
Abstract
Introduction
In 2015, the World Health Organization (WHO) published a framework for healthy ageing, emphasizing the interactions of three constructs: intrinsic capacity (i.e., the composite of all the physical and mental capacities of the individual), environment, and functional ability (i.e., the health-related attributes that enable people to be and to do what they have reason to value) (World Health Organization, 2015). The link between vitality, one of the six domains constituting intrinsic capacity, and nutrition is well-established (Cesari et al., 2018, 2022). The promotion of healthy ageing is closely related to the nutritional status of the individual, and this latter should always be screened, assessed, and monitored when approaching to older persons (Integrated Care for Older People (ICOPE): guidance for person-centred assessment and pathways in primary care, n.d.).
The prevalence of food allergies (FAs) is increasing worldwide (NIAID-Sponsored Expert Panel et al., 2010; Santos et al., 2023). An FA is usually considered as a condition that mostly affects people during their early phases of life, and the problem is often overlooked, if not neglected, in older persons (Azzolino et al., 2024). However, an increase in adult-onset FAs has also been reported (Warren et al., 2023). Several meta-analyses have suggested that the prevalence of FAs in adults ranges from 2% to 35%, depending on assessment methods [1–3]. It has been discussed that, despite the onset of FAs often occurring during the early phases of life, they can become manifest and persist in adulthood and older life (Kamdar et al., 2015; Kanny et al., 2001; NIAID-Sponsored Expert Panel et al., 2010; Santos et al., 2023; Spolidoro et al., 2021).
Literature on FAs has still largely focused on children and young adults, and little is currently known about FAs in later stages of life (Santos et al., 2023). Several age-related factors (Azzolino et al., 2021) may potentially mediate, mask, or enhance the clinical manifestations of FAs in older people (Azzolino et al., 2024). These include mechanisms related to immuno-senescence (Bakos et al., 2006), changes in gastrointestinal function (Bakos et al., 2006; Untersmayr and Jensen-Jarolim, 2008) and microbiota composition (Zhao et al., 2019), as well as conditions typical of old age (e.g., micronutrient deficiencies; (Chambers and Hawrylowicz, 2011; Diesner et al., 2011; Haase and Rink, 2009; Prasad, 1998) and polypharmacy (Chovatiya et al., 2023; Herman, 2020; Schöll et al., 2005)). Symptoms of FAs such as dyspepsia, vomiting, diarrhoea, and skin reactions might be confused with the consequences of other conditions affecting the older person, or remain unexplored because considered an unavoidable corollary of aging (Bakos et al., 2006).
For all the above-mentioned reasons, it can be expected that FAs may represent a relevant health concern in older people, warranting more careful consideration in the clinical setting. In this context, it cannot be overlooked that the main and safest strategy for the FA management is the allergen avoidance (NIAID-Sponsored Expert Panel et al., 2010). The consequent dietary restriction, especially if conducted by the individual without a professional supervision, can exacerbate the risk of nutritional deficiencies and undernutrition in older people (Azzolino et al., 2024; Rathnayake et al., 2015; Skypala and McKenzie, 2019). However, it has been recently highlighted that there is a notable knowledge gap also among food allergy specialists and allied health professionals, especially for what concerns dietary care (Memauri et al., 2022).
This article presents the protocol for a systematic review and meta-analysis specifically aimed at estimating (1) the prevalence of any type of immunoglobulin E (IgE) mediated FAs in older people considering the different assessment methods available, (2) the prevalence of IgE-mediated FAs in low-and-middle-income countries (LMICs) versus high-income countries (HICs), and (3) the prevalence of the most frequent types of IgE mediated FAs (e.g., cow's milk, egg, wheat, tree nuts, peanuts, fish, and shellfish).
Methods
The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement and checklist will be followed for reporting the results of the study. The summary of this systematic review and meta-analysis protocol was registered in the International Prospective Register of Systematic Reviews PROSPERO (registration number: CRD42023445399). If any changes are made to the protocol, these will be registered by submission of an updated version to PROSPERO, and documented on the final manuscript together with the results of the systematic review.
Search strategy
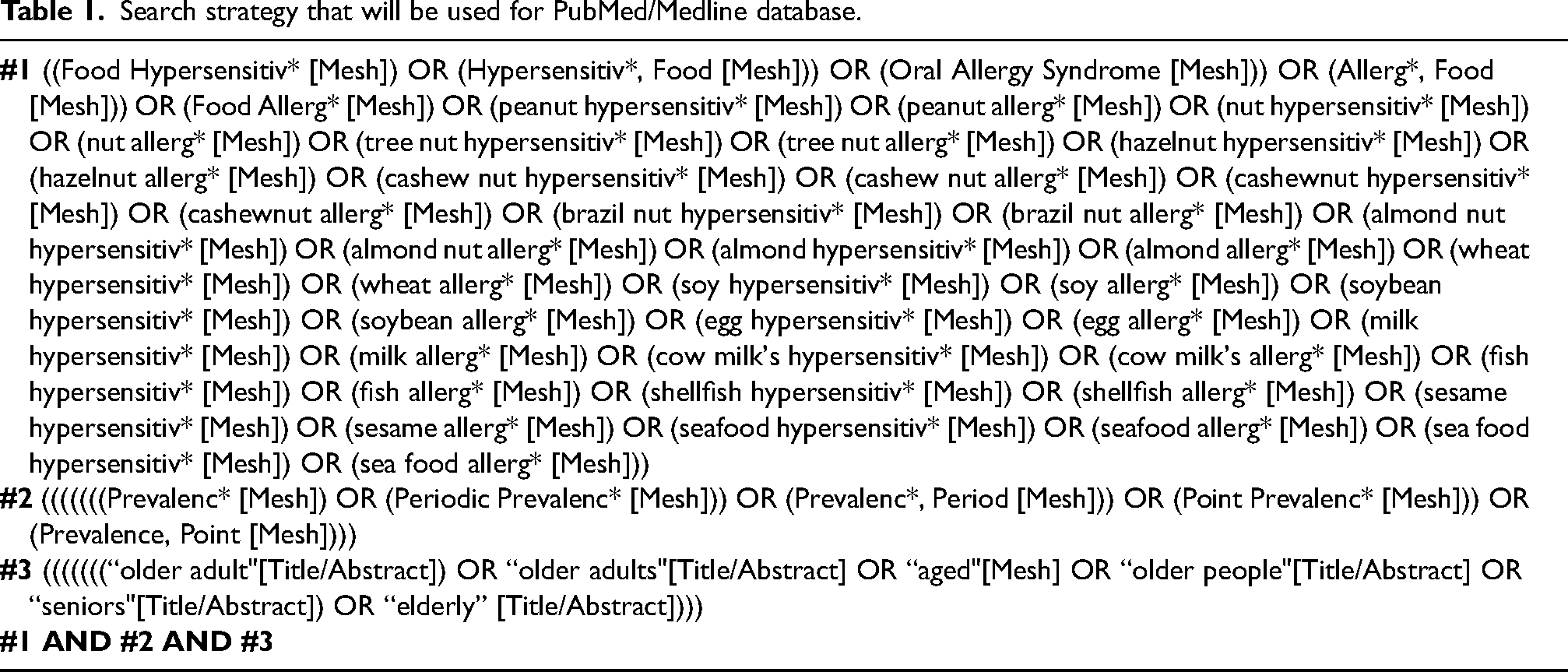
Searches will be conducted using databases such as PubMed/MEDLINE, Scopus (including EMBASE), and Web of Science for peer-reviewed studies. Search dates will be from the inception. Reference lists of included studies will be hand searched for additional relevant studies. Search terms for PubMed/Medline database, detailed in Table 1, will be adapted to other databases.
Search strategy that will be used for PubMed/Medline database.
Inclusion and exclusion criteria
Observational studies including prospective, case-control, and retrospective cohort studies will be included. Systematic reviews and meta-analyses on the topic will also be explored for identifying other relevant studies. As the WHO considers older persons as those aged 60 and older, this will be the cut-point used to select eligible entries.
Only English-language studies with full-text availability will be included. All other study designs, including narrative reviews, abstracts, control arms of clinical trials, expert reviews or other reviews, discussion papers, non-research letters and editorials, qualitative studies, case studies, case series, and animal studies, will be excluded. Studies on children and adolescents, not reporting data on FAs in older people or in which the number of older people with FAs cannot be quantified will be also excluded. Adverse food reactions that are non-IgE mediated (e.g., food protein-induced enteropathy and celiac disease) and non-immune mediated (e.g., lactose intolerance) will be excluded. We will also exclude studies restricted to the prevalence of FAs in groups with asthma, eczema, or allergic rhinitis, and those performed in selected clinical populations, which could lead to a biased estimate of FAs prevalence in the community.
Study selection
The title and abstract of each document will be independently screened by two reviewers to establish whether the document addresses FAs in older people and to be considered for full-text evaluation. If the two reviewers will disagree on the status of a document, the assessment will be discussed to reach an agreement. Subsequently, the full text of all the retained articles will be examined by two reviewers (DA and IB) for relevance against the study objectives. In case of uncertainty, the two reviewers will consult each other. If the consultation will not lead to a decision, another team member (SP or GCIS) will be consulted.
Data extraction
For each selected study, information about the author(s), publication year, country, study design, setting, assessment method(s), type of FAs considered, number of participants aged 60+, number and percentage of FAs events, eventual other comorbid conditions will be extracted by the two reviewers and will be cross-checked to verify the accuracy and consistency of the data. Any differences in the above process will be solved through discussion between the two authors, and any further differences will be arbitrated by a third reviewer. A descriptive summary with data tables will be elaborated.
Outcome assessment
The main outcome will be the prevalence of any type of FA diagnosed through self-reporting, tests for sensitization (e.g., specific IgE and skin prick test), combination of medical history plus tests for sensitization, food challenge (both open challenge and double-blind placebo-controlled food challenge). Stratified analyses according to country income level and FA type (e.g., cow's milk, egg, wheat, tree nuts, peanut fish, and shellfish) will be performed.
Study quality assessment
The risk of bias will be independently assessed for each study by two reviewers using the Joanna Briggs Institute Critical Appraisal Checklists for Prevalence and Cohort Studies. The grading of each study as well as of its components (e.g., appropriateness of the study design for the research question, risk of selection bias, exposure measurement, and outcome assessment) will be provided. Disagreements between the two reviewers will be resolved by the involvement of a third one. There will not be an assessment for publication bias via other standard methods (e.g., funnel plots and associated tests), since these tests have been developed for comparative studies and, therefore, may not produce reliable results for the meta-analysis of proportions (Hunter et al., 2014; Lin, 2019).
Data analysis
All frequency estimates of FAs will be recalculated if adequate data are provided. In case of discrepancies between our recalculated estimates and those of the original authors, we will report our recalculated estimates. Our recalculated estimates will be based on minimal measured events rather than the extrapolated ones.
For outcomes reported by three or more studies, a meta-analysis will be performed. Due to expected clinical and methodological heterogeneity between the primary studies, all meta-analyses will be performed using a random-effect model according to the Der Simonian-Laird approach with inverse variance weights. Heterogeneity between effect sizes of included studies will be evaluated by visual inspection of the forest plots and by using the χ² test for heterogeneity rather than I². All analyses will be performed with R version 4.3.2 (R: The R Project for Statistical Computing, n.d.) using the meta-package (Balduzzi et al., 2019).
Summary
This article describes the protocol of a systematic review and meta-analysis to estimate the prevalence of FAs in older people. If FAs are identified as a prevalent issue in older persons, they should consequently be considered for inclusion in decisional algorithms as potentially affecting the individual's intrinsic capacity and hampering healthy ageing.
Footnotes
Authors’ contributions
DA contributed to conceptualizing and writing the article. IB, SP, EC, GCIS, MC, and TL edited and revised the article. DA, IB, SP, EC, GCIS, MC, and TL approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and dissemination
The present study is exempted from submission to the local Ethics Committee as based on publicly available scientific data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.