
Abstract
Circulating testosterone levels decrease as males age and this is associated with changes in muscle mass, bone density, libido and general wellbeing. Testosterone booster (TB) supplements are purported to increase testosterone and mitigate some of the physical and psychological symptoms of ageing. These supplements are popular in young and middle-aged males yet there is limited assessment of the beliefs, perceptions and experiences of males who use TB supplements. This cross-sectional, online survey explored the motivations, experiences and viewpoints of a sample of 182 males with experience of using TB supplements. Approximately two thirds of survey respondents perceived they had gained expected benefits from TB supplements despite concomitant use of other dietary supplements, instigation of lifestyle change and lack of objective measurement of effects. Perceived benefits included positive body composition alterations and improvements to energy and libido. One quarter of respondents reported mild side-effects from TB supplements. As such, caution is advised when taking TB supplements, and monitoring of adverse events is recommended.
Introduction
Middle age is a significant time for changes in skeletal muscle mass and strength. Skeletal muscle mass decreases by 30–50% between the ages of 40 and 80 years (Akima et al., 2001; Allen et al., 1960; Lexell et al., 1988; Young et al., 1985) with this loss affecting individuals beginning in the fourth decade of life (Lexell et al., 1988). A loss of skeletal muscle mass of 1–2% per year occurs with a corresponding loss of muscle power of 3–4% per year (Skelton et al., 1994) after the age of 50 (Frontera et al., 1991; Macaluso and De Vito, 2004; Roubenoff, 2001). There are numerous contributing factors to these changes including reduced endocrine function, decreased physical activity, and inadequate nutrition. Reduction in testosterone plays an important role in muscle changes with ageing, however testosterone therapy is only clinically indicated for men with proven hypogonadism (Bhasin et al., 2018). Consequently, some males who are concerned about reduced testosterone levels and associated changes to body composition pursue supplementation with testosterone booster (TB) supplements.
The term ‘testosterone booster’ refers to a heterogeneous group of herbal or nutrient-based supplements that claim to increase serum levels of total and free testosterone, enhance the effects of testosterone, or improve symptoms associated with hypogonadism (Aguilar-Morgan et al., 2022; Cui et al., 2015). Social media outlets and the number of TB supplements available in the online retailer space suggest an increasing interest in these supplements (Handelsman, 2017; Pandher et al., 2023; Singh et al., 2023). Interest appears to be driven by a desire to increase testosterone levels ‘naturally’, utilise safer and more affordable alternatives to testosterone replacement therapy (TRT), and support gains in muscle mass (Aguilar-Morgan et al., 2022; Cui et al., 2015; Smith et al., 2021).
A number of TB supplements have potential to increase testosterone in men. Morgado et al. (2023) concluded that β-hydroxy-β-methylbutyrate (HMB), and betaine demonstrated increased testosterone under RCT conditions and tongkat ali (Eurycoma longifolia), purified shilajit extract and ashwagandha (Withania somnifera) possibly increased testosterone levels. Other reviews provide similar evidence that ashwagandha, fenugreek and tongkat ali increase testosterone levels (Aguilar-Morgan et al., 2022; Lazarev & Bezuglov, 2021). These reviews identify limitations in study heterogeneity and a high risk of bias in the existing literature. The specific mechanisms for increasing testosterone are unknown. However, it has been proposed that the biologically active substances in TB supplements inhibit the conversion of testosterone to oestradiol by the aromatase enzyme, thus increasing total testosterone levels, while testosterone release from sex-hormone binding globulin (SHBG) increases total testosterone (Chaing et al., 1994; Talbott et al., 2013).
Assuming TB supplements act as proposed and effectively increase testosterone, these supplements have the capacity to elicit an array of health benefits. Whether or not TB supplements improve muscle mass is equivocal (Isenmann et al., 2023; Wankhede et al., 2015) and other proposed benefits of TB supplements such as improvements in mood, fatigue and mental outlook are under-explored. This exploratory survey seeks to explore the self-reported experiences of males who have used, or are using, TB supplements. We aim to understand the perceived positive and negative effects in order to identify factors to be assessed objectively in future intervention projects.
Materials and methods
An online survey was used to collect data from a sample of males who were either currently using or had used commercial dietary TB supplements. Ethics approval was granted by the University of Canberra Human Research Ethics committee (no: 13598). The survey was conducted and reported according to the Consensus Based Checklist for Reporting of Survey Studies (CROSS) (Sharma et al., 2021) (see Supplementary material).
Participants
Males were recruited through purposive sampling. The survey was advertised on social media pages and groups (Facebook, Instagram and Reddit). Posters advertising the survey with a QR code link were displayed in the male changerooms of three fitness centres in the Australian Capital Territory and an international supplement company shared the survey link via their customer email distribution list. Male participants were eligible to complete the survey if self-reported to be currently using or have used a TB supplement at any time in the past.
Protocol
The survey was developed based on existing literature and discussions with the research team (strength and conditioning coach, exercise physiologist, sports dietitian, sports physician). Qualtrics software (Qualtrics, Provo, UT, USA) was used to house the survey. The survey included a range of question styles (multiple choice, Likert scales, and open-ended questions) to collect participants’ subjective and lived experiences. To achieve maximum clarity, the use of text boxes allowed participants to further elaborate on their experiences and give richer insight. A draft survey was piloted with 10 males to seek feedback on clarity of questions, survey function and completion time. A ‘think aloud’ approach was used to assess cognitive validity of the survey (Wolcott and Lobczowski, 2021). In response, phrasing changes were made to questions about body composition, and the question about measurement of testosterone levels was changed to a free-text response to allow for the varied, unique responses to be captured. As this was an exploratory survey, test–retest response was not measured.
Data collection was conducted between May and September 2024. Participants were asked a total of 44 questions based on their experiences in the following categorised topics: access, season and duration (nine questions), lifestyle changes (seven questions), supplement intake (four questions), body composition changes (four questions), adverse/side effects (four questions), mood and emotional state/other perceived benefits (six questions), monitoring (four questions) and demographics (six questions). A final question asked participants if there was anything else they wanted to share on their experiences with TB supplements. Respondents were required to read explanatory information about the survey and select a consent tick-box before proceeding to survey questions, with the responses recorded anonymously. To prevent multiple participation in the survey, participants were asked to only complete the survey once and no incentive was provided for completing the survey. Participants could exit the survey at any point before submitting their responses and could selectively opt out of completing questions.
Analysis
Data was exported from Qualtrics to Excel and descriptive analysis conducted. Frequency of responses were reported as absolute numbers and percentages. Some questions allowed participants to select multiple answers therefore, the percentage of responses for some questions could add up to more than 100%. Open text responses were analysed via content or thematic analysis depending on the question (Braun and Clarke, 2013). JE and MM independently reviewed raw responses and assigned inductive codes identified from the data. The two researchers then collectively reviewed their coding and reorganised coding into shared deductive codes that aligned with the research question. Codes were further organised into topics or high-level themes.
Results
Survey response and completion
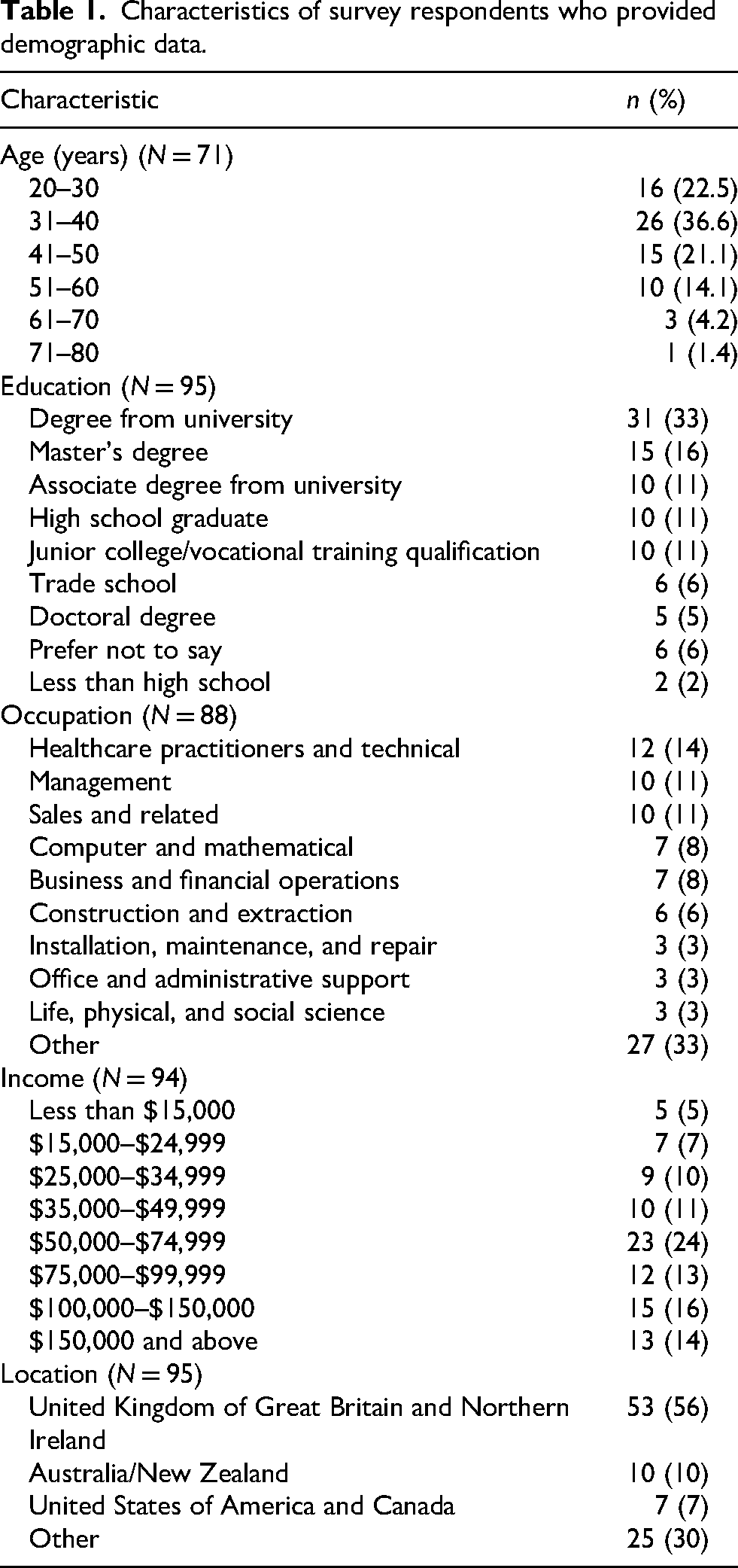
All data from questions answered by participants who entered the survey were included in the analysis irrespective of whether they completed the entire survey. A total of 182 survey participants consented and entered the survey. Participants could selectively respond to questions and therefore the response range for sample sizes was between 182 (100%) and 8 (8%). Refer to supplementary information for sample sizes of each survey section. Characteristics of survey respondents are shown in Table 1.
Characteristics of survey respondents who provided demographic data.
Use of TBs and other supplements
A total of 21 different single ingredient TB supplements were reported to be used by respondents (Table 2). The most common substances reported were tongkat ali (57%, n = 61) followed by Fadogia agrestis (33%, n = 35) and turkesterone/ecdysterone (26%, n = 28). Cistanche (13%, n = 14), ashwagandha (8%, n = 9), shilajit (8%, n = 8), horny goat weed (5%, n = 5) and Tribulus terrestris (5%, n = 5) were used by a smaller proportion of respondents.
Reported usage of single ingredient testosterone booster supplements (N = 111).a
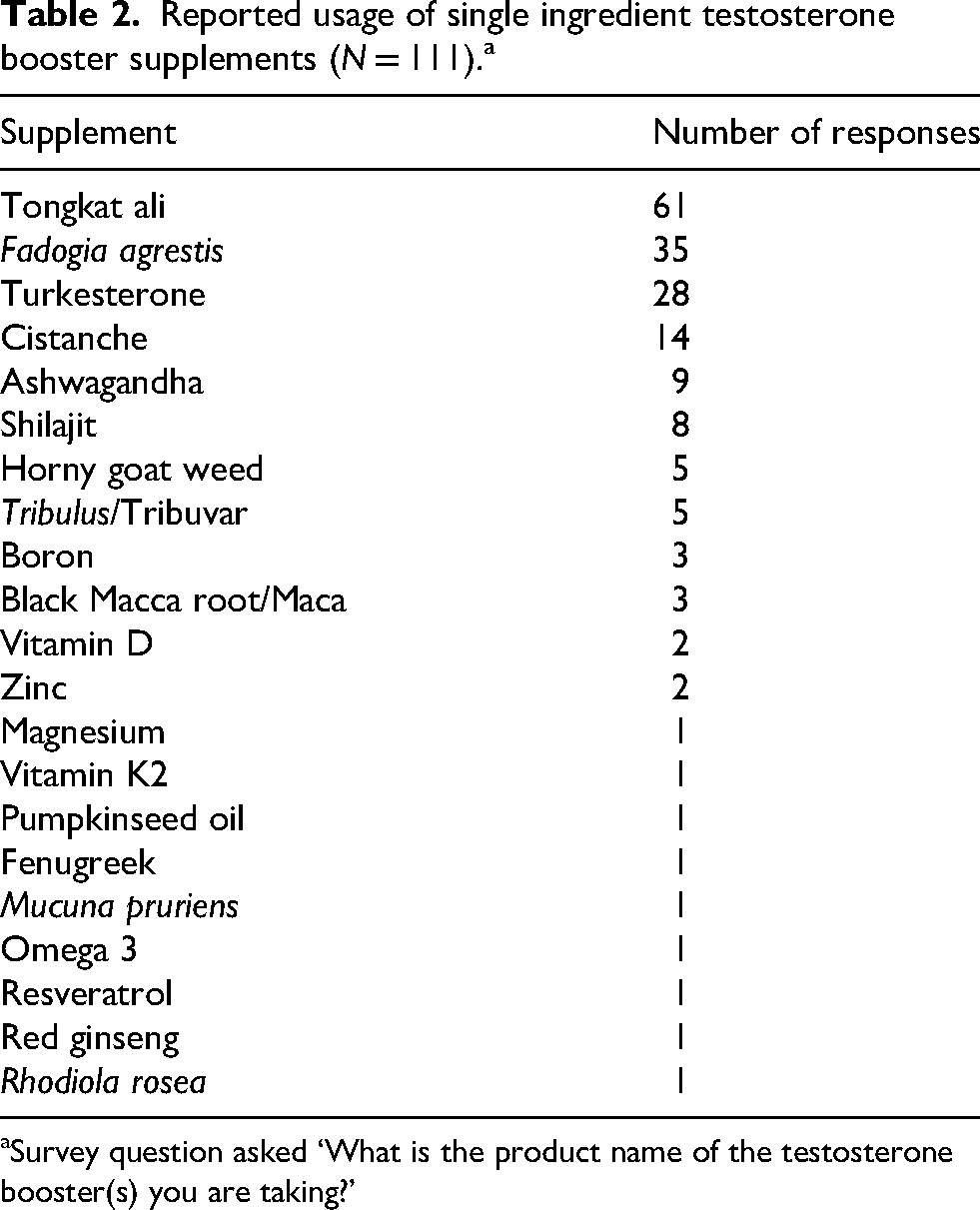
Survey question asked ‘What is the product name of the testosterone booster(s) you are taking?’
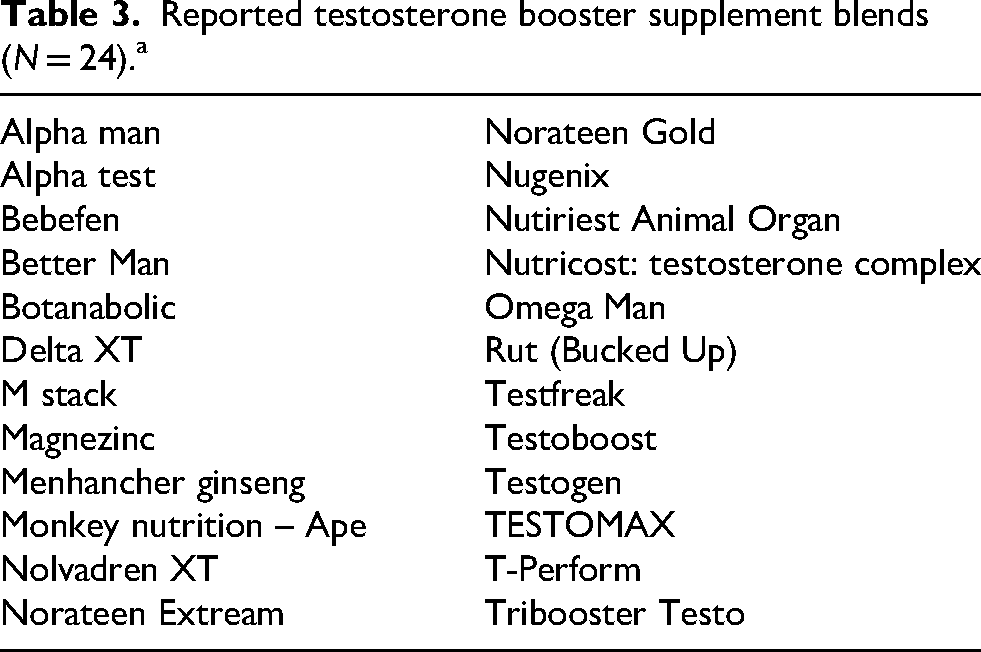
There were 24 supplement blends reported with no single blend reported more than once in the survey (Table 3). Use of supplement stacks (poly-supplementation of more than two TB supplements) was reported by 50 (47%) respondents.
Reported testosterone booster supplement blends (N = 24).a
A third of study participants (36%, n = 43) had been taking TB for three months or less and 33% (n = 39) had been taking them for 4–6 months (Figure 1).
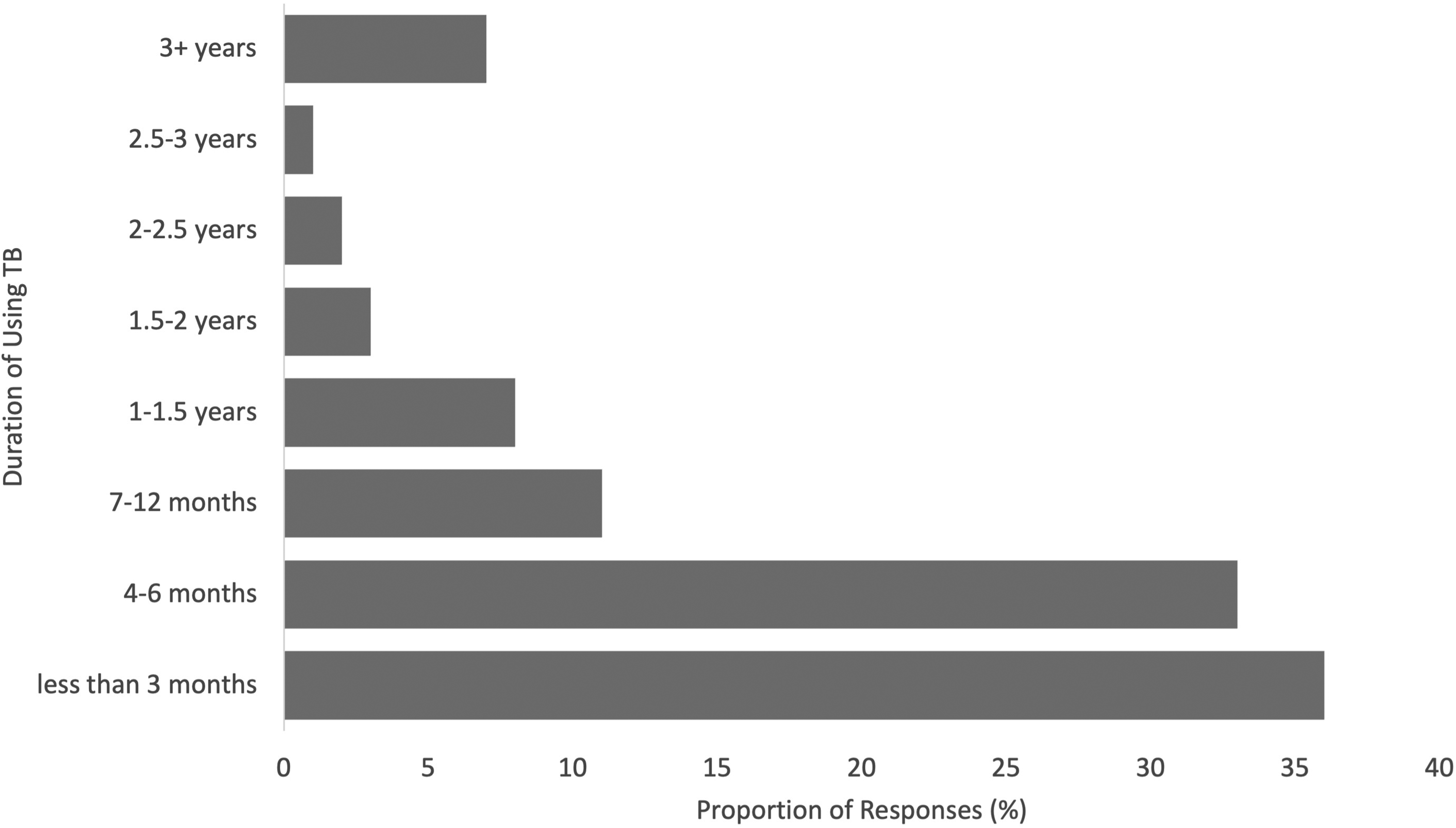
Duration of using testosterone booster supplements (N = 119).
In addition to TB supplements, many participants (57%, n = 60) reported using other supplements at the time they commenced using TB supplements. In total, 34 different supplements were reported including creatine (43%, n = 23), fish oil/omega 3 (33%, n = 17), multivitamin (30%, n = 16), protein/whey protein (24%, n = 13), vitamin D (20%, n = 11) magnesium (20%, n = 11) and zinc (13%, n = 7). Approximately 11% (n = 29) stopped using other supplements when they commenced a TB supplement. However, 28% (n = 29) commenced using additional supplements once they started a TB supplement.
Motivations and purchasing
In addition to the perception of increasing testosterone levels, participants identified a range of other reasons for using TB supplements (Figure 2).
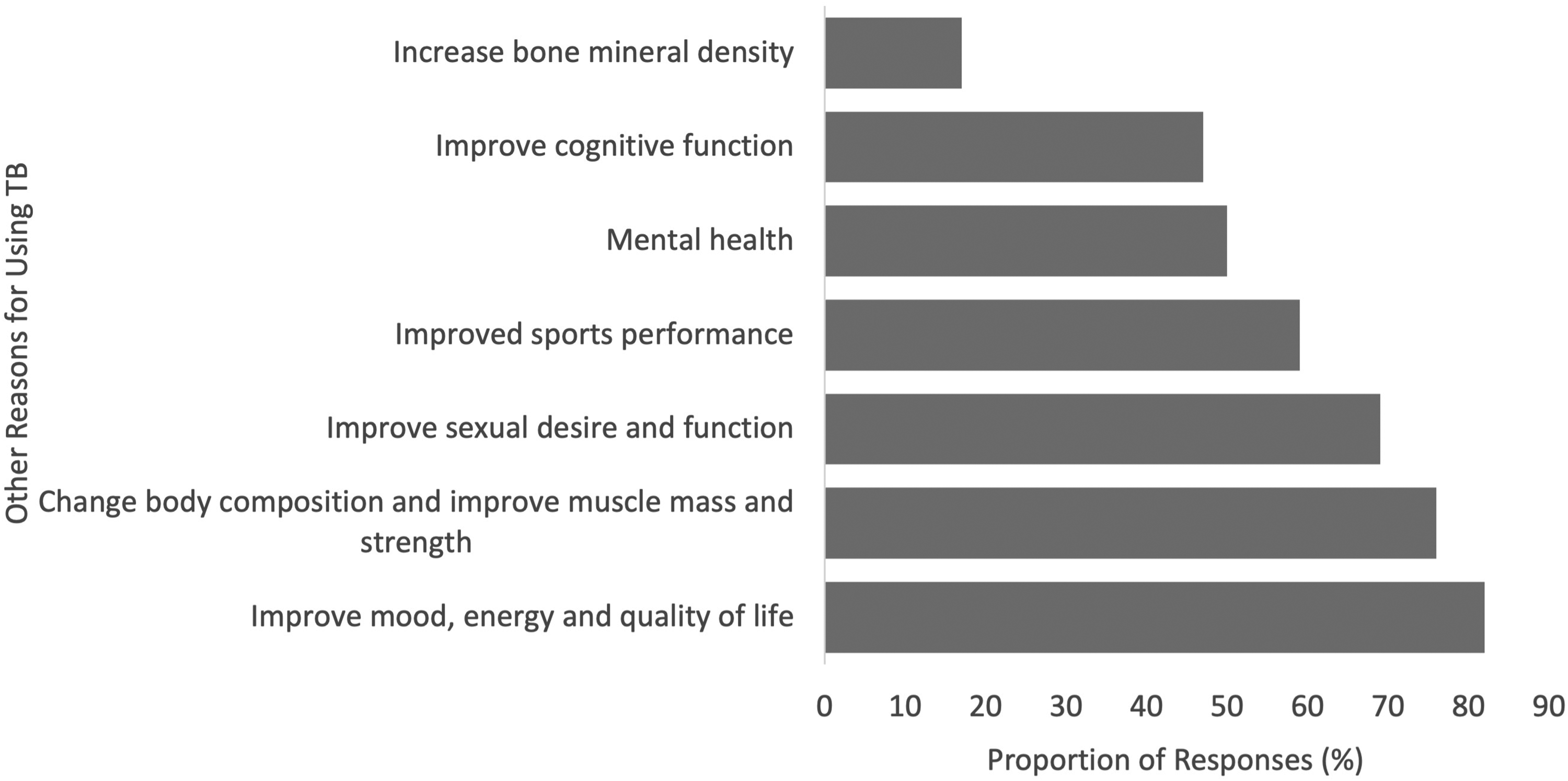
Reported reasons for using testosterone booster supplements (additional to increasing testosterone) (N = 92).
The most common sources of information about TB supplements were social media (35%, n = 63) followed by websites (13%, n = 24), podcasts (12%, n = 22) and YouTube videos (10%, n = 18). Other sources of information (14%, n = 26) were own research, receiving recommendations from others or receiving direct marketing from supplement companies. Open text responses identified two individual social media/podcast accounts (The Huberman Lab, The Joe Rogan Experience) as key influences informing decision-making about use of TB supplements. The most common route for the purchase of TB supplements was online retail outlets (73%, n = 87), followed by dietary supplement shops (13%, n = 16), health food shops (6%, n = 7) and other locations (7%, n = 9).
Perceived benefits of TBs
Most participants (64%, n = 76) indicated that the benefits they gained from TB supplements aligned with their expectations. Open text responses indicated satisfaction with the results achieved from a TB supplement and a desire to continue to use them, e.g., ‘I believe certain ingredients really help. I’m going to finish my bottle of x and start taking pure powder form of certain ingredients’. Some participants experienced better results than expected, ‘I was always under the impression that testosterone boosters didn’t work, and they were all a marketing ploy. After taking the x tablets for a month and having experienced an increase in mood and energy I feel my opinions on them have changed’. Approximately 24% (n = 28) of participants were unsure if they had gained any benefit. This was expressed in open text responses such as ‘Whilst I do feel better, I can't be sure that it isn't a placebo given that I never measured my T-levels before starting. That said, philosophically speaking, even if it is a placebo, if the effect feels real, then I don't think it really matters whether the boosters are actually doing anything’. A smaller proportion of respondents (13%, n = 15) indicated they did not experience the benefits they were expecting.
Approximately one quarter (24%, n = 23) of respondents reported measuring their testosterone levels before starting TB supplementation and 20 respondents indicated how they monitored these. Eleven study participants (55%) used a general practitioner or endocrinologist, three (15%) used a general practitioner at a clinic, two used an at home hormone test (10%), two used some other method (10%) and two (10%) were not monitoring. A total of 10 survey respondents reported their testosterone levels before they started the TB supplement and after a non-specified period of use. All reported an increase in testosterone levels. The magnitude of increase in self-reported values ranged from 2.9 to 34.5 nmol/L.
Over two thirds (66%, n = 68) of respondents reported perceived changes in body composition when taking a TB supplement. Most commonly, a perceived increase in muscle and decrease in body fat was reported (Figure 3).
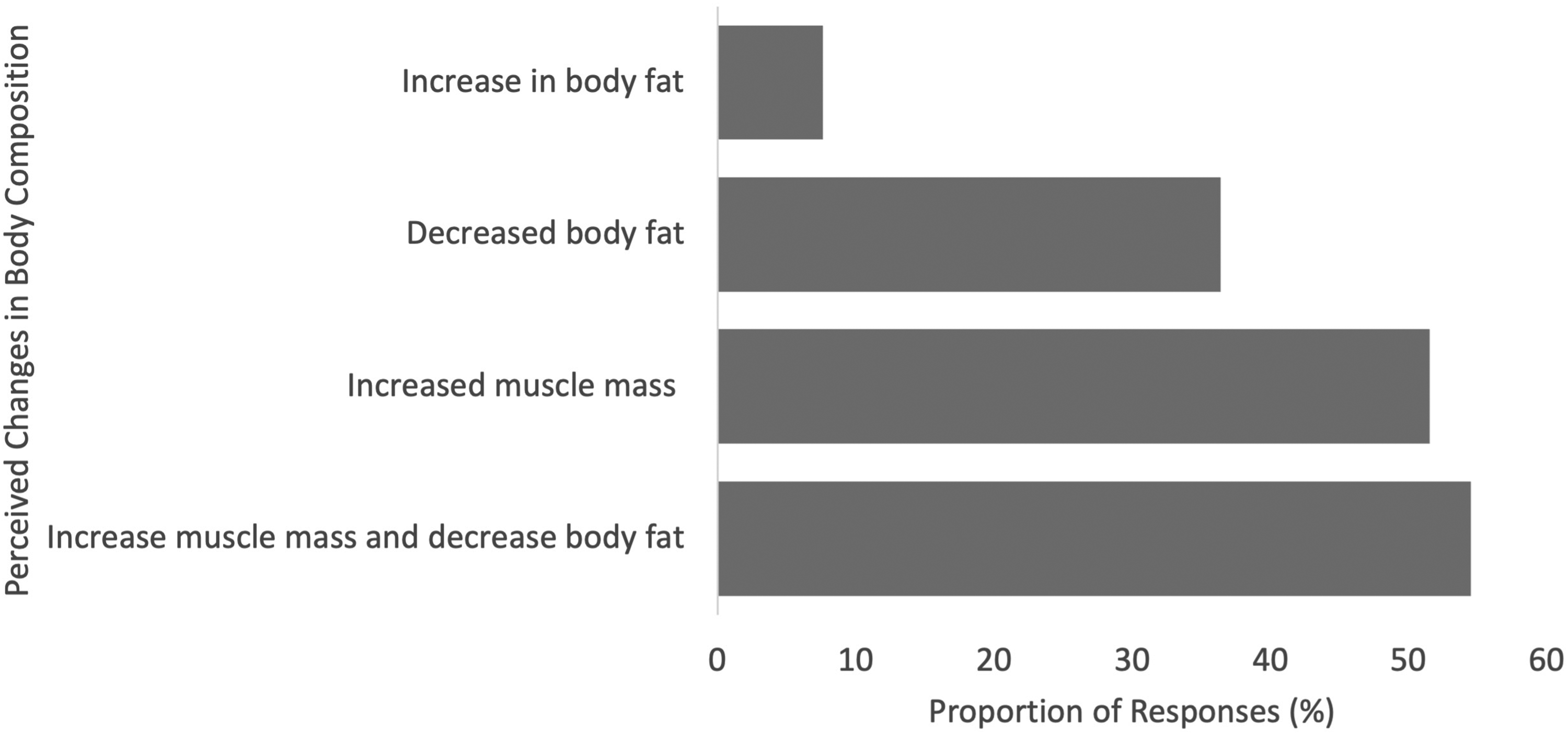
Reported perceived changes in body composition (N = 68).
From our content analysis, body composition changes were typically assessed subjectively via visual inspection (31%, n = 21). Only a small number of respondents had objectively measured body composition changes via bioelectrical impedance (10%, n = 7), girth measurements (9%, n = 6) or surface anthropometry (3%, n = 2). Just under two thirds (62%, n = 62) of survey participants reported experiencing changes to mood and emotional state. Eight respondents reported on anger levels with 50% (n = 4) reporting a slight increase. Slight increases in sex drive/libido (56%, n = 25) and slight (49%, n = 4) or significant increase (44%, n = 22) in energy levels was reported.
Lifestyle changes
Since starting TB supplements, 56% (n = 65) of survey participants reported they had made improvements to their lifestyle, in particular, to physical activity (92% n = 60) and dietary intake (68%, n = 44). Over one third (38%, n = 21) of survey participants significantly increased their physical activity levels, 46% (n = 25) slightly increased their physical activity levels, and 16% (n = 9) remained the same. Regarding dietary changes, 45% (n = 19) of survey participants strongly agreed they were eating healthier since taking a TB supplement, 43% (n = 18) somewhat agreed, and 12% (n = 5) neither agreed nor disagreed. Other lifestyle changes since taking the TB supplement included improvements to alcohol intake (94%, n = 16), stress (47%, n = 8), cigarette smoking (29%, n = 5), and recreational drug use (29% n = 5). Open text responses indicated that lifestyle changes typically coincided or preempted the decision to commence using a TB supplement. For example, ‘I believe I made my dietary and exercise decisions at about the same time that I started taking the testosterone supplement’, and ‘my lifestyle changes happened before boosters. I became a bodybuilder first then implemented the boosters to attempt to improve muscle acquisition and retention’.
Side effects
Approximately one quarter (25%, n = 25) of survey participants experienced a side effect since starting the TB supplement. The most common side effect was gastrointestinal upset (n = 8) including stomach pain/upset, diarrhoea and vomiting (with four responses identifying tongkat ali as the specific supplement). Other reported side effects were nausea (n = 4), mastalgia (n = 2), headache and sleep disturbance. When asked if the side effect made them question the benefit of using the TB supplement, 4% (n = 1) strongly agreed, 16% (n = 4) somewhat agreed, 40% (n = 10) neither agreed nor disagreed, 20% (n = 5) somewhat disagree and 20% (n = 5) strongly disagreed.
Discussion
This study investigates the lived experiences of males taking TB supplements. Notable findings include the wide array of TB supplements reported by participants with only a few of these currently having evidence of efficacy. Interestingly, the majority of survey participants felt they had gained expected benefits from using a TB supplement, despite taking multiple supplements at the same time and making concomitant lifestyle changes. Participants reported perceived benefits to body composition but also to mood and emotional state.
Respondents in our survey reported using an array of TB substances, and often multiple TB substances concurrently, in order to increase testosterone. Reviews of the efficacy of TB supplements to increase testosterone indicate that evidence is sparse, conflicting and affected by methodological limitations (Aguilar-Morgan et al., 2022; Lazarev and Bezuglov, 2021; Smith et al., 2021). However, there is some evidence linking tongkat ali, purified shilajit extract and ashwagandha to increased total testosterone levels in males (Aguilar-Morgan et al., 2022; Leisegang et al., 2022; Pandit et al., 2016). Tongkat ali was used by 57% of participants but shilajit (7.5%) and ashwagandha (8.4%) were less utilised. Interestingly, a number of TB substances with low or no evidence-base were also utilised. Fadogia agrestis was used by 33% of participants. However, there is only one study investigating the effects of Fadogia agrestis on testosterone and this was conducted on rats (Yakubu et al., 2005). Cistanche was used by 13%, however currently no human trials have investigated the capacity of this substance to increase testosterone levels. Horny goat weed (5%) and Tribulus (5%) were reported by less participants. This might reflect decreased marketing of these substances in recent years in response to negative research findings. For example, a 2014 systematic review from Qureshi et al. (2014) concluded that Tribulus terrestris is ineffective for increasing testosterone levels in humans. This has been confirmed with a more recent study concluding 770 mg of Tribulus terrestris in cross fit athletes had no effect on total testosterone after 6 weeks training (Fernández-Lázaro et al., 2021). The evidence for horny goat weed is limited to erectile dysfunction with evidence suggesting it is beneficial for this condition (Nishimatsu et al., 2014; Punyawudho et al., 2013) but there is low-quality evidence for increasing total testosterone (Kuchakulla et al., 2021). The efficacy of many of the other substances utilised by participants to increase testosterone needs to be tested, to better inform consumers about the products they are choosing. The effect of using combinations of TB substances also needs to be considered.
Respondents were primarily motivated to use TB supplements to increase testosterone and improve muscle mass and strength. However, they were also seeking improved mood, mental health, energy, quality of life, and sexual desire and function. The average age of survey participants was 40.1 (±11.9) years with the 31–40-year age group the highest representative group which may coincide with an age where males start to notice declines in physical and health parameters. The motivations reported for using TB supplements are similar to the benefits experienced by males using TRT (Ide, 2023; Matsumoto, 2019). The finding also corresponds with research from Bailey et al. (2013) which found some of the reasons for taking dietary supplements include to increase energy and improve mental health.
Participants in our study were most influenced by online media including social media, websites, podcasts and YouTube. Other research also identifies that supplement use in the fitness industry is strongly driven by social media influencers (Puliyath and Av, 2024). Participants in our study identified two podcasts (The Huberman Lab and The Joe Rogan Experience) as pivotal sources of information and key motivators for sparking interest in TB supplements. Andrew Huberman's appearance on The Joe Rogan Experience on testosterone optimisation (Rogan, 2021) has had over 5.4 million views on YouTube and the full episode from July 2021 has had over 301,000 views as of May 2025. Andrew Huberman's (The Huberman Lab) The Science of How to Optimize Testosterone & Estrogen episode from April 2021 has over 2.3 million views and over 2900 comments (Huberman, 2021). It is likely shortened clips of these episodes have proliferated on various social media platforms including Facebook, Instagram, Reddit and TikTok. Further investigation to measure the influence of social media on consumer behaviour relating to use of TB supplements is warranted.
Few respondents had actually measured their testosterone levels before and during using TB supplements. The small number who had tested their levels via medical or self-kit pathways reported that their values were higher after commencing use. This data needs to be considered with high caution as testosterone levels vary for many reasons. For example, total testosterone should be measured in the morning after an overnight fast between 8 and 10am (Guzelce et al., 2022; Yeap et al., 2016). There may be seasonal variation in total testosterone levels with higher levels measured in summer/autumn and lower levels in winter/spring (Zornitzki et al., 2022). Changes in body mass index (MacDonald et al., 2010), exercise and dietary intake (Whittaker, 2023; Whittaker and Wu, 2021) may all influence total testosterone levels. A difference in values at two different timepoints does not provide evidence for efficacy of TB supplements. Respondents also reported concomitant changes in other supplement use and various lifestyle factors that could also contribute to changes in testosterone. TB supplements need to be objectively tested under well-controlled conditions to determine if they directly or indirectly increase testosterone.
Most respondents in our survey perceived that they had gained muscle mass and reduced body fat as a result of using TB supplements. These findings need to be considered cautiously as few participants had objectively measured body composition by recommended methods and TB supplement use typically coincided with other lifestyle changes. If TB supplements increase testosterone, it makes sense that body composition would improve. Mouser et al. (2016) investigated the association between testosterone levels in males, and lean mass and fat mass. They found men with total testosterone levels in the highest 25% (fourth quartile) had more lean mass and fat mass than those in the 1st quartile. Currently there is limited evidence to indicate that TB supplements significantly change body composition when taken alone. However, some evidence indicates positive body composition changes when some TB substances are combined with resistance exercise. For example, Isenmann et al. (2019) conducted a 10-week trial investigating the effect of ecdysterone and strength training on body composition in 46 young men (25.6 ± 3.7 years). Doses of 200 and 800 mg of ecdysterone, were compared to a placebo. Body composition was measured via bioelectrical impedance analysis (BIA) at baseline and week 10. No significant difference in muscle mass was observed between placebo and 200 mg ecdysterone. However, the increase in muscle mass was statistically higher in the 800 mg group (2.03 ± 1.76 kg). The coefficient of variation for BIA measurements and least-significant change required to indicate a meaningful magnitude of change in BIA measurements was not reported, limiting the ability to interpret this data. However, it is possible that some TB supplements contribute to improvements in body composition when combined with resistance training. For ashwagandha, one study investigated changes to body fat percent. Wankhede et al. (2015) undertook an 8-week trial on 57 young males. Groups were randomised to take either 600 mg of ashwagandha root extract or a placebo in conjunction with 8 weeks of resistance training. Body fat percentage (measured by BIA) reduced by approximately 3.5% in the ashwagandha group (p = 0.05) compared to approximately 1.5% in the placebo group. While some evidence links some TB supplements to improved body composition, the majority of supplements used by respondents are yet to be tested.
In addition to improvement in body composition, respondents in our study attributed changes in mood and emotional state, energy and libido to use of TB supplements. An analysis of the top 50 TB supplements on Amazon Marketplace found the three most common claims for these products were ‘boost/supports testosterone’, ‘increases muscle mass’ and ‘increases energy’ (Singh et al., 2023). Other literature identifies benefits of TB supplements as improvements in energy, increased libido, mental alertness and mood (Balasubramanian et al., 2019; Maheshwari et al., 2017). A small body of evidence supports the efficacy of some TB supplements to influence factors such as energy and libido. For example, an 8-week study investigating the effect of 600 mg of ashwagandha versus a placebo in adults males with lower sexual desire found a statistically significant increase in total DISF-M (Derogatis interview for sexual functioning-male) scores but non-significant increases in scores assessing energy/fatigue, general health and quality of life (Chauhan et al., 2022). A 2017 systematic on Eurycoma longifolia (tongkat ali) identified seven studies showing an association between its use and efficacy in the treatment of male sexual disorders (Thu et al., 2017). Study subjects included both healthy, hypogonadic and stressed males. Overall, they found the herbal supplement improved erectile dysfunction (ED), male infertility and low libido. One study investigating the effect of combined cistanche and ginkgo extracts on chronic fatigue syndrome symptoms and sexual life quality found significantly decreased physical and mental fatigue scores and improved quality of life and sexual life quality scores in 190 men (Kan et al., 2021). Tribulus terrestris has been found to aid in sexual function in males with ED and hypoactive sexual desire disorder (HSDD) (Kamenov et al., 2017; Leisegang and Finelli, 2021). There are no human studies investigating Fadogia agrestis but it has shown to significantly alter sexual behaviour patterns in animal studies (Saikia et al., 2024). The effect of other TB supplements reported in this survey on characteristics such as mood, energy and libido is untested.
Just over half (56%) of survey participants reported making changes to their lifestyle while using TB supplements. Changes primarily included increasing physical activity levels and making healthier food choices but also extended to reducing alcohol consumption, cigarette smoking and recreational drug use for some respondents. This aligns with literature that links lifestyle improvements to supplement use. For example, Alhazmi et al. (2023) reported a higher percentage of supplement users with higher daily physical activity compared to those who reported no physical activity and Burnett et al. (2017) reported those who met physical activity guidelines are also more likely to take dietary supplements. Users of dietary supplements have also been characterised as having healthier lifestyle behaviours, being more health conscious (Kofoed et al., 2015) and consuming higher quality diets compared to supplement non-users (Burnett et al., 2017). These findings are not specific to TB supplements, so it is unknown whether the initiation of TB supplements is a conduit to improved lifestyle characteristics.
Approximately 25% of respondents in our survey reported side effects linked to use of TB supplements. These were primarily minor gastrointestinal effects that align with common side effects reported in clinical trials of TB supplements. For example, a study of 105 male subjects (aged 50–70 years) were given either tongkat ali (Eurycoma longifolia (Physta®) of 100 mg group, 200 mg group or placebo daily for 12 weeks. Side effects (constipation, dyspepsia, abdominal pain, flatulence and abdominal discomfort) were reported by three subjects in the 100 mg and three subjects in the 200 mg group. Ashwagandha has been associated with minimal side effects in clinical trials of 300–1250 mg/day in healthy subjects over periods spanning 4–8 weeks (Lim and Barnes, 2024; Raut et al., 2012; Verma et al., 2021). Two recent reports have presented case studies of adverse effects experienced from people taking ashwagandha outside of clinical research settings (Björnsson et al., 2020; Philips et al., 2023). Side effects resulting from use of other TB supplements reported in our survey are undocumented. Respondents who experienced side effects were divided as to whether the side effect deterred them from continuing to use TB supplements. This perhaps indicates the mild nature of symptoms experienced. Blood examination of renal and liver function may reveal adverse effects that are not apparent as self-reported symptoms. Given a quarter of survey participants experienced a side effect, caution is advised when taking TB supplements and careful monitoring of adverse events is recommended in future studies.
This was an exploratory survey capturing self-reported information at a single point in time. Limitations of this study include a small sample size compared to the market size of TB supplement users and an unequal distribution of responses from different geographical locations. As most respondents were from the United Kingdom, Australia and United States of America, there is a bias towards developed countries. Our survey was open to any male who had used TB supplements at any point in time so males with negative experiences who did not continue to use TB supplements were included. However, we recognise that people with positive experiences were more likely to complete the survey. We invited males to participate and did explicitly identify nor exclude individuals who were assigned female at birth but identify as male. Respondents reported using a variety of TB supplement products, sometimes in conjunction with other supplements, hence the reported benefits and side effects should be interpreted with caution. Participants concurrently taking TRT or anabolic–androgenic steroids in addition to TB supplements were not explicitly excluded which may confound the interpretation of our findings. We allowed respondents to self-report testosterone levels via free-text in a way that was meaningful to them. Sufficient details about collection and analysis protocols were not captured to validate self-reported values.
To conclude, in this study we investigated the motivations, experiences, perceptions and behaviours of males who had used TB supplements to increase testosterone levels. Use of a wide range of TB substances were reported with only a small number of reported substances having evidence of efficacy in a limited number of studies. Most survey participants perceived they had gained the expected benefits from these supplements despite concomitant use of other dietary supplements, instigation of lifestyle change and lack of objective measurement of effects. Perceived benefits included positive body composition changes and improvements to energy and libido.
Supplemental Material
sj-docx-1-nah-10.1177_02601060261431124 - Supplemental material for The experiences and perceptions of males using testosterone booster supplements – An exploratory cross-sectional survey
Supplemental material, sj-docx-1-nah-10.1177_02601060261431124 for The experiences and perceptions of males using testosterone booster supplements – An exploratory cross-sectional survey by Julian Everett, Michelle Minehan, Stephan Praet and Andrew McKune in Nutrition and Health
Supplemental Material
sj-docx-2-nah-10.1177_02601060261431124 - Supplemental material for The experiences and perceptions of males using testosterone booster supplements – An exploratory cross-sectional survey
Supplemental material, sj-docx-2-nah-10.1177_02601060261431124 for The experiences and perceptions of males using testosterone booster supplements – An exploratory cross-sectional survey by Julian Everett, Michelle Minehan, Stephan Praet and Andrew McKune in Nutrition and Health
Supplemental Material
sj-docx-3-nah-10.1177_02601060261431124 - Supplemental material for The experiences and perceptions of males using testosterone booster supplements – An exploratory cross-sectional survey
Supplemental material, sj-docx-3-nah-10.1177_02601060261431124 for The experiences and perceptions of males using testosterone booster supplements – An exploratory cross-sectional survey by Julian Everett, Michelle Minehan, Stephan Praet and Andrew McKune in Nutrition and Health
Footnotes
Acknowledgements
I wish to express thanks to all individuals who shared my survey within their networks.
Ethical considerations and consent to participate
Ethics approval was granted by the University of Canberra Human Research Ethics committee (no: 13598). Participants were required to read explanatory participant information about the survey and select a consent tick-box before proceeding to survey questions, with the responses recorded anonymously.
Consent for publication
All authors have read and agreed to the published version of the manuscript.
Authors’ contributions
Conceptualisation: J.E. and M.M.; methodology: J.E., M.M., and A.M.; data curation: J.E.; validation: J.E., M.M., and A.M.; formal analysis: J.E. and M.M; investigation: J.E. and M.M.; methodology: J.E., M.M. and A.M.; project administration: J.E.; writing – original draft: J.E.; writing – review and editing: J.E., M.M., A.M., and S.P.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.