
Abstract
Background
Only 2% of 4–8-year-old Australian children consume the daily recommended vegetable serves, with implications on the development of lifelong dietary behaviors. Evidence suggests that enhancing children's access, exposure and familiarity with vegetables can help increase their vegetable intake. Most children attend Early Childhood Education and Care (ECEC) services, which are well placed to increase vegetable consumption through curriculum change, play-based learning and parental education.
Aim
We aim to determine the efficacy of the ‘First Bite-Get it Right’ (First Bite) intervention to improve the vegetable intake of 3–5-year-old children in ECEC services compared to a control group.
Method
This 8-week cluster-randomized controlled trial involves ECEC services (n = 30) and children (n∼300) from socioeconomically disadvantaged areas in two local health districts in New South Wales, Australia and includes an intervention and wait-list control group. The First Bite program comprises: 1) Educator professional development; 2) Child daily “Veggie Break”; 3) Child experiential learning activities; and 4) Parent resources. Baseline and post-intervention measures include skin carotenoid scanning, vegetable serves plate waste, lunch box audits, child-reported vegetable preferences, and child parent-reported vegetable intake. Group-by-time interactions will be analyzed by linear mixed model regression, accounting for ECEC clustering.
Summary
This study will evaluate whether a comprehensive ECEC-based intervention can improve children's vegetable consumption in socioeconomically disadvantaged areas. The findings will inform recommendations for ECEC policies, educator training programs, and parent engagement strategies to promote healthy eating in early childhood.
Trial registration
Australian New Zealand Clinical Trials Registry: ACTRN: 12624000249550 (Date: 14/03/2024). https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=387095.
Introduction
Background and rationale
Problem statement
Dietary intake affects a child's weight (Garrido-Miguel et al., 2019) and 25% of Australian children are above a healthy weight before they start primary school. Only 20% of Australian 2–3-year-old children consume enough vegetables, dropping to only 2% of 4–8-year-old children (Australian Bureau of Statistics, 2022). The first 2000 days of life are crucial in developing food preferences (Davies et al., 2016). Experiential food learning in the early years creates the foundation for healthy eating habits. (Varman et al., 2021). Adequate vegetable consumption protects against chronic diseases, strengthens the immune system (Williams et al., 2020) and promotes healthy weight (Kaikkonen et al., 2013). These factors highlight the importance of establishing healthy eating practices early in life (Sunardi, 2022).
Current Early Child Education and Care (ECEC) context
The World Health Organization's Global Standards for Healthy Eating, Physical Activity, Sedentary Behavior and Sleep in Early Childhood Education and Care (ECEC) recommend: a) incorporating activities that develop children's understanding and abilities regarding healthy eating behaviors into ECEC programming; b) promoting supportive social environments around healthy eating behaviors; and c) engaging ECEC families and educators to support healthy eating behaviors being promoted (World Health Organization, 2021).
ECEC is an ideal setting for nutrition promotion. Educators are one of the primary gatekeepers of young children's food environments and experiences (Matwiejczyk et al., 2021). Australian children consume 40–67% of their daily food intake whilst attending ECEC services (Soanes et al., 2001). An Australian ECEC study found that where food is provided from home (lunchbox services), children consumed approximately one quarter of a serve of vegetables per day whilst in care, with less than half of the lunchboxes containing vegetables (Barnes et al., 2021). Over 62% of Australian children attend family day care, center-based ECEC services or preschool programs (Australian Institute of Health and Welfare, 2023) by 5-years-of-age. This highlights the reach and potential impact that these services can have on early childhood nutrition.
Munch & Move® (M&M) is a New South Wales (NSW) Ministry of Health initiative in Australia which aims to support child development through healthy eating and movement behaviors (NSW Ministry of Health, 2020). Almost all center-based ECEC services in NSW (88%–92%) are M&M trained (Green et al., 2020). Despite the other successes of M&M, the nutritional quality of children's lunchboxes remains poor (Barnes et al., 2021). The cost of fresh produce may be too expensive for communities of socioeconomic disadvantage. This creates a barrier to providing healthy family meals and lunch boxes (Barnes et al., 2021). Economic modelling from 2015 to 2016 showed that a 10% increase in population vegetable intake could save A$100 million in healthcare costs (Deloitte Access Economics, 2016). Therefore, programs that provide easier access to additional vegetables to children during care could improve consumption and ultimately benefit child health and government health expenditure.
Evidence gaps
Limited and uncertain evidence exists regarding the effectiveness of dietary interventions in ECEC settings. This is due to the large variety of strategies and measures in study designs and interventions, making it difficult to group them for analysis (Yoong et al., 2023). The validity of studies is also affected by the outcome measures, which rely on parental self-report of children's food intakes. Successful interventions have used more than one approach. These programs combine mealtime environment improvements with curriculum changes to promote fruit and vegetable consumption, as well as providing parents with educational resources. These have integrated ECEC policy changes, educator professional development, parent education and participation, and children's play-based experiential learning. The digital platforms for ECEC-parent communication (Stratigos and Fenech, 2020) can also effectively promote positive feeding strategies while discouraging inappropriate practices (Yoong et al., 2021).
Despite these insights, currently, high-quality evidence for effective interventions that improve preschool children's vegetable intakes is lacking. We have not found any programs that combine multiple efficacious intervention strategies, and also use an objective measure to assess dietary change. First Bite is a comprehensive intervention for children's vegetable consumption in ECEC settings, which aims to address this gap.
Theoretical framework
First Bite development was guided by the following three models –
Informed by the experiential learning model (Kolb and Kolb, 2012), activities were developed to promote child confidence in vegetable exploration and consumption through educator and peer interactions to increase familiarity with vegetables (Bell et al., 2021). They aimed to support greater liking, preference, and willingness to taste, through being actively involved and reflecting on experiences (Chawner and Hetherington, 2021).
Transtheoretical model principles (Prochaska et al., 2002) were used to guide educators and parents in raising awareness about the benefits of vegetables, encouraging changes toward healthier choices and supporting the maintenance of healthy eating habits. This approach aimed to foster a gradual and sustainable improvement in children's dietary intake. Strategies included educator training and social media messaging to parents to encourage movement toward normalising and encouraging vegetable consumption. Information about cheaper food acquisition strategies and recipes for quick meal preparation for time poor parents was provided, including links to supportive websites. These may support the transition into increasing vegetable provision by decreasing perceived or real barriers to change.
From the lens of Social Cognitive Theory, (Glanz et al., 2017) the curriculum provides children with the opportunity to observe healthy eating behaviors modelled by educators and parents. The hands-on activities and positive reinforcement of key messages help to support children's vegetable familiarisation and confidence in trying new vegetables.
Objectives
The aim of the study is to determine the efficacy of the First Bite intervention in improving:
Children's overall vegetable intake (primary outcome); Children's vegetable consumption at a vegetable focused morning tea break; Vegetable provision in lunchboxes; Children's vegetable intake at home; Confidence about child feeding practices related to vegetables.
It is hypothesized that children in the intervention group will demonstrate greater improvements in the following outcomes by the end of the intervention compared to the control group:
An increase in skin carotenoid levels (a marker of increased vegetable and fruit intakes); An increase in quantity of vegetables eaten while attending education and care services; A greater quantity and variety of vegetables packed from home in lunchboxes; Improved child liking for vegetables; An increase in parent-reported vegetables eaten by children at home; An improvement in parent's confidence regarding healthy child feeding practices.
These results will be used to inform future policies and practices in the NSW Early Childhood Education and Care context.
Methods
Trial design
This study protocol aligns with the SPIRIT checklist (SPIRIT Standard Protocol Items: Recommendations for Interventions Trials, 2020). The First Bite study is a parallel two arm clustered randomized control trial, clustered at the ECEC level with a 1:1 ratio using a superiority framework. The intervention group received an 8-week multi-component program informed by evidence from previous studies conducted in the ECEC setting, guidance on best practice (Hodder et al., 2024; Varman et al., 2021; World Health Organization, 2021) and theories of behavior change. The waitlist control group maintained standard Munch & Move® practice (NSW Ministry of Health, 2010). The intervention included strategies to embed vegetable promotion into ECEC curricula, provided opportunities for children to access vegetables while in care and engaged families to reinforce vegetable promotion at home. Center-based lunchbox ECEC services, providing care to children aged 3–5 years were recruited.
The 8-week intervention was designed to be delivered within a school term with a comprehensive curriculum. The duration and timing of the intervention was informed by the ECEC advisory group and the First Bite working group thus reflecting the values for collaboration as identified in the continuum of community participation (Draper et al., 2010). The ECEC Advisory Group played a key role in guiding program optimisation and determining acceptability of resources developed. The group also provided advice on feasible and appropriate implementation strategies within their sector, increasing the likelihood of high implementation fidelity and sustainability for possible future translation (Kirkegaard et al., 2024).
Methods: Participants, interventions and outcomes
Study setting
This study was conducted in ECECs located in areas of social disadvantage from Western Sydney Local Health District (WSLHD) and Illawarra Shoalhaven Local Health District (ISLHD) in NSW, Australia.
Eligibility criteria
ECEC services were eligible if they were ‘lunchbox only’ services (i.e., do not provide meals to children in care) and were located in Socio-Economic Indexes for Areas (SEIFA) 1 or 2 postcodes (Australian Bureau of Statistics, 2021), indicating relative social disadvantage, or if they served a community identified as a priority population by the LHD. Services represented on the ECEC Advisory Group were excluded.
Children were eligible if they were aged 3–5 years, attended the participating ECEC a minimum of two days a week and spoke English. Parents or guardians were eligible if they could read and understand Grade 6 level English.
Intervention
First Bite was delivered by educators within the ECEC setting. The intervention content included several key components: 1) repeated exposure to vegetables (Bell et al., 2021); 2) hands-on experiential learning activities (Varman et al., 2021); 3) encouraged reinforcement of this learning at home through parent information and resources (Savage et al., 2007); and 4) positive eating environment and responsive feeding practices within ECEC services (Byrne et al., 2022). The eight-week program included:
1) Daily “Veggie Break”
This activity provided children with the opportunity to taste different vegetables (Zeinstra et al., 2018), both common and less common. A theme song played at the commencement of the break, helped to orient children's attention to the break and create a positive atmosphere. Each week, three different vegetables were showcased during the break and emphasized during classroom activities. Children explored their vegetable of the week through vision, sound, touch, taste and smell (Bell et al., 2021). This activity provided opportunity for multiple tastings/exposure of the same vegetable, which is required for children to learn acceptance of new tastes and textures of vegetables (Hamdi et al., 2020).
2) Vegetable focused experiential learning activities
A weekly set of six experiential learning activities was presented on Monday/Tuesday and Thursday/Friday for eight weeks. Experiential learning activities enable children to experiment, explore, play and become familiar with materials and concepts through hands-on experiences (Birch et al., 1987; Gold et al., 2017; Illeris, 2007). This approach has been shown to be effective in improving children's nutrition-related behaviors, knowledge, and attitudes (Varman et al., 2021). The activities included vegetable focused storybooks, songs, gardening, art, sensory play and taste exposure experiences and physical activity games. Resources, activities and lesson plans were provided to ECEC educators. The activities aligned with all areas of the Australian Government's Early Years Learning Framework (Australian Government Department of Education [AGDE], 2022).
3) Resources for parents
Parents and caregivers play a key role in modifying healthy eating behaviors in young children, making their involvement in the intervention crucial (Niemeier et al., 2012). ECECs were asked to share weekly social media tiles and newsletters with families through their usual communication methods. The “Veggie of the week” was explored at the service (Nathan et al., 2019) and promoted for use in home meals (Vidgen and Gallegos, 2014). Newsletters included information on preparing vegetables for meals, vegetable eating tips, role modelling, and fussy eating. Practical tips to assist in packing a healthy lunchbox were also provided. Munch & Move® resources were also incorporated, with links provided in newsletters and social media tiles (Niemeier et al., 2012).
4) Professional development for educators
Training was provided on best practices for creating supportive mealtime environments. This included a series of 7 × 15-min video modules covering topics such as feeding roles (Bradbury, 2016), responsive feeding practices, role modelling, food refusal, reducing pressure to eat and addressing fussy eating, all aimed at promoting self-regulation of eating in children. These videos were co-designed by the authors (ED and SD) in collaboration with the LHD Health Promotion Service Early Years teams and the ECEC Advisory Group, and presented by ED and SD. The training modules aimed to assist educators in creating learning opportunities and social interactions for children to learn healthy eating behaviors through multiple learning opportunities and social interactions (Thorpe et al., 2022).
ECECs in the control group maintained Munch & Move® standard practice during the 8-week intervention period and were provided with intervention materials at the conclusion of the post-intervention data collection. Figure 1 illustrates the planned flow of participants throughout the study.
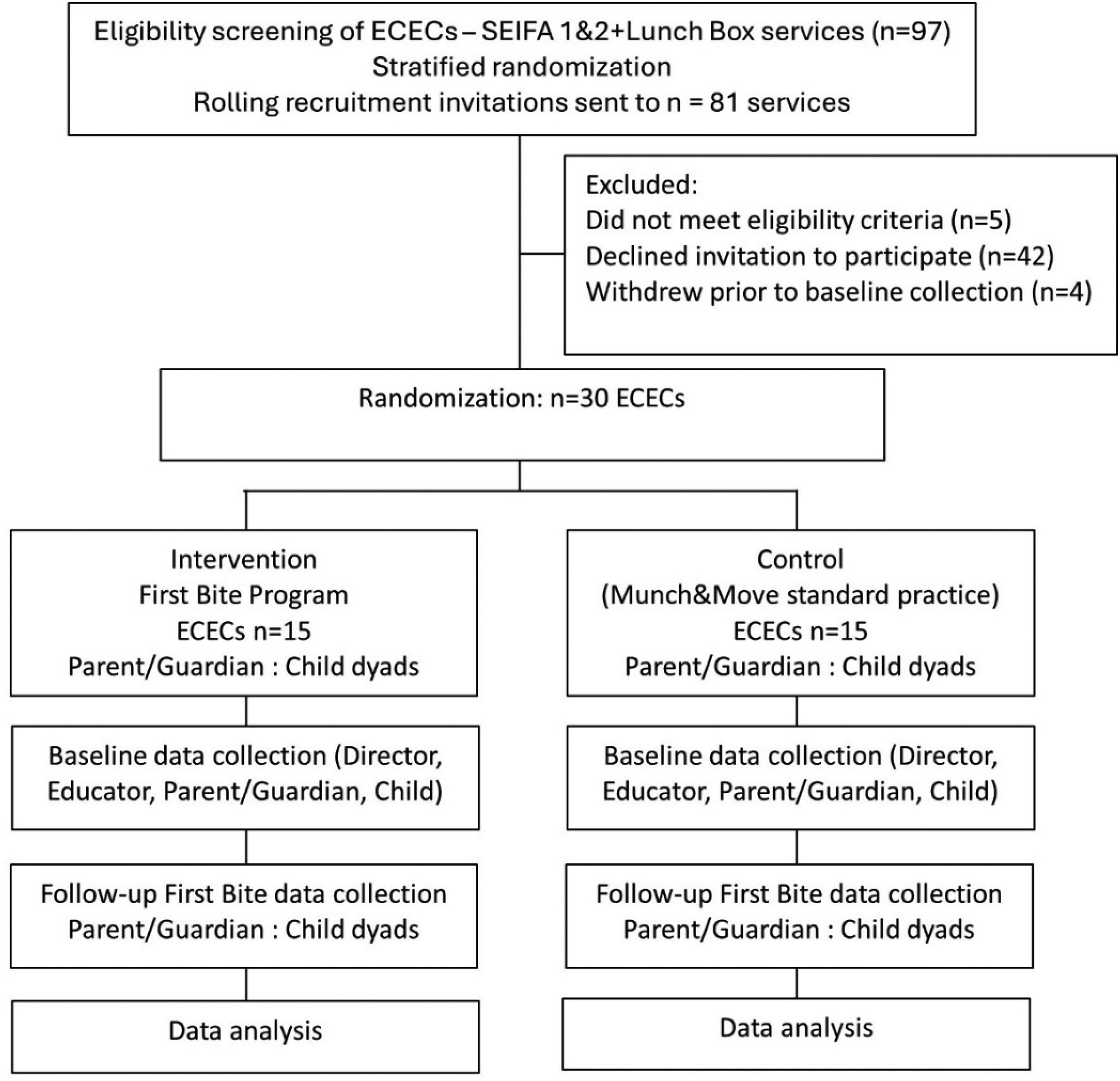
First Bite study flowchart.
Outcomes
Primary outcome
The primary outcome was children's overall vegetable intake, assessed objectively by reflection spectrometry-based Veggie Meter® skin carotenoid measurement (a measure validated in 3–5-year-old children) (Aguilar et al., 2014; Scarmo et al., 2012). The standardized measurement protocol developed by Radtke et al. (2021) was used. The average of three scans was taken for each child at each data collection timepoint. Changes in dietary intake of carotenoids become measurable after six weeks, and levels may start to decrease after three weeks following a reduction in intake (Whitehead et al., 2012). Post intervention carotenoid level data was therefore collected within two weeks of the end of the intervention (Tan et al., 2015).
Secondary outcomes
Children's vegetable consumption was captured using the following measures:
Vegetable serves plate waste (grams) data was measured for each individual child (Buzby and Guthrie, 2002) and aggregated to the ECEC level. This is a validated measure (Chapman et al., 2019) to determine the quantity of vegetables eaten by children. As “lunchbox only” services do not provide food for children, plate waste measurements were only conducted post-intervention to determine the effect of the “Veggie Break” component of First Bite. All children were offered pre-weighed bags of vegetables. Educators were asked to neither encourage nor dissuade children from eating the vegetables. An open invitation was then given for children to eat as many vegetables as they wished. A lunchbox audit (Chapman et al., 2019; Sweitzer et al., 2015) conducted at baseline and post-intervention assessed the presence, type and quantity (grams) of vegetables provided from home (Nathan et al., 2019). Separate vegetables were hygienically removed from their lunchboxes and weighed then returned. Mixed meals were weighed in their containers, and photographed directly from above and again at a 45-degree angle. Container weights were identified, and the percentage of vegetable in the mixed meal was estimated independently by two researchers and a registered dietitian with final percentages decided by consensus. The associated vegetable only weights were then recorded A parent/guardian survey including questions on child vegetable intake at home over the previous week was conducted at baseline and follow-up. The survey asked parents to indicate which vegetables from a list of 35, their children have eaten during the previous week, and their liking of the recipes and healthy eating topics addressed in the newsletters using Likert scales. This was to assess parent engagement with the program.
Children's familiarity and liking of vegetables were measured at baseline and follow-up using a preschool validated, pictorial 3-point face scale tool (Carraway-Stage et al., 2014). Facial expressions representing like, dislike or neutral (not sure) were shown to the children to identify their taste responses.
Parent/guardian confidence about child feeding practices was measured using questions from Go NAPSACC: Nutrition and Physical Activity Self-Assessment for Child Care, 2nd Edition (Ward et al., 2014) at baseline, post-intervention and follow-up.
Personal demographics and a survey of household food security status were measured, including using two questions from The Hunger Vital Sign (Hager et al., 2010). This provided individual-level data to nuance participants’ lower socioeconomic contexts.
Sample size
A target sample size of 30 ECEC services and 288 child participants (approximately 10 children per service) was determined by a statistician using the Parallel Group-Randomized Trial (GRT) Sample Size Calculator (National Institutes of Health, 2024). A mid-range interclass correlation of 0.1 was used, with 80% power to detect a standardized effect size of 0.5 (medium) and significance of 5% (P ≤ 0.05) based on the effect size from a meta-analysis of change in vegetable intake from interventions in children less than 5 years (Hodder et al., 2018). This clustered sample design incorporated a 20% buffer for participant attrition (Mirmiran et al., 2021; Perna et al., 2022; Yoong et al., 2023).
Recruitment
A computerized random number generator selected the ECEC services from a list of 97 eligible services. A statistician with no other involvement in the study performed the stratified randomization of the ECEC services to produce a representative weighted LHD randomized list who were invited to join the study. Following email invitation to join First Bite, successfully recruited services then recruited parent/guardian and child dyads. Services on the randomized list, were sequentially sent invitations, commencing with the first 30 services. Invitees had two weeks to either accept or decline the invitation before the next round of invitations was sent. This process continued until the sample size was achieved. Services randomized from the same ECEC business but at different sites were placed into the same research group to decrease contamination risk between study groups. Following the initial email invitation, researchers followed-up with services’ interest via phone calls and a second email. LHD representatives supported recruitment efforts of parent/guardian and child dyads by designing and sharing targeted social media advertising and via phone calls.
The study invitations included a Participant Information Sheet with a link for directors to provide online consent on behalf of their service. Directors were asked to forward the Participant Information Sheet and online consent form to their educators who were willing to participate. Recruited ECECs distributed the First Bite information video, poster, online Participant Information Sheet and consent form to their families through their centre's usual communication method. Paper consent forms were also available if preferred. Researchers were available via email to answer any questions from directors, educators or parents.
Rolling recruitment commenced in May 2024. Participants could choose to withdraw from data collection at any time without consequence.
Incentives
All ECEC services received a $150 AU voucher for signing up for the study and a $100 AU gift voucher upon full completion of the study. The control group also received a $150 AU supermarket voucher in lieu of vegetables at the end of the study.
Methods: Assignment of intervention for RCT
ECEC services were assigned to the intervention or control group by a computerized random number generator (R) using a 1:1 ratio. ECEC group assignment remained concealed until baseline data collection bookings were arranged. Blinding to group allocation was not feasible as it would be evident to participants and data collectors which ECECs were receiving the intervention. Therefore, data collector training was provided in using objective measures and avoiding bias. Individual services were not told which other ECEC services had been recruited. Participant surveys were accessed by individualised coded links directly to REDCap and could not be shared. All participants received the surveys developed for their particular groups. A 6-month post-intervention follow-up survey will also be sent to parent/guardians and ECEC service directors to identify any longer-term effects of First Bite.
Methods: Data collection, management, and analysis
Data collection methods
Blinding of participants was not possible, given children, parents and educators at the intervention services received vegetable promotion and First Bite branded materials. At baseline data collection, services and their families were not aware whether they were allocated to the intervention or control group. At both baseline and follow-up, families were not aware which day the lunchbox audits would occur, so as not to influence the foods brought on those days. Educators were not involved with data collection for the vegetable serves plate waste, apart from identifying which children had been recruited to the program and handing out the coded, pre-weighed vegetable ziplock bags.
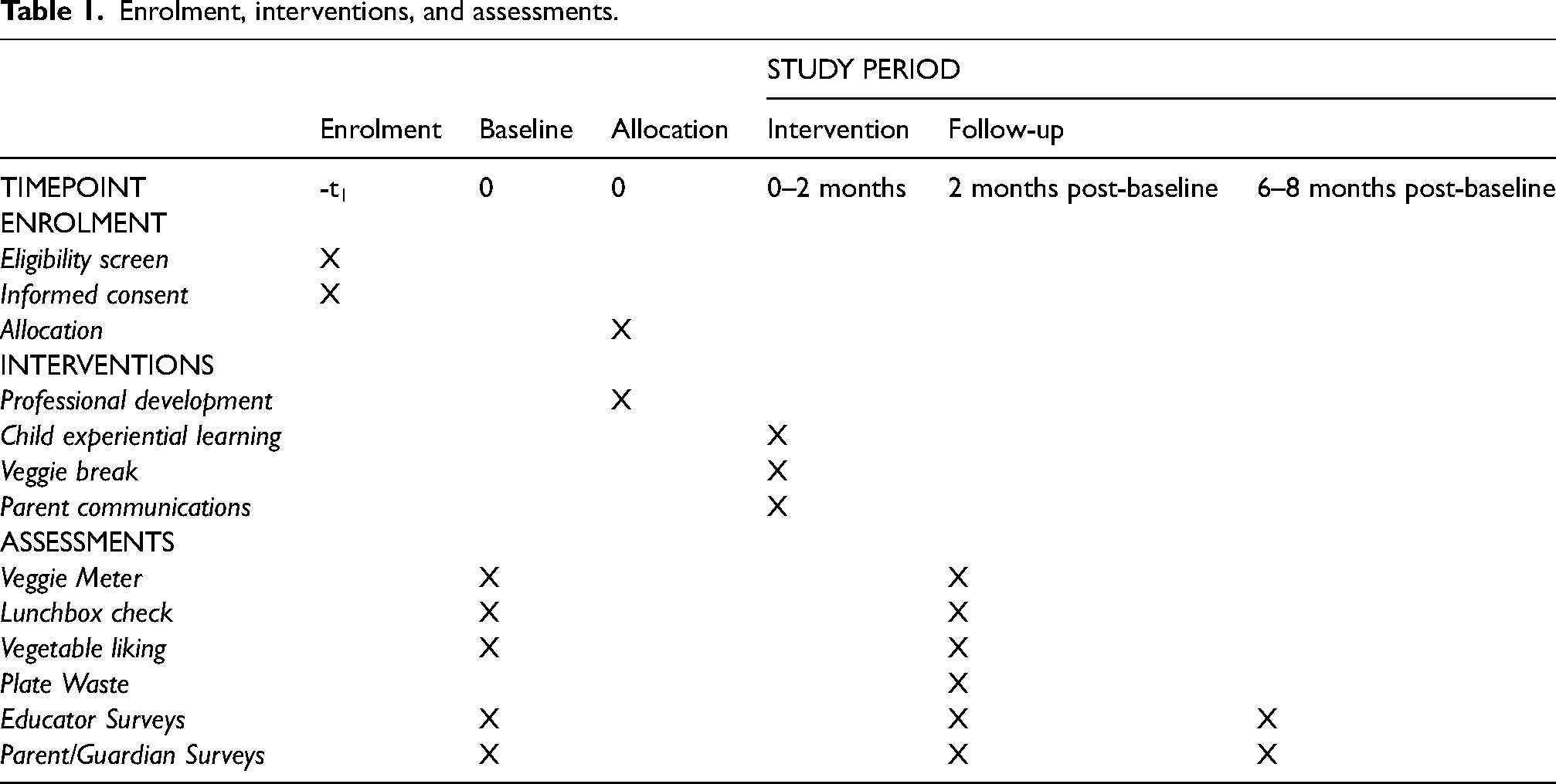
The trained data collection team comprised LHD staff, research assistants, the PhD candidate and academic supervisors. Measures were collected at baseline and post-intervention, which was planned for completion by December 2024. A longer-term follow-up will be completed in 2025. Table 1 enrolment, interventions and assessments illustrates the project timing
Enrolment, interventions, and assessments.
Process evaluation
ECECs received a weekly electronic fidelity survey prompt to record the activities conducted with the children, the “Veggie Break” and any program reflections. Mid-way through the intervention and at the end of the program, a researcher contacted ECEC directors to discuss any implementation challenges.
Parents’ engagement with social media tiles and newsletters was measured through a mixed methods survey. This survey included questions from previously validated tools, incorporating both Likert scoring and qualitative reflection questions (Rylatt and Cartwright, 2016) along with First Bite resource focused questions.
An educator survey assessed changes identified in the ECEC environment over the course of the First Bite intervention. The survey included validated questions from the Creating Healthy Eating & Active Environments survey (CHEERS) (Lafave, 2019) and the Nutrition and Physical Activity Self-Assessment for Child Care (NAPSACC) (Ward et al., 2014) tools, and questions from the Munch & Move® Monitoring Guide for Enhanced Practices for Center-based Early Childhood Services (Farrell et al., 2014) to help understand changes to ECEC service functions.
A director survey identified changes within the ECEC service at an administrative level. An interview with the director at post-intervention also provided their perspective on the First Bite curriculum and any considerations for future improvements. Data collected will be used to assess program implementation variability across centres, which may influence outcomes.
Data management
Study data were collected and managed using REDCap electronic data capture tools, including the REDCap Mobile Application (Harris et al., 2021), hosted at the University of Wollongong (UOW), Australia (Harris et al., 2009, 2019) and will be kept on the UOW Microsoft Teams research data storage service until children are 25 years of age. All participant data will be de-identified prior to any analysis and reporting. Individual participant data will not be reported.
Statistical analysis
The efficacy of First Bite will be tested using an intention-to-treat approach. Statistical analyses will be conducted using IBM SPSS Statistics Version 29.0.2.0 (IBM, 2024). Inferential statistics will be calculated to determine group-by-time interactions for carotenoid level, plate waste and lunchbox audits using linear mixed model regression analyses which can account for missing data. Results will also be triangulated for correlational findings under the guidance of a statistician. Group-by-time interactions for child “liking” of vegetables using Likert scoring will be analyzed with generalized linear mixed model regression analysis. All analyses will account for clustering across ECEC services using random intercepts.
Qualitative analysis
NVivo 14 (2023), will be used to identify relevant themes from ECEC director interviews regarding their perspectives on the First Bite program content. The barriers and enablers to implementation, educator support, and changes identified in child behavior toward vegetables and feedback from the families will be investigated.
Methods: Monitoring
Data monitoring/harms
Researchers all have a current Working with Children Check (a legal requirement for working with children in NSW) (NSW Government, 2024). A data monitoring committee was not formed as the project involves no risk of emotional, social, financial harm or physical harm, and no invasive procedures.
Summary
Very few children consume the recommended servings of vegetables. The formative years while in ECEC provide an opportunity to promote vegetable consumption to children through experiential learning. To our knowledge, First Bite is the first Australian study to test the efficacy of an ECEC intervention that uses a multi-component approach, integrating successful elements of previous experiential learning nutrition interventions. The intervention specifically targets socioeconomically disadvantaged populations, who experience specific barriers to providing healthy foods to their children. Assessing skin carotenoid levels using a validated objective method represents a unique primary outcome measure in the Australian context. If successful, First Bite strategies have the potential for broader application and scalability through integration into the current NSW Health Munch & Move® program.
Supplemental Material
sj-pdf-1-nah-10.1177_02601060251360303 - Supplemental material for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol
Supplemental material, sj-pdf-1-nah-10.1177_02601060251360303 for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol by Sharon Duncan, Megan Hammersley, Jennifer Norman, Sarah T Ryan, Emma Davies, Rebecca Junor Cook, Monica Nour, Laura Attallah and Bridget Kelly in Nutrition and Health
Supplemental Material
sj-pdf-2-nah-10.1177_02601060251360303 - Supplemental material for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol
Supplemental material, sj-pdf-2-nah-10.1177_02601060251360303 for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol by Sharon Duncan, Megan Hammersley, Jennifer Norman, Sarah T Ryan, Emma Davies, Rebecca Junor Cook, Monica Nour, Laura Attallah and Bridget Kelly in Nutrition and Health
Supplemental Material
sj-docx-3-nah-10.1177_02601060251360303 - Supplemental material for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol
Supplemental material, sj-docx-3-nah-10.1177_02601060251360303 for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol by Sharon Duncan, Megan Hammersley, Jennifer Norman, Sarah T Ryan, Emma Davies, Rebecca Junor Cook, Monica Nour, Laura Attallah and Bridget Kelly in Nutrition and Health
Supplemental Material
sj-pdf-4-nah-10.1177_02601060251360303 - Supplemental material for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol
Supplemental material, sj-pdf-4-nah-10.1177_02601060251360303 for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol by Sharon Duncan, Megan Hammersley, Jennifer Norman, Sarah T Ryan, Emma Davies, Rebecca Junor Cook, Monica Nour, Laura Attallah and Bridget Kelly in Nutrition and Health
Supplemental Material
sj-docx-5-nah-10.1177_02601060251360303 - Supplemental material for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol
Supplemental material, sj-docx-5-nah-10.1177_02601060251360303 for “First Bite”: An intervention to increase children's vegetable consumption in Early Childhood Education and Care (ECEC) services in areas of high socioeconomic disadvantage – a cluster randomized controlled trial protocol by Sharon Duncan, Megan Hammersley, Jennifer Norman, Sarah T Ryan, Emma Davies, Rebecca Junor Cook, Monica Nour, Laura Attallah and Bridget Kelly in Nutrition and Health
Footnotes
Ethical considerations
Ethics approval was granted from the Hunter New England Human Research Ethics Committee on 22/11/2023 (Reference: 2023/ETH02497). The trial is registered with the Australian New Zealand Clinical Trials Registry (ACTRN 12624000249550). Date: 14/03/2024. Protocol amendments will be documented in the ANZCTR after Working Group approval. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=387095
All ECEC staff and parents, on behalf of their children, have provided written or digital informed consent before participating.
Consent to participate
All protocols surrounding informed consent, confidentiality and privacy are being upheld. All ECEC staff, and parents/guardians on behalf of their children, provided written or digital informed consent before participating in the study.
Consent for publication
All authors have approved the final manuscript for publication.
Authors’ contributions
BK, MH and JN conceptualized the research, formulated the overarching research goals and aims, supervised the PhD student (SD), supported data collection and provided feedback on this article. RJC was involved in designing the program, supported data collection and review of the article. MN and LA were involved in designing the program and review of the article. SR supported the development of data collection tools, and formatting of the manual and print resources, budget management, assisting with staff and ECEC engagement and reporting and provided feedback on this article. ED and SD contributed to methodology design and resource development, scripting and presenting educator training videos and data collection. SD wrote the original draft and will analyse outcomes. All authors reviewed and edited the manuscript and approved the final draft. There is no intention to use professional writers.
Funding
This work was supported by the Prevention Research Support Program, funded by the New South Wales Ministry of Health. This research has been conducted with the support of the Australian Government Research Training Program Scholarship. Funding was also received from the University of Wollongong Major Equipment Grant for equipment to measure skin carotenoid levels. Dr Jennifer Norman receives salary support from the NSW Health Prevention Research Support Program.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will not be made available in accordance with ethics approval documentation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.