes. In essence, the politics of global redistribution in the form of US government foreign aid assistance has, through the PLGHA, created a politics of regulation that has undermined the reproductive rights of South African people so carefully won through the liberation struggle.
In this paper, we focus on some of the South African government's responses to the PLGHA. There was silence on the matter in legislative branch of government, parliament, with the only mention occurring after we interviewed the parliamentarians. Those parliamentarians we interviewed knew little about the PLGHA prior to the interviews. The only exception was one who had previously worked for an NGO. The parliamentarians from the ruling party, the ANC, did not speak to us, directing us instead to a government employee. As a result of our repeated attempts to elicit an interview, we interpreted this as avoidance and a slippage between state and party. This kind of avoidance is also evidenced in the failure of the Department of Basic Education to answer questions in the workshop referred to by the Director of a SRHR programme cited above.
Reactions to the PLGHA, based on the information we gave our interviewees, were mixed, with the minority ACDP party taking a pro-life approach that aligns with the PLGHA and the rest expressing dismay at the PLGHA being misogynist, racist, imperialist, and in contradiction with the South African Constitution. The government was positioned as able to escape criticism or calls for accountability through the weakening of the NGO sector. Accountability, thus, shifts from internal processes to external funders. The PLGHA was expressly not meant to apply to governments, and yet the extensive task of developing the Comprehensive Sexuality Education Scripted Lesson Plans across multiple grades, which was funded by USAID, neglected to mention abortion. Discussion of women's (including minors’) right to request abortion in the first trimester of abortion, and thereafter under particular conditions, is auspiciously absent from the Lesson Plans, rendering them thus non-comprehensive. The politics of global redistribution and regulation have thus undermined young people's right to knowledge about reproductive legislation.
Conclusions
The GGR, in its multiple forms, has been characterised as a neo-colonialist enterprise (Lane et al., 2021). In such a situation, the response of the governments of recipient countries is important. In this paper, we have shown how, in the case of South Africa, the latest version of the GGR – PLGHA was met with almost complete silence in Parliament, paired with ignorance on the part of parliamentarians, avoidance by the ruling party, and lack of mention of abortion in a government initiated comprehensive sexuality education project (Scripted Lesson Plans).
Conditions attached to foreign aid are often aimed at promoting democratic or economic reform, encouraging development or economic growth, inclusivity, or 'good governance' (Leftwich, 2007). The PLGHA, however, is not evidence-based, nor is it in line with the Constitution of South Africa or its abortion legislation. Rather, it is the export of conservative ideological positions so controversial and contested within the US itself that the policy is rescinded or reinstated every time a new president of a different political party is elected.
Gendered coloniality refers to ongoing social hierarchical relationships of domination. We have shown in this paper how the fact that the PLGHA attached gendered regulation to its mechanisms of global redistribution undermined or shut down democratic processes and accountability in South Africa and deprived young people of their basic right to knowledge about their full range of reproductive health rights.
The parliamentarians were inexcusably ignorant of an issue that affects millions of South Africans’ lives, undermines constitutionally mandated rights, and has a potentially significant effect on unsafe abortion. However, other factors are also in play. Members of the liberal opposition fear providing a platform in Parliament to those who are passionately anti-abortion and well-versed in anti-abortion rhetoric. Reliance on US government foreign funding for HIV programmes serves to hamstring the government's ability to oppose or address conditionalities (Rios, 2019).
This situation is supposed to be remedied by civil society, which is 'as much a core feature of democracy as are competitive elections' (Warren, 2011: 378). The PLGHA, as noted by participants in this research, systematically silences those who are meant to hold the state to account. Their ability to pressure politicians or government to be transparent and accountable regarding their responses to the conditionalities of foreign aid, particularly when such aid is in direct conflict with South African legislation and the Constitution, is limited.
The limitations of this study are that it provides a case study of one country only. While our inability to interview a parliamentary member of the ruling party provides some insight into political obfuscation around politically sensitive issues, it can also be viewed as a limitation. We were not able to access information on the ruling party's knowledge, reaction to or take on PLGHA.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is based on research supported by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation of South Africa (grant number 87582); and the International Women's Health Coalition.
Author biographies
Address: CSSR House, Rhodes University, P O Box 94, Makhanda, 6140, South Africa
Email: