
Abstract
Background
Significant variations in breastfeeding initiation and continuation exist in different global communities. Understanding women's attitude and experiences about breastfeeding within different communities is important to inform optimum infant feeding practices.
Aim
To explore breastfeeding practices and gain insights into women's practices, knowledge and beliefs concerning infant feeding in West Sumatra, Indonesia.
Methods
A mixed methods study was undertaken. Breastfeeding data were collected from mothers at birth, 6 weeks, 6 and 9 months of infant's age within a feasibility study of antenatal nutritional supplementation in West Sumatra (n = 158). Additionally, a convenience sample of mothers (n = 19) undertook qualitative semi-structured interviews. Interviews were analysed thematically.
Results
While only 84.2% of infants were exclusively breastfed within the 24 hours prior to hospital discharge, 93.7% of infants at 6 weeks and 64.7% at 6 months were exclusively breastfed. At 9 months 92.9% of infants continued to breastfeed. Qualitative interviews generated three overarching themes: (1) ‘Mothers’ attitude’. Women viewed breastfeeding as normal and natural and strongly valued the health benefits of exclusive breastfeeding. (2) ‘Cultural perspectives’ showed breastfeeding was the default choice within the women's communities. (3) ‘Family and social support’ found women received good family support and encouragement to breastfeed.
Conclusion
The exclusive breastfeeding rate of 64.7% and any breastfeeding rate of 96.0% at 6 months in West Sumatra is noteworthy. Cultural values, family and social support along with a positive attitude reinforced by information and knowledge regarding breastfeeding appeared to catalyse high rates of breastfeeding. Further international comparative studies to provide insights into the underpinning social and belief constructs that may contribute to these positive health behaviours (or lack of it in other communities) is worthy of further investigation.
Introduction
Exclusive breastfeeding is recommended for the first 6 months of a child's life, with continued breastfeeding alongside consumption of supplementary foods up to 2 years of age or beyond (World Health Organization, 2021). Globally, only 48% of infants aged 0 to 5 months are exclusively breastfed, with breastfeeding rates decreasing with increasing age from 0 to 5 months (UNICEF, 2023). In the most recent Indonesia demographic health survey, 67% of infants were exclusively breastfed at 1 month, 38% exclusively breastfed at 4 to 5 months, and nationally 55% of infants received some breastmilk until age 2 years (National Population and Family Planning Board (BKKBN), Statistics Indonesia (BPS), Ministry of Health (Kemenkes) and ICF 2018).
Adequate nutrition in early life is vital, with breastfeeding providing optimal nutrition and unique health benefits (Eidelman et al., 2012; Victora et al., 2016). Extensive research has shown that breastmilk has a protective effect against infant sickness, including reduced rate of hospitalisations for diarrhoea and respiratory infections (Lessen and Kavanagh, 2015; Victora et al., 2016) and a lower mortality rate (North et al., 2022). This is of importance in Indonesia as infant mortality is a major public health issue. The latest Indonesia Demographic and Health Survey indicated the mortality rate among children under 1 year to be 24 per 1000 live births, and the neonatal mortality (death in the first 28 days of life) to be 15 per 1000 live births, equating to 1 in 67 children dying within the first month of life (BKKBN, BPS, Kemenkes and ICF, 2018). Additionally, the advantages of breastfeeding continue into adulthood with a lower risk of obesity and diabetes in later life (Victora et al., 2016). The benefits of breastfeeding are not just limited to the infant, research has indicated a decline in breast and ovarian cancers, type two diabetes and endometriosis in women who breastfeed (Farland et al., 2017; Modugno et al., 2019; Victora et al., 2016).
In Indonesia, 36.7% of under 5-year-olds suffer from stunting, signalling the necessity for adequate nutrition early in life (Rachmi et al., 2016). That study suggested that Indonesian infants breastfed for 6 months or more were more likely to be stunted or underweight (Rachmi et al., 2016). However, other studies suggest infants are more likely to be undernourished if they are not exclusively breastfed (Ananta et al., 2016) and in areas with higher proportions of infants not receiving any breastmilk from 0 to 23 months (Perdani et al., 2021), in particular among low income women (Hadi et al., 2021).
Many factors have been indicated to improve rates of breastfeeding. Mothers with a higher level of education have been demonstrated to improve rates of breastfeeding in the United Kingdom (McAndrew et al., 2012). To date, there has been little agreement on whether this result is replicated in Indonesia, with some studies reporting a correlation between high education levels and shorter durations of any or predominant breastfeeding (BKKBN, BPS, Kemenkes and ICF, 2018). Conversely, other studies have shown increased exclusive breastfeeding among women receiving any level of formal education compared to no education (Laksono et al., 2021). Other factors that have also been shown to influence breastfeeding rates in Indonesia include employment (Laksono et al., 2021), mode of birth and smoking status (Nurokhmah et al., 2022).
Understanding women's attitudes to and experiences of breastfeeding in different parts of the globe could help in guiding promotional strategies in optimum infant nutrition. This study was therefore aimed to explore breastfeeding practices and gain insights into women's practices, knowledge and beliefs concerning infant feeding in West Sumatra, Indonesia.
Methods
Design
This is part of a feasibility trial aimed to assess the practicality of protocol implementation and acceptability of a food supplementation intervention using a traditional Indonesian yogurt (Dadih) made from buffalo milk during pregnancy. The control group in the study was provided with a gelatine-based pudding with lower fat, protein and calorie content. This intervention was developed in response to the high prevalence of malnutrition during pregnancy in Indonesia, where 20.1% of pregnant women have been found to be underweight (body mass index (BMI) < 18.5 kg/m²) and over 50% of women gain less weight in pregnancy than recommended by the Institute of Medicine (IOM) (Soltani et al., 2017).
Setting
Women were recruited from three areas of West Sumatra: Agam, Padang Panjang and the Lintau Buo district in Tanah Datar from January 2019 to December 2019, with a second wave of recruitment in Padang Panjang from May to September 2020.
Participants
Women were recruited to the feasibility study at their first antenatal clinic appointment. Any woman presenting to antenatal care within the target districts (Agam, Padang Panjang and Lintau Buo) were invited by their midwife to participate in the study through the provision of a participant information sheet. Women willing to participate in the feasibility study signed a consent form. Women were recruited regardless of parity. Exclusion criteria were pre-existing diabetes or a dislike or allergy to Dadih. After inclusion, women were randomly assigned to the intervention or control group using random sequences of block sizes of 2, 4 or 6, and random permutations of group allocation within each block. The intervention group received the high calorie Dadih product from approximately 18 weeks gestation until delivery. Women in the control group received a gelatine-based pudding which was lower in fat, protein, and calorie content than Dadih from approximately 18 weeks gestation until delivery. The feasibility study aimed to recruit approximately 208 women. This was to provide 80% power to detect a reduction in gestational weight gain below IOM recommendations (Rasmussen and Yaktine, 2009) from 57% to 37% with 95% confidence, allowing for a 10% attrition rate. A subsample of 19 women undertook semi-structured interviews, 8 of these had been randomised to the control group and the remaining eleven randomised to the intervention group.
Data collection
Data was collected about breastfeeding status at discharge from hospital, 6 weeks, 6 months and 9 months. Women were asked about exclusive breastfeeding in the previous 24 hours up to 6 months and any breastfeeding in the previous 24 hours and more than 50% of feeds being at the breast in the previous 24 hours at all time points. Exclusive breastfeeding was defined as no nutrition other than breastmilk within the past 24 hours.
Additionally, qualitative semi-structured interviews were undertaken with a convenience subsample of women. The breastfeeding questions employed during the interview can be found in Supplemental File S1. These interviews were undertaken with women individually and occurred when the infant was aged between 9 months and 1 year. During these interviews, women's knowledge and beliefs concerning infant feeding practices were explored. Interviews were conducted in the women's native language, then translated into English by a professional translation service prior to analysis.
Data analysis
Descriptive statistics regarding rate of breastfeeding at each time point were determined. Maternal characteristics including maternal age, BMI, parity, employment outside of the home, educational level and smoking status, alongside mode of birth and infant's birthweight were investigated for any differences in rate of exclusive breastfeeding at discharge, 6 weeks and 6 months and proportion of women who provided more than 50% of feeds at the breast at 9 months. It was not possible to analyse maternal characteristics according to any breastfeeding due to the limited number of women who did not provide any breastmilk within this cohort. Maternal age and infant's birthweight were assessed using independent t-tests. Maternal BMI was not normally distributed, so analysed using the Mann Whitney U test. Binary categorical variables were assessed using Chi Square tests and ordinal categorical variables using the Chi square for trend. Where Chi square test assumptions were violated due to more than 20% of cells having expected counts less than 5, the Fisher exact test was used. p < 0.05 was taken as statistically significant.
For the qualitative data, interview transcripts were transcribed and then coded thematically by one researcher and independently reviewed by two additional researchers. Themes generated within the data were discussed by the research team until consensus was reached. No new themes were identified after interviewing 19 women, so data collection was discontinued.
Ethical implications
Ethical approval was obtained from the ethical committee of the Faculty of Medicine of Andalas University (707/KEP/FK/2019) in January 2019. Informed consent was gained from participants separately for the feasibility study and the qualitative interview component.
Results
In total 229 women were recruited to the feasibility study, with 173 having birth data available and 158 having breastfeeding data available at one or more time points (see Figure 1). Of the 158 women with breastfeeding data, 85 (53.8%) had been allocated to the intervention group and 73 (46.2%) to the control group. The mean gestation at birth within the sample was 39.2 weeks (standard deviation 2.5 weeks). Eight included infants had had a special care baby unit admission prior to hospital discharge.
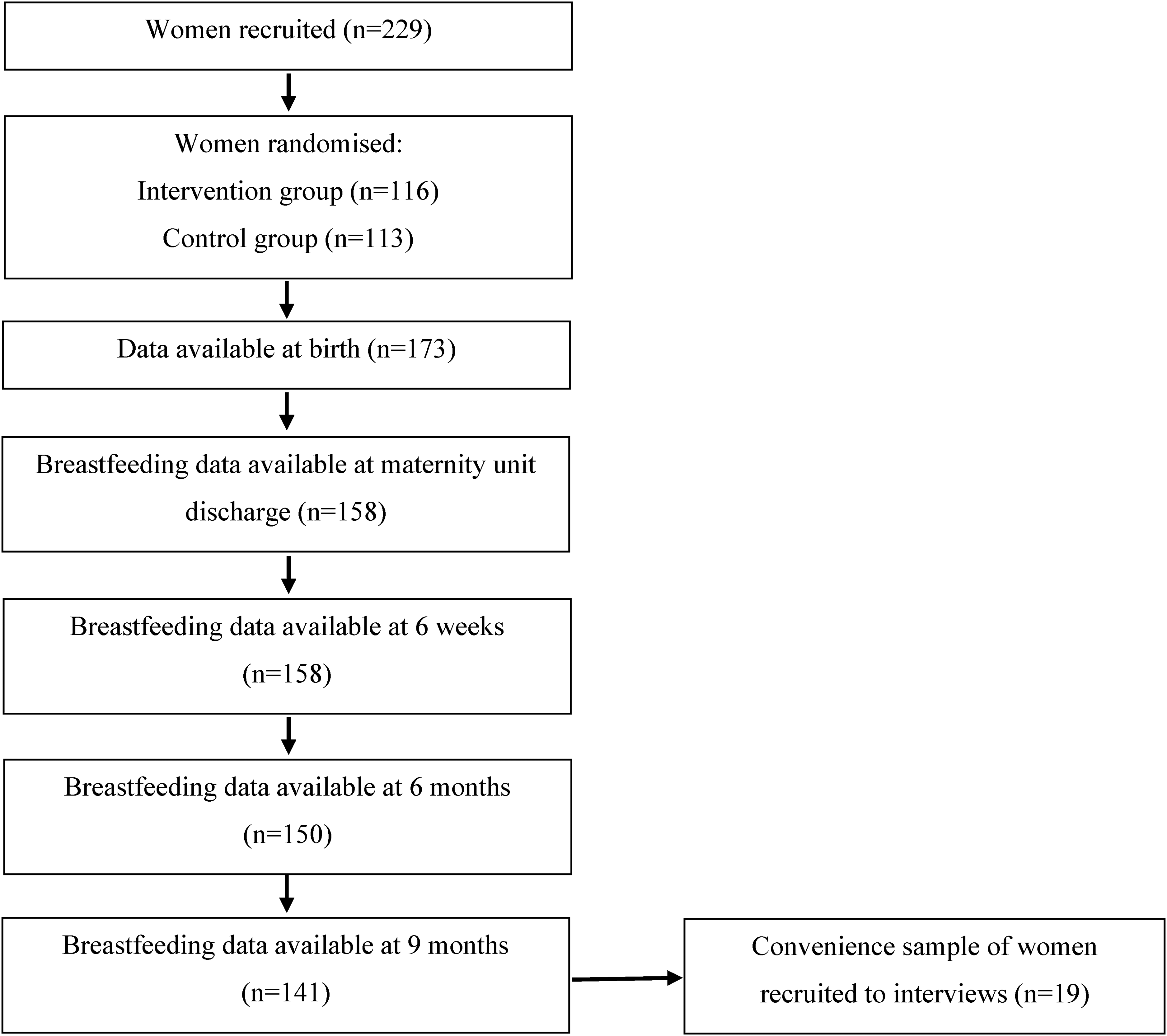
Flow chart of study participation.
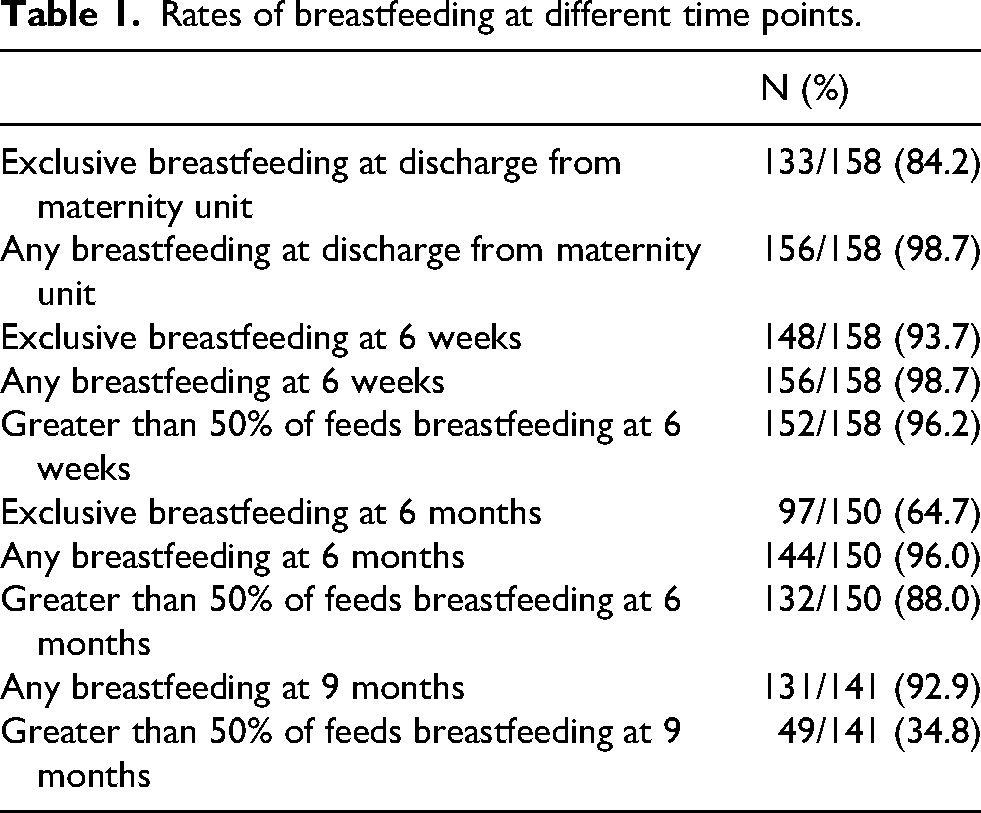
The rate of exclusive, any and more than 50% of feeds at the breast at each time point are given in Table 1. Only 2 women did not undertake any breastfeeding on discharge from hospital or at 6 weeks. And 96% of women continued to provide at least some breastmilk at 6 months, with 64.7% of women exclusively breastfeeding at 6 months.
Rates of breastfeeding at different time points.
The proportion exclusively breastfeeding at discharge, 6 weeks, 6 months or providing more than 50% of feeds at the breast at 9 months according to maternal and infant's birth characteristics are given in Tables 2 and 3. Those with high school or graduate education were significantly more likely to exclusively breastfeed at discharge (p-value = 0.002), but not at other time points. Mothers who smoked were more likely to exclusively breastfeed at discharge (p-value =0.001), but less likely to continue providing more than 50% of feeds at the breast by 9 months (p-value < 0.001). The proportion of women breastfeeding at each time point did not vary according to any other maternal or birth characteristics.
A comparison of maternal and infant characteristics at discharge, 6 weeks, 6 months and 9 months according to breastfeeding status.
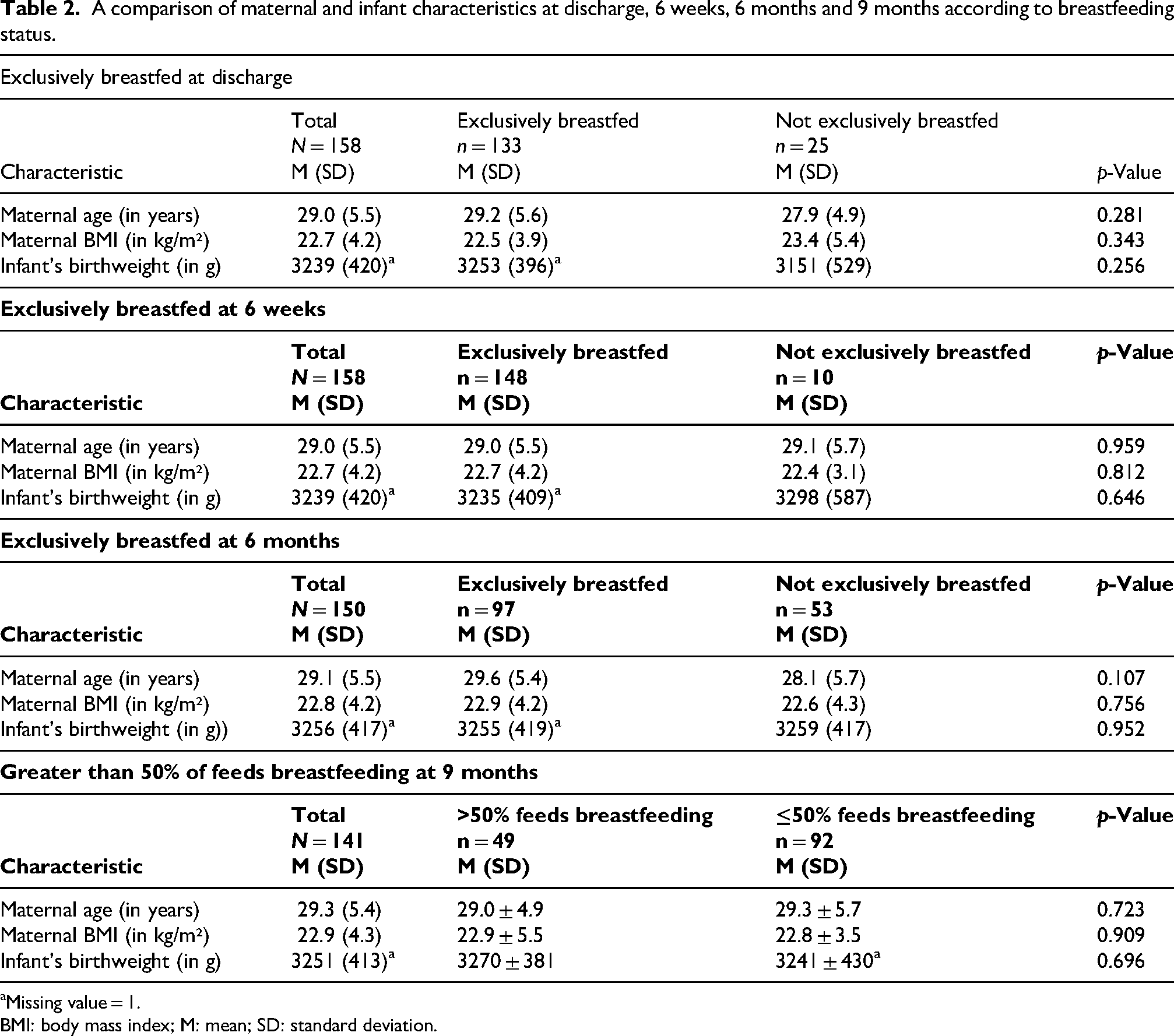
Missing value = 1.
BMI: body mass index; M: mean; SD: standard deviation.
A comparison of maternal background characteristics at discharge, 6 weeks, 6 months and 9 months according to breastfeeding status.
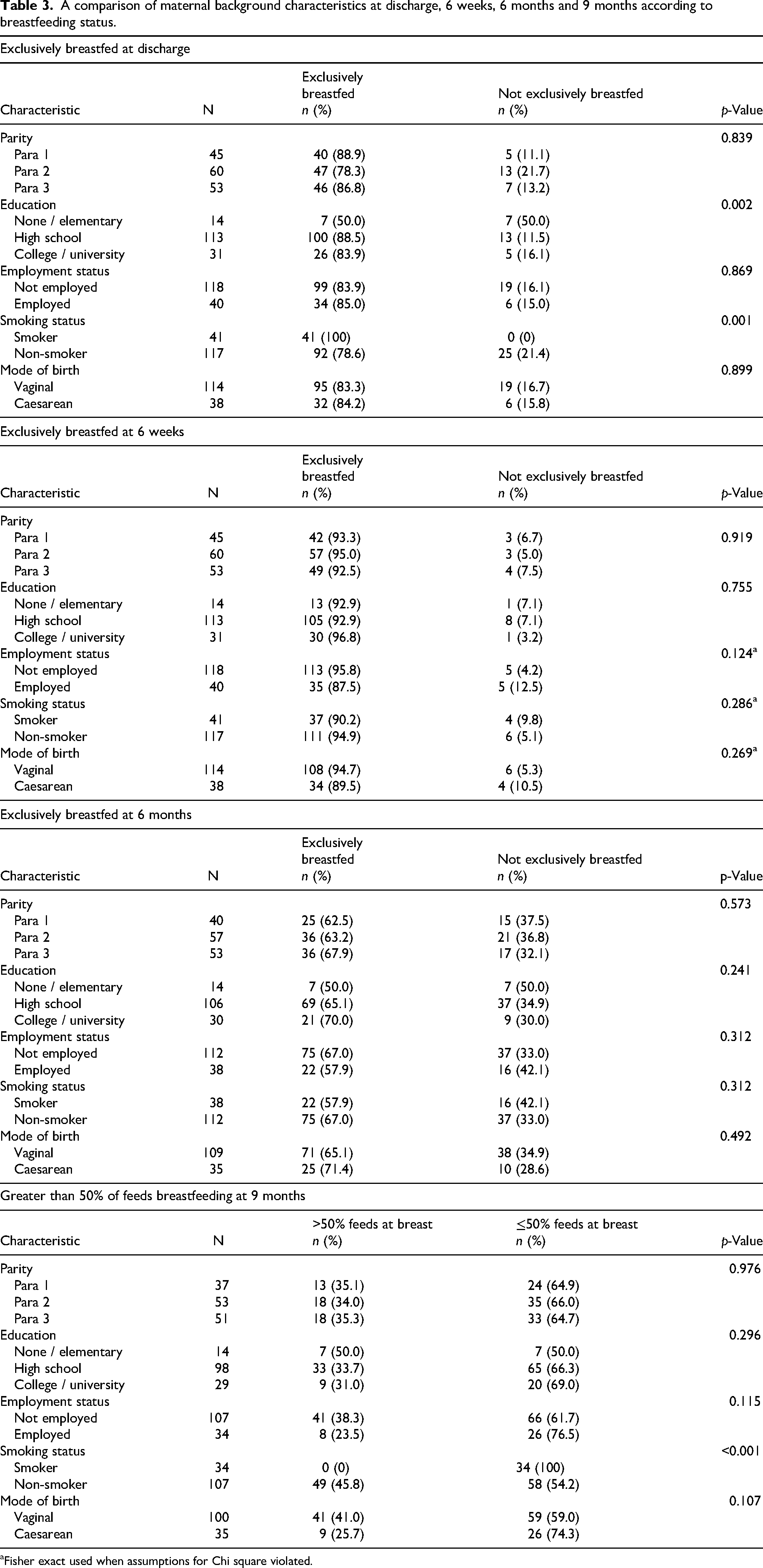
Fisher exact used when assumptions for Chi square violated.
Qualitative results
Three overarching themes were generated from the mothers’ interviews, ‘Mothers’ attitude’; ‘Cultural perspectives’; and ‘Family and social support’.
Mothers’ attitude
There was a very positive attitude and general acceptance of breastfeeding as the best infant feeding method among these mothers. This theme encompassed two subthemes, ‘Belief in the value of breastmilk’ and ‘Baby led complementary feeding’.
Belief in the value of breastmilk
Mothers in this study seemed to have a good level of knowledge and a genuine belief in the benefits of breastmilk from both immunity and nutritional perspectives. The value and importance of exclusive breastfeeding in the first 6 months of life appeared very strongly from the data. “I only gave breastmilk until the age of 6 months because this breastfeeding has benefits such as for immunity, children don't get sick easily.” “Just breastfeed, because XXXX [baby's name] growth has increased, it means that breastmilk is enough.” “I can breastfeed more than 8 times a day, my target is to breastfeed until the age of 2 years because there is a lot of nutrition from breastmilk.” “In my opinion, my baby still needs breastmilk and additional food (rice porridge) at the age of 15 months.”
“I still breastfeed even until now. It’s the baby’s staple food.”
Baby-led complementary feeding
There was a consensus that complementary feeding should begin around 6 months of age, with women showing good awareness that the digestive system may not be adequately developed before this:
“Because breastfeeding alone is not sufficient for children's nutritional needs. If I have been given food before 6 months, I am afraid that the child's intestines will not digest properly. That's why I fed him after he was 6 months old.”
“For me, if the baby doesn't want to eat rice, then replace it with rice porridge. The important thing is the baby eats. For my friends and relatives, if their baby won't eat, they just let it go so that the baby loses weight. But if he doesn't want to eat, I change the menu so he wants to eat, so that his stomach is full.”
“At 7 months I gave him solid food, my son was tired of rice porridge and I introduced him to family food.”
“I tried to feed him at the age of 4 months, but my son didn't want to, he always vomited.”
Cultural perspectives
The majority of participating women expressed no perceived disadvantages with breastfeeding and considered it the normal and natural way to feed their child. The wide cultural acceptance of the superiority of breastfeeding was reinforced by substantial knowledge and information. Women demonstrated very good knowledge of the numerous advantages of breastfeeding, not only for nutrition but also to enhance immune response. They also raised the importance of breastfeeding being of low cost, as well as emotionally advantageous for promoting bonding between mothers and babies: “The advantage is that the immune system is stronger, fever is rare, cheap and simple, no need to pay.”
“The benefits of breastfeeding are clear, the reward is also in practicing my religion [due to Islamic law affirming breastfeeding]. If the children are happy we are also happy. If it is for the child, the child will be stronger, healthier. If we look at children who are given formula [supplementary milk], some are allergic.”
“There are many advantages, the child is full, the child's nutritional intake is fulfilled. There is a bond between the child and the mother.”
“I think my family members, neighbours or friends feed their babies the same way I do. Exclusive breastfeeding remains the same for up to 6 months, after 6 months other foods are introduced.”
Family and social support
The final overarching theme emerging from the data was the importance of family and social support, creating a culture which nurtures mothers and babies. Women saw this support as a catalyst and mediator for a successful breastfeeding experience. Many of the women reported that their husbands and wider family supported and encouraged them to breastfeed:
“So, to facilitate breastfeeding, drink honey and date palm extracts, of course there is support from your husband. My husband even suggested that I should breastfeed until my child is 3 years old.”
“Everyone supports me to breastfeed, especially my husband, parents and the social environment.”
Discussion
The exclusive breastfeeding rate of 64.7% and any breastfeeding rate of 96.0% at 6 months in West Sumatra is noteworthy, given it is higher than in many countries (World Population Review, 2025), and in particular high-income countries (Theurich et al., 2019). Within the qualitative interviews women demonstrated a good level of knowledge about the benefits of breastfeeding and were supported by their families and within their communities to breastfeed.
A high prevalence of any breastfeeding has similarly been reported in various previous Indonesian cohorts, with a very high proportion of infants ever being breastfed consistently noted over time in Indonesia. Within the 2007 Indonesian Family Life Survey, 96.6% of infants were ever breastfed (Rachmi et al., 2016) and 95.0% of infants born within the past 2 years were ever breastfed in the Indonesia Demographic Health Survey in 2017 (BKKBN, BPS, Kemenkes and ICF, 2018). When specifically considering the area of West Sumatra within Indonesia, 97.6% of infants have previously been reported to have ever breastfed (BKKBN, BPS, Kemenkes and ICF, 2018).
Similar rates of exclusive breastfeeding to those found in this research have also been noted previously. The Indonesian National Household Health Survey in 2007 found the rate of exclusive breastfeeding across Indonesia to be 46.3% at 6 months or at the time of survey completion if the infant was less than 6 months (Ananta et al., 2016). The later Indonesia Demographic Health Survey in 2017, found a slightly higher rate of 52.3% of infants aged 0 to 6 months were exclusively breastfed (Gayatri, 2021) and that 77% of infants were still receiving some breastmilk at 1 year of age (BKKBN, BPS, Kemenkes and ICF, 2018). This suggests that Indonesia is well on course regarding the global nutrition target of increasing exclusive breastfeeding for the first 6 months to at least 50% of infants by 2025 (Development Initiatives, 2020). Rates of exclusive breastfeeding at 6 months however varies by region in Indonesia, with only 10.5% of infants in East Java exclusively breastfed at 6 months compared to 66.9% of infants in Jambi (Ananta et al., 2016). Previous estimates in West Sumatra suggested that 56.1% of infants were breastfed exclusively at 6 months of age (Ananta et al., 2016), which was slightly lower than the 64.7% of infants exclusively breastfed at 6 months within this current cohort. It is of particular interest that many infants were exclusively breastfed at 6 months despite the prevalence of early initiation of breastfeeding, defined as within 1 hour of birth, being only 60.9% across Indonesia (Kurniawan et al., 2021), that 43.9% of Indonesian infants are given a feed other than breastmilk in the first 3 days of life (BKKBN, BPS, Kemenkes and ICF, 2018) and that the proportion of women exclusively breastfeeding on discharge from the birthing unit was only 84.2% within this cohort.
Although not significant within this research, women who were employed consistently had lower rates of exclusively breastfeeding at 6 weeks and 6 months, or offering more than 50% of feeds at the breast at 9 months. Employment status has similarly been seen to influence breastfeeding rates in previous Indonesian research, with lower rates of exclusive breastfeeding in mothers who returned to work in Jakarta (Afiyanti and Juliastuti, 2012), urban Central Java (Paramashanti et al., 2022) and across Indonesia (Ananta et al., 2016; Laksono et al., 2021). The 2017 Indonesian Demographic Health survey also found reduced exclusive breastfeeding from 0 to 5 months among woman who worked compared to those who did not work (Gayatri, 2021), particularly in those employed in a non-agricultural setting (Nurokhmah et al., 2022). Other research in West Java has also demonstrated maternal employment outside of the home to be associated with increased supplementation with breastmilk substitutes (Green et al., 2021). Additionally, within this current study, despite that all women who smoked initiated breastfeeding and 57.9% still exclusively breastfed at 6 months, this proportion was lower than for women who did not smoke (67.0%). By 9 months there was a significant difference in breastfeeding according to smoking status with none of the women who smoked still providing more than 50% of feeds at the breast compared to 45.8% of women who did not smoke. The Indonesian Demographic Health Survey has also previously noted that exclusive breastfeeding from 0 to 5 months is reduced among women who smoked (Nurokhmah et al., 2022), with a systematic review of international studies also noting that smokers have reduced production of breastmilk and are likely to discontinue breastfeeding earlier (Napierala et al., 2016). It is suggested that some of these differences may be due to nicotine reducing maternal prolactin levels (Napierala et al., 2016). Smoking is also reported to adversely affect breastmilk composition with reduced fat content of breastmilk (Macchi et al., 2021; Napierala et al., 2016), increased toxic metal levels (Favara et al., 2024; Napierala et al., 2016), reduced antioxidant properties (Macchi et al., 2021) and altered immune molecule content (Favara et al., 2024; Macchi et al., 2021). As a result, infant growth, nervous system development and immunity are impacted in women who smoke, with infants of mothers who smoke more likely to suffer from infections such as respiratory tract and otitis media (Favara et al., 2024; Napierala et al., 2016). To support infant wellbeing and to improve duration of breastfeeding among women who smoke in West Sumatra, it is therefore essential to develop and deliver effective smoking cessation programmes during pregnancy and after birth.
Women with a high school or graduate education were significantly more likely to exclusively breastfeed at discharge within this study. A higher proportion of those with college or university education also exclusively breastfed at 6 weeks and 6 months, although this was no longer significant. Previous research in Indonesia regarding breastfeeding and education level has given conflicting results. Several surveys distributed to women across Indonesia suggested that women with no formal education were less likely to exclusively breastfeed (Laksono et al., 2021) and that women with postgraduate education were significantly more likely to exclusively breastfeed (Ananta et al., 2016). However, another survey in West Java suggested that women with higher education levels were more likely to provide their infant with breastmilk substitutes (Green et al., 2021). The reasons for this discrepancy within different cohorts are unclear.
Within our qualitative interviews, women appeared to be fairly knowledgeable about the benefits of breastfeeding. Other Indonesian studies have however found mixed results. One study found that women had been told by health professionals or community workers to breastfeed for 6 months, but that they had not been given reasons as to why (Hadi et al., 2021). A separate study found that not all rural mothers understood what exclusive breastfeeding was when asked to define it (Paramashanti et al., 2022). Additionally, they found that while women were aware of the health benefits of breastmilk for their infant, none mentioned the health benefits for themselves or the benefits for maternal infant bonding (Paramashanti et al., 2022). Women within our study were however aware of the benefits of breastfeeding for mother–infant bonding. They were also aware that breastfeeding is cheap, which is in line with other studies that also noted that women reported breastfeeding as an inexpensive way to feed their infant (Paramashanti et al., 2022). Women have also previously described being aware of the cost implication of weaning their infant off breastmilk due to the resultant need to buy food or breastmilk substitutes for their infants (Afiyanti and Juliastuti, 2012). Previous research in other areas within Indonesia have looked into women's reasons behind using breastmilk substitutes, not achieving exclusive breastfeeding despite planning to do so or early weaning. A common perception among women was of insufficient breastmilk supply to feed their infant (Afiyanti and Juliastuti, 2012; Paramashanti et al., 2022) especially among urban women (Paramashanti et al., 2022), and a perception that bigger babies required more than just breastmilk (Afiyanti and Juliastuti, 2012). Additional factors cited as reasons for providing nutrition other than breastmilk included infant illness and breast problems (Paramashanti et al., 2022).
Despite it being banned by the Indonesia government, advertising of breastmilk substitutes is still common in Indonesia, with 93.3% of women in one survey in West Java reporting seeing such advertisements on television, social media or in newspapers (Green et al., 2021). It has been suggested that advertisement of breastmilk substitutes influences women's timing of weaning (Afiyanti and Juliastuti, 2012). Of particular concern was that women from West Java commonly reported the use of breastmilk substitutes as they perceived they were beneficial for growth, intelligence and immunity (Green et al., 2021). Additionally, some women reported being hesitant to exclusively breastfeed their infants because a healthcare provider had given their baby breastmilk substitutes when they were in hospital (Afiyanti and Juliastuti, 2012). Healthcare providers recommending the use of breastmilk substitutes at some point since the birth of their child has also been reported by 22.7% of women (Green et al., 2021), with 23.3% of women recounting healthcare providers to have given breastmilk substitutes to their infant without the mother's permission (Ananta et al., 2016). This is of particular concern given that women have previously described being reliant on their midwives and healthcare professionals for receiving the majority of their breastfeeding information (Paramashanti et al., 2022).
The qualitative interviews also highlighted the wide cultural acceptance of the superiority of breastfeeding within West Sumatra and the family and other social support women received to achieve successful breastfeeding. Both of these aspects have previously been shown to be key factors. Normalisation of breastfeeding within a culture has previously been identified as a supportive factor for breastfeeding practice, with high rates noted in societies that value breastfeeding (Prentice, 2022). Additionally, seeing other women breastfeeding in public or seeing positive images of breastfeeding in mainstream or social media have also previously been identified as supporting successful breastfeeding (Snyder et al., 2021). In contrast women's discomfort at breastfeeding in social situations, for example in front of relatives or friends has been associated with lower rates of breastfeeding (Alyousefi, 2021; Gutierrez-de-Terán-Moreno et al., 2022). There are also known links between breastfeeding self-efficacy and social support within other countries, such as Iran and Turkey (Maleki-Saghooni et al., 2020; Mercan and Tari Selcuk, 2021). For example, having a female relative with a positive experience of breastfeeding has been associated with enhanced successful breastfeeding (Prentice, 2022). Conversely, a lack of familial support has been identified previously as a barrier to breastfeeding (Snyder et al., 2021), with the opinions of family and friends known to influence timing of weaning (Afiyanti and Juliastuti, 2012).
Although there are high rates of breastfeeding in Indonesia, the economic burden from treating gastrointestinal and respiratory infection in children under 2 years of age due to infants not being exclusively breastfed up to 6 months is still estimated to be US$118.6 million annually, which equated to 10.6% of the total annual health budget in Indonesia in 2012 (Siregar et al., 2018). Additionally, higher rates of stunting have been shown in children who have not been breastfed (Ananta et al., 2016), although the economic impact of this has not been calculated.
While breastfeeding knowledge has been shown to be high in some Indonesian studies, this is not universal which suggests that further improvements could be achieved. Our study highlights that interventions focussed on those with lower levels of education may potentially enhance breastfeeding rates in Indonesia. Several previous educational interventions have shown to be promising within Indonesia. One intervention that included six 2-hour long nutritional education sessions for pregnant women was beneficial towards knowledge, attitude and practices of child nutrition (Permatasari et al., 2021). A separate educational intervention undertaken in Java Indonesia that provided 30 postnatal women with a booklet within 10 days of giving birth showed increase breastfeeding self-efficacy (Prastyoningsih et al., 2021). However, no control group was included in this study and as breastfeeding self-efficacy would be expected to improve with increasing time postnatally, the impact of the intervention therefore remained unclear. While education can clearly highlight the positive health benefits of breastfeeding, building on existing positive social support and cultural norms about breastfeeding within Indonesia is also recommended to enhance breastfeeding rates. Additionally, interventions targeting smoking cessation during pregnancy and after birth could support enhanced breastfeeding duration within West Sumatra.
Limitations
A strength of this study was the prospective data collection. However, several limitations have to be noted. Firstly, all women within this cohort had received a nutritional supplement during pregnancy, with different forms of supplementation given in the intervention and control groups. It is unknown whether these women were therefore in a better nutritional state by the end of pregnancy, which may have influenced the slightly higher rates of exclusive breastfeeding in this sample compared to previous rates noted in West Sumatra. It should be emphasised that no additional information about the benefits of breastfeeding was provided for the study participants and breastfeeding data was analysed opportunistically. Breastfeeding data was self-reported by the woman, which may have led to social desirability bias. Finally, the limited number of women who did not provide any breastfeeds at each time point prevented analysis of these women according to maternal or birth characteristics.
Conclusions
Within West Sumatra there were exceptionally high rates of any breastfeeding with positive acceptance of breastfeeding by the mothers and their families. The exclusive breastfeeding rate of 64.7% and any breastfeeding of 96.0% at 6 months, is higher than in many other countries but still fell below World Health Organization recommendations. Interventions that support those with the lowest levels of education, as well as promoting smoking cessation during pregnancy and after the birth should be explored to build upon the existing positive social support and cultural norms about breastfeeding seen within West Sumatra. Lessons could also be learnt around socio-cultural and family support influences which may have impacted such high rates of breastfeeding in this community.
Supplemental Material
sj-docx-1-nah-10.1177_02601060251395426 - Supplemental material for Breastfeeding practices and attitudes among women in West Sumatra, Indonesia
Supplemental material, sj-docx-1-nah-10.1177_02601060251395426 for Breastfeeding practices and attitudes among women in West Sumatra, Indonesia by Frankie Fair, Katie Marvin-Dowle, Zuhrah Taufiqa, Nur Indrawaty Lipoeto and Hora Soltani in Nutrition and Health
Footnotes
Acknowledgements
With thanks to all of the women who volunteered to participate within the study and the interviews. With thanks to Amy Furness for her support in finding some of the relevant literature for the introduction and discussion sections.
Ethical approval
Ethical approval was obtained from Andalas University (707/KEP/FK/2019) in January 2019. Informed consent was gained from participants separately for the feasibility study and the qualitative interview component.
Author contribution
HS, NIL and FF contributed to the study conception and design. ZT conducted to the quantitative data collection and the interviews, FF and KMD preformed the data analysis, HS, FF, KMD interpreted the data and FF drafted the manuscript. HS, KMD, NIL and ZT critically revised and reviewed the manuscript. All authors approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was received from the Global Challenges Research Fund (GCRF) Research Councils United Kingdom (RCUK). For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.