
Abstract
Autistic people face more social barriers to, and experience greater anxiety around, intimate relationships than the general population in our majority neurotypical society, leading to increased loneliness and social isolation. National health and social care policies and publications should recognise these inequalities and guide service systems in reducing them. In this paper, we employ a document analysis design to analyse a cross-section of English national health and social care publications to investigate how autistic adults’ intimate lives are represented and prioritised in these publications. Most publications do not adequately and proportionally recognise or prioritise autistic people's intimate lives. They focus on the risks associated with sex and relationships and overlook autism-specific intimacy needs. They prioritise participation in the workforce while renouncing government responsibility for supporting intimate relationships which can reduce loneliness and alienation. We offer recommendations to ensure that health and social care publication processes better recognise intimate lives.
Introduction
In England, national health and social care policies and publications are produced by the Department of Health and Social Care (DHSC) and its ‘Arm's Length's Bodies’ (ALBs). The documents produced by these agencies play an important role in highlighting the social disadvantages and health inequalities that particular groups experience and in guiding service systems in reducing these inequalities (Putnis and Burr, 2020). However, these documents also reflect the priorities, politics, values and power structures of the policy-making elite and contain elements that reproduce and support the social processes that create inequalities, oppression, and exclusion (Burton and Kagan, 2006; Putnis and Burr, 2020). This study forms part of a larger research project examining how adult social care in England can better support autistic adults’ intimate lives. In this paper, we employ a document analysis design to identify documents published by English national health and social care agencies that reference autism and intimate lives to explore how autistic adults’ intimate lives are represented and prioritised within them.
The Autism Strategy is central to autism policy in England. The Autism Act (2009) placed a duty on the government to introduce an Autism Strategy for adults. The first Autism Strategy, ‘Fulfilling and Rewarding Lives’: The strategy for adults with autism in England (Department of Health, 2010) was published in 2010. This was then revised in 2014 with Think Autism. ‘Fulfilling and Rewarding Lives’. The strategy for adults with autism in England: An update (Department of Health, 2014). In 2021, the Autism Strategy was again refreshed and expanded to include autistic children in the National strategy for autistic children, young people and adults: 2021 to 2026 (HM Government, 2021). The joint ministerial foreword for this document reads, ‘Over the next 5 years, we want to create a society that truly understands and includes autistic people in all aspects of life’ (HM Government, 2021: 7). However, the Autism Strategy is silent about an important aspect of autistic people's lives: their intimate relationships.
In preparing the 2021 Autism Strategy, the British government commissioned researchers at the London School of Economics (LSE) to undertake rapid research to ‘improve our understanding of autistic people's experiences during this time, and our ability to respond appropriately' (HM Government, 2021: 9). This research showed that the COVID-19 pandemic has ‘exacerbated challenges many autistic people already faced, such as loneliness and social isolation, and anxiety' (HM Government, 2021: 9). The Autism Strategy also cites the findings from the National Autistic Society's (NAS) Left Stranded report (National Autistic Society, 2020), which states that compared to the general public autistic people were seven times more likely to be chronically lonely during June and July 2020 (during the COVID-19 pandemic). Given that the 2021 Autism Strategy acknowledges the challenges that autistic adults’ face with loneliness and isolation, it is striking that there is no mention of intimate relationships.
Prompted by these silences within the Autism Strategy, we employed a systematic search process to present an overview, the first of its kind, of how autistic adults’ intimate lives are represented and prioritised in English national health and social care publications. We also consider the ways in which these findings can inform future national health and social care publications so that they better recognise and support autistic people's intimate lives.
The publications considered in our analysis include publicly available policy documents, public consultation documents, clinical and practice guidance documents, training documents, reviews, and reports. While these documents are not all designated as policy, we follow Putnis and Burr (2020) who argue that argue that ‘these documents contain reflections of policy-makers and of those decisions and non-decisions, actions and inactions, perspectives and values that ultimately constitute policy'. The documents vary in their purpose, intended readership, and level of influence. However, they are all produced to inform, shape, or guide the health and social care that autistic people receive. They all reflect the priorities of the government officials who write them, and they all contain representations of autistic people and their needs. Therefore, they contribute to public health and social care discourses around autism and support for intimacy.
Defining intimate lives and sexual citizenship
The term ‘intimate relationships' has been used in diverse ways to denote various kinds of interpersonal relationships which involve emotional and/or physical intimacy and closeness. In this paper, we investigate how autistic people's sexual and romantic interpersonal relationships and practices are represented in government health and social care publications, and we use the term ‘intimate lives' to denote this. Aspects of people's intimate lives may include, but are not limited to, any of the following: meeting romantic or sexual partners, going on dates, forming relationships and bonds, expressing one's sexual identity, experiencing romantic love, engaging in preferred sexual practices, having sex, experiencing sexual pleasure, belonging to sexual communities, and starting one's own family. Intimate relationships are an aspect of most adults’ lives. Healthy intimate relationships can mitigate loneliness, act as a protective factor against the risk of suicide, and are proven to improve mental health outcomes and people's overall sense of well-being (Ballester et al., 2012; Byers et al., 2013; Cassidy et al., 2014; Hedley et al., 2019; Hirvikoski et al., 2016).
The question of how intimate lives are represented in national government publications can be linked to the concept of sexual citizenship (Bahner, 2020; Liddiard, 2014, 2017). Richardson (2000) conceptualises sexual citizenship as a collection of sexual rights: the right to express one's desired sexual practice, the right to define one's sexual identity, and the right to have it acknowledged by state institutions. The inclusion of intimate lives in national health and social care publications represents state recognition of autistic people as sexual subjects and sexual citizens with sexual rights and responsibilities. This recognition resists tropes that construct autistic people as inherently disinterested in and unknowledgeable about sex, or as sexually disordered or deviant, which can be situated within broader discourses that pathologise, infantilise, and desexualise people with disabilities (Barnett and Maticka-Tyndale, 2015; Bertilsdotter Rosqvist, 2014; Kellaher, 2015; Sala et al., 2020).
Research on autistic adults’ intimate lives
‘Autism Spectrum Disorder' (ASD) is commonly conceptualised as a life-long developmental ‘condition' characterised by difficulties in social communication and interaction; restrictive, repetitive, and stereotypical behaviours; and sensory sensitivities and differences (American Psychiatric Association, 2013; Bogdashina, 2016). However, many autistic advocates and scholars resist this conception of autism. The neurodiversity paradigm (den Houting, 2019) conceptualises autism as a form of difference and understands autistic people's difficulties as resulting largely from a lack of acceptance and accommodation within a majority neurotypical society. For example, the theory of the double empathy problem (Milton, 2012) posits that while autistic people can struggle to process and understand the intentions of others within social interactions, these challenges are bilateral: non-autistic and autistic people both struggle to empathise with and understand each other.
The majority of research into autistic people's experiences of intimate relationships focuses on asexuality, risks, sexual deficits, or problematic sexual behaviour (Bertilsdotter Rosqvist, 2014; Dewinter et al., 2020). However, there has been a shift towards developing more holistic understandings of autistic people's intimate lives (Dewinter et al., 2020). This research provides clear evidence that while some people identify as asexual or aromantic most autistic people are interested and participate in sexual and/or romantic relationships (Barnett and Maticka-Tyndale, 2015; Dewinter et al., 2013; Parchomiuk, 2019; Sala et al., 2020; Strunz et al., 2017; Yew et al., 2021). However, autistic people do face more challenges in establishing and maintaining relationships and experience more anxiety around intimate engagements than adults who are not autistic (Dewinter et al., 2017; Gavin et al., 2019; Hancock et al., 2020; Sala et al., 2020; Yew et al., 2021). Social norms and cues and normative sexual and romantic scripts and communication patterns present difficulties and elicit anxiety for autistic people (Barnett and Maticka-Tyndale, 2015; Pearlman-Avnion et al., 2017). This may result in autistic people avoiding initiating intimate and sexual relationships and can leave them isolated and feeling excluded from participating in intimate relationships (Byers et al., 2013).
Method
We aimed to develop an overview of how English national health and social care publications represent autistic people's intimate lives and conceptualise and prioritise their needs in this area. We also sought to examine how the state's responsibility for meeting these needs was constructed within these texts. We adapted the systematic search methodology set out by Putnis and Burr (2020) to identify a cross-section of publicly available documents published by English national health and social care agencies that referenced autistic adults and intimacy. We used four online databases to systematically search for all documents published by the selected agencies that contained the terms ‘autism' OR ‘autistic' OR ‘ASD' OR ‘Asperger's' AND any of the following keywords and their variations: ‘intimacy' OR ‘sex' OR ‘sexual' OR ‘romantic' OR ‘courting' OR ‘dating' OR ‘relationship' OR ‘love'. We combined the terms using Boolean function and truncation, where search platforms offered this functionality. On databases where this was not possible, we ran searches by combining the terms manually.
Inclusion criteria
Our search included documents (and guidance on webpages) published by the Department of Health and Social Care or the Department of Health (DH) as it was known prior to 2018, and the following Arm's Length Bodies: NHS England (NHSE), Public Health England (PHE), the National Institute for Health and Care Excellence (NICE), and the Care Quality Commission (CQC), as they play key roles in health and social care service provision and access, commissioning, and regulation throughout England. We limited our search to publications between January 2000 and December 2021, which included documents published in the decade before the 2009 Autism Act and the most recent Autism Strategy.
Exclusion criteria
As the focus of our research is on adult health and social care in England, we excluded publications from outside England. We excluded commissioned documents written by academic institutions as their status as policy documents is not clear (Putnis and Burr, 2020). We excluded documents which were exclusively about children and young people.1
Database search process
As systematic searches for grey literature have no ‘gold standard' (Godin et al., 2015), our aim was to record our search process as methodically as possible to allow for replication. As each search platform functioned slightly differently, there was a need to adjust our search process accordingly, while aiming to keep the search process as uniform as possible to allow for results to be comparable across platforms. The databases and search filters applied are presented in in Figure 1.
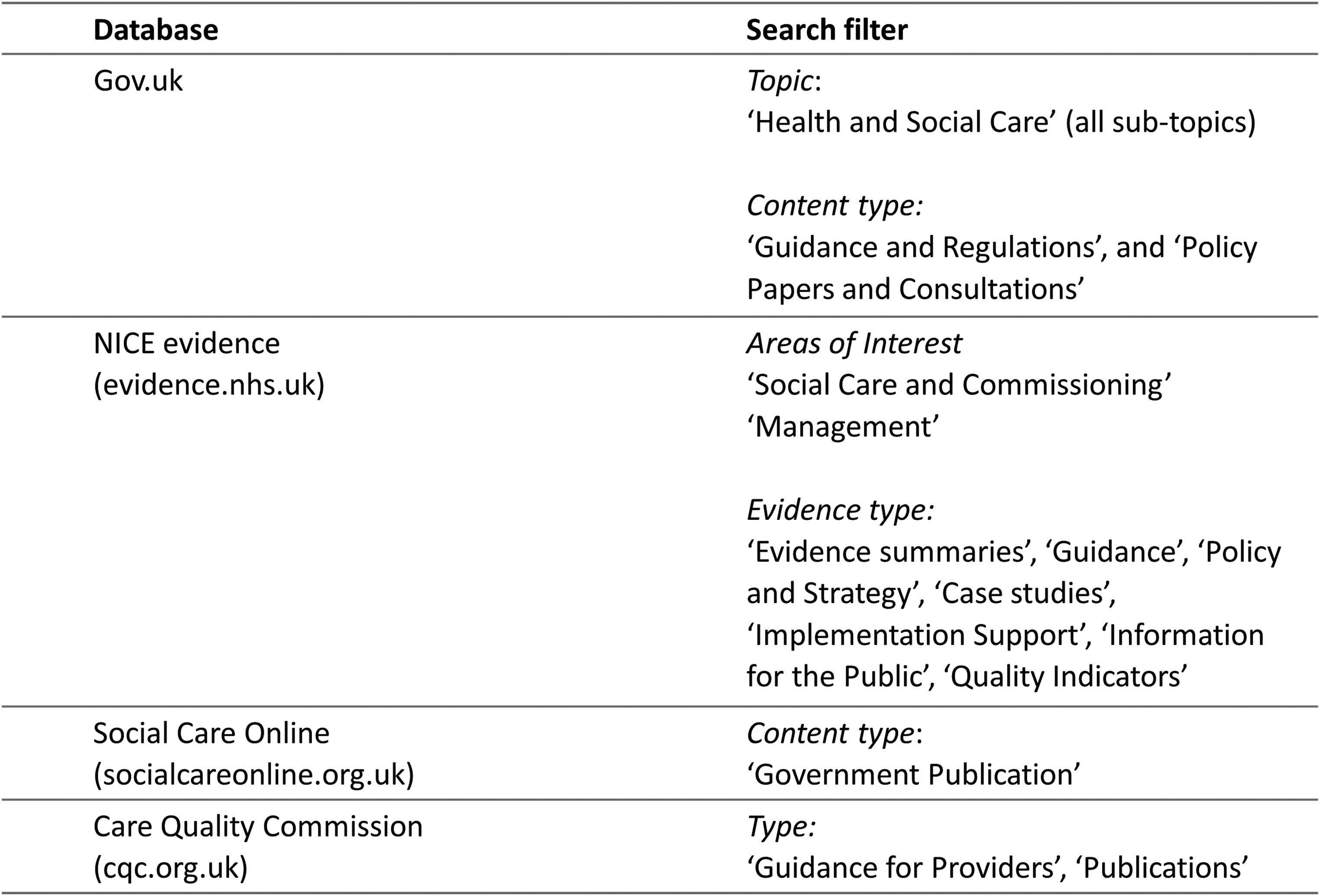
Database search particulars.
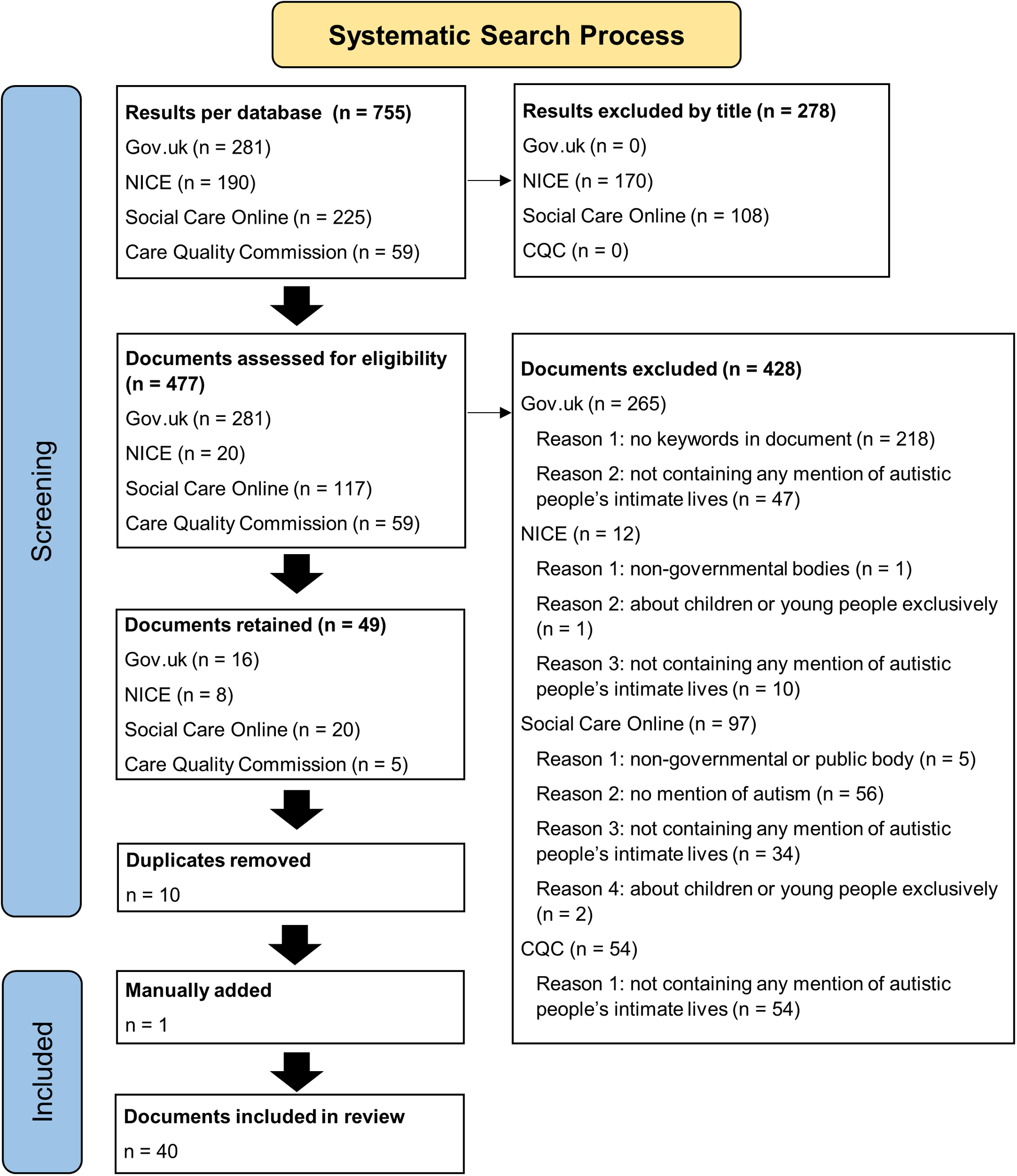
The searches were conducted between 7 September and 15 December 2021. In total, 755 documents were identified across the four databases. A total of 278 documents were excluded by title. The remaining 477 documents were read to assess for eligibility and 428 documents were excluded (see Figure 2). Ten duplicates were removed, and one document was manually added. This process resulted in 40 documents being reserved for analysis (see Addendum A for the list of documents retained).
Systematic search process.
Data analysis process
The data were organised following the principles of Braun and Clarke's approach to thematic analysis (TA) (2006), adapting the process to suit our policy analysis. As we aimed to provide an overview of the extent to which autistic adults’ intimate lives are represented in English health and social care publications, we analysed the data at a content level (Braun and Clarke, 2006). We also analysed the data at the discursive level to examine how language is deployed within the texts to construct particular objects and subjects and to examine their relationships to systems of power (Parker, 2004).
The 40 documents were organised chronologically and then subjected to close reading by the first and the second authors independently. Data was then organised into three broad sub-categories: Autism non-specific documents, Autism Strategy documents, and other autism-specific documents. Each document was then re-read and every instance within each document that contained a reference to autistic people's intimate lives was extracted. Initial themes and sub-themes were identified. In refining the final themes, we returned to the original documents to read the relevant extracted data back in context. As many documents were related to or contingent upon each other, this approach allowed us to analyse the data thematically without losing the temporal relationship between the documents. While this last step was time-consuming, it was essential for developing a detailed and contextualised overview of the discourse in these documents over time.
Results and discussion
The 40 documents retained for analysis include publicly available policy documents, consultation documents, guidance documents, reviews, and reports. Of these documents, 62.5% (n = 25) pertain specifically to autism (autism-specific documents) and 37.5% (n = 15) include but are not exclusively about autistic people (autism non-specific documents). The majority (n = 20) of the autism-specific documents relate to the Autism Strategy and a further five documents are autism-specific guidance documents which are not directly related to the Autism Strategy. We present our analysis in three sub-sections: Autism Non-Specific Documents, Autism Strategy Documents, and Other Autism-Specific Documents.
Autism non-specific documents
We retrieved 15 autism non-specific documents which included but were not solely about autistic people. The autism non-specific documents consist predominantly of clinical and practice guidance documents and reports which often relate to the care of people living in supported housing and residential care settings, including people with learning disabilities and mental health conditions and older people. As such, autism non-specific documents often refer to autistic people with learning disabilities and those with high support needs. We identified two key themes within this data: a failure to recognise and represent autism-specific intimacy needs, and a disproportionate focus on risk.
Failure to recognise autism-specific intimacy needs
Our analysis revealed that sex and relationships were addressed in many of these documents, but there was no acknowledgment of autism-specific needs. For example, our dataset included two guidance documents [36;39] published by the CQC that focus solely on sexuality and intimacy, but neither includes any points on autistic people's particular intimacy needs. Moreover, the phrase ‘people with learning disabilities and/or autism' was prominent within this sub-set of the data. This is a dominant label or identifier used within learning disability policy and practice discourse which recognises that some people with learning disabilities are also autistic. However, this language tends to conflate learning disabilities and autism as though they are one and the same thing. In discussions about sex and relationships, people with learning disabilities and autistic people were referred to together as though all their needs were homogeneous. The material consequences of this are that autistic people with learning disabilities in residential care and supported housing settings may not receive support for their intimate lives that is sensitive and responsive to their needs related to being autistic, such as those related to sensory preferences and needs, social anxiety, and communication differences.
Discursively, language which fuses or merges autism and learning disabilities operates beyond the residential care settings these documents pertain to. The dominant language that associates all the support that autistic people may need with having learning disabilities produces the autistic subject without learning disabilities as devoid of the need for social support. This produces only one kind of autistic subject deserving of and eligible for social care and decentres any emphasis on the kinds of resources and support autistic people without learning disabilities may need, do draw upon, or may be eligible for. This sheds light on the findings of our (forthcoming) research with autistic adults without learning disabilities living in England who reported that they received no or unsatisfactory support around their intimate lives despite facing significant challenges, which many participants felt had severe implications for their mental health.
Disproportionate focus on risk
Our analysis reveals that collectively autism non-specific documents represent issues around sexuality disproportionality in terms of risk, vulnerability, and risk of sexual offending. Case studies of autistic people tend to depict examples of autistic people falling victim to sexual abuse or being otherwise negatively affected by being involved in intimate relationships [26;39]. These documents position autistic people as either vulnerable to exploitation and abuse or as being ‘at high risk of sexual offending' themselves [28;16]. For example: Future guidance needs to recognise and emphasise the increased vulnerability of people with a learning disability or autistic people to sexual harm within care settings, and that they may have greater difficulty talking about issues. We were also told that people with a learning disability or autistic people may have limited knowledge about sex and sexuality, so rely on staff to be proactive in helping them receive advice and education. [39;25]
These discourses frame sex and relationships as ‘risky' for autistic people and position social care providers as primarily responsible for managing and mitigating these risks, rather than placing an onus on them to also support autistic people to develop their intimate lives. It is important to recognise that some autistic people may be vulnerable to being taken advantage of. However, when risks are emphasised disproportionately, and in the absence of positive discourses around sex and relationships, this reinforces common tropes about autistic people as victims or perpetrators of sexual violence, thereby perpetuating tropes that contribute to the marginalisation and social exclusion that autistic people experience (Bertilsdotter Rosqvist, 2014).
Furthermore, we found that CQC guidance documents contain risk-averse language and repeated references to the need to ‘eliminate' ‘mixed-sex' accommodation to ensure sexual safety as a measure of good practice: The trust could not comply with mixed-sex accommodation guidance when they admitted males and females into short breaks units at the same time. On some occasions, patients were placed on enhanced observations to keep them safe, which they would not have needed had they been in single sex accommodation. [37;40]
The values and assumptions underpinning blanket mandates to end ‘mixed-sex' accommodation, particularly the above assertion that placing people in ‘single-sex' accommodation removes the need to take extra measures to keep patients safe, are concerning. Such statements rely on narrow, heteronormative, cisnormative understandings of gender, sexuality, and sexual violence. Future research specifically analysing CQC inspection reports would make a valuable contribution to understanding this landscape.
Autism Strategy documents
Half of all the documents retained for analysis in this study pertain to the Autism Strategy, reflecting the centrality of the Autism Strategy to national health and social care policy and guidance on autism. As the autism strategy sets out the government's approach to improving the lives of all autistic people, these documents include and refer to all autistic people, rather than just those with learning disabilities and those living in residential settings. To date, the government has published three versions of the Autism Strategy: in 2010 [6], in 2014 [12], and in 2021 [24]. In addition, there are numerous documents associated with each strategy, including public consultation documents and government responses, equality impact assessments, implementation plans, statutory guidance, and progress reports, often published alongside easy-read and plain English versions.
Failure to recognise intimate lives proportionally
Despite the design of our study, which only included documents that mention any aspect of intimacy, a key finding within this subset of the data is that autistic adults’ intimate lives are deemphasised and often invisibilised. These documents identify and prioritise many aspects of autistic people's social lives, such as work, community involvement, recreational activities, and supporting relationships with parents and carers. However, none of these documents include similarly weighted discussions relating to intimate relationships, sex, marriage, or parenthood. No documents in the Autism Strategy subset contain a section that specifically addresses intimate lives in any detail.
The Autism Strategy documents claim to be working towards creating ‘fulfilling and rewarding lives' for autistic people and building a society that ‘truly understands and includes autistic people in all aspects of life'. Yet, they fail to include intimate lives proportionally within their pages. In doing so, they construct autistic people as subjects for whom an intimate life is not a necessary or legitimate facet of leading a fulfilling and rewarding life. In turn, these texts reinforce pervasive infantilising understandings of autistic people as devoid of desire to form intimate relationships or to start families of their own (Barnett and Maticka-Tyndale, 2015; Bertilsdotter Rosqvist, 2014). For example, the 2021 Autism Strategy contains a sub-section entitled, ‘Supporting positive transitions into adulthood'. While the document includes detailed information to support autistic people's transition into work, it makes no reference to the intimacy-related changes commonly associated with transitioning into adulthood like moving in with a partner or starting a family. The strategy fails to recognise that autistic people engage in these kinds of transitions and that they have a right to support for them.
While our methodology was not designed to systematically identify how other health and social care needs were represented, we noted a distinct emphasis on work, employment and productivity alongside the silences around intimate lives. While there are zero intimacy keywords in the 2021 Autism Strategy (bar the term ‘sexual orientation' in the foreword), the word ‘employment' appears 35 times and the word ‘employer' a further 11 times. Here, autistic people are produced as subjects who should participate in the workforce, but they are not recognised as sexual citizens who can contribute to and participate in intimate lives. The disproportionate focus on supporting autistic people to participate in the workforce reflects neoliberal market-orientated principles of governance that dominate political and economic discourse and social policy in the UK and worldwide (Burton and Kagan, 2006). This ongoing shift from ‘welfare to workfare', beginning in the UK in the 1980s under the Thatcher government, centres on reduced state expenditure and responsibility by means of increased emphasis on principles of individual responsibility, productivity, self-reliance, resilience, and choice (Burton and Kagan, 2006). Our analysis shows how support for work and employment which offer, according to neoliberal sensibilities, clear financial returns on state expenditure are prioritised. They are prioritised at the expense of support in areas of social life, such as intimate lives, that have the capacity to be humanising and dignifying and to promote social connection and participation which can address the loneliness and alienation that many autistic people experience (Burton and Kagan, 2006; McGimpsey, 2017).
Absence of actionable commitments
While the three versions of the Autism Strategy include very little intimacy-related discourse, some of the associated documents do mention supporting intimate lives. For example, the 2010 Statutory Guidance for Local Authorities and NHS Organisations to Support Implementation of the Autism Strategy [11] states: The ability for people with autism to have relationships that potentially may lead to marriage or civil partnership is included in the Government's goal for people with autism to live fulfilling and rewarding lives, as well as people with autism's right to be treated fairly as individuals when accessing pregnancy and maternity services. [11;32]
Strong, emotive language is used to communicate the governments’ commitment to supporting autistic people to participate in intimate relationships. However, we found no recommendations or concrete commitments within any documents within the Autism Strategy subset that would enable these commitments to be enacted. For example, the 2010 Autism Strategy [6] and its associated implementation plan documents [8, 9, 10, 11] stipulate the specific financial investments the government will make towards each of its listed priority areas and detail the actions to be taken towards each priority area. There are no such specific commitments around support for intimate lives. The presence of broad sweeping statements of support alongside the absence of any of the necessary plans, resources, and actions to realise these commitments is made possible by displacing state responsibility for this support onto the third sector.
Displacing government responsibility
Our analysis reveals that the responsibility for delivering support surrounding intimacy is consistently displaced from the state onto individuals and the third sector. One example from the 2010 Autism Strategy follows: A number of colleges have now developed programmes for adults with autism that focus on social and living skills… West London Community College offers adults with autism courses in emotional health, sexual relationships and living in the community… There are also many support groups, run by third sector organisations, people with autism and their families. These play an important role in giving adults with autism a social life, supporting them to build relationships and enabling them to meet others with autism without worrying about how they will be judged or viewed. They can also provide an invaluable setting for training in life skills, as well as social skills, for example in cooking, dealing with money and bills and relationship advice. [6;64]
Community colleges, user-led and voluntary support groups, and third sector organisations are repeatedly positioned as responsible for and as already providing this support. Reflecting neoliberal principles of self-help, provision of support for intimate lives is consistently positioned outside the domain and responsibility of the state (Ward et al., 2020). This displacement of responsibility exists without any commitments from the government to provide the resources or structures to support and enable third sector organisations to provide these services. These texts operate to absolve the state of responsibility for autistic people's intimate lives.
Equality and diversity discourses
Autistic people are a very diverse group, and Government policy and guidance should recognise the multiple and intersecting inequalities that they may face (Diemer et al., 2022). Many of the documents in our dataset were retrieved because they contained the term ‘sexual orientation'. However, closer analysis revealed that very few of these documents meaningfully address they ways in which sexual orientation intersects autistic people's intimate lives and the support they may need. This is even though a substantial proportion of autistic adults identify as queer or LGBTQIA + (Graham Holmes, et al., 2022). Sexual orientation is most often listed in a generic fashion alongside the other protected characteristics (set out in the 2010 Equality Act), in terms of being a potential barrier for accessing existing services. Further, between 2010 and 2021, discussions of sexual orientation remained static within the Autism Strategy documents. This is best evidenced by the fact that multiple documents published over several years contain identical sentences or paragraphs referring to sexual orientation, lifted verbatim from an earlier document and pasted into the next [e.g., 7, 8, 11, 12]. This repetition reveals the superficial and tokenistic ways in which policy-makers have considered sexual orientation in the Autism Strategy, at the expense of genuine, sustained engagement with the intersecting and complex inequalities that this heterogeneous group experience (Diemer et al., 2022). Though a detailed discussion is beyond the scope of this analysis, it is vital that future research and policy on supporting autistic adults’ intimate lives recognises sexuality, sex, gender, disability, ethnicity, class, culture, religion, and age as important sites of difference for autistic people which may shape individuals’ intimate lives, the challenges they experience, and the support they may need.
Stakeholder consultation and the Autism Strategy policy-making process
All three versions of the Autism Strategy were informed by public consultation processes which collected responses from a wide range of stakeholders, including autistic people and their friends, family, and allies. However, no consultation contained a single question that asked specifically about intimate lives. Failing to ask questions about intimate lives limits the data that can be collected to develop an understanding of autistic people's needs and generate the evidence that is needed to recognise this as a policy priority. On a discursive level, the failure to include intimate relationships in Autism Strategy consultations constructs and maintains intimacy as a ‘non-issue' for public health and social care.
However, despite policy-makers’ failure to include questions about intimate lives in Autism Strategy consultations, people did raise priorities around intimate lives in response to more general open-ended qualitative contributions. This is reflected in the following excerpts from published consultations: I have found the group we work with starting to organise their own free time now they know each other, including having intimate relationships. This needs ongoing support though to untangle misunderstandings. Our group attends music nights, go to the cinema, go round to each other's homes for food and we regularly eat out in local restaurants. With the right type of support all these things are possible. [4;64]
The second can be about future planning and life milestones. My dad is hoping that I could get married so that there can be someone to look after me. [21;26]
Although no direct questions about intimate lives were included in any consultation, support for intimate lives appears in Autism Strategy consultation reports because respondents raised this themselves in their qualitative responses. These quotes provide positive representations and tangible suggestions for how intimate lives may be supported. The first quote (from a care provider) acknowledges that autistic people do enjoy full and rewarding social lives, including having intimate relationships, while also highlighting the need for autism-specific support to facilitate this. In the second excerpt, an autistic respondent touches on the importance of a whole-life approach and shows that transitions related to intimate lives are important to plan for, a priority absent from all three versions of the Autism Strategy. From 2009, the Autism Strategy consultation documents contain detailed stakeholder contributions such as these. Yet, these priorities around intimate lives are not acknowledged in the government's official published responses to the public consultations [5;17] and ultimately do not appear in the Autism Strategy. This demonstrates how autistic people's expressed priorities surrounding their intimate lives are written out of the policy-making process.
Likewise, any social issues raised in public consultations which do not align with existing government priorities are more likely to be side-lined during the policy-making process. While supporting autistic adults to participate in the workforce, which aligns with neoliberal market-orientated principles of governance, is emphasised within the Autism Strategy, support around intimate lives does not feature. However, we argue that priorities around sex and relationships are particularly at risk of being disregarded by policy-makers because, in our society, sex is constructed as something exceptional, private, delicate, and potentially humiliating or dangerous, rather than as an ordinary part of everyday life (Huysamen and Sanders, 2021). Moreover, stigmatising tropes about autism and sexuality position sex and relationships as inherently undesirable, inappropriate, or risky for autistic people. These discourses operate together within a conservative, increasingly risk-averse public health and social care sector. As a result, autistic people's priorities around their intimate lives are particularly likely to be avoided by those responsible for producing policy and practice guidance. This is supported by our data and points to the importance of creating processes which ask autistic people directly about intimate lives, as well as building monitoring and accountability into the policy-making process itself. This will ensure that the insights around sex and relationships generated through consultations are not discarded during later stages of the process.
Other autism-specific documents
Our data set contained five further autism-specific documents which did not pertain to the Autism Strategy. These were all practice guidance documents [15, 18, 22, 23, 25]. Although these documents included more holistic representations of autistic adults’ intimate lives than the rest of the dataset, the majority simultaneously reproduce tired tropes and damaging discourses around autistic people's sexualities. For example, the following NICE clinical guidelines state: All staff working with autistic adults should be sensitive to issues of sexuality, including asexuality and the need to develop personal and sexual relationships. In particular, be aware that problems in social interaction and communication may lead to the autistic person misunderstanding another person's behaviour or to their possible exploitation by others. [25;14]
The NICE guidelines are clear that those working with autistic people should recognise and support people's desires to develop intimate relationships. However, they simultaneously reproduce tropes around autistic people's sexuality, such as the tendency to be asexual or a perceived vulnerability to sexual exploitation. This NICE guidance also reproduced individual/deficit discourses around autism, suggesting that ‘problems in social interaction and communication' may cause autistic people to misunderstand other people's behaviour, failing to recognise that non-autistic people may equally misunderstand autistic people's behaviour (Milton, 2012). This situates the root of challenges surrounding intimate relationships with the autistic individual, rather than drawing on a social model of disability to understand the social determinants of these challenges and to develop strategies to address them (Oliver, 2013).
Principles for good practice
One of the five autism-specific practice guidance documents, the 2019 Core Capabilities Framework for Supporting Autistic People [22] differed from the rest of our dataset because it did proportionately recognise and prioritise autistic adults’ intimate lives. The Core Capabilities Framework is a guidance document that sets out the essential capabilities that all staff involved in supporting autistic people should demonstrate. The framework was co-developed with autistic-led organisations, autistic individuals, and their family members through a consultative process that included a series of co-production workshops and a large online survey consultation.
The framework is comprised of 19 different capabilities encompassing diverse aspects related to autistic people's lives and well-being. Capability ten is Relationships, Sexuality and Sexual Health, making the framework the only autism-specific document published by the English government and its ALBs to contain a dedicated section on autistic adults’ intimate lives. The framework does not privilege intimate lives above any of the other areas but recognises it as one of the 19 priority areas. This is discursively important because it represents autistic people holistically, as multifaceted people. It recognises them as sexual citizens who may participate in, and require support with, intimate relationships along with other areas of social life (Bahner, 2020; Weeks, 1998). The framework also offers balanced representations of autism, intimacy, and risk. It raises issues such as exploitation, abuse, intimate-partner violence, sexual offences, and hate crime. However, these concerns around risk and vulnerability are not discussed in isolation but are presented alongside positive discussions about sex and relationships, producing balanced considerations around supporting autistic people's intimate lives to guide social care.
The Core Capabilities Framework sets out the autism-specific knowledge, skills, and competencies needed to provide adequate support for autistic people's intimate lives. It offers clear and actionable recommendations which both guide practitioners and hold them accountable for providing support around intimate lives. The document is structured around what the practitioner should ‘be able to' do. This flips dominant discourses that locate the responsibility and the root of challenges around intimate relationships with the autistic individual's deficits, disorders, and vulnerabilities. Instead, it positions both the responsibility and the need for improvement with the care provider. This approach to supporting autistic adult's intimate lives is underpinned by a social model of disability (Oliver, 2013), as is reflected in the excerpt below: Our lives are enriched by our hopes and dreams and we aspire to lives enriched by relationships and fulfilling roles in our workplace. Autistic people however, often encounter obstacles in achieving a good life due to insufficient public understanding of autism. [22;4]
The framework is also underpinned by a person-centred, strengths-based approach to supporting sex and relationships, recognising that it is important to ‘work with autistic people to review the support they need to maintain and develop relationships' [22;54] and to utilise autistic people's strengths and aspirations to shape support around their intimate lives. Together, this language resists the deficit/medical models of autism which frame autistic people's challenges in terms of neurodevelopmental discourses and their individual deficits and disabilities (Bertilsdotter Rosqvist, 2014). This allows for a discursive shift from the inherent risks and biological limits to having intimate lives towards discourses that recognise the possibilities and capabilities for intimate lives, achieved through social change.
The Core Capabilities Framework also utilises a ‘whole life' approach to supporting intimate lives. All the discussions on supporting transitions include and recognise the need for support around intimacy-related transitions, such as moving in with a partner, getting married, pregnancy, or becoming a parent. This is in stark contrast to the other documents analysed in this study. The framework is the only document in our dataset that recognises the importance of autism-specific sex and relationship education and support across the whole lifespan. For example, the document states that practitioners need to: Identify and evaluate needs for autism-specific sex and relationship education across the lifespan and across the spectrum and how these needs can be met. [22;55]
This whole-life approach to supporting autistic adults’ intimate lives and thinking about autism-specific sex and relationship education not just for childhood is crucial because many autistic people, particularly those without a learning disability, only receive an autism diagnosis in adulthood (Crane et al., 2020). Our ongoing research with autistic adults without learning disabilities (forthcoming) suggests that recognising that one is autistic as an adult can prompt new realisations about sexual identity, relationship preferences, and intimacy-related needs where age-appropriate resources and support around sex and relationships are sought.
The Core Capabilities Framework can offer a foundation, both in terms of content and process, for producing various types of public health and social care documents that influence or determine the social care autistic people will receive. The level of detail and the intended focus and purpose of this guidance document may not be applicable for every type of government document that we have reviewed here. However, the values and principles that underpin it, and the proportional ways in which intimate lives are represented and prioritised, are. We recommend that it is read by those responsible for producing and reviewing autism-specific health and social care guidance and policy.
Conclusion: Suggestions for future health and social care publications
Our systematic document analysis demonstrates that most national health and social care publications do not adequately and proportionally recognise and prioritise autistic people's intimate lives. The documents that include but are not solely about autistic people focus disproportionately on the risks associated with intimacy and fail to recognise autism-specific needs, such as those relating to sensory preferences and needs, social anxiety, and communication differences. By conflating the needs associated with autism and with learning disabilities, these documents decentre autism-specific needs related to sex and relationships and also obscure the fact that autistic people without learning disabilities may also benefit from support around intimate relationships.
Despite being couched in warm and empowering language, many of the discussions around sex and relationships are underpinned by and reproduce deficit/medical models of autism. These discourses conceal and reproduce the marginalisation of autistic people that health and social care systems are tasked to address. Further, the Autism Strategy and related documents reflect neoliberal values which prioritise autistic people's productivity and participation in the workforce above supporting relationships that can help to alleviate alienation and loneliness.
Our research was initially motivated by the absence of intimate lives from the 2021 Autism Strategy. Our aim was to inform future guidance and policy-making processes, including advising those tasked with reviewing and developing the government's next Autism Strategy. To improve future health and social care publications and ensure that autistic people's priorities around their intimate lives are no longer overlooked, policy-makers must avoid the deficit/medical discourses and the abdication of state responsibility for intimate lives that we have identified in our analysis. However, when thinking for the future, there is no need to start from scratch. The values, principles, and processes reflected within the Core Capabilities Framework offer a valuable starting point.
Our central recommendation is to give autistic people's intimate lives both space and recognition within national policy and practice documents, relative to other aspects of participation in social life. We also stress the importance of providing balanced representations of autistic people's intimate lives which recognise but are not driven by considerations of risk. Our analysis reveals the benefits of recognising autism-specific needs around intimacy and relationships, and the need for health and social care publications to prioritise support and resources around sex and relationship for autistic people across the whole lifespan. The Core Capabilities Framework demonstrates the value of publications that are informed by a social model of disability and person-centred, strengths-based approaches that are both driven by autistic people's aspirations and that address the social barriers produced by our majority neurotypical society. Any publication about intimate lives must recognise that autistic people are not a homogeneous group, and that sexuality, gender, disability, ethnicity, class, culture, religion, and age are important sites of difference which may shape individuals’ intimate lives and their support needs.
Our analysis reveals that policy- and guidance-making processes should employ genuinely participatory processes that include autistic people at all stages. Consultations should include direct questions about sex and relationships and employ open-ended questions and qualitative methods of data collection. Where only closed-ended quantitative responses are collected, consultations are limited to generating evidence on priorities that policy-makers have already set. Including open-ended questions and using qualitative methods of data collection allows autistic people's own agendas to feed into the process. Finally, policy-making processes should incorporate monitoring and accountability mechanisms that ensure that the priorities that autistic people raise during public consultations are reflected in the final publications, and recognition of their intimate lives is not lost along the way.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study represents independent research funded by the National Institute for Health and Care Research (NIHR) School for Social Care Research (NIHR SSCR). The views expressed are those of the authors and not necessarily those of the NIHR SSCR, NIHR or Department of Health and Social Care.
Notes
Author biographies
![]() ). Monique is a critical qualitative researcher with interdisciplinary interests. Her research centres on sexuality, intimacies, sexual health, and social justice. Recent publications include: A Critical Reflexive Approach to Sex Research: Interviews with Men Who Pay for Sex (Routledge) and a co-authored article in Sociological Research Online.
). Monique is a critical qualitative researcher with interdisciplinary interests. Her research centres on sexuality, intimacies, sexual health, and social justice. Recent publications include: A Critical Reflexive Approach to Sex Research: Interviews with Men Who Pay for Sex (Routledge) and a co-authored article in Sociological Research Online.