
Abstract
The parents, especially mothers, of disabled children play a crucial role in coordinating care for their children. This article investigates families’ coordination work using qualitative accounts of the parents of disabled children in Norway. The theoretical concepts of the third shift, hidden work and a broad definition of care are applied. We present a typology of coordination work, consisting of writing, meetings, administration of services, learning, monitoring and emotional work. We describe three cases to show the nature and consequences of having to coordinate the everyday lives of disabled children. The findings show that coordination work is gendered, individualised and taken for granted in service provision. We argue that coordination work should be better recognised in social policy design for these families to provide adequate services and avoid reproducing social inequality.
Introduction
Caring for a disabled child often entails receiving multiple types of benefits and services. Thus, providing parental care requires the coordination and care management of the involved actors. How informal carers cope with coordination is an important aspect of the uptake of benefits and services. The research on uptake for families with disabled children suggests that uptake is lower than one could expect (Brekke et al., 2020; Finnvold, 2009; Vinck et al., 2019). Generous welfare states with expansive rights to receive benefits and services can demand work to gain access. However, although the literature identifies tackling the system as a central challenge (Green, 2007; McLaughlin, 2019), it is not addressed as a type of care, and the content of the work remains underexplored. Adopting a broad definition of care (Fisher and Tronto, 1990) and identifying coordination as a type of hidden work (Wadel, 1979), this article seeks to describe and discuss coordination work as a necessary and demanding part of the care system surrounding the child.
This article considers the parents (particularly mothers) of disabled children in Norway and how they experience coordination and administrative care work for their children. We use qualitative data from a research project investigating how families with disabled children experience the provision of services and benefits. We ask the following: What is coordination work, and how is it experienced by the parents of disabled children? How can we understand coordination as a type of care?
Care work of parents of disabled children
The parents of disabled children deal with a complex system of health and welfare services. There are multiple services and benefits available to families with disabled children in modern welfare states, such as support, respite, child-minding and emergency support (Tétreault et al., 2014). These services provide informational, legal and financial support, rest and relief, the ability to leave the home to work and financial aid and accommodation during unusual and unplanned situations. Although these benefits and services are in place to help with care, gaining access to them can be difficult. The literature reports the paradoxical finding that parents experience a hostile support system forcing them to battle for their rights (Green, 2007; Thomas, 2020). In the literature, parents emphasise this fight as the main contributor to their struggles; the families highlight how fighting with the providers of health care and social services to get adequate support is what they primarily find burdensome (McLaughlin, 2019).
Being the parent of a disabled child is associated with a weaker connection to the labour market, especially for women. Having a disabled or chronically sick child reduces mothers’ working hours, income and labour market participation while increasing long-term sickness absence (Brekke and Nadim, 2016; Reisel et al., 2020; Wondemu et al., 2022). Furthermore, parenting a disabled child reinforces social disadvantage in that reduced parental employment is especially prominent for single parents and parents with low educational qualifications (Vinck and Van Lancker, 2019). The disparate impact on women suggests that the intensified care work needed to provide for disabled children often becomes the mothers’ responsibility. Hence, it is important that research on families of disabled children remain sensitive to the gendered aspect of care (Traustadottir, 1991).
Our theoretical perspective is based on the definition of care provided by Fisher and Tronto (1990): ‘a species activity that includes everything that we do to maintain, continue and repair our world so that we can live in it as well as possible. That world includes our bodies, our selves, and our environment, all of which we seek to interweave in a complex, life-sustaining web’ (1990: 40). Tronto (2013) argues that this understanding goes beyond previous understandings of care as performed in a particular emotional state, as something done face to face or characterised by intimate caring. For example, she emphasises how this definition makes it possible to include both nurturant and non-nurturant caring and care going beyond the dyad of the caregiver and care receiver. We need to see how the care of disabled children rests on several actors that together constitute a care system. This care system involves both practical tasks and ‘ways of structuring and restructuring social relations’ (Daatland, 1983: 2). Care requires organisation, where the links between formal and informal care systems are established and managed. Playing a crucial role in managing this link, parents are the central informal carers of disabled children.
This article aims to highlight the coordinating work done primarily by women, which can be considered a form of hidden work (Wadel, 1979). The third shift—or mental load—is a useful concept for understanding hidden cognitive and administrative work done in families. Hochschild (1997) coined the term ‘third shift’ to describe the planning and organisation of family time that is needed for parents who must juggle their responsibilities in the first shift (paid work) and the second shift (childcare). The literature emphasises how the third shift refers to the responsibility for planning and organising family life and underscores that it falls disproportionally on women (Ericsson et al., 2021; Smeby, 2017). In this article, the third shift is understood as parent's cognitive and emotional work in planning, administrating and ensuring that their disabled child is receiving adequate care and support. The parents of disabled children have to do much more planning and administration than other parents. In a recent survey done by the Norwegian Health Directorate, the parents of disabled children reported using 19 h on average per week on administrative tasks (Norwegian Directorate of Health, 2021). Linking the third shift and Fisher and Tronto's definition of care, our article shows how the cognitive work of coordination is a type of care.
Coordination of services for disabled children in Norway
Representing one of the Scandinavian welfare state models, Norway has an advanced and active public welfare policy, which implies a significant public responsibility for benefits and services covering the entire population and its needs (Halvorsen and Hvinden, 2009; Kildal, 2013; Sandvin et al., 2020). This extended welfare model results in a high degree of social spending and low levels of poverty (Halvorsen et al., 2015). The Norwegian welfare policy is characterised by being service intensive (Anvik et al., 2020; Esping-Andersen, 1990), where responsibility for implementing welfare policy is decentralised down on the local, municipality level (Sandvin et al., 2020; Vike et al., 2016).
Families with disabled children must apply to the municipality for most of the relevant services and benefits, but some benefits are also assessed by the Norwegian Labour and Welfare Organization (NAV). The parents must apply for each benefit and service separately, such as personal assistants (PAs), transportation, respite and different types of income support. Because of this complex system, coordination is a demanding task. Coordinating services for disabled children has been a prioritised policy area for two decades (Kalleson et al., 2021). The main coordinating services provided to families of disabled children are an individual service plan, having an appointed municipal coordinator and having regular meetings with an interprofessional team of service providers.
Despite these legislative efforts, Norwegian families with disabled children do not receive help as intended, as concluded comprehensive audit done by the Office of the Auditor General of Norway (2021) stating that, to a large degree, families are left to coordinate the services on their own and spend a great amount of time communicating with different service providers, applying for help and documenting their needs. This gap between the expectation of a generous welfare state and actual help provided has been shown to create feelings of resentment because parents feel that their work is undervalued (Gundersen, 2012; Kvarme et al., 2016).
Methods
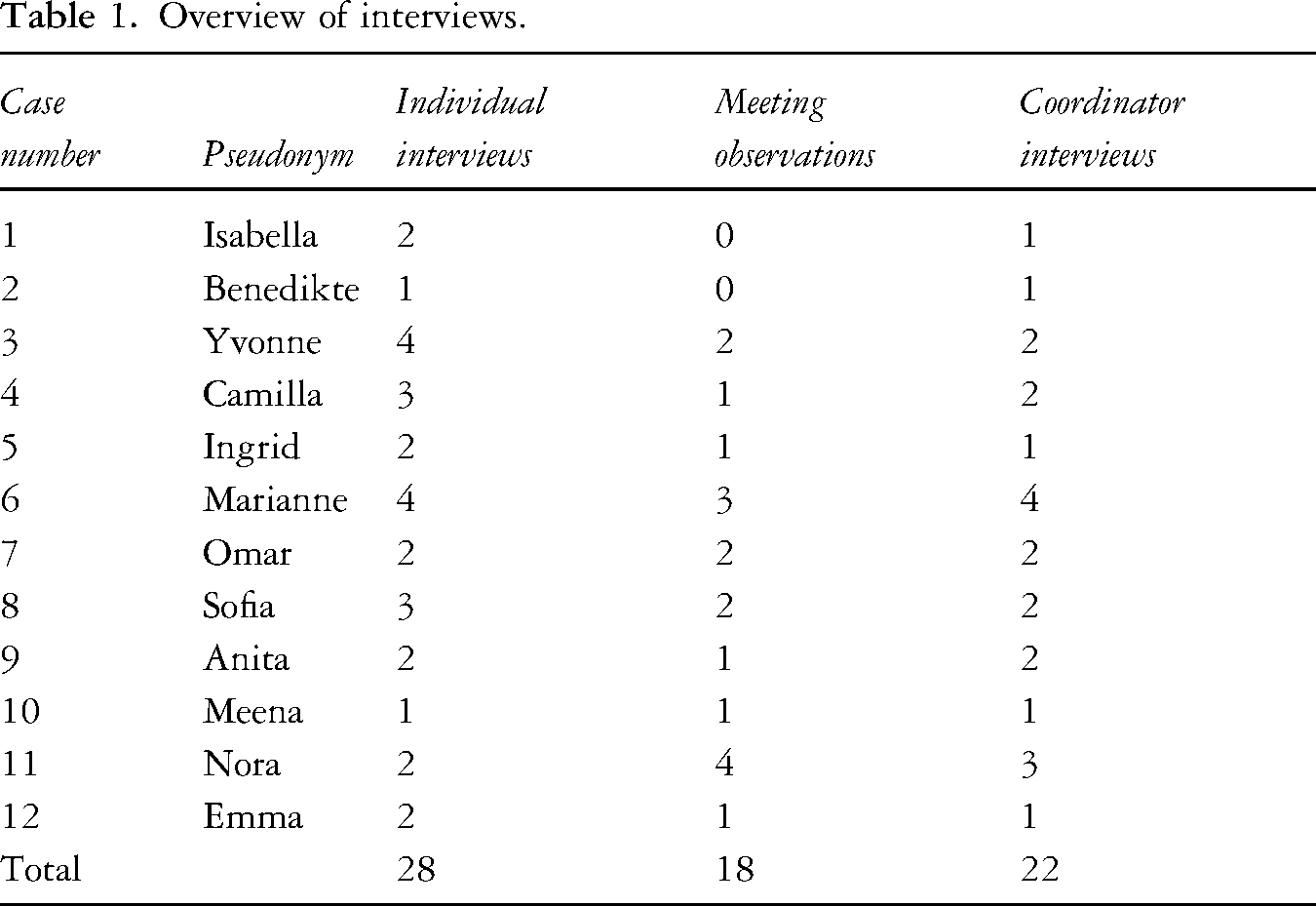
This article is based on qualitative fieldwork and interview data from five Norwegian municipalities or municipality districts. Following a longitudinal multiple case study design (Yin, 2018), 12 families participated in multiple interviews and allowed researchers to observe interprofessional meetings over a period of approximately a year (2021–2022). The families were asked by their coordinators to take part. We did not specify that we wanted contact with mothers, but in all but one case, the mother became our contact person. Most of the families lived in major city areas in the eastern part of Norway, but some also came from more rural areas. The children had multiple types of impairments; most had an intellectual impairment, and having multiple diagnoses was common. All the interviewed families had a long-term need for assistance from different services. All the children were under the age of 18 when the project started, but some turned 18 during the project period. We conducted at least one interview with each family and took part as an observer in at least one interprofessional meeting. There are some families that we have more data on because they differed in how many interviews they could attend or how many meetings we could observe. In addition to interviewing parents, we interviewed their municipal coordinators. We focus on the accounts of the parents in the analysis and presentation of the findings (see Table 1 for an overview of the data).
Overview of interviews.
The analysis combines both a categorising and connecting approach (Maxwell and Miller, 2015); hence, we both provide a broad analysis of the data and an in-depth analysis of the selected cases. To investigate the contents and nature of coordination work, we went through rounds of initial and pattern coding (Saldaña, 2016) by using the qualitative data processing programme NVivo. The parent interviews were read individually, and all statements related to coordination and administrative work were coded. Eventually, we combined the smaller codes into larger overarching categories. These categories were refined and reformulated through an iterative process of reading interview excerpts and writing. The result was a tabular overview of the coordination work. Based on this typology, we chose three cases suitable for illustrating the nature of coordination work. These three represent instrumental case studies that can shed light on the phenomenon in question (Stake, 1995). The cases were selected because they well demonstrated how parents—mothers in particular—do coordination work. The mothers also differed in how much coordination work they did and how well they coped. The cases were analysed using transcriptions of the interviews, meetings and field notes, using the coordination work typology as a guide for finding relevant material.
The project passed evaluation by the Norwegian Centre for Research Data, who reviewed interview guides and consent forms. Informed consent to record, transcribe, analyse and publish anonymised statements was obtained from all interviewees prior to conducting the interviews. All interviewees were given pseudonyms.
Findings
Parents’ coordinating and administrative work
We found six ways in which the parents did coordination work (Table 2). The categories reflect that coordination work requires parents to gain knowledge about and manage a complex system of relations, rules and rights. To navigate the system, the parents have to do a considerable amount of cognitive, relational and emotional work. Here, the mother was doing the coordinating work in all but one of the families. In addition, all the municipal coordinators were women. Hence, the coordination work had a strong gendered aspect. When asked about this pattern, the participants did not generally provide reflective elaboration; instead, it was treated more or less as a given. Consequently, we have few insights into intrahousehold negotiation. However, through the interprofessional meetings, we observed that the mothers played a crucial role in the coordination that the fathers did not. In one case where the father was doing more of the administrative work than the mother, the family were refugees, and he received a lot of assistance from their coordinator and the special school the child attended. The reasons why he did most of the follow-up was unclear. He said it was because the mother had to care for their younger child, but it could also be due to him having lived in Norway for a longer period than his wife and thus having better language skills and knowledge about Norwegian society. The overall picture is however that the mothers took on significantly more administrative work than the fathers.
Different types of coordination work done by parents of disabled children.
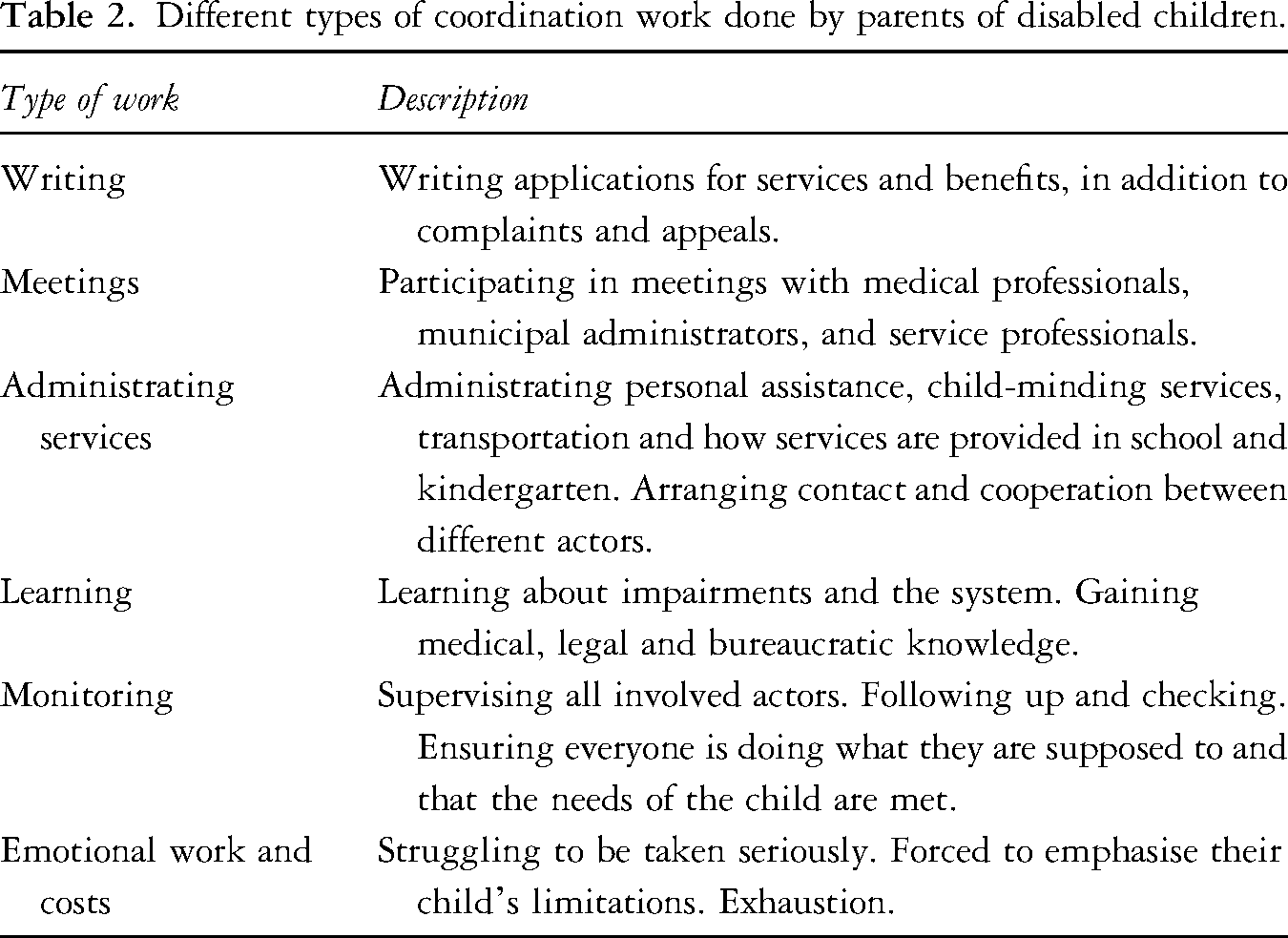
The first coordinating activity identified was writing. Writing applications, plans and appeals are essential in getting access to services and benefits and many describe this work as very time-consuming. Writing appeals and complaints was a frequent endeavour because the parents often experienced rejection on their first attempt. The parents also described attending numerous meetings with medical professionals and service providers, along with interprofessional meetings. These meetings required preparation and follow-up work afterwards. The parents also played an important role in administering services. Particularly important arenas were the school and kindergarten, where the parents ensured that the child received appropriate adjustments. Other services needing parental involvement were PAs, child-minding, transportation and medical treatment.
Another coordinating activity was learning about the child's specific impairment and how the system worked. The parents described acquiring information about diagnoses, treatments, legal rights and service provision possibilities. This information was acquired through formal courses arranged by medical treatment facilities and participation in disability associations, but mostly through their own research and informal networks. The parents also described how they constantly needed to monitor that their child was receiving the help and care that they needed. They said that they needed to be meticulous in their planning and be diligent all the time, making sure everyone was doing what they were supposed to. Constant monitoring was reported as important in uncovering gaps or deficiencies in service provision, allowing parents to quickly intervene. Finally, the parents talked about the emotional work involved in coordination. They said they needed to work hard to be taken seriously and that the feeling of exhaustion was common.
Mastering the demanding tasks of coordination: The case of Marianne
Marianne is Michael's (18) mother. She is married to Michael's father. Michael has multiple impairments and needs a lot of assistance in his daily life. He goes to a special education class in school, to which he needs daily transportation. Although Michael's father was involved in direct care, Marianne took on the role of administrator. Marianne took on extensive coordination work, most clearly shown in her being the one who attended meetings with service providers and taking the lead in documentation and writing.
Caring for her son has impacted Marianne's career. She had a creative job and managed her own company when Michael was born. She had to quit this job because she ‘needed a 9-to-4 type of job’. The job she had now was unrelated to her creative profession. Although she acknowledged intensified direct care tasks, she emphasised that navigating the system was what has taken the greatest toll on her. She said, ‘It is really not Michael who wears me out; it is the system that wears me out because you have to be so diligent’. She described a constant fight with the municipality to get the services that her son needed. Marianne early on got the impression that the municipality was driven by a desire to save as much money as possible: One time, I was introduced to a woman who worked with service allocation in the municipality. She received praise from her colleagues for being so good at reducing expenses.(…) And then I thought, well, that explains why it is so difficult to break through here.
Marianne demonstrated organisational skills in preparation for meetings, documentation work and applying for services and benefits. She also showed persistence and endurance in dealing with delays and setbacks while maintaining good relationships with helpers within the system. Marianne became successful at writing applications, complaints and appeals, and she described how she has adopted certain strategies and techniques, for example, regarding writing complaints and appeals: I have written quite a lot of complaints in the system. Because there was a period when we didn’t get what was promised. When you are in the hospital, you always get the treatment you need, right because the situation is so monitored. But when you get out to the municipality, they don’t have the same overview. So then, I had to start pushing a month after we came back.
She described several instances in which she had to write complaints and appeals to get things going. When the family first moved to the municipality a few years ago, their coordinator was hard to reach. Michael was starting in a new school, which demanded much coordination between different services. Marianne repeatedly tried to contact people within the municipality but met only closed doors in a vulnerable period in Michael's life. She elaborated on her choice of strategy: We became exhausted, my husband and I, we were ready to drop […] I have learned throughout the years that you send out to multiple people so that they know about each other […] So I wrote to the municipal district director, the physical therapist. There were some more people. I think I wrote to quite a lot. I wrote what I was unhappy with, what was difficult, and what Michael would need help with, and then that I wanted interprofessional meetings and a coordinator. And then I wrote, like a small threat, that if I didn’t receive any response within a certain time, I would contact the county governor. Because that is something that you are entitled to, it takes a lot of years to understand that you can contact the county governor.
This complaint was successful, and Marianne stated that she was pleased with the support she then started to receive from her new coordinator, Elin. Elin provided much help in interprofessional meetings and in writing applications and appeals. For example, she helped with the documentation of accommodation needs in the school. Marianne appreciated this help greatly, but getting this capable coordinator was a result of her coordination work and not giving up.
The excerpt above shows how writing a successful complaint needs to be well planned and based on acquired knowledge, demonstrating the learning aspect of coordination work. A stressful element she talked about regarding learning was that one could be entitled to support that one did not know about: ‘You are not offered anything. You need to know about things or hear about them through some acquaintances’. Thus, a key part of the learning aspect was researching what one was entitled to, and Marianne described how this was something she was left to figure out on her own.
Marianne also described spending a great deal of effort on the monitoring aspect of coordination. This is evident in how she dealt with the complaint mentioned above, and it was consistently shown in how she handled the support system. In the interprofessional meetings, Marianne was diligent in making sure that Michael's needs for adjustments at school were met. She monitored the progress on specific issues in the meetings, in communication with the school and with Elin. One of the issues regarding help to navigate within the school building to alleviate Michael's orientation difficulties was the subject of several delays. In the end, Marianne wrote a complaint to the owner of the building, which finally set things in motion. This demonstrates how monitoring requires persistence.
Marianne also mentioned the emotional costs of doing coordination work. She referred to several instances of feeling exhausted. She also highlighted how getting help entails exposing all vulnerabilities and being forced to emphasise everything that is negative with one's child: I’m thinking about parents who don’t get the help they need in the system; it's because it's very vulnerable. It has a lot to do with your feelings and with your own self-esteem and self-image. That you always have to expose your child, that vulnerability […] But I have manned up and written complaints that I found hard to write, but that I knew that I had to do if Michael were to get the help he was supposed to.
This quote illustrates how coordinating and getting adequate services is emotionally demanding.
The complex care management of a child in need of 24/7 supervision—The case of Nora
Nora is a woman in her early thirties. She is the single mother of Rikke (14). Rikke was born with a serious, complex and rare health condition demanding supervision 24/7. Rikke's father has never been involved in her care, leaving full responsibility to Nora. The family received extensive assistance from municipal services and several specialist healthcare services. Rikke attended primary school three hours a day, four days a week. The school was located several kilometres away, making her dependent on school transport. Nora was in paid work until four years ago. Her income was attendance allowance from the Norwegian Labour and Welfare Administration (NAV) and a care benefit from the municipality. Two important municipal services Rikke received were personal assistance and respite care. However, living in a rural area characterised by scattered settlements and long distances made it difficult to hire assistants: ‘We have had a hard time finding people; there are few who have applied’. Nora did not have a car, and public transportation was sparse. They had no family living close by but had kind and helpful neighbours.
Because of the number of service providers involved in Rikke's life, Nora was in touch with many actors within the municipality and specialist health services. Nora did extensive work administrating services, providing an essential link between formal care providers and between formal and informal care systems. She also needed to monitor and make sure that everything was going according to the plan. Additionally, she had to write several applications, complaints and appeals to the municipality administration or NAV. Finally, she planned, participated in and followed up on meetings with health professionals, the school and municipal services.
Nora became a first-time mother in her early twenties and experienced her first contact with the welfare and health system of her municipality as a shock: ‘You know, first-time mother with lots of expectations, and then, you are thrown right into something very, very unknown, with a steep learning curve’. She referred to several early meetings in which representatives of the welfare system seemed unwilling to provide the help she asked for. She described the meetings she did alone with the municipality and NAV as frustrating. The first meeting with the municipality when Rikke was 6 months old took an unexpected turn: ‘I just thought we were going to meet and talk about Rikke and the situation, and well, that it was going to be a pleasant meeting. But I got surprised’.
She said that she had brought documentation on Rikke's extensive care needs and thought her applications would go through easily, but that was not the case: They stood their ground. ‘It might change’, and ‘you do not need this help now’, ‘you can wait’. Even if I held a paper in my hand saying she wouldn’t [be like other children]. But they held on to their opinions. I was so young that I didn’t quite know what to say.
After this meeting, Nora got in touch with Sara, her coordinator, and told her what had happened. Sara quickly intervened by making phone calls and arranging a new meeting. Because of the help Sara provided, Nora eventually got the help she had applied for.
Nora experienced demands that conflicted with the care she provided to her daughter in the meetings with NAV: ‘The case manager meant it was just [for me] to get to work … He did not understand the situation, how serious it was. And they didn’t give in; they just kept on pushing’. Based on this situation, Nora learned never to go to a meeting alone.
Nora and Rikke depended heavily on public benefits and services. At the same time, gaining access to these services demanded that Nora put in a lot of cognitive and emotional effort as well as time. This work exacerbated the already strained situation Nora was in, providing day and night care for her daughter: I wish it was easier because you feel you face a lot of opposition both from the municipality and NAV, especially when you have to argue to get benefits to which you are originally entitled … You have enough with coping with the life you’ve been thrown into; in addition, you have to argue with the municipality and NAV.
As described earlier, the coordinator was of great significance because of the support provided to the family: We are so grateful that the coordinator function exists. You keep working so closely with people and kind of get very attached to them. We cooperate really well. It is vital to have a coordinator who speaks for you or the child, and that is what our coordinator does.
Both Nora and her coordinator did many tasks that were outside of what they were formally required. Sara made herself available to Nora whenever she needed it and helped with applications and appeals. Nora, too, did tasks far outside what can be considered her responsibility. For example, she helped her PAs with night-time transportation planning. Some of the assistants lacked a driving licence and/or a car, and public transport was sparse. Nora said that she had paid for the taxi several times to ensure that the employees met up for nightshifts in their homes. This illustrates how administrating and monitoring entailed filling gaps in service provision. Nora also spent a lot of time writing applications and appeals against decisions made by the municipality, which she described as exhausting. She often had to describe and document their needs in detail: ‘We had to write a kind of time clock, or 24-h clock, from morning until night. We wrote down everything we did and the time it took. When the rejection arrives or too little is being assigned, a lot of times goes into appealing’.
During our research involvement in spring 2022, Nora attended four meetings with several of the professional actors around Rikke. Before the meetings, Nora prepared input for the agenda. The issues discussed during these meetings concerned Rikke's state of health, for example, medical treatment and follow-up, technical equipment like chairs, wheelchairs, glasses, special clothing, nutrition, physiotherapy and occupational therapy. Concerns regarding resources, personnel situation and capacity, the transport for Rikke's home, school and respite care were discussed. What we observed as prominent in the meetings was both the responsibility and capacity Nora possessed to be the only one with a full overview of Rikke's condition and needs. Nora appeared as an expert regarding all the different areas, such as medical conditions, technical issues, transport for Rikke or the employees working nightshifts at their home or to ensure the flow of communication between school, home and respite care.
Nora was the one in charge of the ‘the whole situation’: providing direct care and coordinating the care work around her daughter, both in the daily monitoring and administration of the different aspects of Rikke's needs, in addition to having an overall picture of the public care and welfare system.
Struggling with being the one who keeps it all together: The case of Yvonne
Yvonne was the mother of Oscar (17) and Philip (18), both diagnosed with neurodevelopmental conditions. They both attended special education classes. She had been raising the boys alone since infancy, and their father was never involved in their care, even before any disability was suspected. Yvonne reported being out of paid work and living on a disability benefit. She described coordination as an exhausting part of her life: It's a struggle all the time. I have no time to live my own life. Or I do not have the energy to live my own life because there is work all the time with things that are not working out. So you have to do things over again because of something you misunderstood. And then they do not know the rules themselves, and they say they will ask someone, but they never get back to you. (…) Getting the disability benefit did not help. I work night and day anyway.
Yvonne reported being frustrated and dissatisfied with the support from and communication with the schools and other services. She talked about how she had struggled a lot over the years with accessing different types of services and benefits and that she never really had gotten what she needed. She described this work as elements of learning, writing applications and administrating services. She said that it was difficult to learn what types of services she could access: You must find out for yourself. You hear some rumour somewhere, and you ask them, What is this? Is this something we are entitled to?
Compared with many other participants, Yvonne had limited knowledge about the types of services to which she could apply. She complained about a complex and confusing system and how she became exhausted by requirements to document needs and write extensive applications: They are energy vampires; they drain you. You sit there, ruminating what needs to be done and what you need to remember. We should have somewhere we could go, where they know this stuff, who could help us fill out forms and applications and inform us what we are entitled to. You could just give them the authorisation to collect the information that they need, and then, we could get to just be mums and dads, you know. For there is not much energy left for that.
The monitoring aspect of this was also something she highlighted, saying that there was so much to do, remember and take care of all the time. As reflected in the quote above, a recurring theme in Yvonne's account was also how tired and exhausted the care work made her feel, explicating the emotional side of coordination: I am so glad I have these children; it is what comes with it that kills the joy (…) I would actually be able to do so much more with these kids and get. … I have seen what the right kind of follow-up does. That they actually can get quite far. But you have no strength left for that.
An important aspect of the emotional struggle that Yvonne highlighted was that she often gave up. She had a hard time dealing with the demands of new documentations or rejections of applications and quickly gave up when she experienced resistance. Yvonne said that she did not have the energy to pursue what she believed she and her kids needed. One example was respite care, which she had tried to get for a long time: Now I have given up on the fight for respite care for Philip because I am thinking I don’t have the energy to endure it any longer because I am tired. You get very mentally tired of everything that has to be done all the time. You need to take a lot of care and remember many dates, things need to be applied for again, and things are re-evaluated. There are meetings with all service providers, and it is just so much. (…) Then, you give up on pursuing these rights because you get so tired and if you get another rejection, then you just don’t have the energy to appeal.
The coordinating services Yvonne reported using were the coordinator and interprofessional meetings. This helped her a bit with the coordination work, but how helpful it was varied. She had multiple coordinators over the years, and some she said had helped a lot and almost become her secretary, helping with the documentation and writing of applications. Others had limited their support to taking responsibility for regular interprofessional meetings. She lacked a coordinator who could alleviate aspects of administrating, learning, writing and monitoring.
Discussion
The findings provide insights into the coordination work that parents, especially mothers, do on behalf of their disabled children. We provide an overview of the different types of coordination work demanded by the parents; the three cases are in-depth examples of how coordination work is done and experienced in practice.
Coordination of care is an indispensable part of the care a disabled child's needs. Although care is often associated with more direct and ‘warm’ tasks, the more ‘cold’ and cognitive work that the parents do in coordination is an indispensable part of the care system. As such, it may be seen like a non-nurturant form of care that should be recognised as care because of its purpose of maintaining, continuing and repairing the world of the child (Tronto, 2013).
In the cases, coordination work took the form of hidden work (Wadel, 1979), consisting of working activities that society seems to have little awareness and recognition of. This is reflected in the fact that mothers are expected to do this work on top of more direct care work and paid work. The mothers described time-consuming work requiring organisational and interpersonal skills and the ability to acquire complex legal and medical knowledge. The mothers’ coordination work demonstrated the need for what Döring (2021) calls administrative literacy, ‘the capacity to obtain, process, and understand basic information and services from public organizations needed to make appropriate decisions’ (2021: 1155). The voluminous amount of coordination is reflected in the complexity of the care system, consisting of both formal and informal visible and hidden tasks, responsibilities, actors and relationships. The mothers ended up being managers of the collective activity that constitutes the care the child receives, administrating practical tasks and managing relations between services. Although other actors often have a specific responsibility for a single part of the care event, the mothers end up with holistic responsibility, ensuring that the system as a whole can provide the necessary services.
Although intense, direct care work can be compensated financially through specific benefits, no such compensation exists for coordination or administrative work. Instead, it becomes an individualised responsibility. The gendered aspect of the work could contribute to its hidden nature, as highlighted in previous research concerning the third shift or mental load of parenting (Ericsson et al., 2021; Hochschild, 1997; Smeby, 2017). Interpreted in light of the negative consequences of employment for women (Brekke and Nadim, 2016; Reisel et al., 2020; Wondemu et al., 2022), the mental load of coordination seems a likely contributor to the observed difficulties in staying employed, in addition to the more obvious direct and practical care tasks.
How well mothers can cope with coordination is impacted by the structural disadvantages they face based on characteristics such as income, class, education and disability. These disadvantages can have clear consequences for the uptake of benefits and services because systems that rest on a considerable amount of personal effort are vulnerable to the reproduction of social inequalities (Ong-Dean et al., 2011). This is reflected in research showing how marginalised groups, such as immigrants, struggle to access resources for their child (Kvarme et al., 2016). Furthermore, previous studies have shown the increased negative effect of care work on employment patterns for parents belonging to marginalised groups (Vinck and Van Lancker, 2019).
In the three presented cases, we saw the impact of structural disadvantages on how the mothers coped with and experienced coordination. Marianne had a higher education, maintained an employment income and was married. She displayed a persistent attitude and complex acquired knowledge that she used efficiently to mobilise help. Although coordinating the life of Michael through 18 years entailed exhausting processes of applications, documentation and complaints that have come with a price, here in the form of time, energy, worry and career sacrifices, she has demonstrated her ability to manoeuvre the complex welfare system.
Nora managed the care for a child in need of day and night supervision. Her single parenting responsibility, low income and limited work experience put her in a precarious position. In the beginning of Rikke's life, this left her unprepared for the skills needed to obtain the services she needed. However, through slowly learning with guidance from helpful actors, such as their coordinator, she was able to achieve more support over time.
Yvonne, on the other hand, who must provide care on top of tackling her own disability, low income and raising her boys alone, was driven into resignation and exhaustion. In her case, she was put in a persistent precarious situation because of the system failing to consider factors such as education level, single parenting responsibility and reduced capacity because of the disability and illness of the parent. Her resignation to exhaustion resulted in her deciding not to appeal decisions she thought were wrong. Her marginalised position as a single mother living on a disability benefit was exacerbated because she had no energy left to pursue services that could alleviate her care tasks. The mothers were careful to emphasise, however, that the burden of care did not primarily come from having disabled children but from the constant fighting necessary to receive help from the system, highlighting the importance of the social aspects of disability (McLaughlin, 2019). Still, even though the situation was more precarious for the mothers with access to fewer resources, they all referred to demanding and exhausting processes of receiving help.
Although this article has focused on the care of disabled children, issues concerning care coordination are also relevant to other types of carers. The most relevant example is the carers of elderly people, who also need to interact with multiple actors and service providers (Daatland, 1983; Sussman, 2009). It is also possible to draw a parallel to sick and disabled people who are performing a lot of invisible and mentally challenging work in ‘being a client’ and dealing with health and employment services (Innjord, 2021; Wadel, 1979). Generally, the work described in this article can be applicable to various people who rely on accessing many different types of welfare and health services and interacting with different welfare state actors to achieve a meaningful quality of life. The need for coordination also intensifies in cash-for-care policy schemes towards disabled people, where service users are left to manage and organise care services on their own (Katzman and Kinsella, 2018). Thus, acknowledging the role of such work can be important for understanding the impact of different types of social policies.
Conclusion
Coordination has been highlighted as a part of the third shift (Hochschild, 1997) and a form of hidden work (Wadel, 1979) that, in line with the broad definition of care by Fisher and Tronto (1990), needs to be recognised as care. Coordination work is heavily gendered because it disproportionally falls on women. The typology presented here illustrates the complex nature of the coordination of care within an advanced welfare state. The three cases elucidate what coordination work can look like for different families in Norway, showing how obtaining adequate services demands a set of skills and persistence that leaves service provision vulnerable to the reproduction of social inequality. Despite the strong Norwegian welfare policies characterised by a significant public responsibility for serving the needs of the population, accessing the services and benefits appear to be challenging and inflexible. Thus, the mental work is substantial, which impacts parents’ employment, health and well-being. To provide families with more appropriate support, the existing coordination-oriented services (individual service plan, coordinator and interprofessional meetings) need to be strengthened. In particular, the coordinator seems to have the potential to provide crucial support. However, as highlighted in this article, the coordinators making the biggest difference for the families often went beyond their job description to do so, meaning that investing in the coordinators could contribute to the level of support being less tied to the families’ persistence. More importantly, in a stronger recognition of coordination as a form of care, support systems need to move beyond the view of care coordination that mothers do as an individualised responsibility.
Footnotes
Acknowledgements
First, we would like to thank the participants of this study who so generously gave their precious time to take part in our research project. Additionally, we thank Janikke Solstad Vedeler, Sigurd Eid Jacobsen and Elena Albertini Früh who have contributed to the data collection process and given feedback on earlier versions of the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Research Council of Norway (grant number 201877).
Author biographies
Orcid: https://orcid.org/0000-0002-6171-9890